
Long-COVID Prevalence and Its Association with Health Outcomes in the Post-Vaccine and Antiviral-Availability Era

 , , and
, , and
Abstract
1. Introduction
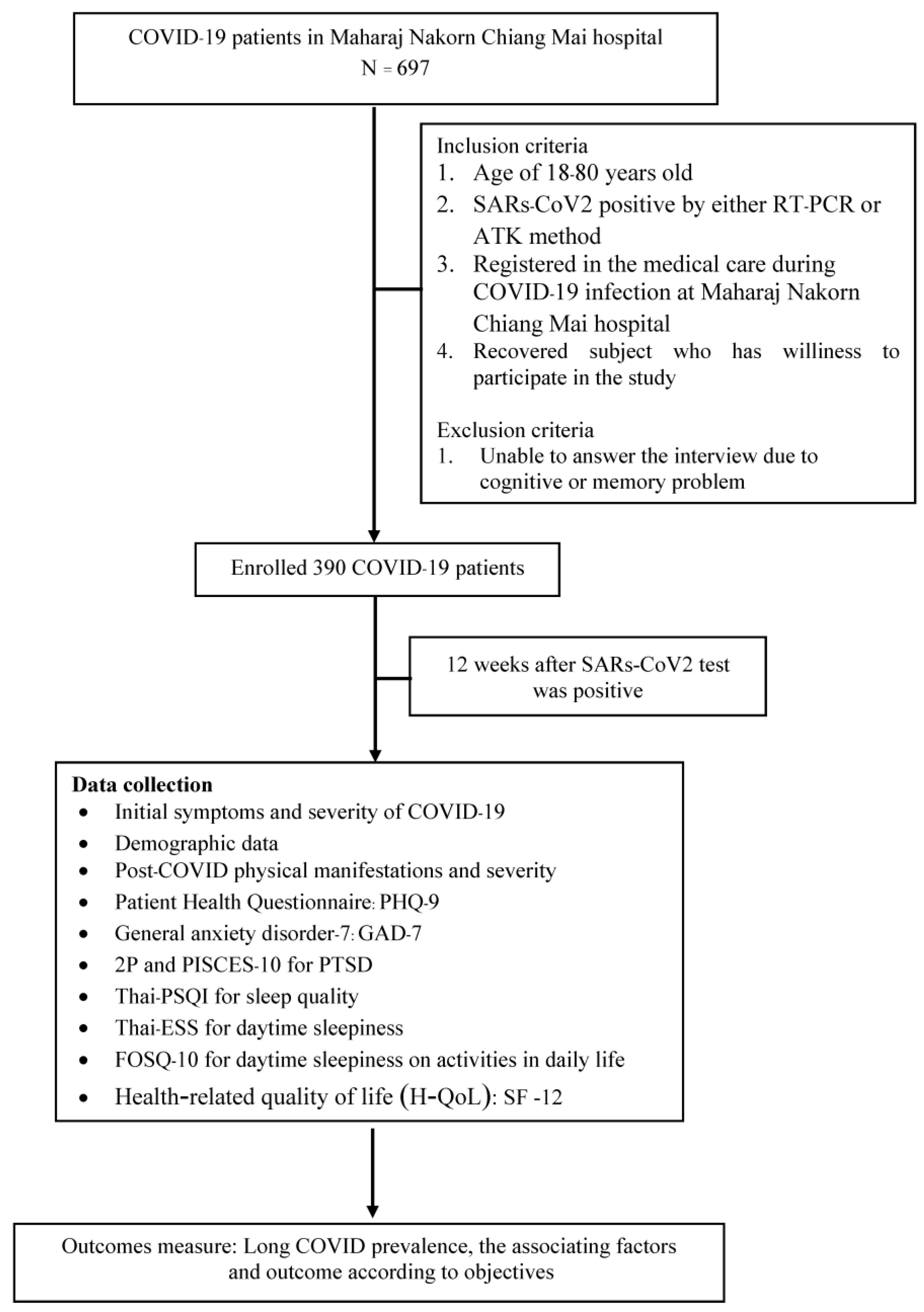
2. Method
2.1. Study Design
2.2. Data Collection
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Coronavirus Disease (COVID-19) 2021. Available online: https://www.who.int/health-topics/coronavirus#tab=tab_1 (accessed on 25 October 2021).
- Lopes-Pacheco, M.; Silva, P.L.; Cruz, F.F.; Battaglini, D.; Robba, C.; Pelosi, P.; Morales, M.M.; Caruso Neves, C.; Rocco, P.R.M. Pathogenesis of Multiple Organ Injury in COVID-19 and Potential Therapeutic Strategies. Front. Physiol. 2021, 12, 593223. [Google Scholar] [CrossRef] [PubMed]
- Guedj, E.; Campion, J.Y.; Dudouet, P.; Kaphan, E.; Bregeon, F.; Tissot-Dupont, H.; Guis, S.; Barthelemy, F.; Habert, P.; Ceccaldi, M.; et al. 18F-FDG brain PET hypometabolism in patients with long COVID. Eur. J. Nucl. Med. Mol. Imaging 2021, 48, 2823–2833. [Google Scholar] [CrossRef] [PubMed]
- Department of Disease Control, Ministry of Public Health. Situation Report in Thailand Coronavirus Disease 2019 (COVID-19) 2021. Available online: https://ddc.moph.go.th/viralpneumonia/index.php (accessed on 25 October 2021).
