

Infective Endocarditis in Belgium: Prospective Data in Adults from the ESC EORP European Endocarditis Registry
 , ,
, ,  , , , ,
, , , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Data Collection
2.2. Data Management and Statistical Analysis
3. Results
3.1. Patient Demographics and Characteristics
3.2. Clinical and Biological Features
3.3. Imaging
3.4. In-Hospital Complications under Treatment
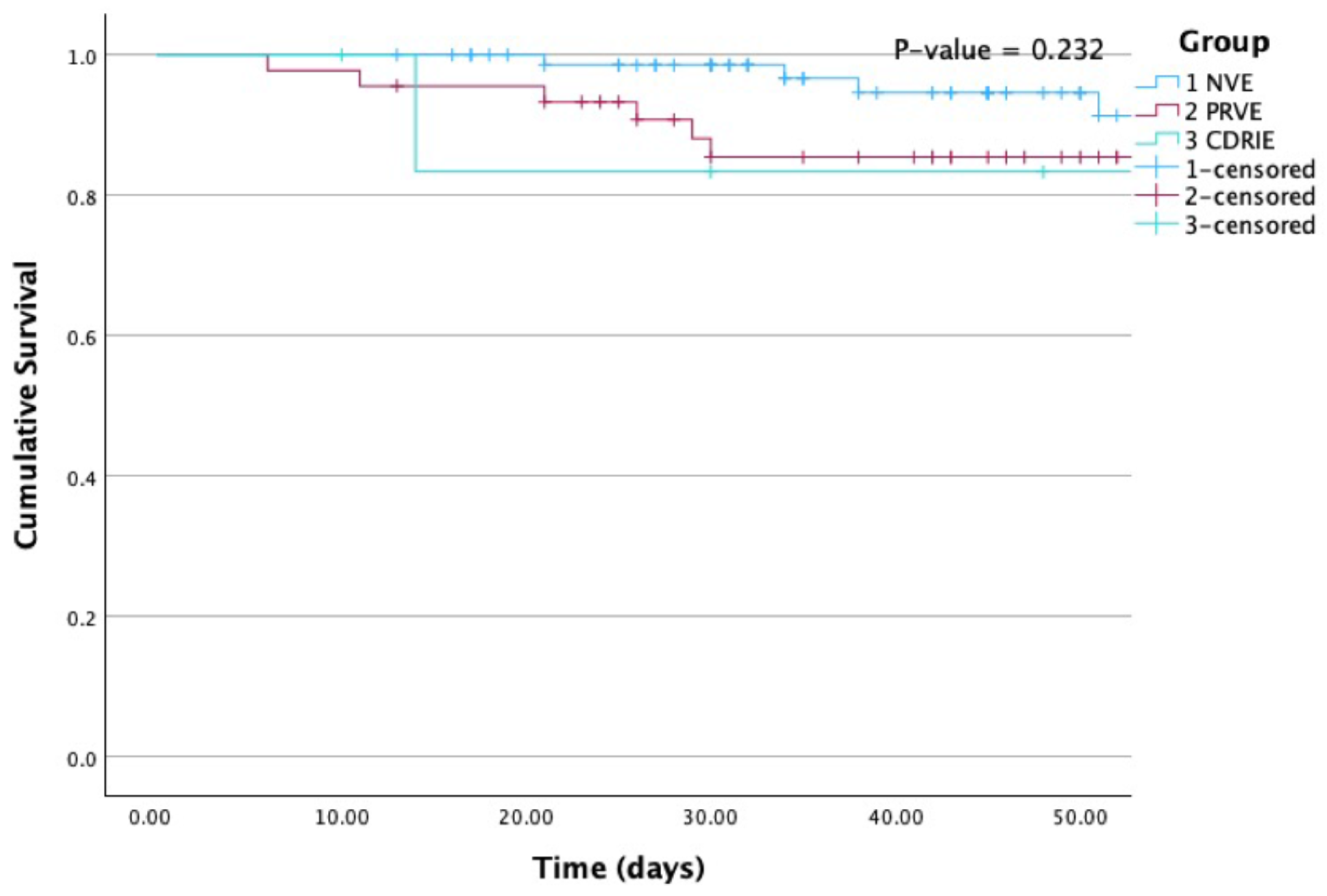
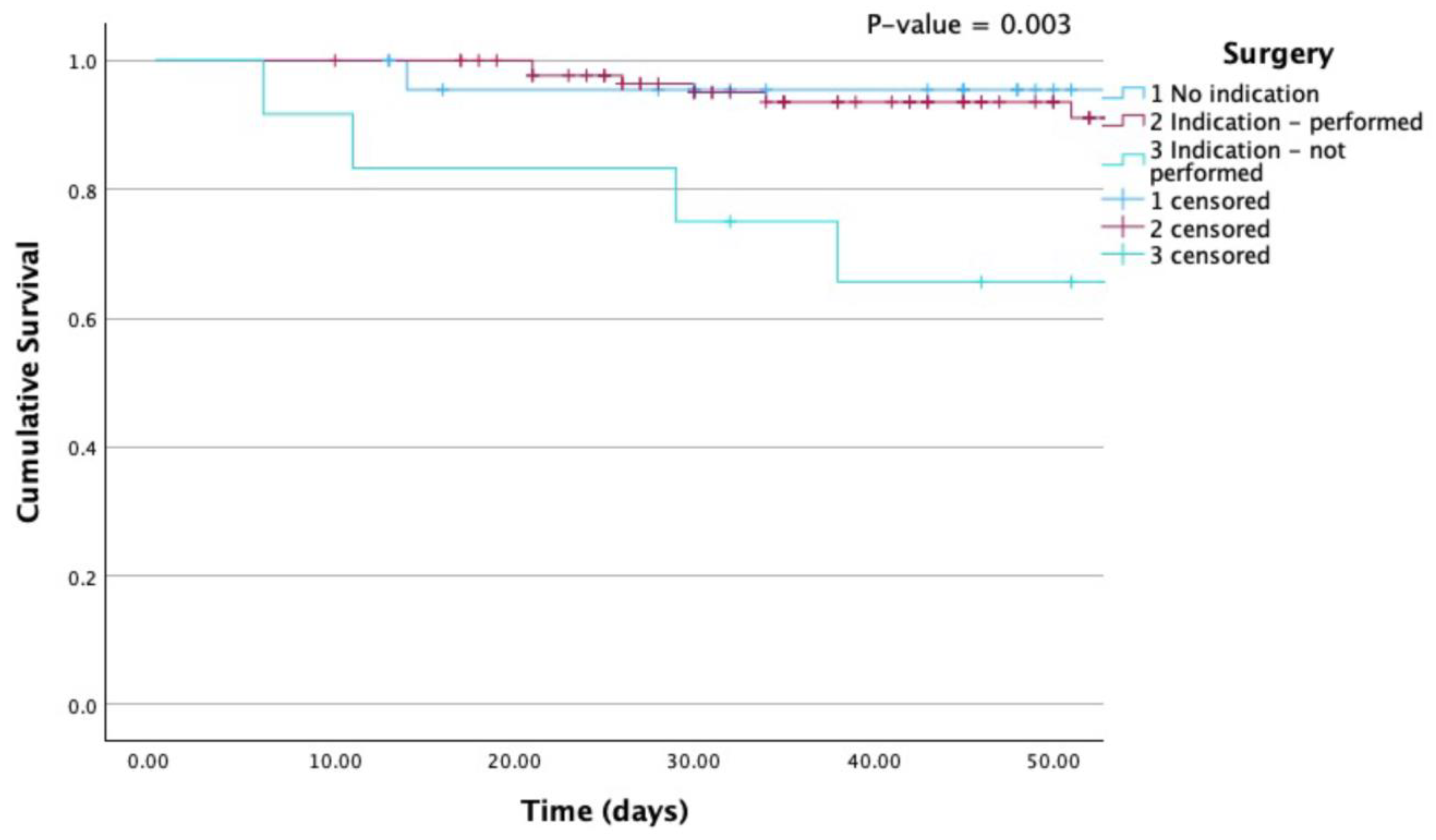
3.5. Cardiac Surgery and Mortality
4. Discussion
4.1. Demographics, Clinical and Microbiological Characteristics
4.2. Imaging
4.3. Management and Outcome of IE in Belgium
4.3.1. In-Hospital Complications
4.3.2. Surgery
4.3.3. In-Hospital Mortality
4.4. Study Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Habib, G. Management of Infective Endocarditis. Heart 2006, 92, 124–130. [Google Scholar] [CrossRef]
- Delgado, V.; Ajmone Marsan, N.; De Waha, S.; Bonaros, N.; Brida, M.; Burri, H.; Caselli, S.; Doenst, T.; Ederhy, S.; Erba, P.A.; et al. 2023 ESC Guidelines for the Management of Endocarditis. Eur. Heart J. 2023, 44, 3948–4042. [Google Scholar] [CrossRef] [PubMed]
- Momtazmanesh, S.; Moghaddam, S.S.; Rad, E.M.; Azadnajafabad, S.; Ebrahimi, N.; Mohammadi, E.; Rouhifard, M.; Rezaei, N.; Masinaei, M.; Rezaei, N.; et al. Global, Regional, and National Burden and Quality of Care Index of Endocarditis: The Global Burden of Disease Study 1990–2019. Eur. J. Prev. Cardiol. 2022, 29, 1287–1297. [Google Scholar] [CrossRef] [PubMed]
- Habib, G.; Lancellotti, P.; Antunes, M.J.; Bongiorni, M.G.; Casalta, J.P.; Del Zotti, F.; Dulgheru, R.; El Khoury, G.; Erba, P.A.; Iung, B.; et al. 2015 ESC Guidelines for the Management of Infective Endocarditis. Eur. Heart J. 2015, 36, 3075–3123. [Google Scholar] [CrossRef]
- Motoc, A.; Kessels, J.; Roosens, B.; Lacor, P.; Van de Veire, N.; De Sutter, J.; Magne, J.; Droogmans, S.; Cosyns, B. Impact of the Initial Clinical Presentation on the Outcome of Patients with Infective Endocarditis. Cardiol. J. 2023, 30, 385–390. [Google Scholar] [CrossRef] [PubMed]
