
Is Resistance Training an Option to Improve Functionality and Muscle Strength in Middle-Aged People with Multiple Sclerosis? A Systematic Review and Meta-Analysis


 ,
,  ,
,  ,
,  ,
,  and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Sources of Information
2.2. Search Strategy
2.3. Inclusion Criteria
2.4. Exclusion Criteria
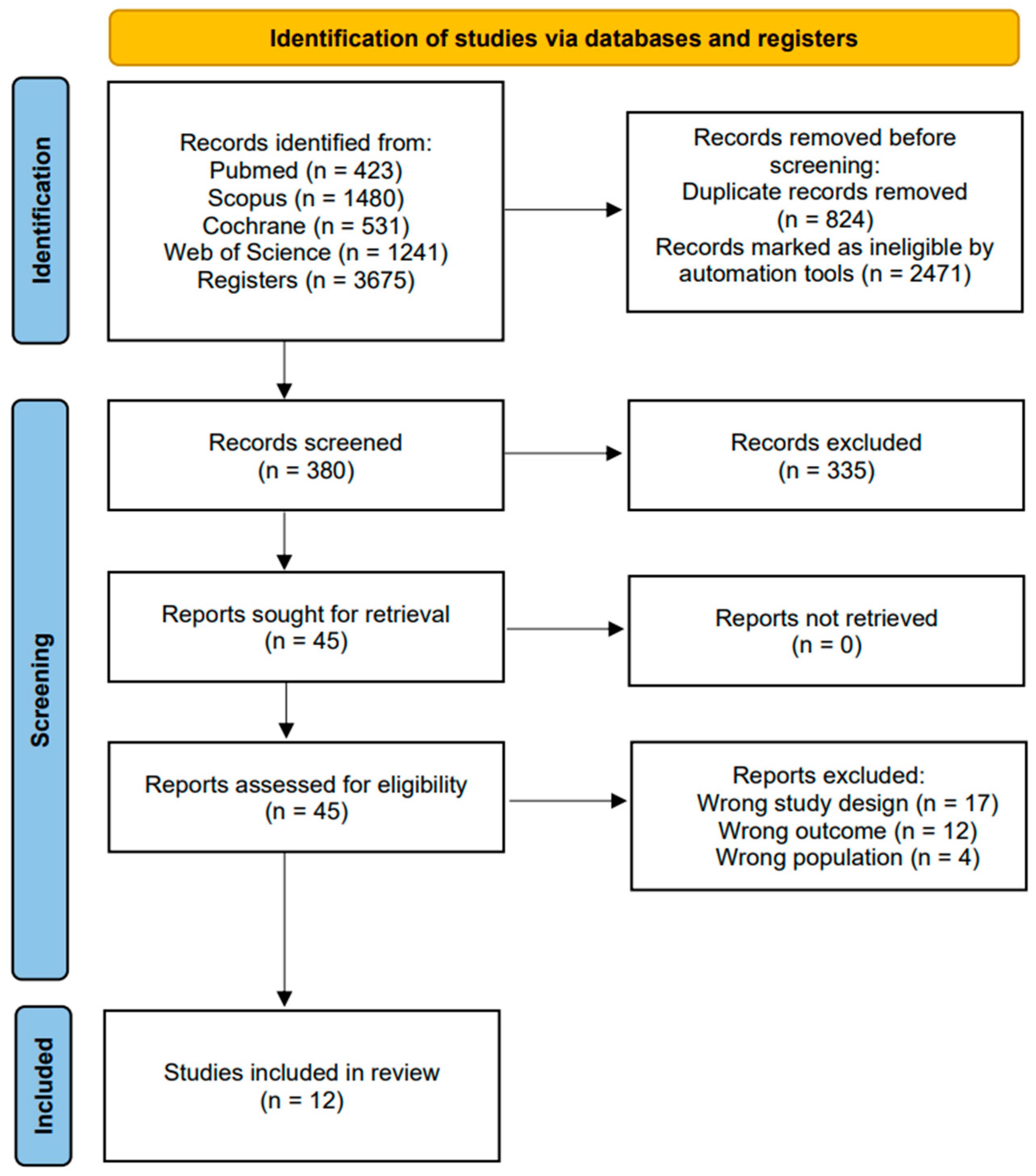
2.5. Study Selection Process
2.6. Data Extraction
2.7. Assessment of Methodological Quality
2.8. Analytic Decisions for Meta-Analysis
3. Results
3.1. Methodological Quality
3.2. Characteristics of the Studies
3.3. Outcomes
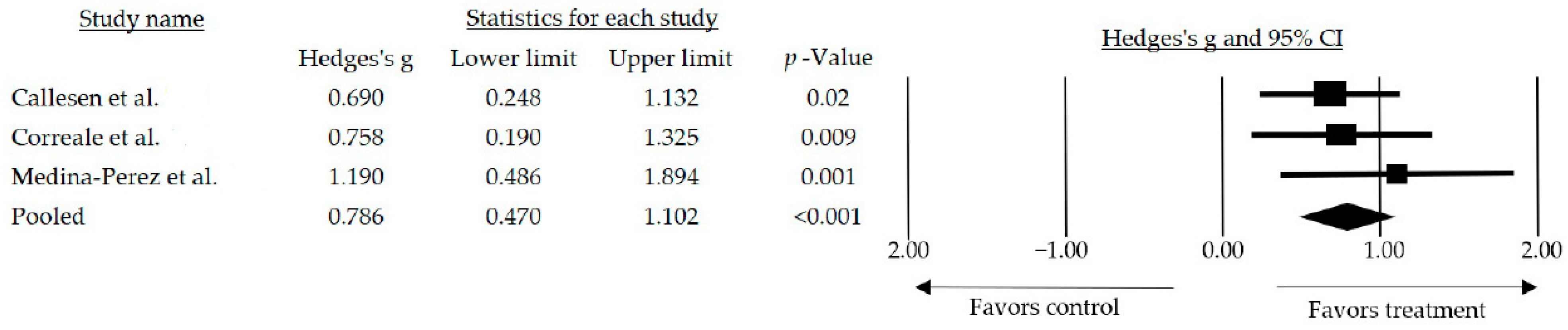
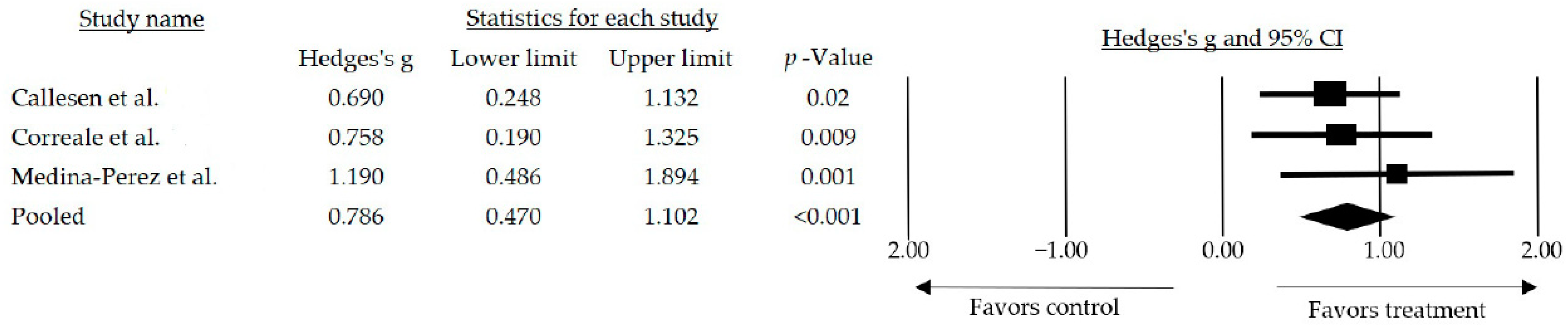
3.3.1. Muscle Strength
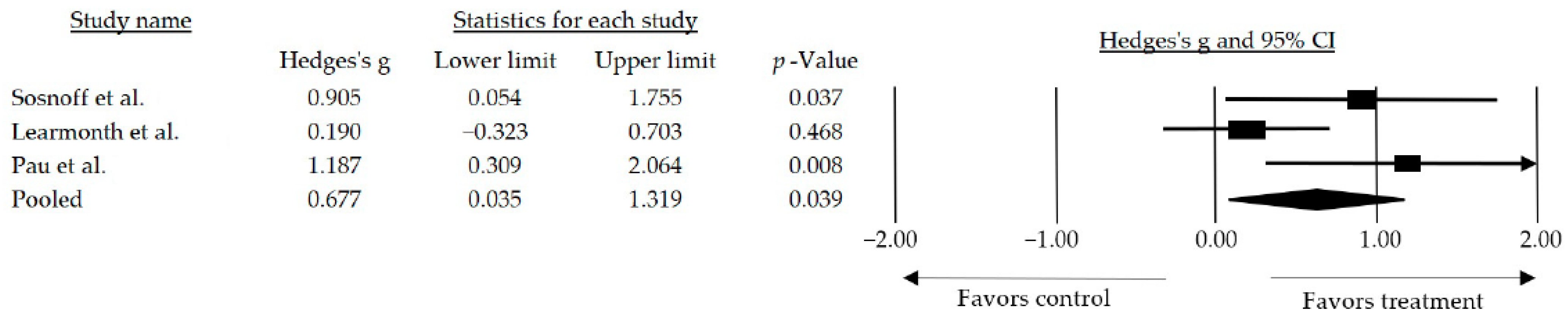
3.3.2. Walk Performance
3.3.3. Fatigue
3.3.4. The Quality of Life
3.4. Adverse Events
3.5. Publication Bias
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Oh, J.; Vidal-Jordana, A.; Montalban, X. Multiple sclerosis: Clinical aspects. Curr. Opin. Neurol. 2018, 31, 752–759. [Google Scholar] [CrossRef]
- Filippi, M.; Bar, A.; Piehl, F.; Preziosa, P.; Solari, A.; Vukusic, S.; Rocca, M. Mulitple sclerosis. Nat. Rev. Dis. Primer. 2018, 4, 43. [Google Scholar] [CrossRef]
- Correale, J.; Gaitán, M.I.; Ysrraelit, M.C.; Fiol, M.P. Progressive multiple sclerosis: From pathogenic mechanisms to treatment. Brain 2017, 140, 527–546. [Google Scholar] [CrossRef] [PubMed]
- Marcus, R. What Is Multiple Sclerosis? JAMA 2022, 328, 2078. [Google Scholar] [CrossRef] [PubMed]
- Dobson, R.; Giovannoni, G. Multiple sclerosis—A review. Eur. J. Neurol. 2019, 26, 27–40. [Google Scholar] [CrossRef] [PubMed]
- Dardiotis, E.; Arseniou, S.; Sokratous, M.; Tsouris, Z.; Siokas, V.; Mentis, A.F.A.; Michalopoulou, A.; Andravizou, A.; Dastamani, M.; Paterakis, K.; et al. Vitamin B12, folate, and homocysteine levels and multiple sclerosis: A meta-analysis. Mult. Scler. Relat. Disord. 2017, 17, 190–197. [Google Scholar] [CrossRef]
- Nourbakhsh, B.; Mowry, E.M. Multiple sclerosis risk factors and pathogenesis. Contin. Lifelong Learn. Neurol. 2019, 25, 596–610. [Google Scholar] [CrossRef]
- Fernández, O.; Fernández, V.E.; Guerrero, M. Esclerosis múltiple. Med.-Programa Form. Médica Contin. Acreditado 2015, 11, 4610–4621. [Google Scholar] [CrossRef]
- Browne, P.; Chandraratna, D.; Angood, C.; Tremlett, H.; Baker, C.; Taylor, B.V.; Thompson, A.J. Atlas of multiple sclerosis 2013: A growing global problem with widespread inequity. Neurology 2014, 83, 1022–1024. [Google Scholar] [CrossRef]
- Rotstein, D.L.; Chen, H.; Wilton, A.S.; Kwong, J.C.; Marrie, R.A.; Gozdyra, P.; Krysko, K.M.; Kopp, A.; Copes, R.; Tu, K. Temporal trends in multiple sclerosis prevalence and incidence in a large population. Neurology 2018, 90, 1435–1441. [Google Scholar] [CrossRef]
- Izquierdo, G.; Venegas, A.; Sanabria, C.; Navarro, G. Long-term epidemiology of multiple sclerosis in the Northern Seville District. Acta Neurol. Scand. 2015, 132, 111–117. [Google Scholar] [CrossRef]
- Ostolaza-Ibáñez, A.; Corroza-Laviñeta, J.; Ayuso-Blanco, T. Immunosenescence: The role of age in multiple sclerosis. Neurologia 2020, S0213–4853, 30226–30227. [Google Scholar] [CrossRef]
