
Heterogeneity in Measures of Illness among Patients with Myalgic Encephalomyelitis/Chronic Fatigue Syndrome Is Not Explained by Clinical Practice: A Study in Seven U.S. Specialty Clinics

 ,
,  , , ,
, , ,
Abstract
1. Background/Introduction
2. Methods
3. Results
3.1. Clinical Practice Characteristics of Study Sites
3.2. Description of Study Sample
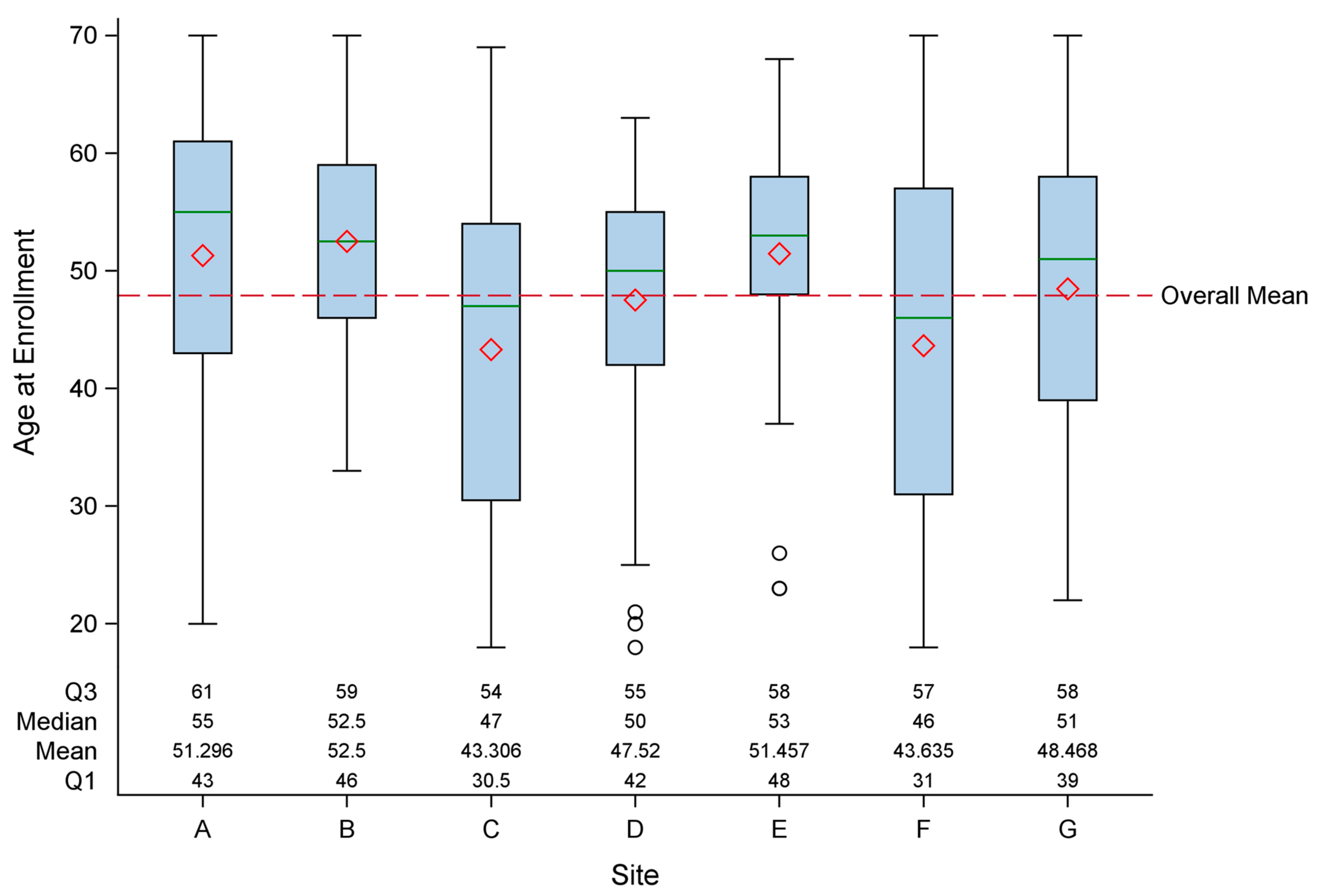
3.2.1. Socio-Demographic Characteristics
3.2.2. General Clinical Characteristics
3.3. Description of Illness
3.3.1. Functional Impairment
3.3.2. Measures of Post-Exertional Malaise (PEM)
3.3.3. Measures of Fatigue
3.3.4. Measures of Sleep
3.3.5. Measures of Neurocognitive/Autonomic Symptoms
3.3.6. Measures of Pain
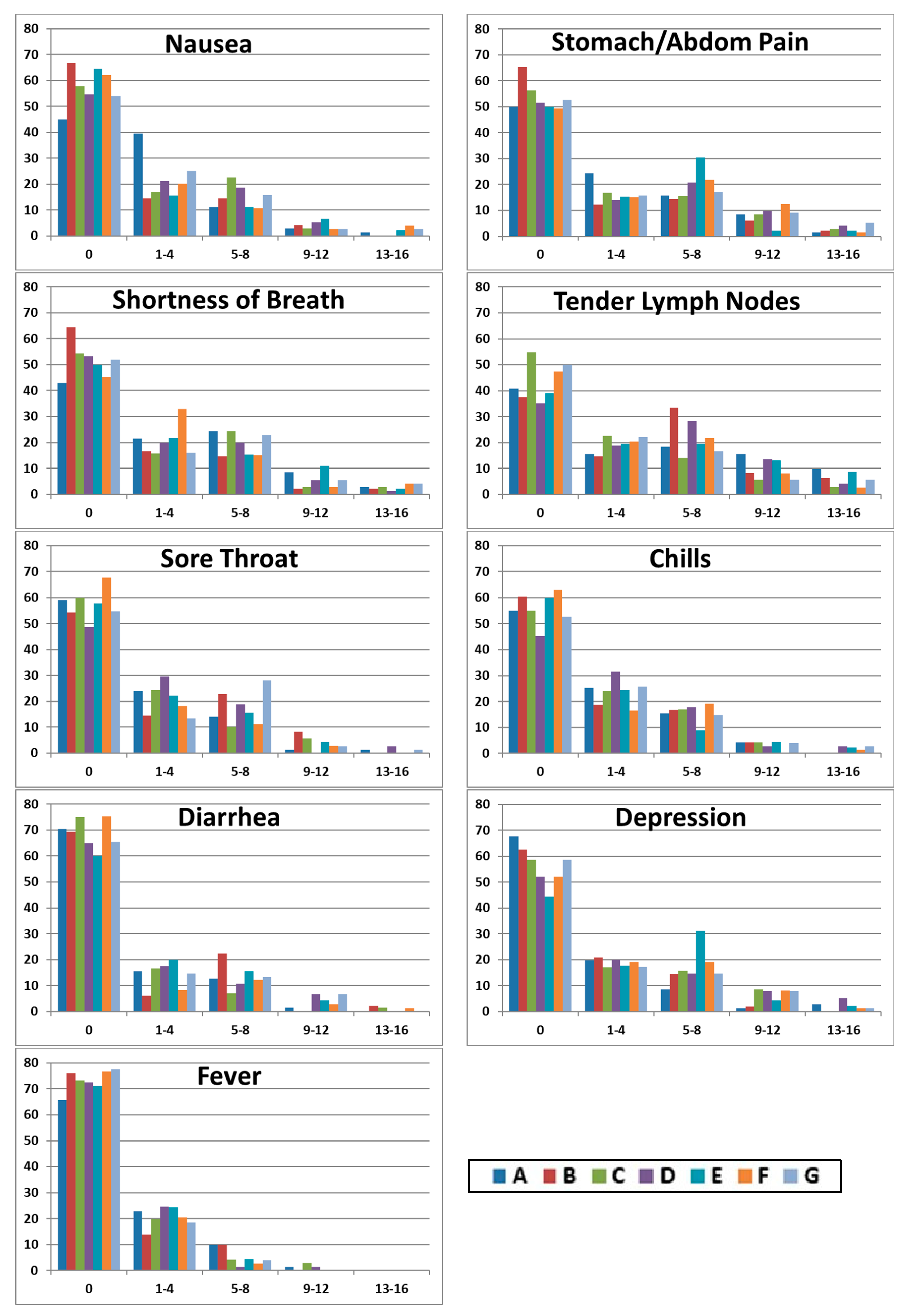
3.3.7. Measures of Other Symptoms
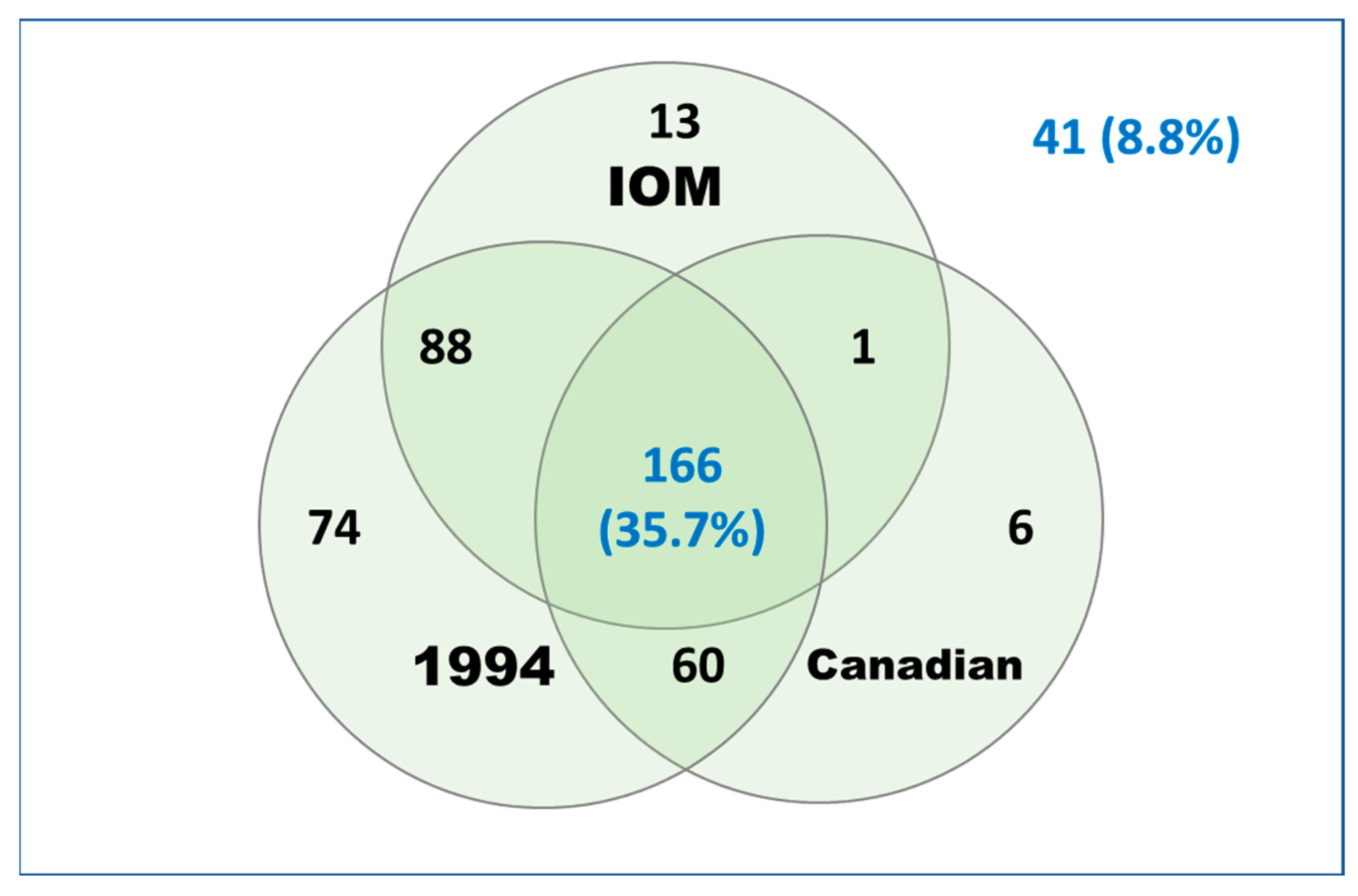
3.3.8. Proportion Meeting Case Definitions
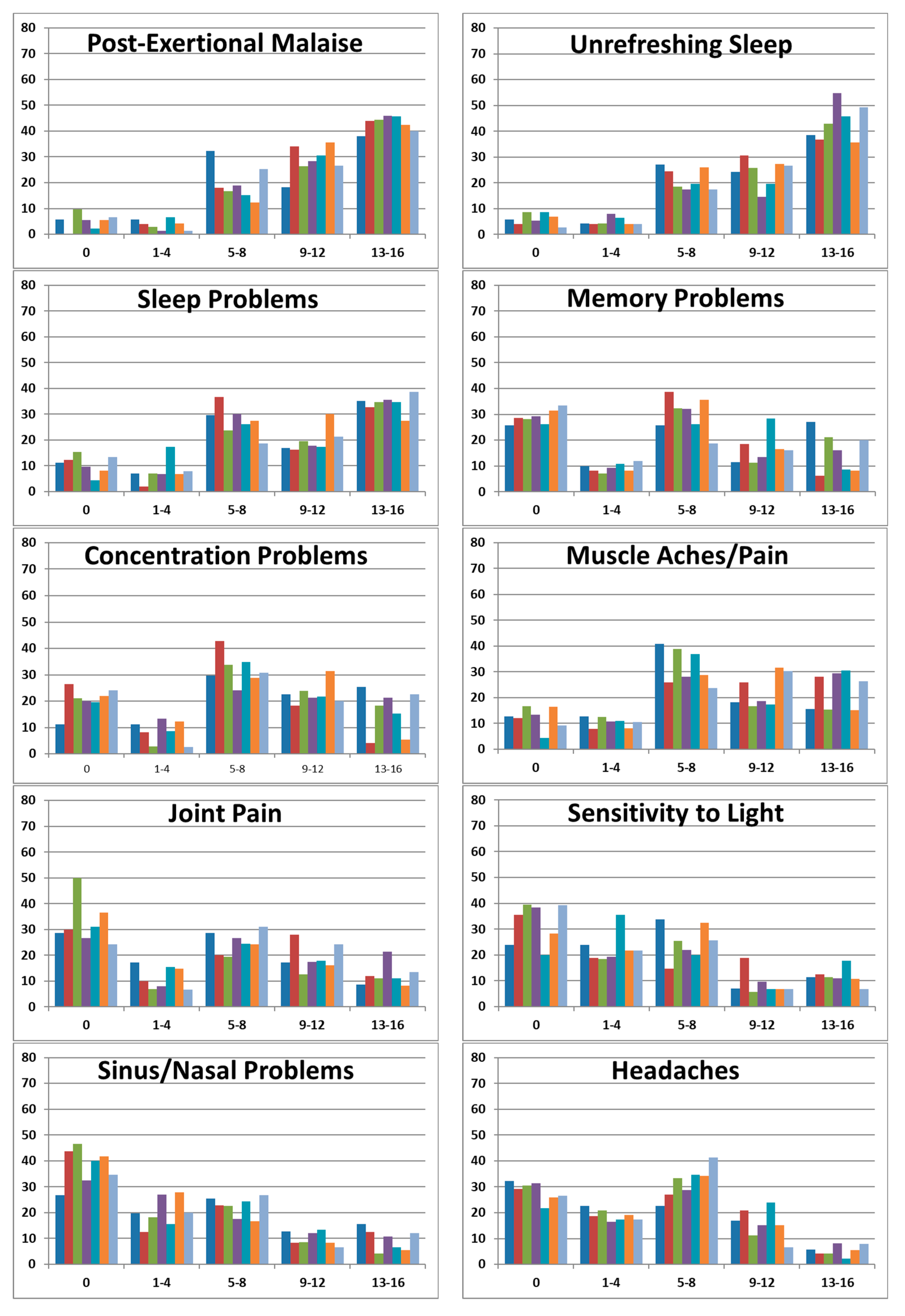
3.3.9. Histograms of CDC SI Scores
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Disclaimer
References
- Lin, J.M.S.; Resch, S.C.; Brimmer, D.J.; Johnson, A.; Kennedy, S.; Burstein, N.; Simon, C.J. The economic impact of chronic fatigue syndrome in Georgia: Direct and indirect costs. Cost. Eff. Resour. Alloc. 2011, 9, 1. [Google Scholar] [CrossRef]