- Kamal, M.; Abo Omirah, M.; Hussein, A.; Saeed, H. Assessment and characterisation of post-COVID-19 manifestations. Int. J. Clin. Pract. 2021, 75, e13746. [Google Scholar] [CrossRef]
- World Health Organization. A Clinical Case Definition of Post COVID-19 Condition by a Delphi Consensus 2022. Available online: https://apps.who.int/iris/rest/bitstreams/1376291/retrieve (accessed on 16 November 2021).
- Kayaaslan, B.; Eser, F.; Kalem, A.K.; Kaya, G.; Kaplan, B.; Kacar, D.; Hasanoglu, I.; Coskun, B.; Guner, R. Post-COVID syndrome: A single-center questionnaire study on 1007 participants recovered from COVID-19. J. Med. Virol. 2021, 93, 6566–6574. [Google Scholar] [CrossRef] [PubMed]
- Pavli, A.; Theodoridou, M.; Maltezou, H.C. Post-COVID Syndrome: Incidence, Clinical Spectrum, and Challenges for Primary Healthcare Professionals. Arch. Med. Res. 2021, 52, 575–581. [Google Scholar] [CrossRef]
- Phu, D.H.; Maneerattanasak, S.; Shohaimi, S.; Trang, L.T.T.; Nam, T.T.; Kuning, M.; Like, A.; Torpor, H.; Suwanbamrung, C. Prevalence and factors associated with long COVID and mental health status among recovered COVID-19 patients in southern Thailand. PLoS ONE 2023, 18, e0289382. [Google Scholar] [CrossRef] [PubMed]
- Halpin, S.J.; McIvor, C.; Whyatt, G.; Adams, A.; Harvey, O.; McLean, L.; Walshaw, C.; Kemp, S.; Corrado, J.; Singh, R.; et al. Postdischarge symptoms and rehabilitation needs in survivors of COVID-19 infection: A cross-sectional evaluation. J. Med. Virol. 2021, 93, 1013–1022. [Google Scholar] [CrossRef] [PubMed]
- Garg, P.; Arora, U.; Kumar, A.; Wig, N. The “post-COVID” syndrome: How deep is the damage? J. Med. Virol. 2021, 93, 673–674. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. COVID-19 Situation, Thailand 16 March 2022. 2022. Available online: https://cdn.who.int/media/docs/default-source/searo/thailand/2022_03_16_tha-sitrep-227-covid-19.pdf (accessed on 6 November 2022).
- Chrisler, J.C. Chapter 14—Epilogue. In The Psychology of Gender and Health; Sánchez-López, M.P., Limiñana-Gras, R.M., Eds.; Academic Press: San Diego, CA, USA, 2017; pp. 401–405. [Google Scholar]
- Sugiyama, A.; Miwata, K.; Kitahara, Y.; Okimoto, M.; Abe, K.; E, B.; Ouoba, S.; Akita, T.; Tanimine, N.; Ohdan, H.; et al. Long COVID occurrence in COVID-19 survivors. Sci. Rep. 2022, 12, 6039. [Google Scholar] [CrossRef] [PubMed]
- Lotrakul, M.; Sumrithe, S.; Saipanish, R. Reliability and validity of the Thai version of the PHQ-9. BMC Psychiatry 2008, 8, 46. [Google Scholar] [CrossRef] [PubMed]
- Mental Health Crisis Assessment and Treatment Team (MCATT). Trial Manual. 2021. Available online: https://mhso.dmh.go.th/fileupload/20201006154069894.pdf (accessed on 1 October 2021).