- Hanlon, P.; Nicholl, B.I.; Jani, B.D.; Lee, D.; McQueenie, R.; Mair, F.S. Frailty and pre-frailty in middle-aged and older adults and its association with multimorbidity and mortality: A prospective analysis of 493 737 UK Biobank participants. Lancet Public Health 2018, 3, 323–332. [Google Scholar] [CrossRef]
- Halabchi, F.; Alizadeh, Z.; Sahraian, M.A.; Abolhasani, M. Exercise prescription for patients with multiple sclerosis; potential benefits and practical recommendations. BMC Neurol. 2017, 17, 185. [Google Scholar] [CrossRef] [PubMed]
- Motl, R.W.; Sandroff, B.M. Benefits of Exercise Training in Multiple Sclerosis. Curr. Neurol. Neurosci. Rep. 2015, 15, 62. [Google Scholar] [CrossRef] [PubMed]
- Donze, C.; Massot, C.; Hautecoeur, P.; Cattoir-Vue, H.; Guyot, M.A. The Practice of Sport in Multiple Sclerosis: Update. Curr. Sport. Med. Rep. 2017, 16, 274–279. [Google Scholar] [CrossRef] [PubMed]
- Hoang, P.D.; Gandevia, S.C.; Herbert, R.D. Prevalence of joint contractures and muscle weakness in people with multiple sclerosis. Disabil. Rehabil. 2014, 36, 1588–1593. [Google Scholar] [CrossRef] [PubMed]
- Wagner, J.M.; Kremer, T.R.; Van Dillen, L.R.; Naismith, R.T. Plantarflexor weakness negatively impacts walking in persons with multiple sclerosis more than plantarflexor spasticity. Arch. Phys. Med. Rehabil. 2014, 95, 1358–1365. [Google Scholar] [CrossRef] [PubMed]
- Lim, C.; Kim, H.J.; Morton, R.W.; Harris, R.; Phillips, S.M.; Jeong, T.S.; Kim, C.K. Resistance exercise-induced changes in muscle phenotype are load dependent. Med. Sci. Sport. Exerc. 2019, 51, 2578–2585. [Google Scholar] [CrossRef] [PubMed]
- Fragala, M.S.; Cadore, E.L.; Dorgo, S.; Izquierdo, M.; Kraemer, W.J.; Peterson, M.D.; Ryan, E.D. Resistance training for older adults: Position statement from the national strength and conditioning association. J. Strength Cond. Res. 2019, 33, 2019–2052. [Google Scholar] [CrossRef]
- Lopez, P.; Radaelli, R.; Taaffe, D.R.; Newton, R.U.; Galvão, D.A.; Trajano, G.S.; Teodoro, J.L.; Kraemer, W.J.; Häkkinen, K.; Pinto, R.S. Resistance Training Load Effects on Muscle Hypertrophy and Strength Gain: Systematic Review and Network Meta-analysis. Med. Sci. Sport. Exerc. 2021, 53, 1206–1216. [Google Scholar] [CrossRef]
- Zhang, Y.; Taylor, B.V.; Simpson, S.; Blizzard, L.; Campbell, J.A.; Palmer, A.J.; van der Mei, I. Feelings of depression, pain and walking difficulties have the largest impact on the quality of life of people with multiple sclerosis, irrespective of clinical phenotype. Mult. Scler. J. 2021, 27, 1262–1275. [Google Scholar] [CrossRef]
- Cameron, M.H.; Nilsagard, Y. Balance, gait, and falls in multiple sclerosis. Handb. Clin. Neurol. 2018, 159, 237–250. [Google Scholar] [PubMed]
- Shamsi, M.; Sarrafzadeh, J.; Jamshidi, A.; Arjmand, N.; Ghezelbash, F. Comparison of spinal stability following motor control and general exercises in nonspecific chronic low back pain patients. Clin. Biomech. 2017, 48, 42–48. [Google Scholar] [CrossRef]
- Malfliet, A.; Kregel, J.; Coppieters, I.; De Pauw, R.; Meeus, M.; Roussel, N.; Cagnie, B.; Danneels, L.; Nijs, J. Effect of pain neuroscience education combined with cognition-targeted motor control training on chronic spinal pain a randomized clinical trial. JAMA Neurol. 2018, 75, 808–817. [Google Scholar] [CrossRef] [PubMed]
