
Pregnancy Arrhythmias: Management in the Emergency Department and Critical Care

 ,
,  ,
,
Abstract
1. Introduction
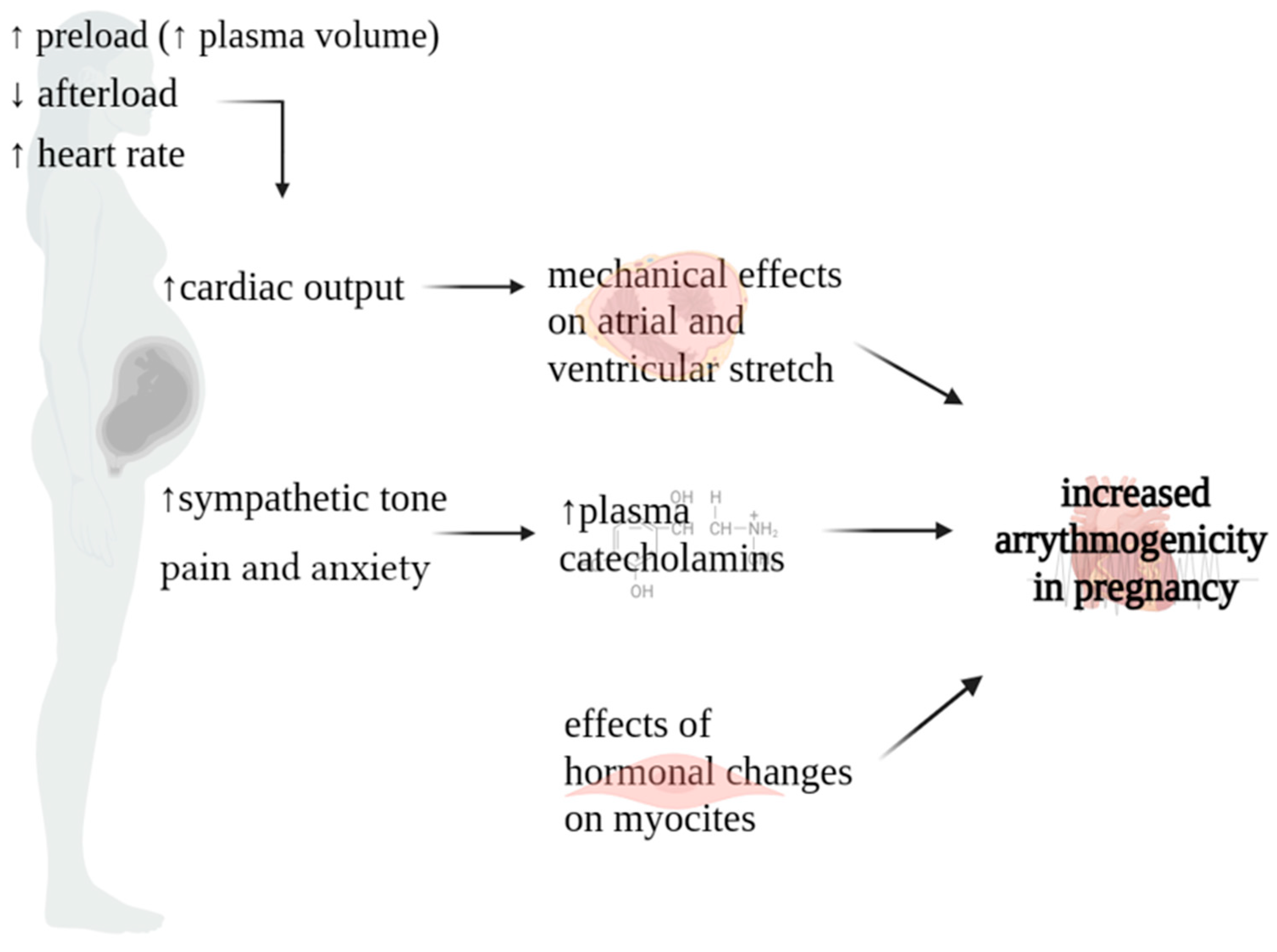
2. Pathophysiology of Arrythmias in Pregnancy
3. Echocardiographic and Electrocardiographic Changes during Pregnancy
3.1. Echocardiographic Changes
3.2. Electrocardiographic Changes
4. Pharmacotherapy and Cardiological Procedures during Pregnancy and Lactation
4.1. Beta-Blockers (FDA Class C)
4.2. Calcium Channel Blockers (FDA Class C)
4.3. Class IA AADs (FDA Class C)
4.4. Class IB AADs
4.5. Class IC AADs (FDA Class C)
4.6. Class III AADs
4.7. Other Antiarrhythmic Drugs
4.8. Electrical Synchronized Cardioversion
4.9. Electrophysiology Procedures
5. Management of Different Types of Arrhythmias in Pregnancy
5.1. Premature Beats
5.2. Inappropriate Sinus Tachycardia
5.3. Atrial Fibrillation and Atrial Flutter
5.4. Supraventricular Tachycardia
5.5. Ventricular Arrhythmias
5.6. Bradyarrhythmias
5.7. Cardiac Arrest in Pregnancy
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Williams, D.S.; Mikhova, K.; Sodhi, S. Arrhythmias and Pregnancy: Management of Preexisting and New-Onset Maternal Arrhythmias. Cardiol. Clin. 2021, 39, 67–75. [Google Scholar] [CrossRef] [PubMed]
- Tamirisa, K.P.; Elkayam, U.; Briller, J.E.; Mason, P.K.; Pillarisetti, J.; Merchant, F.M.; Patel, H.; Lakkireddy, D.R.; Russo, A.M.; Volgman, A.S.; et al. Arrhythmias in Pregnancy. JACC Clin. Electrophysiol. 2022, 8, 120–135. [Google Scholar] [CrossRef]
- Vaidya, V.R.; Arora, S.; Patel, N.; Badheka, A.O.; Patel, N.; Agnihotri, K.; Billimoria, Z.; Turakhia, M.P.; Friedman, P.A.; Madhavan, M.; et al. Burden of arrhythmia in pregnancy. Circulation 2017, 135, 619–621. [Google Scholar] [CrossRef] [PubMed]
- Briller, J.; Koch, A.R.; Geller, S.E. Illinois Department of Public Health Maternal Mortality Review Committee Working Group. Maternal cardiovascular mortality in Illinois, 2002–2011. Obstet. Gynecol. 2017, 129, 819–826. [Google Scholar] [CrossRef] [PubMed]
- Lima, F.V.; Yang, J.; Xu, J.; Stergiopoulos, K. National Trends and in-hospital outcomes in pregnant women with heart disease in the United States. Am. J. Cardiol. 2017, 119, 1694–1700. [Google Scholar] [CrossRef]
- Opotowsky, A.R.; Siddiqi, O.K.; D’Souza, B.; Webb, G.D.; Fernandes, S.M.; Landzberg, M.J. Maternal cardiovascular events during childbirth among women with congenital heart disease. Heart 2012, 98, 145–151. [Google Scholar] [CrossRef]
- Silversides, C.K.; Grewal, J.; Mason, J.; Sermer, M.; Kiess, M.; Rychel, V.; Wald, R.M.; Colman, J.M.; Siu, S.C. Pregnancy outcomes in women with heart disease: The CARPREG II study. J. Am. Coll. Cardiol. 2018, 71, 2419–2430. [Google Scholar] [CrossRef]
- Fu, Q.; Lin, J. Risk factors for heart failure during pregnancy among Chinese women with cardiac disease. Int. J. Gynecol. Obstet. 2015, 130, 266–269. [Google Scholar] [CrossRef]
- Rashba, E.J.; Zareba, W.; Moss, A.J.; Hall, W.J.; Robinson, J.; Locati, E.H.; Schwartz, P.J.; Andrews, M. Influence of Pregnancy on the Risk for Cardiac Events in Patients With Hereditary Long QT Syndrome. Circulation 1998, 97, 451–456. [Google Scholar] [CrossRef]
- Ishibashi, K.; Aiba, T.; Kamiya, C.; Miyazaki, A.; Sakaguchi, H.; Wada, M.; Nakajima, I.; Miyamoto, K.; Okamura, H.; Noda, T.; et al. Arrhythmia risk and Beta-blocker therapy in pregnant women with long QT syndrome. Heart 2017, 103, 1374–1379. [Google Scholar] [CrossRef]
- Adamson, D.L.; Nelson-Piercy, C. Managing palpitations and arrhythmias during pregnancy. Heart 2007, 93, 1630–1636. [Google Scholar] [CrossRef] [PubMed]
- Wong, A.Y.; Kulandavelu, S.; Whiteley, K.J.; Qu, D.; Langille, B.L.; Adamson, S.L. Maternal cardiovascular changes during pregnancy and postpartum in mice. Am. J. Physiol. Heart Circ. Physiol. 2002, 282, H918–H925. [Google Scholar] [CrossRef] [PubMed]
- Abbas, A.E.; Lester, S.J.; Connolly, H. Pregnancy and the cardiovascular system. Int. J. Cardiol. 2005, 98, 179–189. [Google Scholar] [CrossRef] [PubMed]
- Sanghavi, M.; Rutherford, J.D. Cardiovascular physiology of pregnancy. Circulation 2014, 130, 1003–1008. [Google Scholar] [CrossRef] [PubMed]
- Morton, A. Physiological Changes and Cardiovascular Investigations in Pregnancy. Heart Lung Circ. 2021, 30, e6. [Google Scholar] [CrossRef] [PubMed]
- Conrad, K.P. Emerging role of relaxin in the maternal adaptations to normal pregnancy: Implications for preeclampsia. Semin. Nephrol. 2011, 31, 15–32. [Google Scholar] [CrossRef] [PubMed]
- Osol, G.; Ko, N.L.; Mandala, M. Plasticity of the maternal vasculature during pregnancy. Annu. Rev. Physiol. 2019, 81, 89–111. [Google Scholar] [CrossRef]