- Reynolds, K.J.; Vernon, S.D.; Bouchery, E.; Reeves, W.C. The economic impact of chronic fatigue Syndr. Eff. Resour. Alloc. 2004, 2, 4. [Google Scholar] [CrossRef]
- Komaroff, A.L. Advances in Understanding the Pathophysiology of Chronic Fatigue Syndrome. JAMA 2019, 322, 499–500. [Google Scholar] [CrossRef]
- Hickie, I.; Davenport, T.; Vernon, S.D.; Nisenbaum, R.; Reeves, W.C.; Hadzi-Pavlovic, D.; Lloyd, A. Are chronic fatigue and chronic fatigue syndrome valid clinical entities across countries and health-care settings? Aust. N. Z. J. Psychiatry 2009, 43, 25–35. [Google Scholar] [CrossRef]
- Unger, E.R.; Lin, J.M.S.; Tian, H.; Gurbaxani, B.M.; Boneva, R.S.; Jones, J.F. Methods of applying the 1994 case definition of chronic fatigue syndrome—Impact on classification and observed illness characteristics. Popul. Health Metr. 2016, 14, 5. [Google Scholar] [CrossRef] [PubMed][Green Version]
- IOM (Institute of Medicine). Beyond Myalgic Encephalomyelitis/Chronic Fatigue Syndrome: Redefining an Illness; The National Academies Press: Washington, DC, USA, 2015; Available online: https://www.nap.edu/catalog/19012/beyond-myalgic-encephalomyelitischronic-fatigue-syndrome-redefining-an-illness (accessed on 21 February 2024).