- Theerakittikul, T.; Chaiard, J.; Deeluea, J. Sleep quality, daytime sleepiness and daytime functioning among Thai obstructive sleep apnea patients receiving continuous positive airway pressure therapy. J. Health Res. 2022, 36, 972–982. [Google Scholar] [CrossRef]
- Krittayaphong, R.; Bhuripanyo, K.; Raungratanaamporn, O.; Chotinaiwatarakul, C.; Chaowalit, N.; Punlee, K.; Kangkagate, C.; Chaithiraphan, S. Reliability of Thai version of SF-36 questionnaire for the evaluation of quality of life in cardiac patients. J. Med. Assoc. Thai. 2000, 83 (Suppl. 2), S130–S136. [Google Scholar] [PubMed]
- Tsampasian, V.; Elghazaly, H.; Chattopadhyay, R.; Debski, M.; Naing, T.K.P.; Garg, P.; Clark, A.; Ntatsaki, E.; Vassiliou, V.S. Risk Factors Associated with Post-COVID-19 Condition: A Systematic Review and Meta-analysis. JAMA Intern. Med. 2023, 183, 566–580. [Google Scholar] [CrossRef] [PubMed]
- Carvalho-Schneider, C.; Laurent, E.; Lemaignen, A.; Beaufils, E.; Bourbao-Tournois, C.; Laribi, S.; Flament, T.; Ferreira-Maldent, N.; Bruyère, F.; Stefic, K.; et al. Follow-up of adults with noncritical COVID-19 two months after symptom onset. Clin. Microbiol. Infect. 2021, 27, 258–263. [Google Scholar] [CrossRef] [PubMed]
- Makboon, K.; Intree, S.; Sreedee, S.; Mungme, K.; Komonmusik, K.; Samnao, R. Factors Relating to Post Discharge Persistence of Symptoms After Hospitalization Among Persons with Coronavirus Disease 2019. J. Health Nurs. Educ. 2022, 17, 125–136. [Google Scholar]


{kind=link}
{kind=link}
{kind=link}
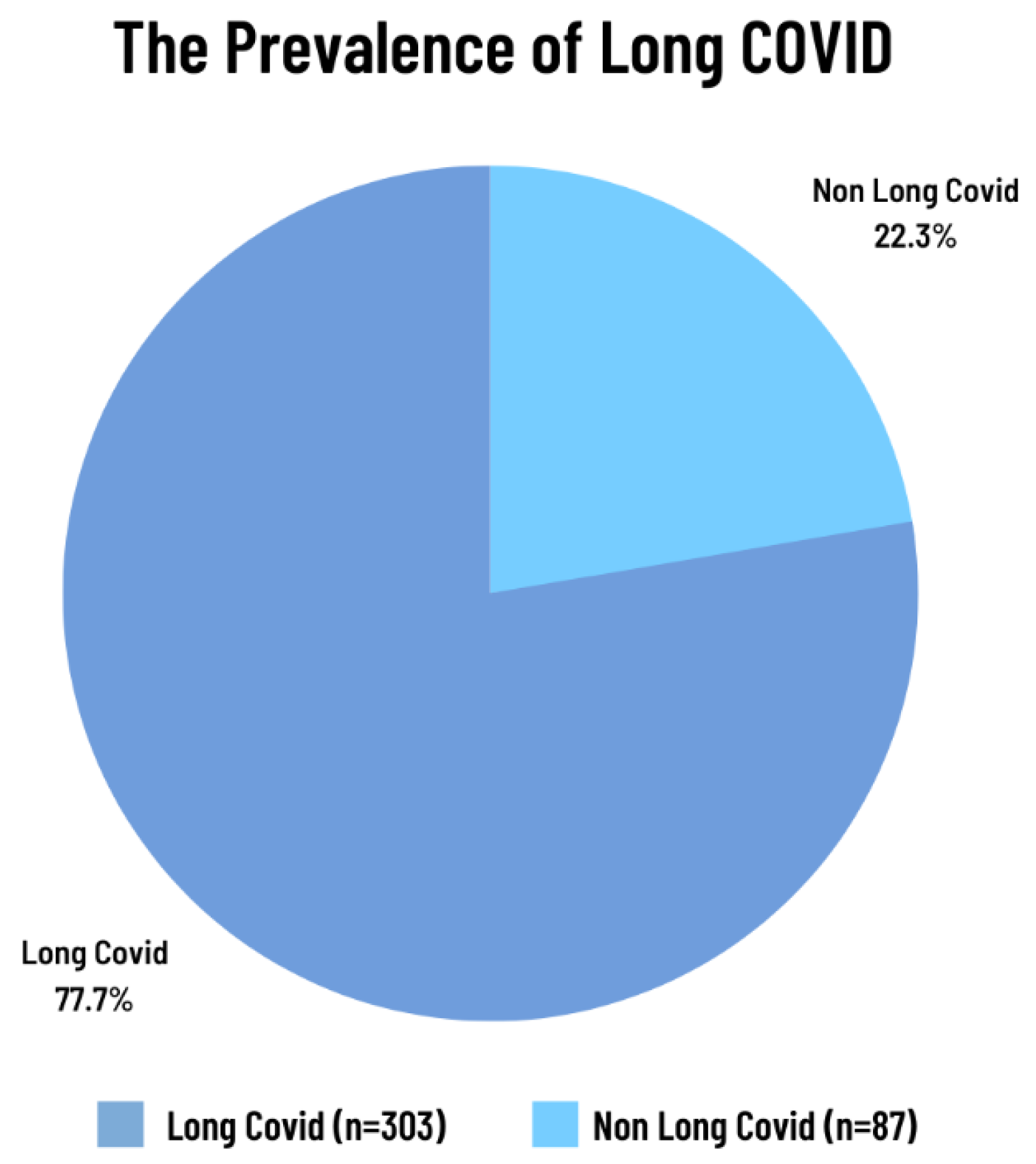