- Green, L.J.B.; Mackillop, L.H.M.; Salvi, D.; Pullon, R.; Loerup, L.; Tarassenko, L.; Mossop, J.B.; Edwards, C.B.; Gerry, S.M.; Birks, J.M.; et al. Gestation-Specific Vital Sign Reference Ranges in Pregnancy. Obstet. Gynecol. 2020, 135, 653. [Google Scholar] [CrossRef]
- Angeli, F.; Angeli, E.; Verdecchia, P. Novel Electrocardiographic Patterns for the Prediction of Hypertensive Disorders of Pregnancy—From Pathophysiology to Practical Implications. Int. J. Mol. Sci. 2015, 16, 18454–18473. [Google Scholar] [CrossRef]
- Wang, Y.; Joyner, R.W.; Wagner, M.B.; Cheng, J.; Lai, D.; Crawford, B.H. Stretch-activated channel activation promotes early afterdepolarizations in rat ventricular myocytes under oxidative stress. Am. J. Physiol. Heart Circ. Physiol. 2009, 296, H1227–H1235. [Google Scholar] [CrossRef]
- Enriquez, A.D.; Economy, K.E.; Tedrow, U.B. Contemporary management of arrhythmias during pregnancy. Circ. Arrhythm. Electrophysiol. 2014, 7, 96. [Google Scholar] [CrossRef]
- Ekholm, E.M.; Erkkola, R.U. Autonomic cardiovascular control in pregnancy. Eur. J. Obstet. Gynecol. Reprod. Biol. 1996, 64, 29–36. [Google Scholar] [CrossRef]
- Shen, M.J.; Zipes, D.P. Role of the autonomic nervous system in modulating cardiac arrhythmias. Circ. Res. 2014, 114, 1004–1021. [Google Scholar] [CrossRef]
- Vaseghi, M.; Shivkumar, K. The role of the autonomic nervous system in sudden cardiac death. Prog. Cardiovasc. Dis. 2008, 50, 404–419. [Google Scholar] [CrossRef]
- Wu, P.; Vaseghi, M. The autonomic nervous system and ventricular arrhythmias in myocardial infarction and heart failure. Pacing Clin. Electrophysiol. 2020, 43, 172–180. [Google Scholar] [CrossRef] [PubMed]
- Barron, W.M.; Mujais, S.K.; Zinaman, M.; Bravo, E.L.; Lindheimer, M.D. Plasma catecholamine responses to physiologic stimuli in normal human pregnancy. Am. J. Obstet. Gynecol. 1986, 154, 80–84. [Google Scholar] [CrossRef] [PubMed]
- Roberts, J.M.; Insel, P.A.; Goldfien, A. Regulation of myometrial adrenoreceptors and adrenergic response by sex steroids. Mol. Pharmacol. 1981, 20, 52–58. [Google Scholar] [PubMed]
- Robson, S.C.; Hunter, S.; Boys, R.J.; Dunlop, W. Serial study of factors influencing changes in cardiac output during human pregnancy. Am. J. Physiol. 1989, 256, H1060. [Google Scholar] [CrossRef]
- Curtis, S.L.; Belham, M.; Bennett, S.; James, R.; Harkness, A.; Gamlin, W.; Thilaganathan, B.; Giorgione, V.; Douglas, H.; Carroll, A.; et al. Transthoracic Echocardiographic Assessment of the Heart in Pregnancy-a position statement on behalf of the British Society of Echocardiography and the United Kingdom Maternal Cardiology Society. Echo Res. Pract. 2023, 10, 7. [Google Scholar] [CrossRef] [PubMed]
- O’Kelly, A.C.; Sharma, G.; Vaught, A.J.; Zakaria, S. The Use of Echocardiography and Advanced Cardiac Ultrasonography During Pregnancy. Curr. Treat. Options Cardiovasc. Med. 2019, 21, 71. [Google Scholar] [CrossRef] [PubMed]
- Eghbali, M.; Deva, R.; Alioua, A.; Minosyan, T.Y.; Ruan, H.; Wang, Y.; Toro, L.; Stefani, E. Molecular and functional signature of heart hypertrophy during pregnancy. Circ. Res. 2005, 96, 1208. [Google Scholar] [CrossRef] [PubMed]
- Ristić, A.D.; Seferović, P.M.; Ljubić, A.; Jovanović, I.; Ristić, G.; Pankuweit, S.; Ostojić, M.; Maisch, B. Pericardial disease in pregnancy. Herz 2003, 28, 209. [Google Scholar] [CrossRef] [PubMed]
- Joglar, J.A.; Page, R.L. Management of arrhythmia syndromes during pregnancy. Curr. Opin. Cardiol. 2014, 29, 36. [Google Scholar] [CrossRef]
- Tanindi, A.; Akgun, N.; Pabuccu, E.G.; Gursoy, A.Y.; Yüce, E.; Tore, H.F.; Duvan, C.I. Electrocardiographic P-wave duration, QT interval, T peak to end interval and Tp-e/QT ratio in pregnancy with respect to trimesters. Ann. Noninvas Electrocardiol. 2016, 21, 169–174. [Google Scholar] [CrossRef]
- Kandzia, T.; Markiewicz-Łoskot, G.; Binkiewicz, P. Tpeak-Tend Interval during Pregnancy and Postpartum. Int. J. Environ. Res. Public. Health 2022, 19, 12638. [Google Scholar] [CrossRef]
- Lechmanová, M.; Kittnar, O.; Mlček, M.; Slavíček, J.; Dohnalová, A.; Havranek, S.; Kolařík, J.; Pařízek, A. QT dispersion and T-loop morphology in late pregnancy and after delivery. Physiol. Res. 2002, 51, 121–129. [Google Scholar] [CrossRef]
- Zamani, M.; Esmailian, M.; Yoosefian, Z. QT interval in pregnant and non-pregnant women. Emergency 2014, 2, 22–25. [Google Scholar]
- Yamaguchi, M.; Shimizu, M.; Ino, H.; Terai, H.; Uchiyama, K.; Oe, K.; Mabuchi, T.; Konno, T.; Kaneda, T.; Mabuchi, H. T wave. peak-to-end interval and QT dispersion in acquired long QT syndrome: A new index for arrhythmogenicity. Clin. Sci. 2003, 105, 671–676. [Google Scholar] [CrossRef]