- Unger, E.R.; Lin, J.M.S.; Tian, H.; Natelson, B.H.; Lange, G.; Vu, D.; Blate, M.; Klimas, N.G.; Balbin, E.G.; Bateman, L.; et al. Multi-Site Clinical Assessment of Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (MCAM): Design and Implementation of a Prospective/Retrospective Rolling Cohort Study. Am. J. Epidemiol. 2017, 185, 617–626. [Google Scholar] [CrossRef] [PubMed]
- Myalgic Encephalomyelitis/Chronic Fatigue Syndrome Common Data Elements 2019. Available online: https://www.commondataelements.ninds.nih.gov/Myalgic%20Encephalomyelitis/Chronic%20Fatigue%20Syndrome (accessed on 31 August 2019).
- Fukuda, K.; Straus, S.E.; Hickie, I.; Sharpe, M.C.; Dobbins, J.G.; Komaroff, A. International Chronic Fatigue Syndrome Study Group The chronic fatigue syndrome: A comprehensive approach to its definition and study. Ann. Intern. Med. 1994, 121, 953–959. [Google Scholar] [CrossRef]
- Cortes, R.M.; Mastronardi, C.; Silva-Aldana, C.T.; Arcos-Burgos, M.; Lidbury, B.A. Myalgic Encephalomyelitis/Chronic Fatigue Syndrome. J. Chronic Fatigue Syndr. 2003, 11, 7–115. [Google Scholar]
- De Meirleir, K.; Friedberg, F.; Jason, L.; Evans, M.; Porter, N.; Brown, M.; Brown, A.; Hunnell, J.; Anderson, V.; Lerch, A. The Development of a Revised Canadian Myalgic Encephalomyelitis Chronic Fatigue Syndrome Case Definition. Am. J. Biochem. Biotechnol. 2010, 6, 120–135. [Google Scholar]
- Yang, M.; Keller, S.; Lin, J.S. Psychometric properties of the PROMIS((R)) Fatigue Short Form 7a among adults with myalgic encephalomyelitis/chronic fatigue syndrome. Qual. Life Res. 2019, 28, 3375–3384. [Google Scholar] [CrossRef]
- Terwee, C.B.; Peipert, J.D.; Chapman, R.; Lai, J.S.; Terluin, B.; Cella, D.; Griffith, P.; Mokkink, L.B. Minimal important change (MIC): A conceptual clarification and systematic review of MIC estimates of PROMIS measures. Qual. Life Res. 2021, 30, 2729–2754. [Google Scholar] [CrossRef] [PubMed]
- Nacul, L.; Lacerda, E.M.; Kingdon, C.C.; Curran, H.; Bowman, E.W. How have selection bias and disease misclassification undermined the validity of myalgic encephalomyelitis/chronic fatigue syndrome studies? J. Health Psychol. 2019, 24, 1765–1769. [Google Scholar] [CrossRef]
- Klimas, N.G.; Ironson, G.; Carter, A.; Balbin, E.; Bateman, L.; Felsenstein, D.; Levine, S.; Peterson, D.; Chiu, K.; Allen, A.; et al. Findings from a clinical and laboratory database developed for discovery of pathogenic mechanisms in myalgic encephalomyelitis/chronic fatigue syndrome. Fatigue Biomed. Health Behav. 2015, 3, 75–96. [Google Scholar] [CrossRef]
- O’Boyle, S.; Nacul, L.; Nacul, F.E.; Mudie, K.; Kingdon, C.C.; Cliff, J.M.; Clark, T.G.; Dockrell, H.M.; Lacerda, E.M. A Natural History of Disease Framework for Improving the Prevention, Management, and Research on Post-viral Fatigue Syndrome and Other Forms of Myalgic Encephalomyelitis/Chronic Fatigue Syndrome. Front. Med. 2021, 8, 688159. [Google Scholar] [CrossRef] [PubMed]
- Davis, H.E.; Assaf, G.S.; McCorkell, L.; Wei, H.; Low, R.J.; Re’em, Y.; Redfield, S.; Austin, J.P.; Akrami, A. Characterizing long COVID in an international cohort: 7 months of symptoms and their impact. EClinicalMedicine 2021, 38, 101019. [Google Scholar] [CrossRef] [PubMed]
- Cotler, J.; Holtzman, C.; Dudun, C.; Jason, L.A. A Brief Questionnaire to Assess Post-Exertional Malaise. Diagnostics 2018, 8, 66. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Data Sources for Measures of Illness Domains |
|---|
| Functional impairment Medical Outcomes Study 36-Item Short Form Survey (SF-36) v2 Hours Vertical Report of Exercise CDC Health-related Quality of Life (HRQoL) (physically unhealthy days) |
| Post-exertional malaise Illness Abstraction Form (IAF) (medical records abstraction) CDC Symptom Inventory (PEM) DePaul Symptom Questionnaire (items 14–18) |
| Fatigue 20-item Multi-dimensional Fatigue Inventory (MFI-20) PROMIS Fatigue Short Form 7a (PROMIS F-SF 7a) |
| Sleep problems CDC Symptom Inventory (unrefreshing sleep, sleep problems) PROMIS Sleep Disturbance 8-Item Short Form PROMIS Sleep-Related Impairment Short Form v1.0 DePaul Symptom Questionnaire (items 19–24) |