- Poesen, K.; Pottel, H.; Colaert, J.; De Niel, C. Epidemiology of Infective Endocarditis in a Large Belgian Non-Referral Hospital. Acta Clin. Belg. 2014, 69, 183–190. [Google Scholar] [CrossRef]
- Yombi, J.C.; Yuma, S.N.; Pasquet, A.; Astarci, P.; Robert, A.; Rodriguez, H.V. Staphylococcal versus Streptococcal Infective Endocarditis in a Tertiary Hospital in Belgium: Epidemiology, Clinical Characteristics and Outcome. Acta Clin. Belgica Int. J. Clin. Lab. Med. 2017, 72, 417–423. [Google Scholar] [CrossRef] [PubMed]
- Tahon, J.; Geselle, P.J.; Vandenberk, B.; Hill, E.E.; Peetermans, W.E.; Herijgers, P.; Janssens, S.; Herregods, M.C. Long-Term Follow-up of Patients with Infective Endocarditis in a Tertiary Referral Center. Int. J. Cardiol. 2021, 331, 176–182. [Google Scholar] [CrossRef]
- Habib, G.; Lancellotti, P.; Erba, P.A.; Sadeghpour, A.; Meshaal, M.; Sambola, A.; Furnaz, S.; Citro, R.; Ternacle, J.; Donal, E.; et al. The ESC-EORP EURO-ENDO (European Infective Endocarditis) Registry. Eur. Heart J. Qual. Care Clin. Outcomes 2019, 5, 202–207. [Google Scholar] [CrossRef]
- Habib, G.; Erba, P.A.; Iung, B.; Donal, E.; Cosyns, B.; Laroche, C.; Popescu, B.A.; Prendergast, B.; Tornos, P.; Sadeghpour, A.; et al. Clinical Presentation, Aetiology and Outcome of Infective Endocarditis. Results of the ESC-EORP EURO-ENDO (European Infective Endocarditis) Registry: A Prospective Cohort Study. Eur. Heart J. 2019, 40, 3222–3232B. [Google Scholar] [CrossRef]
- Arora, N.; Panda, P.K.; CR, P.; Uppal, L.; Saroch, A.; Angrup, A.; Sharma, N.; Sharma, Y.P.; Vijayvergiya, R.; Rohit, M.K.; et al. Changing Spectrum of Infective Endocarditis in India: An 11-Year Experience from an Academic Hospital in North India. Indian Heart J. 2021, 73, 711–717. [Google Scholar] [CrossRef]
- Liaqat, W.; Palaiodimos, L.; Li, W.; Karamanis, D.; Tahir, A.; Tzoumas, A.; Nagraj, S.; Tiwari, N.; Grushko, M.; Kokkinidis, D.; et al. Epidemiologic and Clinical Characteristics of Infective Endocarditis: A Single-Center Retrospective Study in the Bronx, New York. Infection 2022, 50, 1349–1361. [Google Scholar] [CrossRef] [PubMed]