- Yagishita, D.; Chui, R.W.; Yamakawa, K.; Rajendran, P.S.; Ajijola, O.A.; Nakamura, K.; So, E.L.; Mahajan, A.; Shivkumar, K.; Vaseghi, M. Sympathetic nerve stimulation, not circulating norepinephrine, modulates T-peak to T-end interval by increasing global dispersion of repolarization. Circ. Arrhythm. Electrophysiol. 2015, 8, 174–185. [Google Scholar] [CrossRef]
- Akboga, M.K. Tp-e interval and Tp-e/QTc ratio as novel surrogate markers for prediction of ventricular arrhythmic events in hypertrophic cardiomyopathy. Anatol. J. Cardiol. 2017, 18, 48–53. [Google Scholar] [CrossRef]
- Longhitano, Y.; Bottinelli, M.; Pappalardo, F.; Maj, G.; Audo, A.; Srejic, U.; Rasulo, F.A.; Zanza, C. Electrocardiogram alterations in non-traumatic brain injury: A systematic review. J. Clin. Monit. Comput. 2023. [Google Scholar] [CrossRef]
- Costantine, M.M. Physiologic and pharmacokinetic changes in pregnancy. Front. Pharmacol. 2014, 5, 65. [Google Scholar] [CrossRef] [PubMed]
- Joglar, J.A.; Kapa, S.; Saarel, E.V.; Dubin, A.M.; Gorenek, B.; Hameed, A.B.; Lara de Melo, S.; Leal, M.A.; Mondésert, B.; Pacheco, L.D.; et al. 2023 HRS expert consensus statement on the management of arrhythmia during pregnancy. Heart Rhythm 2023, 20, e175–e264. [Google Scholar] [CrossRef]
- Schoenfeld, N.; Epstein, O.; Rosen, M.; Atsmon, A. Effects of propranolol during pregnancy and development of rats. II. Adverse effects on development. Eur. J. Pediatr. 1985, 143, 194–195. [Google Scholar] [CrossRef] [PubMed]
- Bateman, B.T.; Patorno, E.; Desai, R.J.; Seely, E.W.; Mogun, H.; Maeda, A.; Fischer, M.A.; Hernandez-Diaz, S.; Huybrechts, K.F. Late pregnancy beta blocker exposure and risks of neonatal hypoglycemia and bradycardia. Pediatrics 2016, 138, e20160731. [Google Scholar] [CrossRef] [PubMed]
- CA, F.; Steiner, M.F.; Aucott, L.; Pell, J.P.; Mackay, D.F.; Fleming, M.; McLay, J.S. In-utero exposure to antihypertensive medication and neonatal and child health outcomes: A systematic review. J. Hypertens 2017, 35, 2123–2137. [Google Scholar]
- Jannet, D.; Carbonne, B.; Sebban, E.; Milliez, J. Nicardipine versus metoprolol in the treatment of hypertension during pregnancy: A randomized comparative trial. Obstet. Gynecol. 1994, 84, 354–359. [Google Scholar] [PubMed]
- Livingstone, I.; Craswell, P.W.; Bevan, E.B.; Smith, M.T.; Eadie, M.J. Propranolol in pregnancy three year prospective study. Clin. Exp. Hypertension. Part B Hypertens. Pregnancy 1983, 2, 341–350. [Google Scholar] [CrossRef]
- Magee, L.A.; Elran, E.; Bull, S.B.; Logan, A.; Koren, G. Risks and benefits of beta-receptor blockers for pregnancy hypertension: Overview of the randomized trials. Eur. J. Obstet. Gynecol. Reprod. Biol. 2000, 88, 15–26. [Google Scholar] [CrossRef]
- Eliahou, H.E.; Silverberg, D.S.; Reisin, E.; Romem, I.; Mashiach, S.; Serr, D.M. Propranolol for the treatment of hypertension in pregnancy. Br. J. Obstet. Gynaecol. 1978, 85, 431–436. [Google Scholar] [CrossRef]
- Grewal, J.; Siu, S.C.; Lee, T.; D’souza, R.; Dvir, M.; Singer, J.; Rychel, V.; Kiess, M.; Sermer, M.; Silversides, C.K. Impact of betablockers on birth weight in a high-risk cohort of pregnant women with CVD. J. Am. Coll. Cardiol. 2020, 75, 2751–2752. [Google Scholar] [CrossRef]
- Fox, R.E.; Marx, C.; Stark, A.R. Neonatal effects of maternal nadolol therapy. Am. J. Obstet. Gynecol. 1985, 152, 1045–1046. [Google Scholar] [CrossRef]
- Lip, G.Y.; Beevers, M.; Churchill, D.; Shaffer, L.M.; Beevers, D.G. Effect of atenolol on birth weight. Am. J. Cardiol. 1997, 79, 1436–1438. [Google Scholar] [CrossRef]
- Lydakis, C.; Lip, G.Y.; Beevers, M.; Beevers, D.G. Atenolol and fetal growth in pregnancies complicated by hypertension. Am. J. Hypertens. 1999, 12, 541–547. [Google Scholar] [CrossRef] [PubMed]
- Montan, S.; Ingemarsson, I.; Marsal, K.; Sjoberg, N.O. Randomised controlled trial of atenolol and pindolol in human pregnancy: Effects on fetal haemodynamics. BMJ 1992, 304, 946–949. [Google Scholar] [CrossRef] [PubMed]
- Butters, L.; Kennedy, S.; Rubin, P.C. Atenolol in essential hypertension during pregnancy. BMJ 1990, 301, 587–589. [Google Scholar] [CrossRef] [PubMed]
- Rubin, P.C.; Butters, L.; Clark, D.M.; Reynolds, B.; Sumner, D.J.; Steedman, D.; A Low, R.; Reid, J.L. Placebocontrolled trial of atenolol in treatment of pregnancy-associated hypertension. Lancet 1983, 1, 431–434. [Google Scholar]
- Weber-Schoendorfer, C.; Hannemann, D.; Meister, R.; Eléfant, E.; Cuppers-Maarschalkerweerd, B.; Arnon, J.; Vial, T.; Rodriguez-Pinilla, E.; Clementi, M.; Robert-Gnansia, E.; et al. The safety of calcium channel blockers during pregnancy: A prospective, multi center, observational study. Reprod. Toxicol. 2008, 26, 24–30. [Google Scholar] [CrossRef]
- Magee, L.A.; Schick, B.; Donnenfeld, A.E.; Sage, S.R.; Conover, B.; Cook, L.; McElhatton, P.R.; Schmidt, M.A.; Koren, G. The safety of calcium channel blockers in human pregnancy: A prospective, multicenter cohort study. Am. J. Obstet. Gynecol. 1996, 174, 823–828. [Google Scholar] [CrossRef]