- DeBolt, L.S.; McCubbin, J.A. The Effects of Home-Based Resistance Exercise on Balance, Power, and Mobility in Adults with Multiple Sclerosis. Arch. Phys. Med. Rehabil. 2004, 85, 290–297. [Google Scholar] [CrossRef]
- Marck, C.H.; De Livera, A.M.; Weiland, T.J.; Jelinek, P.L.; Neate, S.L.; Brown, C.R.; Taylor, K.L.; Khan, F.; Jelinek, G.A. Pain in people with multiple sclerosis: Associations with modifiable lifestyle factors, fatigue, depression, anxiety, and mental health quality of life. Front. Neurol. 2017, 8, 461. [Google Scholar] [CrossRef]
- Grazioli, E.; Tranchita, E.; Borriello, G.; Cerulli, C.; Minganti, C.; Parisi, A. The Effects of Concurrent Resistance and Aerobic Exercise Training on Functional Status in Patients with Multiple Sclerosis. Curr. Sport. Med. Rep. 2019, 18, 452–457. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.; Lai, B.; Mehta, T.; Thirumalai, M.; Padalabalanarayanan, S.; Rimmer, J.H.; Motl, R.W. Exercise Training Guidelines for Multiple Sclerosis, Stroke, and Parkinson Disease: Rapid Review and Synthesis. Am. J. Phys. Med. Rehabil. 2019, 98, 613–621. [Google Scholar] [CrossRef]
- Mardaniyan-Ghahfarrokhi, M.; Banitalebi, E.; Faramarzi, M.; Motl, R. Feasibility and efficacy of home-based neurofunctional exercise vs. resistance exercise programs for ambulatory disability of multiple sclerosis patients with cognitive impairment. Mult. Scler. Relat. Disord. 2022, 58, 103400. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Higgins, J.P. Cochrane Handbook for Systematic Reviews of Interventions; Version 5.1.0 [Updated March 2011]; The Cochrane Collaboration: London, UK, 2011. [Google Scholar]
- Cashin, A.G.; McAuley, J.H. Clinimetrics: Physiotherapy Evidence Database (PEDro) Scale. J. Physiother. 2020, 66, 59. [Google Scholar] [CrossRef]
- De Morton, N.A. The PEDro scale is a valid measure of the methodological quality of clinical trials: A demographic study. Aust. J. Physiother. 2009, 55, 129–133. [Google Scholar] [CrossRef]
- Akbar, N.; Sandroff, B.M.; Wylie, G.R.; Strober, L.B.; Smith, A.; Goverover, Y.; Motl, R.W.; DeLuca, J.; Genova, H. Progressive resistance exercise training and changes in resting-state functional connectivity of the caudate in persons with multiple sclerosis and severe fatigue: A proof-of-concept study. Neuropsychol. Rehabil. 2020, 30, 54–66. [Google Scholar] [CrossRef]
- Arntzen, E.C.; Straume, B.; Odeh, F.; Feys, P.; Normann, B. Group-based, individualized, comprehensive core stability and balance intervention provides immediate and long-term improvements in walking in individuals with multiple sclerosis: A randomized controlled trial. Physiother. Res. Int. 2020, 25, e1798. [Google Scholar] [CrossRef]
- Sandroff, B.M.; Bollaert, R.E.; Pilutti, L.A.; Peterson, M.L.; Baynard, T.; Fernhall, B.; McAuley, E.; Motl, R.W. Multimodal exercise training in multiple sclerosis: A randomized controlled trial in persons with substantial mobility disability. Contemp. Clin. Trials 2017, 61, 39–47. [Google Scholar] [CrossRef]
- Sosnoff, J.J.; Finlayson, M.; McAuley, E.; Morrison, S.; Motl, R.W. Home-based exercise program and fall-risk reduction in older adults with multiple sclerosis: Phase 1 randomized controlled trial. Clin. Rehabil. 2014, 28, 254–263. [Google Scholar] [CrossRef] [PubMed]