- Solari, S.; Tamer, S.; Aphram, G.; Mastrobuoni, S.; Navarra, E.; Noirhomme, P.; Poncelet, A.; Astarci, P.; Rubay, J.; El Khoury, G.; et al. Aortic Valve Repair in Endocarditis: Scope and Results. Indian J. Thorac. Cardiovasc. Surg. 2020, 36, 104–112. [Google Scholar] [CrossRef]
- Hoen, B.; Alla, F.; Selton-Suty, C.; Béguinot, I.; Bouvet, A.; Briançon, S.; Casalta, J.P.; Danchin, N.; Delahaye, F.; Etienne, J.; et al. Changing Profile of Infective Endocarditis: Results of a 1-Year Survey in France. JAMA 2002, 288, 75–81. [Google Scholar] [CrossRef] [PubMed]
- Murdoch, D.R.; Corey, R.G.; Hoen, B.; Miró, M.; Fowler, V.G.; Bayer, A.S.; Karchmer, A.W.; Olaison, L.; Pappas, P.A.; Moreillon, P.; et al. Clinical Presentation, Etiology, and Outcome of Infective Endocarditis in the 21st Century the International Collaboration on Endocarditis-Prospective Cohort Study. Arch. Intern. Med. 2009, 169, 463–473. [Google Scholar] [CrossRef]
- Cosyns, B.; Roosens, B.; Lancellotti, P.; Laroche, C.; Dulgheru, R.; Scheggi, V.; Vilacosta, I.; Pasquet, A.; Piper, C.; Reyes, G.; et al. Cancer and Infective Endocarditis: Characteristics and Prognostic Impact. Front. Cardiovasc. Med. 2022, 8, 766996. [Google Scholar] [CrossRef]
- von Kemp, B. Belgian Guidelines on Supportive Care: Cardiotoxicity of Cancer Treatments. Belgian J. Med. Oncol. 2021, 15, 367–373. [Google Scholar]
- Kong, W.K.F.; Salsano, A.; Giacobbe, D.R.; Popescu, B.A.; Laroche, C.; Duval, X.; Schueler, R.; Moreo, A.; Colonna, P.; Piper, C.; et al. Outcomes of Culture-Negative vs. Culture-Positive Infective Endocarditis: The ESC-EORP EURO-ENDO Registry. Eur. Heart J. 2022, 43, 2770–2780. [Google Scholar] [CrossRef]
- Sambola, A.; Lozano-Torres, J.; Boersma, E.; Olmos, C.; Ternacle, J.; Calvo, F.; Tribouilloy, C.; Reskovic-Luksic, V.; Separovic-Hanzevacki, J.; Park, S.-W.; et al. Predictors of Embolism and Death in Left-Sided Infective Endocarditis: The European Society of Cardiology EURObservational Research Programme European Infective Endocarditis Registry. Eur. Heart J. 2023, 44, 4566–4575. [Google Scholar] [CrossRef]