- Bateman, B.T.M.; Huybrechts, K.F.; Maeda, A.; Desai, R.; Patorno, E.M.; Seely, E.W.; Ecker, J.L.; Allen-Coleman, C.B.; Mogun, H.; Hernandez-Diaz, S.M.; et al. Calcium channel blocker exposure in late pregnancy and the risk of neonatal seizures. Obstet. Gynecol. 2015, 126, 271–278. [Google Scholar] [CrossRef]
- Page, R.L. Treatment of arrhythmias during pregnancy. Am. Heart J. 1995, 130, 871–876. [Google Scholar] [CrossRef]
- Chaffman, M.; Brogden, R.N. Diltiazem. A review of its pharmacological properties and therapeutic efficacy. Drugs 1985, 29, 387–454. [Google Scholar] [CrossRef]
- Airyuki, F. Effects of diltiazem hydrochloride on embryonic development: Species differences in susceptibility and stage specificity in mice, rats, and rabbits. Anat. Jap. 1975, 52, 103–117. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Byerly, W.G.; Hartmann, A.; Foster, D.E.; Tannenbaum, A.K. Verapamil in the treatment of maternal paroxysmal supraventricular tachycardia. Ann. Emerg. Med. 1991, 20, 552–554. [Google Scholar] [CrossRef] [PubMed]
- Allen, N.M.; Page, R.L. Procainamide administration during pregnancy. Clin. Pharm. 1993, 12, 58–60. [Google Scholar] [PubMed]
- Rotmensch, H.H.; Elkayam, U.; Frishman, W. Antiarrhythmic drug therapy during pregnancy. Ann. Intern. Med. 1983, 98, 487–497. [Google Scholar] [CrossRef] [PubMed]
- Biehl, D.; Shnider, S.M.; Levinson, G.; Callender, K. The direct effects of circulating lidocaine on uterine blood flow and foetal well-being in the pregnant ewe. Can. Anaesth. Soc. J. 1977, 24, 445–451. [Google Scholar] [CrossRef] [PubMed]
- Teramo, K.; Benowitz, N.; Heymann, M.A.; Kahanpaa, K.; Siimes, A.; Rudolph, A.M. Effects of lidocaine on heart rate, blood pressure, and electrocorticogram in fetal sheep. Am. J. Obstet. Gynecol. 1974, 118, 935–949. [Google Scholar] [CrossRef] [PubMed]
- January, C.T.; Wann, L.S.; Alpert, J.S.; Calkins, H.; Cigarroa, J.E.; Cleveland, J.C., Jr.; Conti, J.B.; Ellinor, P.T.; Ezekowitz, M.D.; Field, M.E.; et al. 2014 AHA/ ACC/HRS guideline for the management of patients with atrial fibrillation: Executive summary: A report of the American College of Cardiology/American heart association task force on practice guidelines and the heart rhythm society. Circulation 2014, 130, 2071–2104. [Google Scholar] [CrossRef]
- Regitz-Zagrosek, V.; Roos-Hesselink, J.W.; Bauersachs, J.; Blomström-Lundqvist, C.; Cífková, R.; De Bonis, M.; Iung, B.; Johnson, M.R.; Kintscher, U.; Kranke, P.; et al. 2018 ESC guidelines for the management of cardiovascular diseases during pregnancy. Eur. Heart J. 2018, 39, 3165–3241. [Google Scholar] [CrossRef]
- Hall, C.M.; Ward Platt, M.P. Neonatal flecainide toxicity following supraventricular tachycardia treatment. Ann. Pharmacother. 2003, 37, 1343–1344. [Google Scholar] [CrossRef]
- O’Hare, M.F.; Leahey, W.; Murnaghan, G.A.; McDevitt, D.G. Pharmacokinetics of sotalol during pregnancy. Eur. J. Clin. Pharmacol. 1983, 24, 521–524. [Google Scholar] [CrossRef]
- Webster, W.S.; Brown-Woodman, P.D.; Snow, M.D.; Danielsson, B.R. Teratogenic potential of almokalant, dofetilide, and d-sotalol: Drugs with potassium channel blocking activity. Teratology 1996, 53, 168–175. [Google Scholar] [CrossRef]
- Rocca, E.; Zanza, C.; Longhitano, Y.; Piccolella, F.; Romenskaya, T.; Racca, F.; Savioli, G.; Saviano, A.; Piccioni, A.; Mongodi, S. Lung Ultrasound in Critical Care and Emergency Medicine: Clinical Review. Adv. Respir. Med. 2023, 91, 203–223. [Google Scholar] [CrossRef]
- Burkart, T.A.; Kron, J.; Miles, W.M.; Conti, J.B.; Gonzalez, M.D. Successful termination of atrial flutter by ibutilide during pregnancy. PACE 2007, 30, 283–286. [Google Scholar] [CrossRef] [PubMed]
- Kockova, R.; Kocka, V.; Kiernan, T.; Fahy, G.J. Ibutilide-induced cardioversion of atrial fibrillation during pregnancy. J. Cardiovasc. Electrophysiol. 2007, 18, 545–547. [Google Scholar] [CrossRef] [PubMed]
- Elkayam, U.; Goodwin, T.M. Adenosine therapy for supraventricular tachycardia during pregnancy. Am. J. Cardiol. 1995, 75, 521–523. [Google Scholar] [CrossRef]
- Dunn, J.S., Jr.; Brost, B.C. Fetal bradycardia after IV adenosine for maternal PSVT. Am. J. Emerg. Med. 2000, 18, 234–235. [Google Scholar] [CrossRef]
- Harrison, J.K.; Greenfield, R.A.; Wharton, J.M. Acute termination of supraventricular tachycardia by adenosine during pregnancy. Am. Heart J. 1992, 123, 1386–1388. [Google Scholar] [CrossRef]
- Leffler, S.; Johnson, D.R. Adenosine use in pregnancy: Lack of effect on fetal heart rate. Am. J. Emerg. Med. 1992, 10, 548–549. [Google Scholar] [CrossRef]