| Neurocognitive/Autonomic Symptoms CDC Symptom Inventory (memory, concentration, sensitive to light, short of breath) DePaul Symptom Questionnaire (items 32–51) |
| Pain Brief Pain Inventory (long form) PROMIS Pain Interference Short Form 8a (PROMIS PI-SF 8a) PROMIS Pain Behavior Short Form 8a (PROMIS PB-SF 8a) CDC Symptom Inventory (headaches, joint pain, muscle aches) DePaul Symptom Questionnaire (items 25–31) |
| Other symptoms Immunologic/inflammation CDC Symptom Inventory (sore throat, sinus problems, tender lymph nodes, fever, chills) DePaul Symptom Questionnaire (items 62–66) Gastrointestinal CDC Symptom Inventory (stomach/abdominal pain, diarrhea) Emotional or behavioral CDC Symptom Inventory (Depression) Zung Self-Rating Depression Scale (SDS) 7-item Generalized Anxiety Disorder (GAD-7) CDC Health-Related Quality of Life (HRQoL) (mentally unhealthy days) 8-item Patient Health Questionnaire (PHQ-8) |
| A (n = 71, 15.3%) | B (n = 50, 10.8%) | C (n = 72, 15.5%) | D (n = 75, 16.1%) | E (n = 46, 9.9%) | F (n = 74, 15.9%) | G (n = 77, 16.7%) | Overall (n = 465) | |
|---|---|---|---|---|---|---|---|---|
| Age at enrollment, yrs, mean (SEM) *** | 51.3 (13.3) | 52.5 (8.5) | 43.3 (14.1) | 47.5 (10.5) | 51.5 (9.7) | 43.6 (14.8) | 48.5 (11.5) | 47.9 (12.6) |
| Sex * | ||||||||
| Male | 27 (38%) | 10 (20%) | 25 (34.7%) | 14 (18.7%) | 7 (15.2%) | 21 (28.4%) | 16 (20.8%) | 120 (25.8%) |
| Female | 44 (62%) | 40 (80%) | 47 (65.3%) | 61 (81.3%) | 39 (84.8%) | 53 (71.6%) | 61 (79.2%) | 345 (74.2%) |
| Female–male ratio | 1.6 | 4.0 | 1.9 | 4.4 | 5.6 | 2.5 | 3.8 | 2.9 |
| Race *** | ||||||||
| White | 70 (98.6%) | 47 (94%) | 65 (90.3%) | 75 (100%) | 45 (97.8%) | 72 (97.3%) | 65 (84.4%) | 439 (94.4%) |
| Black/African American | 0 | 1 (2%) | 0 | 0 | 1 (2.2%) | 0 | 4 (5.2%) | 6 (1.3%) |
| All others | 1 (1.4%) | 2 (4%) | 7 (9.7%) | 0 | 0 | 2 (2.7%) | 8 (10.4%) | 20 (4.3%) |
| Marital status ** | ||||||||
| Married/committed relationship | 41 (58.6%) | 30 (60%) | 37 (53.6%) | 42 (57.5%) | 33 (73.3%) | 42 (57.5%) | 31 (40.8%) | 256 (56.1%) |
| Previously married | 13 (18.6%) | 14 (28%) | 9 (13%) | 12 (16.4%) | 4 (8.9%) | 6 (8.2%) | 17 (22.4%) | 75 (16.5%) |
| Never married | 16 (22.9%) | 6 (12%) | 23 (33.3%) | 19 (26%) | 8 (17.8%) | 25 (34.2%) | 28 (36.8%) | 125 (27.4%) |
| Employment | ||||||||
| Full-time | 9 (12.9%) | 8 (16.3%) | 10 (14.3%) | 13 (17.3%) | 3 (6.5%) | 6 (8.2%) | 17 (22.1%) | 66 (14.4%) |
| Part-time | 8 (11.4%) | 5 (10.2%) | 15 (21.4%) | 8 (10.7%) | 2 (4.3%) | 6 (8.2%) | 7 (9.1%) | 51 (11.1%) |
| Not employed | 53 (75.7%) | 36 (73.5%) | 45 (64.3%) | 54 (72%) | 41 (89.1%) | 61 (83.6%) | 53 (68.8%) | 343 (74.6%) |
| Insurance ** | ||||||||
| Yes | 64 (95.5%) | 50 (100%) | 62 (89.9%) | 75 (100%) | 40 (87%) | 68 (91.9%) | 71 (94.7%) | 430 (94.3%) |
| No | 3 (4.5%) | 0 | 7 (10.1%) | 0 | 6 (13%) | 6 (8.1%) | 4 (5.3%) | 26 (5.7%) |
| Education *** | ||||||||
| Less than high school | 0 | 0 | 0 | 1 (1.5%) | 0 | 3 (4.1%) | 0 | 4 (0.9%) |
| High school graduate | 18 (26.5%) | 9 (18%) | 10 (14.1%) | 17 (25%) | 6 (13.3%) | 27 (37%) | 14 (18.2%) | 101 (22/4%) |
| College graduate | 22 (32.4%) | 26 (52%) | 28 (39.4%) | 23 (33.8%) | 19 (42.2%) | 32 (43.8%) | 28 (36.4%) | 178 (39.4%) |
| Post-college | 28 (41.2%) | 15 (30%) | 33 (46.5%) | 27 (39.7%) | 20 (44.4%) | 11 (15.1%) | 35 (45.5%) | 169 (37.4%) |
| A (n = 71, 15.3%) | B (n = 50, 10.8%) | C (n = 72, 15.5%) | D (n = 75, 16.1%) | E (n = 46, 9.9%) | F (n = 74, 15.9%) | G (n = 77, 16.7%) | Overall (n = 465) | |
|---|---|---|---|---|---|---|---|---|
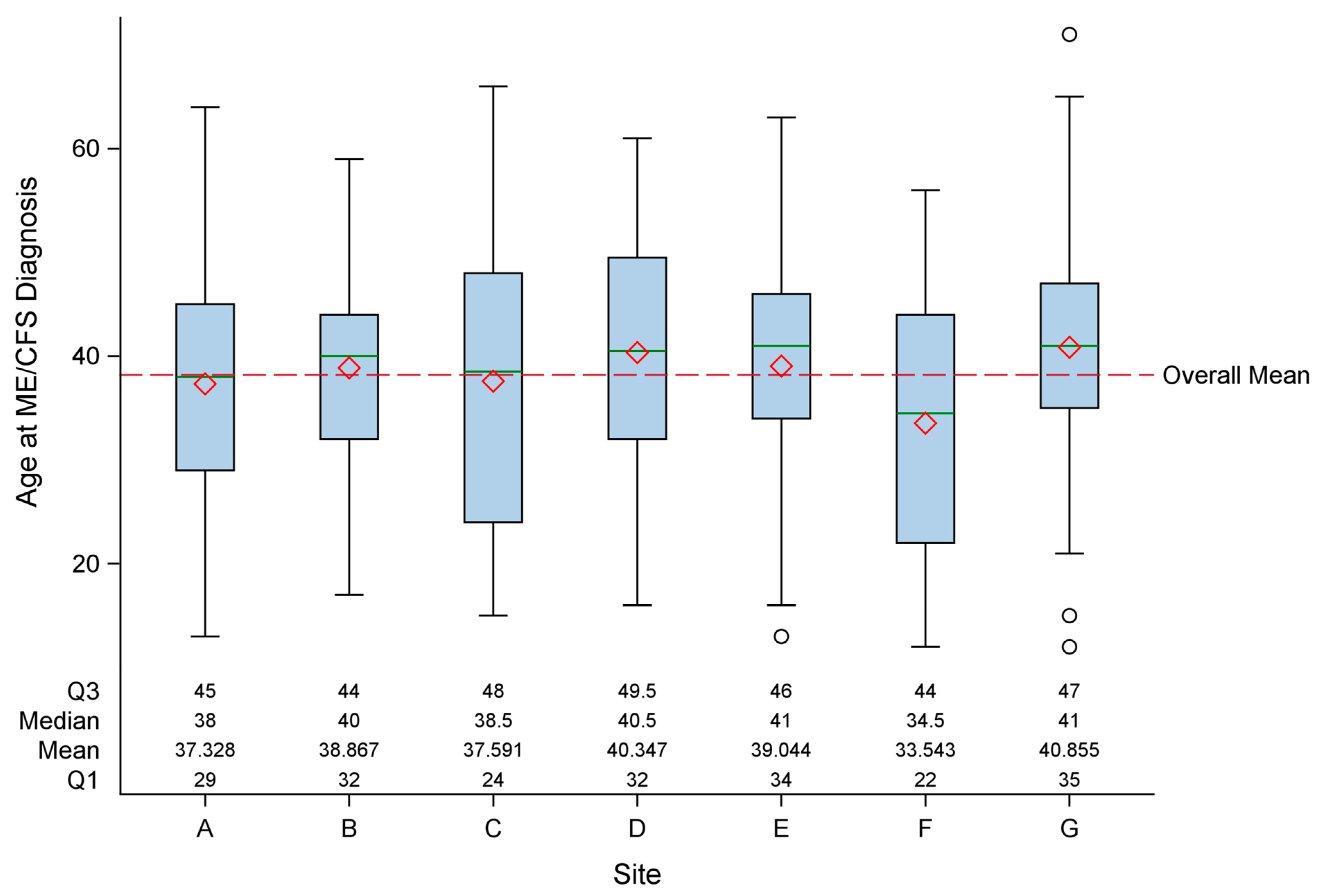
| Age at diagnosis (yrs) ** | 37.3 (11) | 38.9 (9.9) | 37.6 (14) | 40.3 (11.4) | 39.0 (11) | 33.5 (12.2) | 40.9 (11.9) | 38.2 (12.6) |
| Mode of onset ** | ||||||||
| Sudden | 46 (75.4%) | 22 (52.4%) | 48 (72.7%) | 41 (63.1%) | 27 (67.5%) | 47 (74.6%) | 33 (49.3%) | 264 (65.4%) |
| Gradual | 15 (24.6%) | 20 (47.6%) | 18 (27.3%) | 24 (36.9%) | 13 (32.5%) | 16 (25.4%) | 34 (50.7%) | 140 (34.6%) |
| Duration of fatigue (yrs) *** | 17.9 (9.9) | 16.5 (8.3) | 9.4 (8.0) | 10.9 (9.6) | 17.8 (10.8) | 13.5 (8.9) | 14.7 (10.6) | 14.1 (9.9) |
| BMI (kg/m2) ** | 26.2 (4.5) | 28.8 (7.6) | 24.3 (4.9) | 26.6 (6.1) | 29.2 (7) | 25.5 (5.7) | 25.9 (7.3) | 26.6 (6.3) |