- Kim, K.; Kim, D.; Lee, S.E.; Cho, I.J.; Shim, C.Y.; Hong, G.R.; Ha, J.W. Infective Endocarditis in Cancer Patients: Causative Organisms, Predisposing Procedures, and Prognosis Differ from Infective Endocarditis in Non-Cancer Patients. Circ. J. 2019, 83, 452–460. [Google Scholar] [CrossRef]
- Oliver, L.; Lavoute, C.; Giorgi, R.; Salaun, E.; Hubert, S.; Casalta, J.P.; Gouriet, F.; Renard, S.; Saby, L.; Avierinos, J.F.; et al. Infective Endocarditis in Octogenarians. Heart 2017, 103, 1602–1609. [Google Scholar] [CrossRef] [PubMed]
- Fernández-Cruz, A.; Muñoz, P.; Sandoval, C.; Fariñas-Álvarez, M.C.; Gutiérrez-Cuadra, M.; Pericás Pulido, J.M.; Miró, J.M.; Goenaga-Sánchez, M.; De Alarcón, A.; Bonache-Bernal, F.; et al. Infective Endocarditis in Patients with Cancer: A Consequence of Invasive Procedures or a Harbinger of Neoplasm? A Prospective, Multicenter Cohort. Medicine 2017, 96, e7913. [Google Scholar] [CrossRef] [PubMed]
- Habib, G.; Badano, L.; Tribouilloy, C.; Vilacosta, I.; Zamorano, J.L.; Galderisi, M.; Voigt, J.U.; Sicari, R.; Cosyns, B.; Fox, K.; et al. Recommendations for the Practice of Echocardiography in Infective Endocarditis. Eur. J. Echocardiogr. 2010, 11, 202–219. [Google Scholar] [CrossRef] [PubMed]
- El Kadi, S.; van den Buijs, D.M.F.; Meijers, T.; Gilbers, M.D.; Bekkers, S.C.A.M.; van Melle, J.P.; Riezebos, R.K.; Blok, W.L.; Tanis, W.; Wahadat, A.R.; et al. Infective Endocarditis in the Netherlands: Current Epidemiological Profile and Mortality: An Analysis Based on Partial ESC EORP Collected Data. Netherlands Heart J. 2020, 28, 526–536. [Google Scholar] [CrossRef]
- Iung, B.; Baron, G.; Butchart, E.G.; Delahaye, F.; Gohlke-Bärwolf, C.; Levang, O.W.; Tornos, P.; Vanoverschelde, J.L.; Vermeer, F.; Boersma, E.; et al. A Prospective Survey of Patients with Valvular Heart Disease in Europe: The Euro Heart Survey on Valvular Heart Disease. Eur. Heart J. 2003, 24, 1231–1243. [Google Scholar] [CrossRef]
- Tornos, P.; Iung, B.; Permanyer-Miralda, G.; Baron, G.; Delahaye, F.; Gohlke-Bärwolf, C.; Butchart, E.G.; Ravaud, P.; Vahanian, A. Infective Endocarditis in Europe: Lessons from the Euro Heart Survey. Heart 2005, 91, 571–575. [Google Scholar] [CrossRef]