- Chan, V.; Tse, T.F.; Wong, V. Transfer of digoxin across the placenta and into breast milk. Br. J. Obstet. Gynaecol. 1978, 85, 605–609. [Google Scholar] [CrossRef]
- Soyka, L.F. Digoxin: Placental transfer, effects on the fetus, and therapeutic use in the newborn. Clin. Perinatol. 1975, 2, 23–35. [Google Scholar]
- Rotmensch, H.H.; Rotmensch, S.; Elkayam, U. Management of cardiac arrhythmias during pregnancy. Curr. Concepts Drugs 1987, 33, 623–633. [Google Scholar] [CrossRef]
- Saad, A.F.; Monsivais, L.; Pacheco, L.D. Digoxin therapy of fetal superior ventricular tachycardia: Are digoxin serum levels reliable? AJP Rep. 2016, 6, e272–e276. [Google Scholar]
- Gilardi, E.; Pomero, F.; Ravera, E.; Piccioni, A.; Santoro, M.C.; Bonadia, N.; Carnicelli, A.; Di Maurizio, L.; Sabia, L.; Longhitano, Y.; et al. Intravenous Magnesium Sulfate Reduces the Need for Antiarrhythmics during Acute-Onset Atrial Fibrillation in Emergency and Critical Care. J. Clin. Med. 2022, 11, 5527. [Google Scholar] [CrossRef]
- Tromp, C.H.; Nanne, A.C.; Pernet, P.J.; Tukkie, R.; Bolte, A.C. Electrical cardioversion during pregnancy: Safe or not? Heart J. 2011, 19, 134–136. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.-C.; Chen, C.-H.; Su, H.-Y.; Yu, M.-H. The impact of maternal cardioversion on fetal haemodynamics. Eur. J. Obstet. Gynecol. Reprod. Biol. 2006, 126, 268–269. [Google Scholar] [CrossRef] [PubMed]
- Zanza, C.; Longhitano, Y.; Artico, M.; Cammarota, G.; Barbanera, A.; Racca, F.; Audo, A.; Ravera, E.; Migneco, A.; Piccioni, A.; et al. Bedside Cardiac Pocus in Emergency Setting: A Practice Review. Rev. Recent Clin. Trials 2021, 15, 269–277. [Google Scholar] [CrossRef]
- Driver, K.; Chisholm, C.A.; Darby, A.E.; Malhotra, R.; Dimarco, J.P.; Ferguson, J.D. Catheter ablation of arrhythmia during pregnancy. J. Cardiovasc. Electrophysiol. 2015, 26, 698. [Google Scholar] [CrossRef]
- ACOG Committee on Obstetric Practice. ACOG Committee Opinion. Number 299, September 2004 (replaces No. 158, September 1995). Guidelines for diagnostic imaging during pregnancy. Obstet Gynecol. 2004, 104, 647–651. [Google Scholar]
- Best, P.; Skelding, K.; Mehran, R.; Chieffo, A.; Kunadian, V.; Madan, M.; Mikhail, G.; Mauri, F.; Takahashi, S.; Honye, J.; et al. SCAI consensus document on occupational radiation exposure to the pregnant cardiologist and technical personnel. EuroIntervention 2011, 6, 866–874. [Google Scholar] [CrossRef]
- Patel, S.J.; Reede, D.L.; Katz, D.S.; Subramaniam, R.; Amorosa, J.K. Imaging the pregnant patient for nonobstetric conditions: Algorithms and radiation dose considerations. Radiographics 2007, 27, 1705–1722. [Google Scholar] [CrossRef] [PubMed]
- Doll, R.; Wakeford, R. Risk of childhood cancer from fetal irradiation. Br. J. Radiol. 1997, 70, 130–139. [Google Scholar] [CrossRef] [PubMed]
- Miyoshi, T.; Kamiya, C.A.; Katsuragi, S.; Ueda, H.; Kobayashi, Y.; Horiuchi, C.; Yamanaka, K.; Neki, R.; Yoshimatsu, J.; Ikeda, T.; et al. Safety and efficacy of implantable cardioverter-defibrillator during pregnancy and after delivery. Circ. J. 2013, 77, 1166–1170. [Google Scholar] [CrossRef] [PubMed]
- Al-Khatib, S.M.; Stevenson, W.G.; Ackerman, M.J.; Bryant, W.J.; Callans, D.J.; Curtis, A.B.; Deal, B.J.; Dickfeld, T.; Field, M.E.; Fonarow, G.C.; et al. 2017 AHA/ACC/HRS Guideline for Management of Patients With Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society. J. Am. Coll. Cardiol. 2018, 72, e91–e220, Erratum in J. Am. Coll. Cardiol. 2018, 72, 1760. [Google Scholar] [CrossRef] [PubMed]
- Marcus, G.M. Evaluation and management of premature ventricular complexes. Circulation 2020, 141, 1404–1418. [Google Scholar] [CrossRef] [PubMed]
- Chong, B.-H.; Pong, V.; Lam, K.-F.; Liu, S.; Zuo, M.-L.; Lau, Y.-F.; Lau, C.-P.; Tse, H.-F.; Siu, C.-W. Frequent premature atrial complexes predict new occurrence of atrial fibrillation and adverse cardiovascular events. Europace 2012, 14, 942–947. [Google Scholar] [CrossRef]
- Lin, C.; Lin, Y.; Chen, Y.; Chang, S.; Lo, L.; Chao, T.; Chung, F.; Hu, Y.; Chong, E.; Cheng, H.; et al. Prognostic significance of premature atrial complexes burden in prediction of long-term outcome. J. Am. Heart Assoc. 2015, 4, e002192. [Google Scholar] [CrossRef]
- Loerup, L.; Pullon, R.M.; Birks, J.; Fleming, S.; Mackillop, L.H.; Gerry, S.; Watkinson, P.J. Trends of blood pressure and heart rate in normal pregnancies: A systematic review and meta-analysis. BMC Med. 2019, 17, 167. [Google Scholar] [CrossRef]
- Shabtaie, S.A.; Witt, C.M.; Asirvatham, S.J. Natural history and clinical outcomes of inappropriate sinus tachycardia. J. Cardiovasc. Electrophysiol. 2020, 31, 137–143. [Google Scholar] [CrossRef]