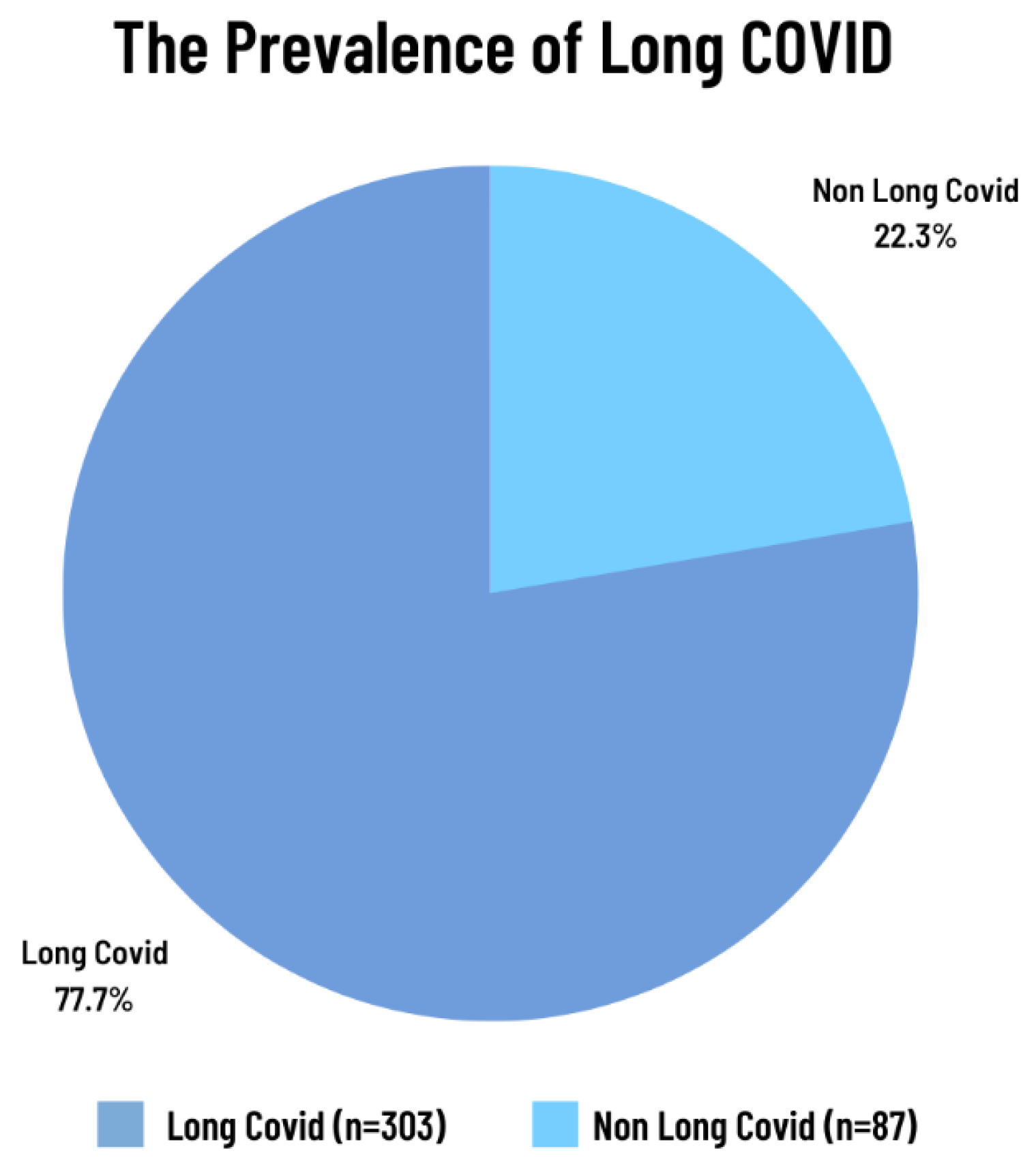
| Variable | Total | Long COVID (n = 390) | p-Value | |
|---|---|---|---|---|
| Yes (n = 303) | No (n = 87) | |||
| Age, (y) Mean ± SD | 31.8 ± 13.6 | 31.7 ± 14.8 | 31.8 ± 13.2 | 0.431 |
| Male gender, N (%) | 173 (44.4) | 128 (42.2) | 45 (51.7) | 0.074 |
| BMI, N (%) | 0.281 | |||
| Underweight <18.5 | 43 (11.0) | 29 (9.6) | 14 (16.1) | |
| Normal (18.5–24.9) | 233 (59.7) | 181 (59.7) | 52 (59.8) | |
| Overweight (25–29.9) | 76 (19.5) | 61 (20.1) | 15 (17.2) | |
| Obesity (>30) | 38 (9.7) | 32 (10.6) | 6 (6.9) | |
| Co-morbidities, N (%) | 159 (40.8) | |||
| Obesity (>30) | 38 (9.7) | 32 (10.6) | 6 (6.9) | 0.212 |
| Allergic rhinitis | 34 (8.7) | 28 (9.2) | 6 (6.9) | 0.33 |
| Hypertension | 33 (8.5) | 27 (8.9) | 6 (6.9) | 0.365 |
| Dyslipidemia | 27 (6.9) | 23 (7.6) | 4 (4.6) | 0.239 |
| Cerebrovascular disease | 16 (4.1) | 11 (3.6) | 5 (5.7) | 0.273 |
| Diabetes mellitus | 12 (3.1) | 11 (3.6) | 1 (1.1) | 0.211 |
| Respirator disease | 12 (3.1) | 8 (2.6) | 4 (4.6) | 0.268 |
| Chronic kidney disease | 10 (2.6) | 7 (2.3) | 3 (3.4) | 0.393 |
| Gastrointestinal disease | 4 (1) | 4 (1.3) | 0 | 0.363 |
| Major depressive disorder | 4 (1) | 4 (1.3) | 0 | 0.363 |
| History of COVID-19 Vaccination, N (%) | 377 (96.7) | 295 (97.4) | 82 (94.3) | 0.14 |
| 1 shot | 7 (1.8) | |||
| 2 shots | 158 (40.5) | |||
| 3 shots | 116 (29.7) | |||
| 4 shots | 96 (24.6) | |||
| Initial symptom during COVID-19 infection, N (%) | ||||
| Cough | 175 (44.9) | 144 (47.5) | 31 (36.5) | 0.049 |
| Sore throat | 135 (34.6) | 106 (35) | 29 (33.3) | 0.766 |