- Toyoda, N.; Itagaki, S.; Egorova, N.N.; Tannous, H.; Anyanwu, A.C.; El-Eshmawi, A.; Adams, D.H.; Chikwe, J. Real-World Outcomes of Surgery for Native Mitral Valve Endocarditis. J. Thorac. Cardiovasc. Surg. 2017, 154, 1906–1912.e9. [Google Scholar] [CrossRef]
- Charlson, M.; Szatrowski, T.P.; Peterson, J.; Gold, J. Validation of a Combined Comorbidity Index. J. Clin. Epidemiol. 1994, 47, 1245–1251. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Total | NVE | PRVE | CDRIE | p-Value | |
|---|---|---|---|---|---|
| N | 127 | 75 | 45 | 7 | |
| Demographics | |||||
| Age (years) | |||||
| Mean ± SD | 62.8 ± 14.9 | 60.6 ± 15.4 | 66.5 ± 14.0 | 63.6 ± 10.5 | 0.073 |
| <65 years old | 57/127 (44.9%) | 40/75 (53.3%) | 15/45 (33.3%) | 2/7 (28.6%) | |
| 65–80 years old | 56/127 (45.1%) | 29/75 (38.7%) | 22/45 (48.9%) | 5/7 (71.4%) | |
| ≥80 years old | 14/127 (11.0%) | 6/75 (8.0%) | 8/45 (17.8%) | 0/7 (0.0%) | |
| Males (%) | 92/127 (72.4%) | 53/75 (70.1%) | 33/45 (73.3%) | 6/7 (85.7%) | 0.801 |
| History of cardiovascular diseases | |||||
| Atrial fibrillation | 38/127 (29.9%) | 15/75 (20.0%) | 19/45 (42.2%) | 4/7 (57.1%) | 0.009 * |
| Known valve murmur | 26/127 (20.5%) | 12/75 (16.0%) | 14/45 (31.1%) | 0/7 (0.0%) | 0.073 |
| Ischemic heart disease | 25/127 (19.7%) | 6/75 (8%) | 15/45 (33.3%) | 4/7 (57.1%) | <0.001 * |
| Congenital heart disease | 19/127 (15.0%) | 10/75 (13.3%) | 9/45 (20.0%) | 0/7 (0.0%) | 0.409 |
| Heart failure | 15/127 (11.8%) | 5/75 (6.7%) | 6/45 (13.3%) | 4/7 (57.1%) | 0.003 * |
| Previous IE (%) | 7/127 (5.5%) | 1/75 (1.3%) | 5/45 (11.1%) | 1/7 (14.3%) | 0.024 * |
| Hypertrophic cardiomyopathy | 4/127 (3.1%) | 2/75 (2.7%) | 2/45 (4.4%) | 0/7 (0.0%) | 0.703 |
| Risk factors | |||||
| Arterial hypertension | 68/127 (53.5%) | 37/75 (49.3%) | 27/45 (60.0%) | 4/7 (57.1%) | 0.531 |
| Smoking | 34/127 (26.8%) | 25/75 (33.3%) | 7/45 (15.6%) | 2/7 (28.6%) | 0.107 |
| Cancer | 30/127 (23.6%) | 16/75 (21.3%) | 14/45 (31.1%) | 0/7 (0.0%) | 0.176 |
| COPD/asthma | 23/127 (18.1%) | 11/75 (14.7%) | 8/45 (17.8%) | 4/7 (57.1%) | 0.034 * |