| Number of medications *** | 5.6 (4.2) | 6.5 (4.7) | 4.1 (3.4) | 6.4 (4.4) | 8.2 (4.8) | 6.4 (4.5) | 5.0 (4.1) | 5.9 (4.4) |
| A (n = 71, 15.3%) | B (n = 50, 10.8%) | C (n = 72, 15.5%) | D (n = 75, 16.1%) | E (n = 46, 9.9%) | F (n = 74, 15.9%) | G (n = 77, 16.7%) | Overall (n = 465) | |
|---|---|---|---|---|---|---|---|---|
| SF-36 (0–100) | ||||||||
| Physical Functioning | 38.9 (27.8) | 41 (23.1) | 38.8 (24.8) | 36.8 (22.5) | 35.2 (25.2) | 38.7 (20.1) | 39.9 (19.7) | 38.5 (23.3) |
| Role Physical | 7.4 (22.9) | 4.5 (12.0) | 4.0 (18.0) | 6.3 (20.2) | 7.2 (22.4) | 3.8 (14.8) | 4.0 (15.4) | 5.2 (18.3) |
| Bodily Pain | 39.2 (25.3) | 34.7 (24.1) | 41.6 (24.2) | 37.2 (26.0) | 36.3 (24.1) | 37.3 (23.4) | 33.9 (20.8) | 37.3 (24.0) |
| General Health | 25.1 (19.2) | 28.5 (18.5) | 23.7 (13.6) | 24.8 (16.6) | 28.4 (16.7) | 24.5 (13.4) | 27.7 (17.1) | 25.9 (16.5) |
| Vitality/energy/fatigue | 20.7 (21.0) | 19.1 (14.9) | 15.9 (18.5) | 14.3 (16.3) | 17.4 (21) | 18.1 (14.4) | 15.5 (12.0) | 17.1 (17.0) |
| Social Functioning | 26.6 (26.4) | 31.9 (20.1) | 21.7 (24.3) | 23.6 (23.5) | 27.2 (28.8) | 26.4 (21.8) | 25.2 (18.5) | 25.7 (23.4) |
| Role Emotion | 82.8 (36.6) | 74.7 (41.3) | 70.4 (43.5) | 69.8 (42.4) | 62.3 (45.9) | 62.6 (44.8) | 73.6 (40.6) | 71.1 (42.4) |
| Mental Health | 69.6 (22.3) | 67.3 (20.3) | 61.4 (20.4) | 65 (21.8) | 66.1 (24.5) | 65.5 (20.5) | 66.1 (20.1) | 65.7 (21.3) |
| Hours of Vertical Activity (0–15) | 7.8 (4.2) | 8.0 (3.7) | 7.3 (4.7) | 7.9 (4.5) | 6.3 (4.1) | 7.5 (3.7) | 7.5 (4.1) | 7.5 (4.2) |
| Exercise (Yes/No) | ||||||||
| Strenuous exercise | 7 (10.9%) | 4 (10.0%) | 8 (11.6%) | 5 (6.7%) | 2 (4.6%) | 5 (7.7%) | 3 (4.1%) | 34 (7.8%) |
| Moderate exercise | 19 (28.4%) | 16 (36.4%) | 21 (30.4%) | 17 (23.3%) | 11 (25.0%) | 22 (32.8%) | 23 (31.1%) | 129 (29.5%) |
| Mild exercise | 40 (66.7%) | 37 (84.1%) | 49 (71.0%) | 47 (65.3%) | 32 (71.1%) | 53 (75.7%) | 60 (83.3%) | 318 (73.6%) |
| CDC Health-related QoL (0–30 days) | ||||||||
| Physically unhealthy days | 22.4 (10.0) | 20.6 (9.7) | 25.1 (9.1) | 24.8 (9.4) | 21.8 (9.2) | 20.5 (9.5) | 25.0 (9.1) | 23.2 (9.5) |
| A (n = 71, 15.3%) | B (n = 50, 10.8%) | C (n = 72, 15.5%) | D (n = 75, 16.1%) | E (n = 46, 9.9%) | F (n = 74, 15.9%) | G (n = 77, 16.7%) | Overall (n = 465) | |
|---|---|---|---|---|---|---|---|---|
| Illness Abstraction Form 1 | ||||||||
| PEM present (%) | 60 (84.5%) | 44 (88.0%) | 63 (87.5%) | 68 (90.7%) | 40 (87.0%) | 62 (83.8%) | 67 (87.0%) | 421 (87.5%) |
| CDC SI (score range 0–16) 1 | ||||||||
| PEM score, 0–16 | 10.8 (5.1) | 12.6 (3.3) | 11.5 (5.3) | 12.1 (4.7) | 12.1 (4.7) | 11.8 (4.8) | 11.4 (4.9) | 11.7 (4.8) |
| PEM present (%) 2 | 67 (94.4%) | 50 (100%) | 65 (90.3%) | 70 (94.6%) | 45 (97.8%) | 69 (94.5%) | 70 (93.3%) | 446 (94.7%) |
| DePaul Symptom Questionnaire (DSQ) (score range 0–16) 1 | ||||||||
| 14—Dead/heavy feeling after starting exercise | 8.3 (5.3) | 8.2 (5.8) | 8.9 (5.3) | 8.8 (5.9) | 8.9 (6) | 8.4 (5.3) | 7.6 (5.6) | 8.4 (5.5) |
| 15—Sore/fatigue next day after usual activity | 7.4 (4.9) | 7.9 (5.6) | 8.1 (5.2) | 9.2 (5.7) | 8.5 (5.5) | 7.5 (4.5) | 9.1 (5.1) | 8.3 (5.2) |
| 16—Mentally tired after slightest effort | 6.4 (5.1) | 5.8 (5.2) | 7.3 (4.9) | 7.1 (5.6) | 6.8 (5.3) | 5.2 (4.4) | 7 (5.1) | 6.5 (5.1) |
| 17—Tired after minimal exercise | 7.9 (5.7) | 8.3 (5.1) | 9.5 (5.3) | 10.1 (5.6) | 9.5 (5.6) | 8.9 (4.9) | 9.4 (5.1) | 9.1 (5.4) |
| 18—Physically drained or sick after mild activity | 7.2 (5.6) | 7.4 (5.6) | 8.4 (5.4) | 8.5 (5.4) | 8.3 (5.5) | 7.1 (4.4) | 8.4 (5.4) | 7.9 (5.3) |
| PEM present (%) 3 | 64 (90.1%) | 48 (96.0%) | 69 (95.8%) | 69 (92.0%) | 41 (89.1%) | 71 (96.0%) | 75 (97.4%) | 437 (94.0%) |
| A (n = 71, 15.3%) | B (n = 50, 10.8%) | C (n = 72, 15.5%) | D (n = 75, 16.1%) | E (n = 46, 9.9%) | F (n = 74, 15.9%) | G (n = 77, 16.7%) | Overall (n = 465) | |
|---|---|---|---|---|---|---|---|---|
| MFI-20 (score range 4–20) | ||||||||
| General Fatigue | 17.7 (3.0) | 18.1 (2.3) | 18.4 (2.0) | 18.6 (2.1) | 18.1 (2.8) | 18.2 (2.2) | 18.5 (1.5) | 18.2 (2.3) |
| Physical Fatigue * | 16.9 (3.5) | 16.5 (3.0) | 17.9 (2.7) | 17.7 (2.7) | 17 (3.3) | 17.9 (2.2) | 17.7 (2.3) | 17.4 (2.8) |