- Callesen, J.; Cattaneo, D.; Brincks, J.; Kjeldgaard-Jørgensen, M.L.; Dalgas, U. How do resistance training and balance and motor control training affect gait performance and fatigue impact in people with multiple sclerosis? A randomized controlled multi-center study. Mult. Scler. J. 2020, 26, 1420–1432. [Google Scholar] [CrossRef] [PubMed]
- Correale, L.; Buzzachera, C.F.; Liberali, G.; Codrons, E.; Mallucci, G.; Vandoni, M.; Montomoli, C.; Bergamaschi, R. Effects of Combined Endurance and Resistance Training in Women With Multiple Sclerosis: A Randomized Controlled Study. Front. Neurol. 2021, 12, 698460. [Google Scholar] [CrossRef] [PubMed]
- Uszynski, M.K.; Purtill, H.; Donnelly, A.; Coote, S. Comparing the effects of whole-body vibration to standard exercise in ambulatory people with Multiple Sclerosis: A randomised controlled feasibility study. Clin. Rehabil. 2016, 30, 657–668. [Google Scholar] [CrossRef] [PubMed]
- Learmonth, Y.C.; Adamson, B.C.; Kinnett-Hopkins, D.; Bohri, M.; Motl, R.W. Results of a feasibility randomised controlled study of the guidelines for exercise in multiple sclerosis project. Contemp. Clin. Trials 2017, 54, 84–97. [Google Scholar] [CrossRef]
- Manca, A.; Cabboi, M.P.; Dragone, D.; Ginatempo, F.; Ortu, E.; De Natale, E.R.; Mercante, B.; Mureddu, G.; Bua, G.; Deriu, F. Resistance Training for Muscle Weakness in Multiple Sclerosis: Direct Versus Contralateral Approach in Individuals With Ankle Dorsiflexors’ Disparity in Strength. Arch. Phys. Med. Rehabil. 2017, 98, 1348–1356. [Google Scholar] [CrossRef]
- Medina-Perez, C.; De Souza-Teixeira, F.; Fernandez-Gonzalo, R.; De Paz-Fernandez, J.A. Effects of a resistance training program and subsequent detraining on muscle strength and muscle power in multiple sclerosis patients. NeuroRehabilitation 2014, 34, 523–530. [Google Scholar] [CrossRef]
- Brændvik, S.M.; Koret, T.; Helbostad, J.L.; Lorås, H.; Bråthen, G.; Hovdal, H.O.; Aamot, I.L. Treadmill Training or Progressive Strength Training to Improve Walking in People with Multiple Sclerosis? A Randomized Parallel Group Trial. Physiother. Res. Int. 2016, 21, 228–236. [Google Scholar] [CrossRef]
- Pau, M.; Corona, F.; Coghe, G.; Marongiu, E.; Loi, A.; Crisafulli, A.; Concu, A.; Galli, M.; Marrosu, M.G.; Cocco, E. Quantitative assessment of the effects of 6 months of adapted physical activity on gait in people with multiple sclerosis: A randomized controlled trial. Disabil. Rehabil. 2018, 40, 144–151. [Google Scholar] [CrossRef]
- Savović, J.; Jones, H.; Altman, D.; Harris, R.; Jűni, P.; Pildal, J.; Als-Nielsen, B.; Balk, E.; Gluud, C.; Gluud, L.; et al. Influence of reported study design characteristics on intervention effect estimates from randomised controlled trials: Combined analysis of meta-epidemiological studies. Health Technol. Assess. 2012, 16, 1–82. [Google Scholar] [CrossRef]
- Cruickshank, T.M.; Reyes, A.R.; Ziman, M.R. A systematic review and meta-analysis of strength training in individuals with multiple sclerosis or parkinson disease. Medicine 2015, 94, e411. [Google Scholar] [CrossRef] [PubMed]
