
Improved Outcomes and Therapy Longevity after Salvage Using a Novel Spinal Cord Stimulation System for Chronic Pain: Multicenter, Observational, European Case Series

 ,
,  , ,
, ,  ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Study Setting and Participants
2.3. IPG Conversion
- MICC-tonic SCS: supra-perception, paresthesia-based SCS modality that uses MICC technology and the Illumina 3DTM programming algorithm (Boston Scientific). Illumina 3DTM is a proprietary, neural-targeting algorithm that takes into account the 3D anatomical environment around the SCS leads to compute the electrical field that will best engage specific dorsal column fibers and cover the desired pain areas.
- Customized burst SCS (Burst 3D or MicroBurst 3D, Boston Scientific): sub-perception SCS modality delivering packets of burst stimuli in a regular manner. Burst stimulation leverages the Illumina 3DTM algorithm to target the stimulation area and offers various settings (e.g., intra-burst frequency, inter-burst frequency, pulse width, number of pulses, etc.) that help to personalize the waveform to each patient.
- High-frequency/dorsal horn modulation (DHM) SCS: sub-perception SCS modality using high-frequency (≤1.2 kHz) stimulation and MICC and/or the Illumina 3D algorithm. High-frequency SCS can either use a focal target or a broad uniform field of stimulation using the Contour algorithm (Boston Scientific). High-frequency SCS has been shown to significantly reduce the wide dynamic range output [36], and the Contour algorithm implements a stimulation field designed to preferentially modulate the dorsal horn inhibitory interneurons [18,37].
- Fast-acting sub-perception SCS therapy (FAST) enables rapid onset of analgesia that combines precise placement of the stimulating electric field and precise dosing of a biphasic symmetric waveform at low frequency in a manner intended to engage surround inhibition for pain relief [38,39]. FAST therapy is programmed with the proprietary Illumina 3DTM algorithm and