| Chronic renal failure | 22/127 (17.3%) | 9/75 (12.0%) | 9/45 (20.0%) | 4/7 (57.1%) | 0.013 * |
| Dialysis | 4/22 (18.2%) | 3/9 (33.3%) | 0/9 (0.0%) | 1/4 (18.2%) | 0.202 |
| Previous stroke/TIA | 20/127 (15.7%) | 9/75 (12.0%) | 10/45 (22.2%) | 1/7 (14.3%) | 0.316 |
| Alcohol abuse | 15/127 (11.8%) | 10/75 (13.3%) | 4/45 (8.9%) | 1/7 (14.3%) | 0.798 |
| Hypo/hyperthyroidism | 14/127 (11.0%) | 9/75 (12.0%) | 3/45 (6.7%) | 2/7 (28.6%) | 0.192 |
| Long corticotherapy | 11/127 (8.7%) | 6/75 (8.0%) | 4/45 (8.9%) | 1/7 (14.3%) | 0.652 |
| Chronic autoimmune disease | 9/127 (7.1%) | 7/75 (9.3%) | 2/45 (4.4%) | 0/7 (0.0%) | 0.700 |
| Intravenous drug dependency | 8/127 (6.3%) | 8/75 (10.7%) | 0/45 (0.0%) | 0/7 (0.0%) | 0.059 |
| Intravenous catheter | 8/127 (6.3%) | 3/75 (4.0%) | 5/45 (11.1%) | 0/7 (0.0%) | 0.290 |
| Immunosuppressive treatment | 5/127 (3.9%) | 2/75 (2.7%) | 3/45 (6.7%) | 0/7 (0.0%) | 0.519 |
| Previous haemorrhagic events | 4/127 (3.1%) | 0/75 (0.0%) | 3/45 (6.7%) | 1/7 (14.3%) | 0.021 * |
| Previous Pulmonary embolism | 3/127 (2.4%) | 2/75 (2.7%) | 1/45 (2.2%) | 0/7 (0.0%) | 1.000 |
| HIV | 1/127 (0.8%) | 0/75 (0;0%) | 1/45 (2.2%) | 0/7 (0.0%) | 0.653 |
| Charlson index mean ± SD | 3.96 ± 3.04 | 3.39 ± 2.52 | 4.51 ± 3.50 | 6.14 ± 3.29 | 0.027 * |
| Antithrombotic treatment at admission | 76/127 (59.8%) | 32/75 (42.7%) | 38/45 (84.4%) | 6/7 (85.7%) | <0.001 * |
| Recent procedures | |||||
| Dental procedure | 9/127 (7.1%) | 7/75 (9.3%) | 2/45 (4.4%) | 0/7 (0.0%) | 0.696 |
| Colonoscopy | 7/127 (5.5%) | 4/75 (5.3%) | 2/45 (4.4%) | 1/7 (14.3%) | 0.505 |
| Urogenital intervention | 5/127 (3.9%) | 2/75 (2.7%) | 3/45 (6.7%) | 0/7 (0.0%) | 0.577 |
| Total | NVE | PRVE | CDRIE | p-Value | |
|---|---|---|---|---|---|
| N | 127 | 75 | 45 | 7 | |
| Death | 20/127 (15.7%) | 8/75 (10.7%) | 9/45 (20.0%) | 3/7 (42.9%) | 0.051 |
| Cause of death | |||||
| Cardiovascular | 3/20 (15%) | 0/8 (0.0%) | 3/9 (33.3%) | 0/3 (0.0%) | 0.338 |
| Non cardiovascular | 12/20 (60.0%) | 5/8 (62.5%) | 5/9 (55.6%) | 2/3 (66.7%) | |
| Cardiovascular + non cardiovascular | 5/20 (25.0%) | 3/8 (37.5%) | 1/9 (11.1%) | 1/3 (33.3%) | |
| If cardiovascular: | |||||