- Chokesuwattanaskul, R.; Thongprayoon, C.; Bathini, T.; O’Corragain, O.A.; Sharma, K.; Prechawat, S.; Ungprasert, P.; Watthanasuntorn, K.; Pachariyanon, P.; Cheungpasitporn, W. Incidence of atrial fibrillation in pregnancy and clinical significance: A meta-analysis. Adv. Med. Sci. 2019, 64, 415–422. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.S.; Chen, W.; Zhang, Z.; Duan, L.; Ng, A.; Spencer, H.T.; Kwan, D.M.; Shen, A.Y. Atrial fibrillation and atrial flutter in pregnant women—A population-based study. J. Am. Heart Assoc. 2016, 5, e003182. [Google Scholar] [CrossRef]
- Salam, A.M.; Ertekin, E.; van Hagen, I.M.; Al Suwaidi, J.; Ruys, T.P.E.; Johnson, M.R.; Gumbiene, L.; Frogoudaki, A.A.; Sorour, K.A.; Iserin, L. Atrial fibrillation or flutter during pregnancy in patients with structural heart disease: Data from the ROPAC [Registry on pregnancy and cardiac disease]. JACC Clin. Electrophysiol. 2015, 1, 284–292. [Google Scholar] [CrossRef]
- Henry, D.; Gonzalez, J.M.; Harris, I.S.; Sparks, T.N.; Killion, M.; Thiet, M.-P.; Bianco, K. Maternal arrhythmia and perinatal outcomes. J. Perinatol. 2016, 36, 823–827. [Google Scholar] [CrossRef]
- Hindricks, G.; Potpara, T.; Dagres, N.; Arbelo, E.; Bax, J.J.; Blomström-Lundqvist, C.; Boriani, G.; Castella, M.; Dan, G.A.; Dilaveris, P.E.; et al. 2020 ESC guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS): The Task Force for the diagnosis and management of atrial fibrillation of the European Society of Cardiology (ESC) Developed with the special contribution of the European Heart Rhythm Association (EHRA) of the ESC. Eur. Heart J. 2021, 42, 373–498. [Google Scholar]
- Szumowski, L.; Szufladowicz, E.; Orczykowski, M.; Bodalski, R.; Derejko, P.; Przybylski, A.; Urbanek, P.; Kuśmierczyk, M.; Koźluk, E.; Sacher, F.; et al. Ablation of severe drug-resistant tachyarrhythmia during pregnancy. J. Cardiovasc. Electrophysiol. 2010, 21, 877–882. [Google Scholar] [CrossRef]
- Ferguson, J.D.; Helms, A.; Mangrum, J.M.; DiMarco, J.P. Ablation of incessant left atrial tachycardia without fluoroscopy in a pregnant woman. J. Cardiovasc. Electrophysiol. 2011, 22, 346–349. [Google Scholar] [CrossRef]
- Razminia, M.; Willoughby, M.C.; Demo, H.; Keshmiri, H.; Wang, T.; D’Silva, O.J.; Zheutlin, T.A.; Jibawi, H.; Okhumale, P.; Kehoe, R.F. Fluoroless Catheter Ablation of Cardiac Arrhythmias: A 5-Year Experience. Pacing Clin. Electrophysiol. 2017, 40, 425–433. [Google Scholar] [CrossRef]
- Lemery, R.; Brugada, P.; Bella, P.D.; Dugernier, T.; van den Dool, A.; Wellens, H.J. Nonischemic ventricular tachycardia. Clinical course and long-term follow-up in patients without clinically overt heart disease. Circulation 1989, 79, 990–999. [Google Scholar] [CrossRef]
- European Heart Rhythm Association; Heart Rhythm Societ; Zipes, D.P.; Camm, A.J.; Borggrefe, M.; Buxton, A.E.; Chaitman, B.; Fromer, M.; Gregoratos, G.; Klein, G.; et al. ACC/ AHA/ESC 2006 guidelines for management of patients with ventricular arrhythmias and the prevention of sudden cardiac death: A report of the American College of Cardiology/American Heart Association Task Force and the European Society of Cardiology Committee for Practice Guidelines (writing committee to develop Guidelines for Management of Patients With Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death): Developed in collaboration with the European Heart Rhythm Association and the Heart Rhythm Society. J. Am. Coll. Cardiol. 2006, 48, 1064–1108. [Google Scholar]
- Seth, R.; Moss, A.J.; McNitt, S.; Zareba, W.; Andrews, M.L.; Qi, M.; Robinson, J.L.; Goldenberg, I.; Ackerman, M.J.; Benhorin, J.; et al. “Rescue” ablation of electrical storm in arrhythmogenic right ventricular cardiomyopathy in pregnancy. BMC Cardiovasc. Disord. 2013, 13, 58. [Google Scholar]
- Chandra, N.C.; Gates, E.A.; Thamer, M. Conservative treatment of paroxysmal ventricular tachycardia during pregnancy. Clin. Cardiol. 1991, 14, 347–350. [Google Scholar] [CrossRef] [PubMed]
- Khositseth, A.; Tester, D.J.; Will, M.L.; Bell, C.M.; Ackerman, M.J. Identification of a common genetic substrate underlying postpartum cardiac events in congenital long QT syndrome. Heart Rhythm. 2004, 1, 60–64. [Google Scholar] [CrossRef] [PubMed]
- Seth, R.; Moss, A.J.; McNitt, S.; Zareba, W.; Andrews, M.L.; Qi, M.; Robinson, J.L.; Goldenberg, I.; Ackerman, M.J.; Benhorin, J.; et al. Long QT syndrome and pregnancy. J. Am. Coll. Cardiol. 2007, 49, 1092–1098. [Google Scholar] [CrossRef] [PubMed]
- Roston, T.M.; van der Werf, C.; Cheung, C.C.; Grewal, J.; Davies, B.; Wilde, A.A.; Krahn, A.D. Caring for the pregnant woman with an inherited arrhythmia syndrome. Heart Rhythm. 2020, 17, 341–348. [Google Scholar] [CrossRef] [PubMed]
- Zeven, K. Pregnancy-Associated Spontaneous Coronary Artery Dissection in Women: A Literature Review. Curr. Ther. Res. Clin. Exp. 2023, 98, 100697. [Google Scholar] [CrossRef]