uses a 90 Hz active recharge waveform to achieve 100% coverage before reducing the amplitude to a sub-perception level.
- Combination SCS therapy allows multiple waveforms to be layered in a simultaneous or sequential manner to engage various modalities and mechanisms of action. For example, MICC-tonic SCS could be simultaneously delivered with Contour SCS to produce both dorsal column activation and dorsal horn modulation to optimize pain relief.
2.4. Outcome Measures
2.5. Statistical Analysis
3. Results
3.1. Patient Population
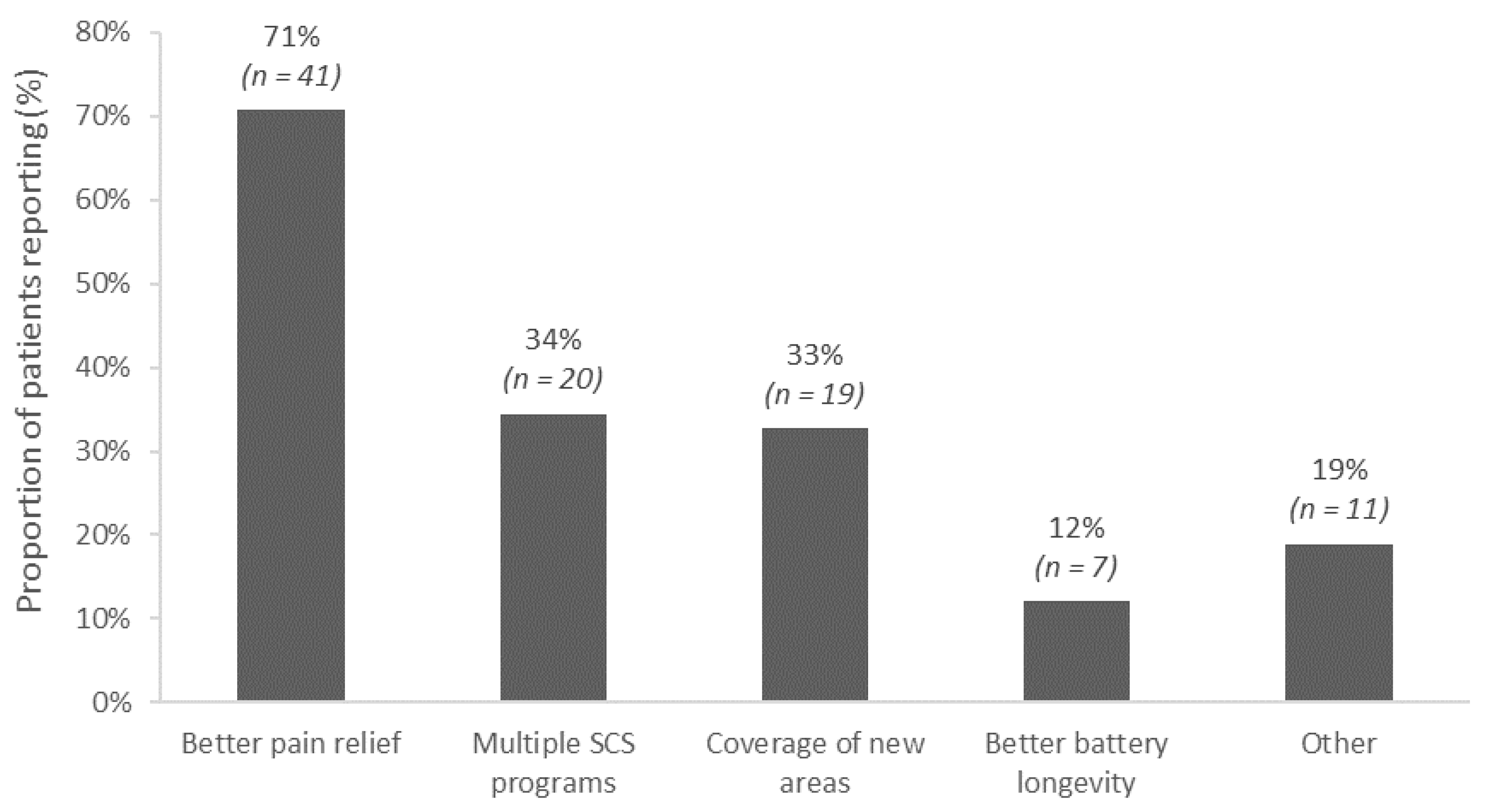
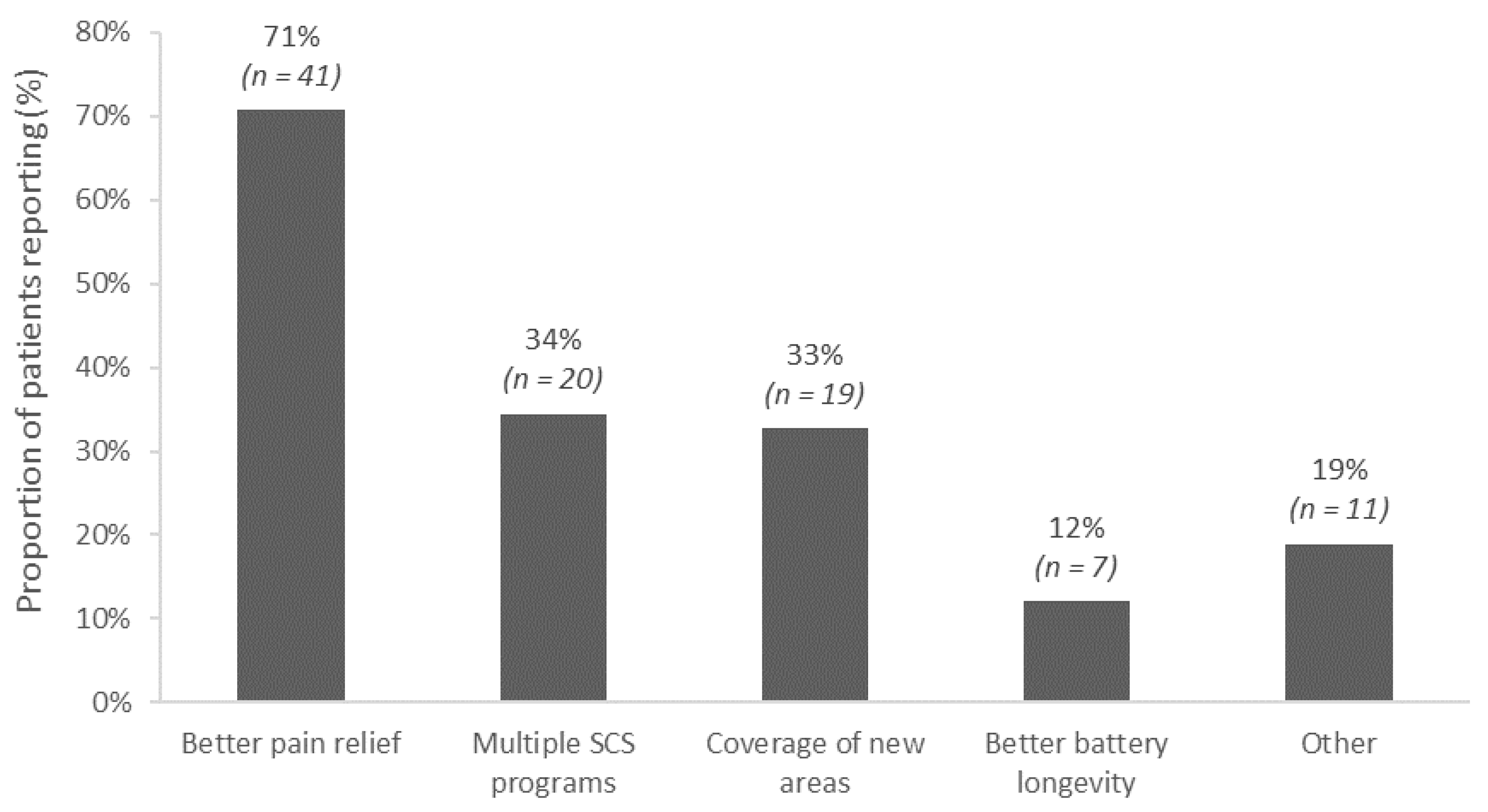