| Rhinorrhea | 69 (17.7) | 55 (18.2) | 14 (16.1) | 0.657 |
| Fever | 65 (16.7) | 48 (15.8) | 17 (19.5) | 0.253 |
| Sputum | 40 (10.3) | 30 (9.9) | 10 (11.5) | 0.666 |
| Fatigue | 13 (3.3) | 10 (3.3) | 3 (3.4) | 0.584 |
| Headache | 11 (2.8) | 9 (3) | 2 (2.3) | 0.739 |
| Chest tight | 9 (2.3) | 9 (3) | 0 | 0.217 |
| Anosmia | 7 (1.8) | 6 (2) | 1 (1.1) | 0.607 |
| Myalgia | 6 (1.5) | 5 (1.7) | 1 (1.1) | 0.738 |
| Pneumonia | 21 (5.4) | 19 (6.3) | 2 (2.3) | 0.185 |
| Nasal congestion | 5 (1.3) | 3 (1) | 2 (2.3) | 0.310 |
| Receiving anti-viral drug during disease, N (%) | 383 (98.2) | 297 (98.3) | 86 (98.9) | 0.597 |
| Receiving O2 therapy during disease, N (%) | 14 (3.6) | 0.804 | ||
| Nasal canular | 11 (2.8) | 9 (3) | 2 (2.3) | |
| Non invasive | 2 (0.5) | 2 (0.7) | 0 | |
| Mechanical ventilator | 1 (0.3) | 1 (0.3) | 0 | |
| Mental Symptoms: Parameters | Total (n = 390) n (%) | Long COVID | p-Value | |
|---|---|---|---|---|
| Yes | No | |||
| Depression: PHQ-9 | ||||
| None to minimal (0–4) | 357 (91.8) | 270 (89.1) | 87 (100) | 0.035 |
| Mild (5–9) | 17 (4.4) | 17 (5.6) | 0 | |
| Moderate (10–14) | 13 (3.3) | 13 (4.3) | 0 | |
| Moderately severe (15–19) | 2 (0.5) | 2 (0.7) | 0 | |
| Anxiety: GAD-7 | ||||
| No anxiety | 257 (65.9) | 182 (60.1) | 75 (86.2) | <0.001 |
| Minimal (1–4) | 117 (30.0) | 105 (34.7) | 12 (13.8) | |
| Mild (5–9) | 11 (2.8) | 11 (3.6) | 0 | |
| Moderate (10–14) | 5 (1.3) | 5 (1.7) | 0 | |
| Severe (≥15) | 0 | 0 | 0 | |
| PTSD: 2P, PISCES-10 | ||||
| No | 3 (0.8) | 3 (0.8) | 0 | |
| Yes | 1 (0.3) | 1 (0.3) | 0 | |