| Heart failure | 6/20 (30.0%) | 3/8 (12.5) | 3/9 (33.3%) | 0/3 (0.0%) | |
| Arrhythmia | 1/20 (5.0%) | 0/8 (0.0%) | 0/9 (0.0%) | 1/3 (33.3%) | |
| Cerebral embolism | 1/20 (5.0%) | 0/8 (0.0%) | 1/9 (11.1%) | 0/3 (0.0%) | |
| If non cardiovascular: | |||||
| Sepsis | 14/20 (70.0%) | 8/8 (100.0%) | 4/9 (44.4%) | 2/3 (66.6%) | |
| Neoplasia | 1/20 (5.0%) | 0/8 (0.0%) | 1/9 (11.1%) | 0/3 (0.0%) |
| Hazard Ratio | 95% CI | p-Value | |
|---|---|---|---|
| Surgical Indication—not performed | 19.54 | [1.91–200.17] | 0.012 * |
| S. aureus | 2.99 | [1.07–8.33] | 0.036 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Roosens, B.; Cosyns, B.; Lancellotti, P.; Laroche, C.; Selton-Suty, C.; Pasquet, A.; De Sutter, J.; Unger, P.; Paelinck, B.; Vermeersch, P.; et al. Infective Endocarditis in Belgium: Prospective Data in Adults from the ESC EORP European Endocarditis Registry. J. Clin. Med. 2024, 13, 1371. https://doi.org/10.3390/jcm13051371
Roosens B, Cosyns B, Lancellotti P, Laroche C, Selton-Suty C, Pasquet A, De Sutter J, Unger P, Paelinck B, Vermeersch P, et al. Infective Endocarditis in Belgium: Prospective Data in Adults from the ESC EORP European Endocarditis Registry. Journal of Clinical Medicine. 2024; 13(5):1371. https://doi.org/10.3390/jcm13051371
Chicago/Turabian StyleRoosens, Bram, Bernard Cosyns, Patrizio Lancellotti, Cécile Laroche, Christine Selton-Suty, Agnès Pasquet, Johan De Sutter, Philippe Unger, Bernard Paelinck, Paul Vermeersch, and et al. 2024. "Infective Endocarditis in Belgium: Prospective Data in Adults from the ESC EORP European Endocarditis Registry" Journal of Clinical Medicine 13, no. 5: 1371. https://doi.org/10.3390/jcm13051371
APA StyleRoosens, B., Cosyns, B., Lancellotti, P., Laroche, C., Selton-Suty, C., Pasquet, A., De Sutter, J., Unger, P., Paelinck, B., Vermeersch, P., Motoc, A., Galloo, X., Iung, B., Habib, G., & on behalf of the EURO-ENDO Investigators Group. (2024). Infective Endocarditis in Belgium: Prospective Data in Adults from the ESC EORP European Endocarditis Registry. Journal of Clinical Medicine, 13(5), 1371. https://doi.org/10.3390/jcm13051371