- Kjølhede, T.; Vissing, K.; Dalgas, U. Multiple sclerosis and progressive resistance training: A systematic review. Mult. Scler. J. 2012, 18, 1215–1228. [Google Scholar] [CrossRef] [PubMed]
- Flensner, G.; Ek, A.C.; Landtblom, A.M.; Söderhamn, O. Fatigue in relation to perceived health: People with multiple sclerosis compared with people in the general population. Scand. J. Caring Sci. 2008, 22, 391–400. [Google Scholar] [CrossRef]
- Bird, S.P.; Tarpenning, K.M.; Marino, F.E. Designing resistance training programmes to enhance muscular fitness: A review of the acute programme variables. Sport. Med. 2005, 35, 841–851. [Google Scholar] [CrossRef] [PubMed]
- Andreasen, A.K.; Stenager, E.; Dalgas, U. The effect of exercise therapy on fatigue in multiple sclerosis. Mult. Scler. J. 2011, 17, 1041–1054. [Google Scholar] [CrossRef] [PubMed]
- Dalgas, U.; Stenager, E.; Jakobsen, J.; Petersen, T.; Hansen, H.J.; Knudsen, C.; Overgaard, K.; Ingemann-Hansen, T. Resistance training improves muscle strength and functional capacity in multiple sclerosis. Neurology 2009, 73, 1478–1484. [Google Scholar] [CrossRef] [PubMed]
- Claerbout, M.; Gebara, B.; Ilsbroukx, S.; Verschueren, S.; Peers, K.; Van Asch, P.; Feys, P. Effects of 3 weeks’ whole body vibration training on muscle strength and functional mobility in hospitalized persons with multiple sclerosis. Mult. Scler. J. 2012, 18, 498–505. [Google Scholar] [CrossRef] [PubMed]
- Eftekhari, E.; Mostahfezian, M.; Etemadifar, M.; Zafari, A. Resistance training and vibration improve muscle strength and functional capacity in female patients with multiple sclerosis. Asian J. Sport. Med. 2012, 3, 279–284. [Google Scholar] [CrossRef] [PubMed]
- Yeh, S.W.; Lin, L.F.; Tam, K.W.; Tsai, C.P.; Hong, C.H.; Kuan, Y.C. Efficacy of robot-assisted gait training in multiple sclerosis: A systematic review and meta-analysis. Mult. Scler. Relat. Disord. 2020, 41, 102034. [Google Scholar] [CrossRef] [PubMed]
- Kjølhede, T.; Vissing, K.; De Place, L.; Pedersen, B.G.; Ringgaard, S.; Stenager, E.; Petersen, T.; Dalgas, U. Neuromuscular adaptations to long-term progressive resistance training translates to improved functional capacity for people with multiple sclerosis and is maintained at follow-up. Mult. Scler. J. 2015, 21, 599–611. [Google Scholar] [CrossRef]
- Callesen, J.; Dalgas, U.; Brincks, J.; Cattaneo, D. How much does balance and muscle strength impact walking in persons with multiple sclerosis?-A cross-sectional study. Mult.Scler. Relat. Disord. 2019, 29, 137–144. [Google Scholar] [CrossRef]
- Wezenberg, D.; De Haan, A.; Van Bennekom, C.A.M.; Houdijk, H. Mind your step: Metabolic energy cost while walking an enforced gait pattern. Gait Posture 2011, 33, 544–549. [Google Scholar] [CrossRef]
- Gomez-Illan, R.; Reina, R.; Barbado, D.; Sabido, R.; Moreno-Navarro, P.; Roldan, A. Effects of Maximal Strength Training on Perceived-Fatigue and Functional Mobility in Persons with Relapsing-Remitting Multiple Sclerosis. Medicina 2020, 56, 718. [Google Scholar] [CrossRef]
- Hebert, J.R.; Corboy, J.R.; Vollmer, T.; Forster, J.E.; Schenkman, M. Efficacy of Balance and Eye-Movement Exercises for Persons With Multiple Sclerosis (BEEMS). Neurology 2018, 90, 797–807. [Google Scholar] [CrossRef] [PubMed]