| Sleep quality: Thai-PSQI | ||||
| Normal | 258 (66.7) | 187 (61.9) | 71 (83.5) | <0.001 |
| Poor | 129 (33.3) | 115 (38.1) | 14 (16.5) | |
| Daytime sleepiness: Thai-ESS | ||||
| Lower normal daytime symptoms (0–5) | 316 (81) | 242.0 (79.9) | 74 (85.1) | 0.390 |
| Higher normal daytime symptoms (6–10) | 65 (16.7) | 52.0 (17.2) | 13 (14.9) | |
| Mild excessive daytime symptoms (11–12) | 6 (1.5) | 6.0 (2) | 0 | |
| Moderate excessive daytime symptoms (13–15) | - | 0 | 0 | |
| Severe excessive daytime symptoms (16–24) | 3 (0.8) | 3.0(1.0) | 0 | |
| Daytime function: FOSQ-10 | ||||
| Normal | 387 (99.2) | 300 (99.0) | 87 (100) | 0.351 |
| Poor (<18) | 3 (0.8) | 3.0 (1.0) | 0 | |
| H-QoL: SF-12 (Mean ± SD) | 49.0 ± 4.0 | |||
| Physical | 83.25 ± 11.75 | 81.38 ± 12.37 | 89.77 ± 5.65 | <0.001 |
| Mental | 82.30 ± 8.50 | 81.30 ± 8.87 | 85.78 ± 5.92 | <0.001 |
| Univariable Logistic Regression | Multivariable Logistic Regression | |||||
|---|---|---|---|---|---|---|
| Variable | OR | 95% CI | p-Value | OR | 95% CI | p-Value |
| Sex | 1.465 | 0.908–2.363 | 0.118 | 1.431 | 0.874–2.344 | 0.154 |
| Age (y) | ||||||
| <60 | Ref. | Ref. | ||||
| ≥60 | 0.471 | 0.180–1.236 | 0.126 | 0.299 | 0.094–0.955 | 0.042 |
| Comorbidity | ||||||
| Participant with ≥ 1 disease | 1.605 | 0.969–2.656 | 0.066 | 1.635 | 0.957–2.794 | 0.072 |
| 1. Hypertension | 1.321 | 0.527–3.309 | 0.553 | |||
| 2. Diabetes Mellitus | 3.24 | 0.412–25.449 | 0.264 | |||
| 3. Dyslipidemia | 1.704 | 0.573–5.068 | 0.337 | |||
| 4. Allergic rhinitis | 1.375 | 0.55–3.435 | 0.496 | |||