| Mental Fatigue | 14.3 (4.1) | 14.1 (4.2) | 15.2 (4.2) | 14.9 (4.1) | 14.7 (3.8) | 14.7 (3.4) | 15.2 (4.0) | 14.8 (4.0) |
| Reduced Activity * | 15.1 (3.8) | 15.3 (3.8) | 17.2 (2.9) | 16.2 (4.0) | 16.4 (3.9) | 16.2 (3.4) | 16.2 (3.3) | 16.1 (3.6) |
| Reduced Motivation | 11.4 (3.7) | 11.5 (4.8) | 11.6 (4.7) | 12.1 (4.1) | 13.7 (4.2) | 11.9 (3.7) | 12.3 (4.3) | 12.0 (4.2) |
| PROMIS Fatigue | ||||||||
| T-Score (range 29.4–83.2) | 67.0 (8.4) | 67.4 (5.9) | 68.7 (7.4) | 68.5 (7.4) | 69.7 (8.1) | 67.9 (5.3) | 68.9 (6.4) | 68.3 (7.0) |
| A (n = 71, 15.3%) | B (n = 50, 10.8%) | C (n = 72, 15.5%) | D (n = 75, 16.1%) | E (n = 46, 9.9%) | F (n = 74, 15.9%) | G (n = 77, 16.7%) | Overall (n = 465) | |
|---|---|---|---|---|---|---|---|---|
| CDC-SI (score range 0–16) | ||||||||
| Unrefreshing sleep | 11.1 (5.0) | 11.3 (4.7) | 11.3 (5.3) | 11.8 (5.5) | 11.1 (5.6) | 10.8 (5.0) | 12.4 (4.5) | 11.4 (5.1) |
| Sleeping problems | 9.8 (5.6) | 9.8 (5.5) | 9.6 (6.0) | 9.8 (5.6) | 9.8 (5.7) | 10.1 (5.1) | 10.1 (6) | 9.9 (5.6) |
| PROMIS Sleep | ||||||||
| Sleep disturbance T-score (range 28.4–83.2) | 59.5 (8.2) | 59.7 (8.0) | 59.3 (8.4) | 59.3 (8.3) | 59.5 (8.8) | 58.5 (7.7) | 60.4 (7.6) | 59.4 (8.1) |
| Sleep-related impairment T-score (range 30.0–80.0) * | 61.5 (8.4) | 64.2 (6.7) | 62 (8.4) | 61.6 (8.6) | 61.9 (8.6) | 60.5 (7.1) | 64.3 (7.6) | 62.2 (8.0) |
| DePaul Symptom Questionnaire (score range 0–16) | ||||||||
| 19—Unrefreshed * | 9.6 (5.1) | 10.4 (5.5) | 10.8 (4.9) | 10.9 (5.3) | 9.9 (5.9) | 9.4 (4.7) | 11.8 (4.3) | 10.4 (5.1) |
| 20—Need to nap | 5.7 (5.5) | 7.1 (5.5) | 6.3 (5.8) | 7 (5.8) | 7.6 (5.6) | 5.2 (5) | 7.1 (5.8) | 6.5 (5.6) |
| 21—Problems falling asleep | 7.4 (5.7) | 6 (5.2) | 6.6 (5.5) | 6.5 (6) | 7.2 (5.6) | 7.2 (5.4) | 8 (6) | 7.0 (5.7) |
| 22—Problems staying asleep | 6.6 (5.2) | 6.5 (5.7) | 6.1 (5.6) | 6.8 (6.3) | 6.9 (6.2) | 5.9 (5.3) | 6.9 (6) | 6.5 (5.7) |
| 23—Awaking too early | 6.2 (5.7) | 6 (5.4) | 4.4 (5.4) | 5.7 (6.1) | 5.8 (6.2) | 3.9 (4.5) | 4.9 (5.3) | 5.2 (5.5) |
| 24—Sleep all day/awake all night | 1.5 (3.5) | 1.3 (3.4) | 1.9 (3.7) | 1.4 (2.9) | 1.2 (2.2) | 2.0 (3.1) | 1.4 (3.5) | 1.5 (3.3) |
| A (n = 71, 15.3%) | B (n = 50, 10.8%) | C (n = 72, 15.5%) | D (n = 75, 16.1%) | E (n = 46, 9.9%) | F (n = 74, 15.9%) | G (n = 77, 16.7%) | Overall (n = 465) | |
|---|---|---|---|---|---|---|---|---|
| CDC-SI (score range 0–16) | ||||||||
| Memory | 7.7 (6.3) | 6.1 (5.0) | 7.2 (6.0) | 6.5 (5.8) | 6.9 (5.4) | 6.0 (5.3) | 6.7 (6.3) | 6.7 (5.8) |
| Concentration | 8.9 (5.6) | 6.0 (4.7) | 8.3 (5.5) | 7.7 (6.0) | 7.7 (5.4) | 6.9 (5.2) | 8.3 (5.9) | 7.8 (5.6) |
| Sensitive to light | 5.5 (5.2) | 5.6 (5.8) | 4.5 (5.4) | 4.7 (5.4) | 5.7 (5.8) | 5.2 (5.2) | 4.0 (4.8) | 5.0 (5.3) |
| Short of breath | 3.6 (4.5) | 1.9 (3.6) | 2.6 (3.9) | 2.5 (3.8) | 3.0 (4.4) | 2.7 (4.0) | 3.1 (4.4) | 2.8 (4.1) |
| DePaul Symptom Questionnaire (score range 0–16) | ||||||||
| 32—Muscle twitch | 2.7 (3.6) | 3.1 (4.3) | 2.3 (3.6) | 2.3 (3.2) | 3.2 (3.5) | 1.8 (2.9) | 2.8 (3.5) | 2.5 (3.5) |
| 33—Muscle weak | 6.1 (5) | 5.6 (5.2) | 6.0 (5.1) | 6.1 (5.6) | 7.8 (5.4) | 5.6 (4.5) | 6.4 (4.6) | 6.2 (5.0) |
| 34—Noise sensitive ** | 6.1 (5.1) | 6.5 (5.4) | 5.6 (4.9) | 4.5 (5) | 8.4 (5.5) | 5.8 (4.9) | 5.5 (4.8) | 5.9 (5.1) |
| 35—Bright light sensitive | 5.9 (5.1) | 6.2 (5.8) | 4.9 (4.8) | 5.5 (5.3) | 7.6 (5.9) | 5 (4.9) | 4.9 (4.6) | 5.6 (5.2) |
| 36—Memory | 7.2 (5.5) | 7.0 (4.5) | 7.5 (5.5) | 7.0 (5.6) | 7.6 (4.6) | 5.8 (4.1) | 7.2 (5.2) | 7.0 (5.1) |
| 37—Concentration | 8.2 (5.4) | 6.3 (5.3) | 8.1 (5.5) | 8.5 (5.7) | 7.9 (5.4) | 6.5 (4.4) | 8.2 (5.4) | 7.7 (5.3) |
| 38—Word-finding difficulty | 6.8 (5.4) | 6.2 (5.1) | 6.8 (5) | 6.5 (5.9) | 7.2 (5.4) | 6.1 (4.1) | 7.2 (5.2) | 6.7 (5.1) |
| 39—Difficulty understanding | 5.0 (5) | 3.5 (4) | 4.5 (4.7) | 3.8 (4.9) | 5.2 (4.9) | 3.4 (3) | 3.9 (4.3) | 4.2 (4.4) |
| 40—Only focus on one thing | 7.1 (5.1) | 6.2 (5) | 7.7 (5.7) | 7.4 (5.3) | 8.1 (5.6) | 5.6 (4.8) | 6.9 (5) | 7.0 (5.2) |
| 41—Unable to focus vision/attention | 4.7 (5.3) | 3.6 (4.4) | 5.7 (5.3) | 4.4 (5) | 5.4 (5.3) | 3.5 (3.8) | 4.9 (4.8) | 4.6 (4.9) |