- Gutierrez, G.M.; Chow, J.W.; Tillman, M.D.; McCoy, S.C.; Castellano, V.; White, L.J. Resistance training improves gait kinematics in persons with multiple sclerosis. Arch. Phys. Med. Rehabil. 2005, 86, 1824–1829. [Google Scholar] [CrossRef]
- Pilutti, L.A.; Lelli, D.A.; Paulseth, J.E.; Crome, M.; Jiang, S.; Rathbone, M.P.; Hicks, A.L. Effects of 12 weeks of supported treadmill training on functional ability and quality of life in progressive multiple sclerosis: A pilot study. Arch. Phys. Med. Rehabil. 2011, 92, 31–36. [Google Scholar] [CrossRef] [PubMed]
- Kwok, J.Y.Y.; Kwan, J.C.Y.; Auyeung, M.; Mok, V.C.T.; Lau, C.K.Y.; Choi, K.C.; Chan, H.Y. Effects of Mindfulness Yoga vs Stretching and Resistance Training Exercises on Anxiety and Depression for People with Parkinson Disease: A Randomized Clinical Trial. JAMA Neurol. 2019, 76, 755–763. [Google Scholar] [CrossRef] [PubMed]
- Rahmati, M.; Malakoutinia, F. Aerobic, resistance and combined exercise training for patients with amyotrophic lateral sclerosis: A systematic review and meta-analysis. Physiotherapy 2021, 113, 12–28. [Google Scholar] [CrossRef] [PubMed]
- Lamberti, N.; Straudi, S.; Malagoni, A.M.; Argirò, M.; Felisatti, M.; Nardini, E.; Zambon, C.; Basaglia, N.; Manfredini, F. Effects of low-intensity endurance and resistance training on mobility in chronic stroke survivors: A pilot randomized controlled study. Eur. J. Phys. Rehabil. Med. 2017, 53, 228–239. [Google Scholar] [CrossRef]
- Keytsman, C.; Van Noten, P.; Verboven, K.; Van Asch, P.; Eijnde, B.O. Periodized versus classic exercise therapy in Multiple Sclerosis: A randomized controlled trial. Mult. Scler. Relat. Disord. 2021, 49, 102782. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| 1* | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | Total Score | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Akbar et al. [35] | Y | Y | N | Y | N | N | N | Y | Y | Y | Y | 5 |
| Arntzen et al. [36] | Y | Y | Y | Y | N | N | Y | Y | N | Y | Y | 7 |
| Sandroff et al. [37] | Y | Y | N | Y | N | N | N | N | Y | Y | Y | 5 |
| Sosnoff et al. [38] | Y | Y | Y | Y | N | N | Y | N | N | Y | Y | 6 |
| Callesen et al. [39] | Y | Y | Y | Y | N | N | Y | Y | N | Y | Y | 7 |
| Correale et al. [40] | N | Y | N | Y | N | N | Y | Y | N | Y | Y | 6 |
| Uszynski et al. [41] | Y | Y | Y | Y | N | N | Y | Y | N | Y | Y | 7 |
| Learmonth et al. [42] | Y | Y | Y | Y | N | N | N | Y | N | Y | Y | 6 |
| Manca et al. [43] | N | Y | Y | Y | N | N | Y | Y | N | Y | Y | 7 |
| Medina-Perez et al. [44] | Y | Y | N | Y | N | N | N | Y | N | Y | Y | 5 |
| Braendvik et al. [45] | Y | Y | N | Y | N | N | N | Y | Y | Y | Y | 6 |
| Pau et al. [46] | Y | Y | N | Y | N | N | N | Y | Y | Y | Y | 6 |
| Author and Year | Sex | Sample CG/IG | Control Group | Intervention Group | Results | ||||
|---|---|---|---|---|---|---|---|---|---|
| Disability Range of the Included Patients | Age Mean ± SD Median (IQR) | Treatment | Exercise Parameters | EDSS Score Pre-Intervention Mean ± SD Median (IQR) | |||||