| 5. Anemia | 1.151 | 0.127–10.429 | 0.901 | |||
| 6. Hyperthyroid | 1.761 | 0.209–14.828 | 0.603 | |||
| 7. Chronic kidney disease | 0.662 | 0.168–2.616 | 0.557 | |||
| 8. Respiratory | 0.563 | 0.165–1.915 | 0.357 | |||
| 9. Gout | 0.425 | 0.070–2.585 | 0.353 | |||
| 10. Cerebrovascular disease | 0.618 | 0.209–1.829 | 0.384 | |||
| 11. Obesity | 1.594 | 0.644–3.947 | 0.313 | |||
| COVID symptoms | ||||||
| Symptomatic COVID ≥ 1 symptom | 1.318 | 0.802–2.164 | 0.213 | 0.737 | 0.385–1.412 | 0.359 |
| Cough | 1.636 | 0.999–2.679 | 0.05 | 1.911 | 1.015–3.598 | 0.045 |
| Fever | 0.775 | 0.420–1.431 | 0.415 | |||
| Sore throat | 1.076 | 0.650–1.782 | 0.776 | |||
| Sputum | 0.846 | 0.396–1.808 | 0.666 | |||
| Rhinorrhea | 1.156 | 0.608–2.198 | 0.657 | |||
| Anosmia | 1.737 | 0.206–14.628 | 0.611 | |||
| Fatigue | 0.956 | 0.257–3.552 | 0.946 | |||
| Headache | 1.301 | 0.276–6.136 | 0.739 | |||
| Myalgia | 1.443 | 0.166–12.517 | 0.739 | |||
| Nasal congestion | 0.425 | 0.070–2.585 | 0.353 | |||
| Pneumonia | 2.843 | 0.650–12.453 | 0.166 | 2.044 | 0.528–7.907 | 0.065 |
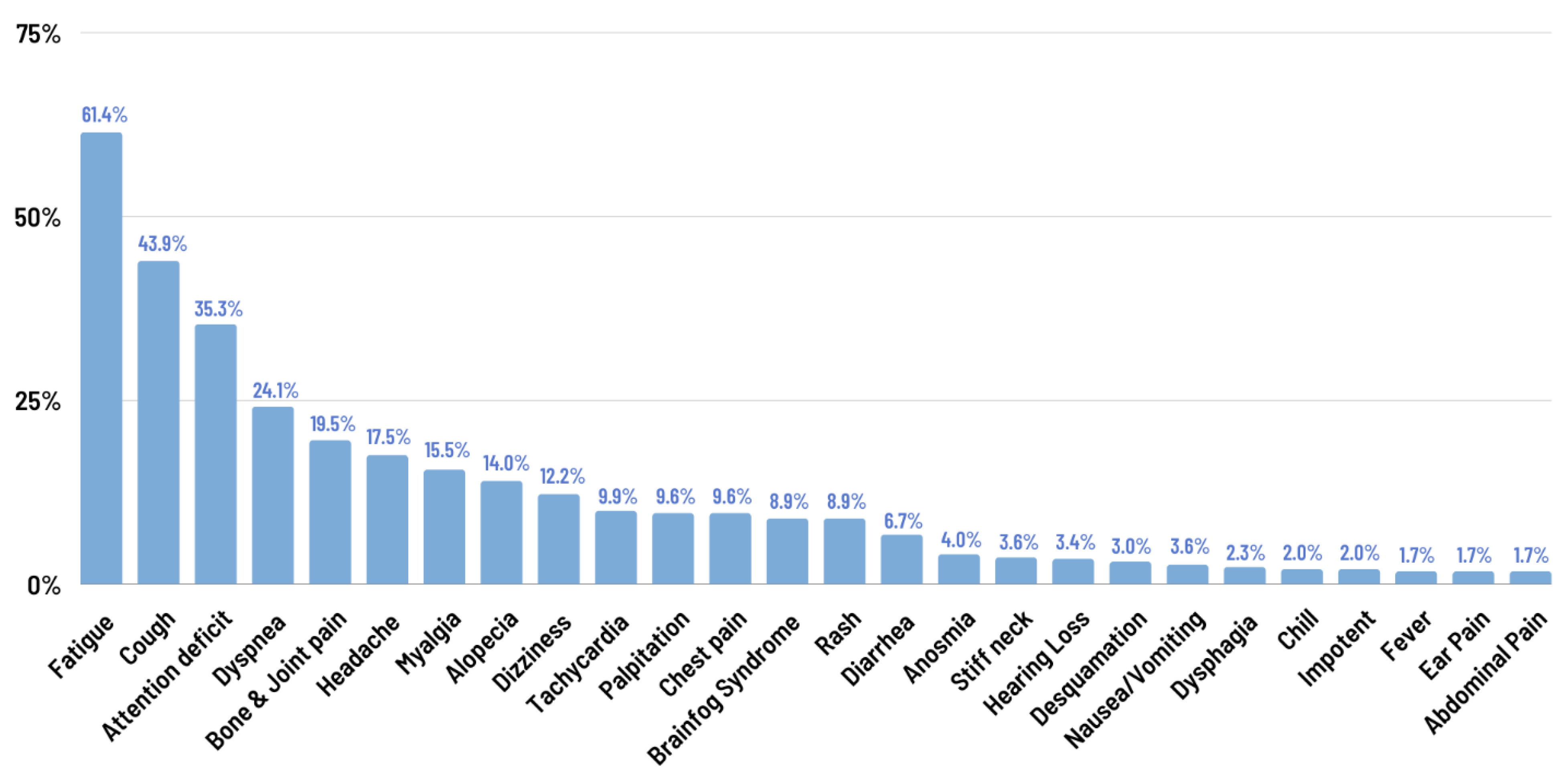
| Physical Symptoms | Long COVID (n = 303), n (%) | Female (n = 175), n (%) | Male (n = 128), n (%) | OR | 95% CI | p-Value |
|---|---|---|---|---|---|---|
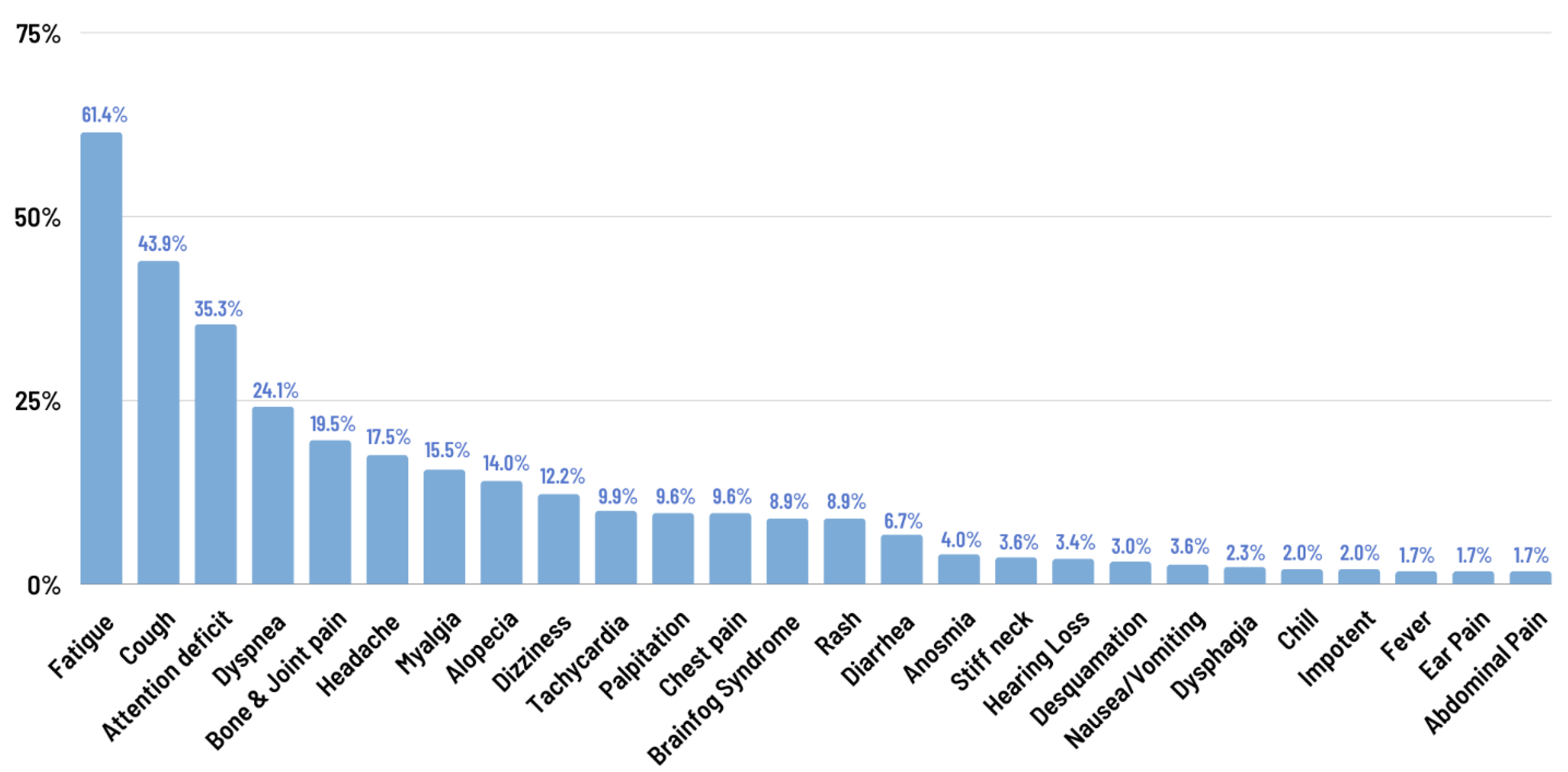
| Fatigue | 186 (61.4) | 110 (62.9) | 76 (59.4) | |||
| Cough | 133 (43.9) | 81 (46.3) | 52 (40.6) | |||
| Dyspnea | 73 (24.1) | 42 (24.0) | 31 (24.2) | |||
| Headache | 53 (17.5) | 41 (23.4) | 12 (9.4) | 0.338 | (0.170, 0.674) | 0.001 |