- Zelop, C.M.; Einav, S.; Mhyre, J.M.; Martin, S. Cardiac arrest during pregnancy: Ongoing clinical conundrum: An expert review. Am. J. Obstet. Gynecol. 2018, 219, 52–61. [Google Scholar] [CrossRef] [PubMed]
- Suresh, M.S.; LaToya Mason, C.; Munnur, U. Cardiopulmonary resuscitation and the parturient. Best. Pract. Res. Clin. Obstet. Gynaecol. 2010, 24, 383. [Google Scholar] [CrossRef]
- Mogos, M.F.; Salemi, J.L.; Spooner, K.K.; McFarlin, B.L.; Salihu, H.M. Differences in mortality between pregnant and nonpregnant women after cardiopulmonary resuscitation. Obstet. Gynecol. 2016, 128, 880–888. [Google Scholar] [CrossRef]
- Nolan, J.P.; Sandroni, C.; Böttiger, B.W.; Cariou, A.; Cronberg, T.; Friberg, H.; Genbrugge, C.; Haywood, K.; Lilja, G.; Moulaert, V.R.M.; et al. European Resuscitation Council and European Society of Intensive Care Medicine guidelines 2021: Post-resuscitation care. Intensive Care Med. 2021, 47, 369–421. [Google Scholar] [CrossRef]


{kind=link}
| AR Drug | FDA Category | Fetal Adverse Effect | Use in Pregnancy | Lactation |
|---|---|---|---|---|
| Adenosine | C | No significant adverse events. Fetal monitoring for transient fetal bradycardia | Safe | Safe |
| Amiodarone | D | Fetal hypothyroidism with congenital goiter, growth retardation, preterm birth, and neurodevelopmental abnormalities | Only if other options are not available | Do not use |
| Atenolol | D | Increased risk of congenital malformations, FGR, and fetal bradycardia | Not safe | Do not use |
| Atropine | C | Scant literature regarding the safety profile | Used for emergent resuscitation | Not safe |
| Diltiazem | C | Increased risk of FGR. Skeletal, cardiac, tongue, and retinal abnormalities in animal models | Use with caution | Use with caution |
| Digoxin | C | No significant adverse effects | Safe | Safe |
| Dofetilide | C | In animal models, fetal resorption and skeletal abnormalities have been observed if administered during organogenesis, and significant bradycardia even at the lower doses | Do not use | Do not use |
| Dronedarone | X | Significant fetal adverse events including vascular and limb abnormalities and cleft palate | Do not use | Do not use |
| Flecainide | C | Animal data have confirmed that it is free from teratogenic effects. At very high doses, delayed sternal and vertebral ossification observed in rats | Use with caution | Safe |
| Ibutilide | C | No adverse events reported in case reports. In rats, skeletal and cardiac abnormalities noted with daily exposure | Use with caution | Use with caution |
| Ivabradine | NA | High incidence of fetal cardiac defects in rats and ectrodactyly in rabbits. FGR, neonatal bradycardia, and hypotension can occur | Do not use | Do not use |
| Lidocaine | B | No increased risk of birth defects or adverse events have been observed at therapeutic doses | Safe | Safe |
| Metoprolol | C | No significant adverse effects. Small risk of FGR, neonatal bradycardia, and hypoglycemia | Use with caution | Safe |
| Mexiletine | C | Minimal data. Concern for lower Apgar scores. Increased fetal resorption at 4× maximum RHD in rats and rabbits | Use with caution | Use with caution |
| Nadolol | C | Small risk of apnea, FGR, and hypoglycemia | Use with caution | Do not use |
| Procainamide | C | No teratogenic effects, limited data reported | Use with caution | Use with caution |
| Propafenone | C | Minimal human data. Reduction in neonatal survival, weight gain, and development abnormalities observed at 3–6× maximum RHD | Use with caution | Do not use |
| Propranolol | C | No significant adverse effects. Small risk of FGR, neonatal bradycardia, and hypoglycemia | Use with caution | Safe |
| Quinidine | C | No teratogenicity observed. Rarely, mild uterine contractions, premature labor, neonatal thrombocytopenia, and cranial nerve VIII damage have been reported | Use with caution | Use with caution |
| Sotalol | C | No teratogenic potential. Small risk of fetal bradycardia and hypoglycemia | Safe | Use with caution |
| Verapamil | C | No significant teratogenicity risk, only maternal hypotension and fetal bradycardia | Use with caution | Use with caution |
| ATRIAL FIBRILLATION (AF) | |||
| Patient Hemodynamically Stable | Patient Hemodynamically Unstable * | Recurrent AF | |
| Obtain rate control: | Electrical synchronized cardioversion | Flecainide or sotalol | |
| 1st line: beta-blockers +/− digoxin | |||
| 2nd line: ca-channel blockers | |||
| In case of inadequate rate control: electrical synchronized cardioversion | If refractory, consider ablation with minimal fluoroscopy | ||
| AF persisting for more than 48 h should be managed with anticoagulation before cardioversion | |||