| Akbar et al. [35] | F: 100% | 5/5 | Fully ambulatory/ability to walk without an assistive device | Stretching | 45.6 ± 12.8 | Progressive resistance training | I: Adjusted to each participant F: 3 times/week #S: 48 sessions D: 600 min | Not reported | Progressive resistance training improves fatigue (main effect of time: F = 0.84, d = 0.65), functional connectivity between the left inferior caudate and parietal (F = 66.0, p < 0.001), bilateral frontal (both p < 0.001), and right insula (F = 21.8, p = 0.002) regions and grip strength (d = 1.11). |
| Arntzen et al. [36] | F: 69.2% M: 30.8% | 40/39 | EDSS 1–6.5; mean = 2.37 | Usual care + walking | 52.2 ± 12.9 | Dynamic core stability training | I: Adjusted to each participant F: 3 times/week #S: 18 sessions D: 60 min | 2.45 ± 1.65 | Dynamic core stability training significantly improved walking (2MWT) immediately after the intervention for up to 24 weeks of follow-up (Post: 6.7 m, 95% CI [8.15, 25.25], p < 0.001; Follow-Up: 15.08 m, 95% CI [6.39, 23.77] p = 0.001). |
| Sandroff et al. [37] | F: 85.5% M: 14.5% | 40/43 | EDSS 4–6; PDDS mean = 3.5 | Stretching and toning activities | 49.8 ± 8.5 | Aerobic, resistance, and balance exercise | I: Vigorous F: 3 times/week #S: 18 sessions D: 25 min | Not reported | This RCT provides novel, preliminary evidence that multimodal exercise training may improve endurance walking (r = 0.25) performance and cognitive processing speed. |
| Sosnoff et al. [38] | F: 77.7% M: 22.3% | 14/13 | EDSS 2.5–6.5; mean = 5 | Waiting list | 60.0 ± 6.1 | Balance, walking and resistance training | I: Adjusted to each participant F: 3 times/week #S: 38 sessions D: 45–60 min | 5.5 ± 2.5 | A home-based exercise program enhanced walking (T25FW, Pre: 6.6 ± 1.3; Post: 6.4 ± 1.4; p = 0.040). |
| Callesen et al. [39] | M: 23% F: 77% | 20/23 | EDDS 2.0–6.5; mean = 3.5 | Usual care | 52 (30–75) | Progressive resistance training | I: Moderate F: 2 times/week #S: 21 sessions D: 60 min | 4 (2–6.5) | Progressive resistance training reduced fatigue impact, however, had no impact on gait when compared to control group (Mean diff: 0.02; 95% CI [−0.08; 0.13], p = 0.660) |
| Correale et al. [40] | F: 100% | 9/14 | Mean EDSS = 2.25 | Usual care | 45.4 ±7.2 | Endurance and resistance training | I: Moderate to Vigorous F: 2 times/week #S: 24 sessions D: 30 min | Not reported | Endurance and resistance training leads to enhanced muscle strength, along with decreased fatigue, depressive symptoms, and greater overall health-related quality of life (p < 0.05). Notably, these positive changes endure even after a 12-week period of detraining. |
| Uszynski et al. [41] | M: 28.57% F: 71.43% | 13/14 | Participants with MS who walked independently or used an assistive device with scores of 0, 1, 2, and 3, inclusive on the Guys Neurological Disability scale (GNDS). | Resistance training | 45.5 (38.5–52.3) | Vibration + resistance training | I: Moderate to Vigorous F: 3 times/week #S: 36 sessions D: 20 min | Not reported | No between group differences were found for muscle strength, balance, or gait (p > 0.05). |
| Learmonth et al. [42] | F: 96.55% M: 3.45% | 28/29 | EDSS 1–6; mean = 1.5 | Waitlist | 48.4 ± 9.7 | Resistance and aerobic training | I: Mild to moderate F: 4 times/week #S: 64 sessions D: 45 min | 1.25 ± 2.5 | A small, non-statistically significant effect size of combined exercise on MSWS-12 in patients with MS is presented. (Cohen’s D: −0.10, F: 0.47) |