| Dizziness | 37 (12.2) | 29 (16.6) | 8 (6.3) | 0.336 | (0.148, 0.761) | 0.007 |
| Brain fog syndrome | 27 (8.9) | 22 (12.6) | 5 (3.9) | 0.283 | (0.104, 0.768) | 0.013 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jangnin, R.; Ritruangroj, W.; Kittisupkajorn, S.; Sukeiam, P.; Inchai, J.; Maneeton, B.; Maneetorn, N.; Chaiard, J.; Theerakittikul, T. Long-COVID Prevalence and Its Association with Health Outcomes in the Post-Vaccine and Antiviral-Availability Era. J. Clin. Med. 2024, 13, 1208. https://doi.org/10.3390/jcm13051208
Jangnin R, Ritruangroj W, Kittisupkajorn S, Sukeiam P, Inchai J, Maneeton B, Maneetorn N, Chaiard J, Theerakittikul T. Long-COVID Prevalence and Its Association with Health Outcomes in the Post-Vaccine and Antiviral-Availability Era. Journal of Clinical Medicine. 2024; 13(5):1208. https://doi.org/10.3390/jcm13051208
Chicago/Turabian StyleJangnin, Ramida, Worraya Ritruangroj, Sirada Kittisupkajorn, Pattarapa Sukeiam, Juthamas Inchai, Benchalak Maneeton, Narong Maneetorn, Jindarat Chaiard, and Theerakorn Theerakittikul. 2024. "Long-COVID Prevalence and Its Association with Health Outcomes in the Post-Vaccine and Antiviral-Availability Era" Journal of Clinical Medicine 13, no. 5: 1208. https://doi.org/10.3390/jcm13051208
APA StyleJangnin, R., Ritruangroj, W., Kittisupkajorn, S., Sukeiam, P., Inchai, J., Maneeton, B., Maneetorn, N., Chaiard, J., & Theerakittikul, T. (2024). Long-COVID Prevalence and Its Association with Health Outcomes in the Post-Vaccine and Antiviral-Availability Era. Journal of Clinical Medicine, 13(5), 1208. https://doi.org/10.3390/jcm13051208