| 42—Loss depth perception | 2.6 (4.3) | 2.4 (4.4) | 2.8 (4.6) | 1.9 (3.8) | 3.3 (4.5) | 1.3 (2.8) | 1.5 (3.1) | 2.2 (3.9) |
| 43—Slow thought | 6.5 (5.6) | 4.7 (4.5) | 6.7 (5.4) | 5.5 (5.5) | 6.1 (5) | 4.7 (4.3) | 5.7 (5) | 5.7 (5.1) |
| 44—Forgetful | 6.6 (5.6) | 5.8 (4.7) | 7.3 (5.6) | 6.5 (5.5) | 7.3 (5.4) | 5.1 (4.3) | 6 (5.3) | 6.3 (5.3) |
| 45—Bladder problems | 3.4 (4.9) | 3.6 (5.4) | 2.9 (4.6) | 3.9 (5.1) | 4 (4.9) | 2.1 (3.2) | 2.8 (4) | 3.2 (4.6) |
| 46—Irritable bowel problems | 3.8 (4.7) | 5.0 (6) | 3.4 (4.9) | 4.8 (5.8) | 4.8 (5.5) | 3.9 (4.6) | 4.3 (4.7) | 4.2 (5.1) |
| 47—Nausea | 1.9 (2.7) | 1.7 (3.2) | 2.4 (3.3) | 2.4 (3.5) | 2.3 (3.2) | 2.5 (4.2) | 1.9 (2.9) | 2.2 (3.3) |
| 48—Unsteady on feet * | 2.7 (3.4) | 2.9 (4.1) | 3.6 (4.1) | 3.1 (3.7) | 5.2 (5.3) | 2.9 (3.2) | 3.3 (3.8) | 3.3 (3.9) |
| 49—Shortness of breath | 3.5 (4.6) | 2.1 (3.9) | 3.2 (4) | 2.7 (3.9) | 3.4 (4.3) | 2.6 (3.5) | 3.2 (4.2) | 3.0 (4.1) |
| 50—Dizziness or fainting | 2.8 (3.4) | 2 (3.3) | 3.3 (3.6) | 3.2 (3.6) | 2.8 (3.7) | 2.9 (3.2) | 2.6 (2.9) | 2.8 (3.4) |
| 51—Irregular heart beats | 2.0 (3) | 1.3 (2.1) | 1.9 (3) | 2.1 (3.3) | 1.6 (2.5) | 1.5 (2.1) | 1.5 (2.9) | 1.7 (2.8) |
| A (n = 71, 15.3%) | B (n = 50, 10.8%) | C (n = 72, 15.5%) | D (n = 75, 16.1%) | E (n = 46, 9.9%) | F (n = 74, 15.9%) | G (n = 77, 16.7%) | Overall (n = 465) | |
|---|---|---|---|---|---|---|---|---|
| Brief Pain Inventory (score range 0–10) | ||||||||
| Interference of pain | 4.6 (0.4) | 5.3 (0.4) | 4.1 (0.4) | 5.1 (0.3) | 5.1 (0.4) | 4.9 (0.3) | 5 (0.3) | 4.8 (0.1) |
| Severity of pain ** | 3.8 (0.3) | 4.7 (0.4) | 3.4 (0.3) | 4.8 (0.3) | 4.5 (0.3) | 4.1 (0.3) | 4.9 (0.3) | 4.3 (0.1) |
| PROMIS | ||||||||
| Pain Interference T-Score (range 41.0–78.3) | 61.1 (1.1) | 63.9 (1.3) | 59.6 (1.2) | 62.2 (1.2) | 64.1 (1.4) | 62.5 (1) | 62.8 (1.1) | 62.2 (0.4) |
| Pain Behavior T-Score (range 36.7–75.9) | 56.9 (0.9) | 58.6 (1) | 55.5 (1) | 56.3 (1) | 58.8 (1.1) | 58 (0.8) | 58 (0.8) | 57.3 (0.3) |
| CDC-SI (score range 0–16) | ||||||||
| Headaches | 4.8 (5.2) | 5.3 (5.1) | 4.4 (4.6) | 5.3 (5.2) | 5.7 (4.7) | 5.3 (4.9) | 5.4 (4.8) | 5.2 (4.9) |
| Joint pain * | 5.7 (5.3) | 6.7 (5.8) | 4.7 (5.7) | 7.4 (6.0) | 5.9 (5.7) | 5.2 (5.3) | 7.1 (5.5) | 6.1 (5.7) |
| Muscle aches | 7.7 (5.1) | 9.4 (5.6) | 7.2 (5.2) | 8.9 (5.8) | 9.5 (5.3) | 8.2 (5.3) | 9.5 (5.3) | 8.5 (5.4) |
| DePaul Symptom Questionnaire (score range 0–16) | ||||||||
| 25—Muscle pain or ache * | 7 (5.2) | 8.4 (5.6) | 6.5 (5.1) | 8.3 (5.6) | 8.4 (5.4) | 6.8 (4.4) | 9.1 (5.4) | 7.7 (5.3) |
| 26—Pain/stiffness without swelling >1 joint * | 5.8 (5.6) | 7.1 (6) | 4.9 (5.4) | 7.6 (6) | 6.9 (5.7) | 5.5 (5.1) | 7.2 (5.4) | 6.4 (5.6) |
| 27—Eye pain | 2.3 (3.5) | 2.2 (3.6) | 1.7 (2.7) | 2.2 (3.5) | 2.6 (4.1) | 1.9 (3) | 2.1 (3.7) | 2.1 (3.4) |
| 28—Chest pain | 1.8 (3.6) | 0.9 (2.3) | 2.2 (3.7) | 2 (3.5) | 1.5 (2.2) | 1.4 (2.6) | 1.2 (2.4) | 1.6 (3.0) |
| 29—Bloating | 4 (4.3) | 4.8 (5.1) | 3.8 (4.8) | 4.1 (4.6) | 3.6 (4) | 2.9 (4) | 3.4 (4.6) | 3.8 (4.5) |
| 30—Stomach pain | 2.5 (2.8) | 3.2 (4.1) | 3.1 (3.7) | 3.4 (4.6) | 3.5 (4.2) | 2.7 (3.1) | 2.5 (3.4) | 2.9 (3.7) |
| 31—Headaches | 4.4 (4.7) | 4.6 (4.7) | 4.3 (3.9) | 4.6 (4.2) | 4.5 (3.7) | 4.1 (3.6) | 4.7 (4.8) | 4.4 (4.2) |
| A (n = 71, 15.3%) | B (n = 50, 10.8%) | C (n = 72, 15.5%) | D (n = 75, 16.1%) | E (n = 46, 9.9%) | F (n = 74, 15.9%) | G (n = 77, 16.7%) | Overall (n = 465) | |
|---|---|---|---|---|---|---|---|---|
| Immunologic/inflammation | ||||||||
| CDC SI (score range 0–16) | ||||||||
| Sore throat | 1.7 (3.0) | 2.8 (3.9) | 1.8 (3.1) | 2.4 (3.5) | 1.9 (3.0) | 1.4 (2.7) | 2.7 (3.7) | 2.1 (3.3) |
| Sinus problems | 6.0 (5.6) | 4.9 (5.6) | 3.7 (4.6) | 4.8 (5.4) | 4.5 (5.1) | 3.8 (4.7) | 5.0 (5.4) | 4.7 (5.2) |
| Tender lymph nodes * | 4.9 (5.6) | 4.5 (4.8) | 2.4 (3.8) | 4.5 (4.6) | 4.6 (5.3) | 3.2 (4.2) | 3.2 (4.6) | 3.8 (4.8) |
| Fever | 1.2 (2.3) | 0.8 (1.9) | 1.0 (2.5) | 0.6 (1.6) | 0.9 (1.7) | 0.6 (1.3) | 0.7 (1.6) | 0.8 (1.9) |
| Chills | 1.9 (3.2) | 1.8 (3.1) | 1.9 (3.1) | 2.4 (3.6) | 1.8 (3.7) | 1.8 (3.1) | 2.3 (3.8) | 2.0 (3.4) |
| DePaul Symptom Questionnaire (score range 0–16) | ||||||||