| Manca et al. [43] | F: 80% M: 20% | 15/15 | EDDS ≤ 6; mean = 3.4 | Contralateral resistance training | 47.3 ± 9.4 | Direct resistance training | I: Vigorous F: 3 times/week #S: 18 sessions D: 25 min | 3.0 ± 1.00 | Both direct and indirect resistance training led to significant gains in muscle strength. However, only direct resistance training increased walking speed (Pre: 085 ± 0.14; Post: 0.99 ± 0.15; p < 0.0001) |
| Medina-Perez et al. [44] | NR | 12/30 | Mean EDSS = 4.3 | Usual care | 49.6 ± 11 | Resistance training | I: Vigorous F: 3 times/week #S: 18 sessions D: 25 min | 4.5 ± 2.1 | A 12-week RTP improved extension, maximal voluntary isometric contraction, and muscle power in MS patients. |
| Braendvik et al. [45] | M: 34.6% F: 65.4% | 11/15 | EDSS ≤ 6; mean = 3.15 | Treadmill training | 49.1 ± 6.2 | Resistance training | I: Moderate to Vigorous F: 3 times/week #S: 24 sessions D: 30 min | 3.2 ± 1.4 | Resistance training had no significant effect over gait assessed with the Functional Ambulation Profile (Pre: 91.7, Post: 90.3; p = 0.844) |
| Pau et al. [46] | M: 54.54% F: 45.45% | 11/11 | EDSS 1.5–5.5; mean = 3.5 | Usual care | 47.4 ± 10.8 | Aerobic and resistance training | I: Moderate F: 3 times/week #S: 72 sessions D: 60 min | 3.6 ± 0.9 | Although some improvements have been observed, the substantial constancy of kinematic patterns of gait suggests that the full transferability of the administered training on the ambulation function may require more specific exercises. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cano-Sánchez, J.; Aibar-Almazán, A.; Hita-Contreras, F.; Afanador-Restrepo, D.F.; Martínez-Amat, A.; Achalandabaso-Ochoa, A.; Carcelén-Fraile, M.d.C. Is Resistance Training an Option to Improve Functionality and Muscle Strength in Middle-Aged People with Multiple Sclerosis? A Systematic Review and Meta-Analysis. J. Clin. Med. 2024, 13, 1378. https://doi.org/10.3390/jcm13051378
Cano-Sánchez J, Aibar-Almazán A, Hita-Contreras F, Afanador-Restrepo DF, Martínez-Amat A, Achalandabaso-Ochoa A, Carcelén-Fraile MdC. Is Resistance Training an Option to Improve Functionality and Muscle Strength in Middle-Aged People with Multiple Sclerosis? A Systematic Review and Meta-Analysis. Journal of Clinical Medicine. 2024; 13(5):1378. https://doi.org/10.3390/jcm13051378
Chicago/Turabian StyleCano-Sánchez, Javier, Agustín Aibar-Almazán, Fidel Hita-Contreras, Diego Fernando Afanador-Restrepo, Antonio Martínez-Amat, Alexander Achalandabaso-Ochoa, and María del Carmen Carcelén-Fraile. 2024. "Is Resistance Training an Option to Improve Functionality and Muscle Strength in Middle-Aged People with Multiple Sclerosis? A Systematic Review and Meta-Analysis" Journal of Clinical Medicine 13, no. 5: 1378. https://doi.org/10.3390/jcm13051378
APA StyleCano-Sánchez, J., Aibar-Almazán, A., Hita-Contreras, F., Afanador-Restrepo, D. F., Martínez-Amat, A., Achalandabaso-Ochoa, A., & Carcelén-Fraile, M. d. C. (2024). Is Resistance Training an Option to Improve Functionality and Muscle Strength in Middle-Aged People with Multiple Sclerosis? A Systematic Review and Meta-Analysis. Journal of Clinical Medicine, 13(5), 1378. https://doi.org/10.3390/jcm13051378