| SUPRAVENTRICULAR TACHYCARDIA (SVT) | |||
| Patient hemodynamically stable | Patient hemodynamically unstable * | Recurrent SVT | |
| 1st line: vagal maneuvers (Valsalva maneuver or carotid sinus massage) | Electrical synchronized cardioversion | 1st line: beta-blockers +/− digoxin in patients without pre-excitation | |
| 2nd line: adenosine | 2nd line: ca-channel blockers | ||
| In patients with pre-excitation: beta-blockers + flecainide | |||
| If refractory consider ablation with minimal fluoroscopy | |||
| VENTRICULAR TACHYCARDIA (VT) | |||
| Patient hemodynamically stable | Patient hemodynamically unstable * | Polymorphic VT or torsade de pointes | Long-QT syndorme |
| 1st line: lidocaine | Electrical synchronized cardioversion | Magnesium sulfate | Avoid QT-prolonging medications |
| 2nd line: procainamide or quinidine Amiodarone is reserved for life-threatening situations when other options have failed | Propranolol prevents arrhythmic events | ||
| Monomorphic ventricular tachycardia: ablation with minimal fluoroscopy only if refractory | |||
| Point | Recommendation/Action |
|---|---|
| Multidisciplinary Team | Ensure a multidisciplinary team, including anesthesiologists, cardiologists, obstetricians, and neonatologists, for optimal maternal and fetal care during cardiac arrest. |
| Chest Compressions | Perform chest compressions in the standard position on the sternum. |
| Intravenous Access | Place intravenous access above the diaphragm to ensure drug efficacy, as femoral administration may not reach the maternal heart until fetal delivery. |
| Medication Administration | Do not withhold medications due to concerns for fetal teratogenicity, including amiodarone. |
| Drug Doses and Defibrillation Protocols | Maintain standard drug doses and defibrillation protocols during resuscitation efforts. |
| Fetal Monitoring | Interrupt fetal monitoring and remove equipment during defibrillation to prevent electrocution injury to the patient or rescuers. |
| Airway Management | Assume a difficult airway. Intubation via video-laryngoscopy using a smaller-sized endotracheal tube is recommended; consider supraglottic airway devices if intubation is challenging. |
| Gestational Age Estimation | Estimate gestational age, taking into account the common occurrence of aorto-caval compression after 20 weeks. Additionally, acknowledge that neonates born at 23 and 24 weeks have demonstrated a reasonable chance of survival without severe deficits. When prenatal records are unavailable, rely on physical examination, considering key indicators. Notably, by 20 weeks in a singleton pregnancy, the top of the uterine fundus is typically aligned with the umbilicus. |
| Uterine Displacement | Manually displace the uterus laterally and to the left (left uterine displacement) for pregnancies ≥20 weeks to avoid aorto-caval compression. If manual displacement is not possible, tilt the operating table or use towels/blankets to achieve a tilt of no more than 30°. |
| Emergency Cesarean Delivery Preparation | Prepare for early emergency caesarean delivery for pregnancies ≥20 weeks. |
| Cesarean Delivery Timing | If spontaneous circulation is not restored within five minutes of maternal cardiac arrest, initiate emergency caesarean delivery at 20 weeks of gestation and beyond. |
| Extracorporeal Life Support Evaluation | Evaluate the need for instituting extracorporeal life support based on the clinical scenario. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Conti, E.; Cascio, N.D.; Paluan, P.; Racca, G.; Longhitano, Y.; Savioli, G.; Tesauro, M.; Leo, R.; Racca, F.; Zanza, C. Pregnancy Arrhythmias: Management in the Emergency Department and Critical Care. J. Clin. Med. 2024, 13, 1095. https://doi.org/10.3390/jcm13041095
Conti E, Cascio ND, Paluan P, Racca G, Longhitano Y, Savioli G, Tesauro M, Leo R, Racca F, Zanza C. Pregnancy Arrhythmias: Management in the Emergency Department and Critical Care. Journal of Clinical Medicine. 2024; 13(4):1095. https://doi.org/10.3390/jcm13041095
Chicago/Turabian StyleConti, Elena, Nunzio Dario Cascio, Patrizia Paluan, Giulia Racca, Yaroslava Longhitano, Gabriele Savioli, Manfredi Tesauro, Roberto Leo, Fabrizio Racca, and Christian Zanza. 2024. "Pregnancy Arrhythmias: Management in the Emergency Department and Critical Care" Journal of Clinical Medicine 13, no. 4: 1095. https://doi.org/10.3390/jcm13041095
APA StyleConti, E., Cascio, N. D., Paluan, P., Racca, G., Longhitano, Y., Savioli, G., Tesauro, M., Leo, R., Racca, F., & Zanza, C. (2024). Pregnancy Arrhythmias: Management in the Emergency Department and Critical Care. Journal of Clinical Medicine, 13(4), 1095. https://doi.org/10.3390/jcm13041095