| 62—Sore throat | 2.5 (3.3) | 2.6 (3.5) | 2.5 (3) | 2.7 (3.4) | 2.8 (3.3) | 2 (2.3) | 2.7 (3.3) | 2.5 (3.2) |
| 63—Tender lymph nodes | 4.1 (4.3) | 4 (4.6) | 2.6 (3.3) | 4.4 (4.4) | 4.7 (4.9) | 3 (3.9) | 3.3 (4.3) | 3.7 (4.2) |
| 64—Fever ** | 1.5 (2.5) | 1.1 (1.8) | 1.4 (2.3) | 0.6 (0.9) | 1.7 (3) | 0.6 (1.1) | 0.8 (1.7) | 1.1 (2.0) |
| 65—Flu-like symptoms | 4.7 (4.5) | 4 (4.9) | 5.2 (4.8) | 4.8 (4.7) | 5.7 (4.8) | 4.4 (4.1) | 3.5 (4.4) | 4.6 (4.6) |
| 66—Sickened by smells, food, medications, chemicals | 4.8 (5) | 5.2 (5.8) | 4.2 (5.3) | 4.2 (4.9) | 6.5 (6) | 4.3 (5) | 5 (5.1) | 4.8 (5.2) |
| Gastrointestinal | ||||||||
| CDC SI (score range 0–16) | ||||||||
| Stomach pain | 2.8 (4.1) | 2.3 (4.0) | 2.9 (4.4) | 3.5 (4.8) | 2.9 (3.8) | 3.2 (4.3) | 3.4 (4.9) | 3.0 (4.4) |
| Diarrhea | 1.1 (2.3) | 1.8 (3.3) | 0.9 (2.5) | 1.8 (3.3) | 1.9 (3.2) | 1.5 (3.4) | 1.9 (3.4) | 1.5 (3.1) |
| Emotional or behavioral | ||||||||
| CDC SI (score range 0–16) | ||||||||
| Depression | 1.5 (3.4) | 1.5 (2.8) | 2.4 (3.9) | 3.1 (4.8) | 3.3 (4.1) | 2.7 (4.1) | 2.4 (4.1) | 2.4 (4.0) |
| Zung SDS (score range 0–80) | ||||||||
| 42.6 (7.7) | 42.8 (8.4) | 46.0 (9.8) | 46.7 (9.7) | 45.6 (10.4) | 45.3 (8.8) | 45.3 (8.1) | 45.0 (9.0) | |
| GAD-7 Anxiety (score range 0–21) | ||||||||
| 3.9 (5.2) | 5.0 (5.4) | 5.3 (5.4) | 6.7 (6.2) | 4.7 (4.1) | 4.7 (5.1) | 4.7 (5.2) | 5.1 (5.3) | |
| CDC Health-related QoL (0–30 days) | ||||||||
| Mentally unhealthy days | 8.3 (10.2) | 9.0 (9.4) | 10.7 (11) | 8.4 (11.5) | 10.6 (10.6) | 10.1 (10) | 7.8 (10.1) | 9.2 (10.5) |
| PHQ-8 Depression (score range 0–24) | ||||||||
| 9.8 (5.4) | 9.6 (5.8) | 10.2 (5.5) | 11.4 (5.1) | 9.0 (4.9) | 9.7 (5) | 10.0 (4.1) | 10.0 (5.1) | |
| Case Definition Number Meeting (%) | A (n = 71, 15.3%) | B (n = 50, 10.8%) | C (n = 72, 15.5%) | D (n = 75, 16.1%) | E (n = 46, 9.9%) | F (n = 74, 15.9%) | G (n = 77, 16.7%) | Overall (n = 465) |
|---|---|---|---|---|---|---|---|---|
| 1994 Research | 58 (81.7%) | 45 (90.0%) | 58 (80.6%) | 64 (85.3%) | 39 (84.8%) | 57 (77.0%) | 67 (87.0%) | 388 (83.4%) |
| 2003 Canadian | 33 (46.5%) | 24 (48.0%) | 35 (48.6%) | 41 (54.7%) | 22 (47.8%) | 34 (45.9%) | 44 (57.4%) | 233 (50.1%) |
| 2015 IOM | 38 (53.5%) | 26 (52.0%) | 43 (59.7%) | 42 (56.0%) | 29 (63.0%) | 44 (59.5%) | 46 (59.7%) | 268 (57.6%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Unger, E.R.; Lin, J.-M.S.; Chen, Y.; Cornelius, M.E.; Helton, B.; Issa, A.N.; Bertolli, J.; Klimas, N.G.; Balbin, E.G.; Bateman, L.; et al. Heterogeneity in Measures of Illness among Patients with Myalgic Encephalomyelitis/Chronic Fatigue Syndrome Is Not Explained by Clinical Practice: A Study in Seven U.S. Specialty Clinics. J. Clin. Med. 2024, 13, 1369. https://doi.org/10.3390/jcm13051369
Unger ER, Lin J-MS, Chen Y, Cornelius ME, Helton B, Issa AN, Bertolli J, Klimas NG, Balbin EG, Bateman L, et al. Heterogeneity in Measures of Illness among Patients with Myalgic Encephalomyelitis/Chronic Fatigue Syndrome Is Not Explained by Clinical Practice: A Study in Seven U.S. Specialty Clinics. Journal of Clinical Medicine. 2024; 13(5):1369. https://doi.org/10.3390/jcm13051369
Chicago/Turabian StyleUnger, Elizabeth R., Jin-Mann S. Lin, Yang Chen, Monica E. Cornelius, Britany Helton, Anindita N. Issa, Jeanne Bertolli, Nancy G. Klimas, Elizabeth G. Balbin, Lucinda Bateman, and et al. 2024. "Heterogeneity in Measures of Illness among Patients with Myalgic Encephalomyelitis/Chronic Fatigue Syndrome Is Not Explained by Clinical Practice: A Study in Seven U.S. Specialty Clinics" Journal of Clinical Medicine 13, no. 5: 1369. https://doi.org/10.3390/jcm13051369
APA StyleUnger, E. R., Lin, J.-M. S., Chen, Y., Cornelius, M. E., Helton, B., Issa, A. N., Bertolli, J., Klimas, N. G., Balbin, E. G., Bateman, L., Lapp, C. W., Springs, W., Podell, R. N., Fitzpatrick, T., Peterson, D. L., Gottschalk, C. G., Natelson, B. H., Blate, M., Kogelnik, A. M., ... on behalf of the MCAM Study Group. (2024). Heterogeneity in Measures of Illness among Patients with Myalgic Encephalomyelitis/Chronic Fatigue Syndrome Is Not Explained by Clinical Practice: A Study in Seven U.S. Specialty Clinics. Journal of Clinical Medicine, 13(5), 1369. https://doi.org/10.3390/jcm13051369