- Rescue of LoE (Rescue group): patients who had moderate to severe pain based on pre-conversion overall pain scores (NRS ≥ 4/10) or those who chose to convert for any one of the following reasons: better pain relief, access to multiple stimulation modalities, or coverage of new pain areas (n = 51).
- Sustain group: patients who had mild pain based on their pre-conversion overall pain score (NRS ≤ 3/10) or who chose to convert for better battery longevity (n = 7).
3.2. Conversion Procedure
3.3. Post-Conversion Clinical Outcomes
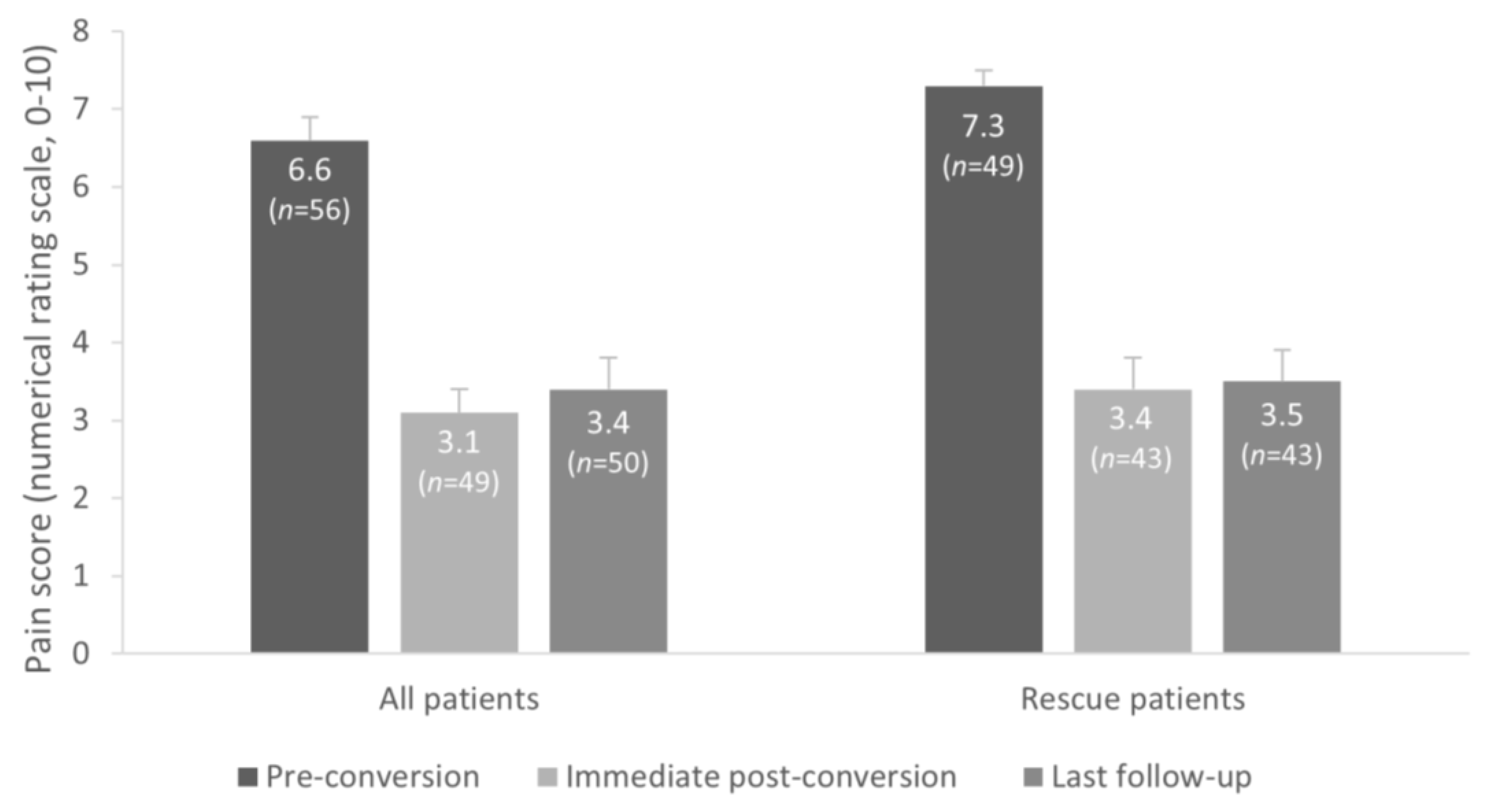
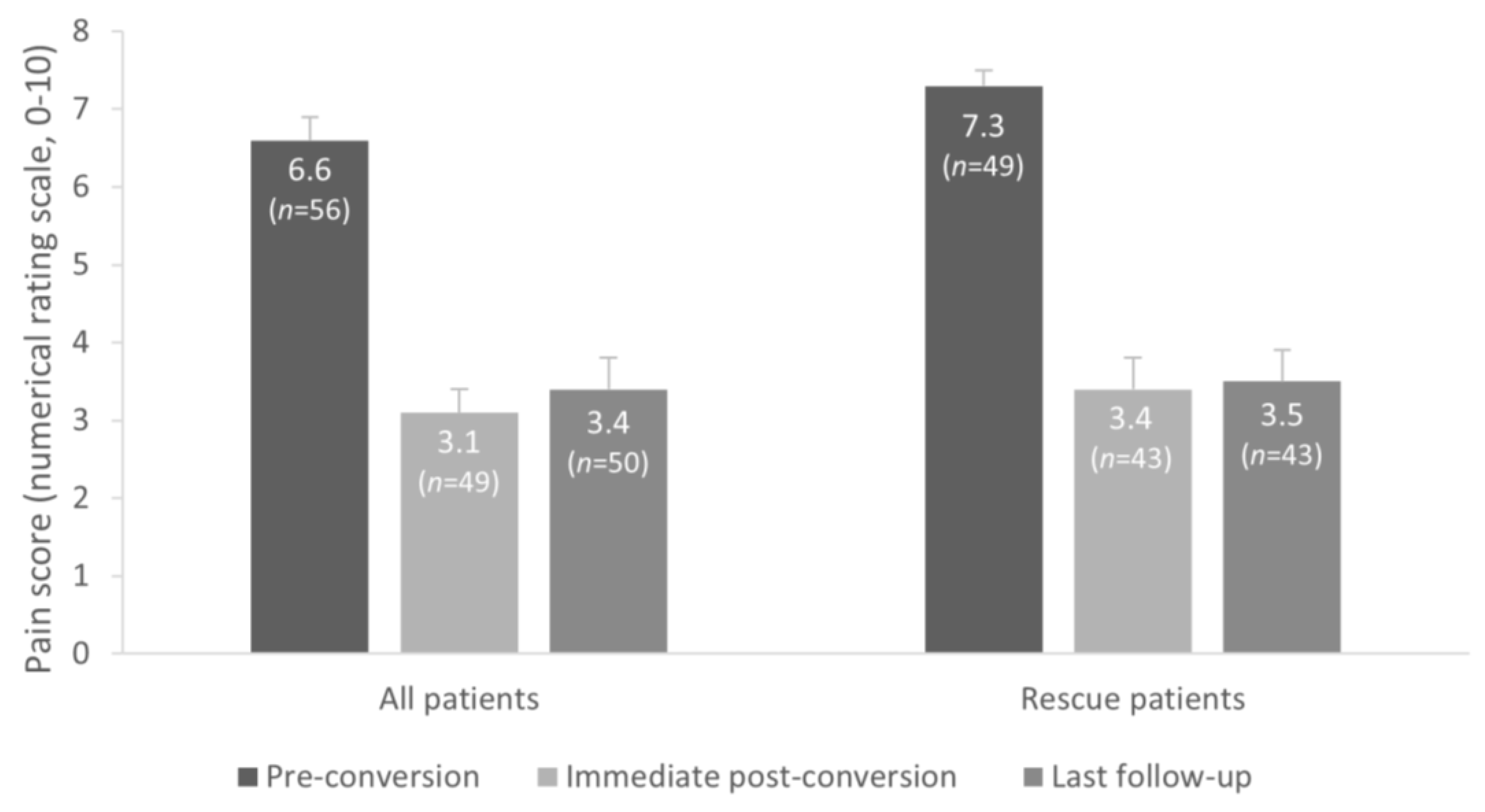
3.3.1. All Patients
3.3.2. Rescue (LoE) Subgroup
3.3.3. Sustain Subgroup
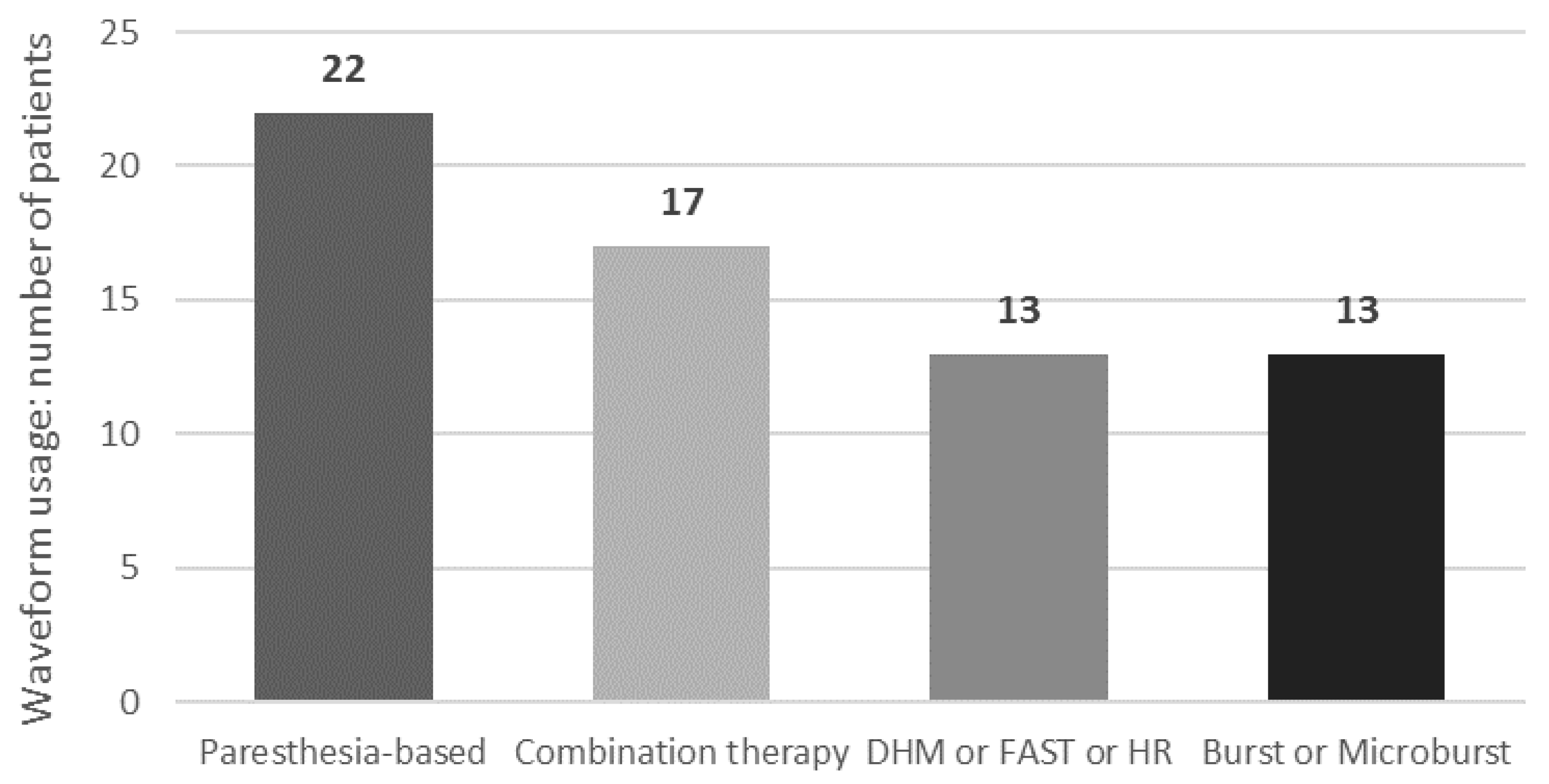
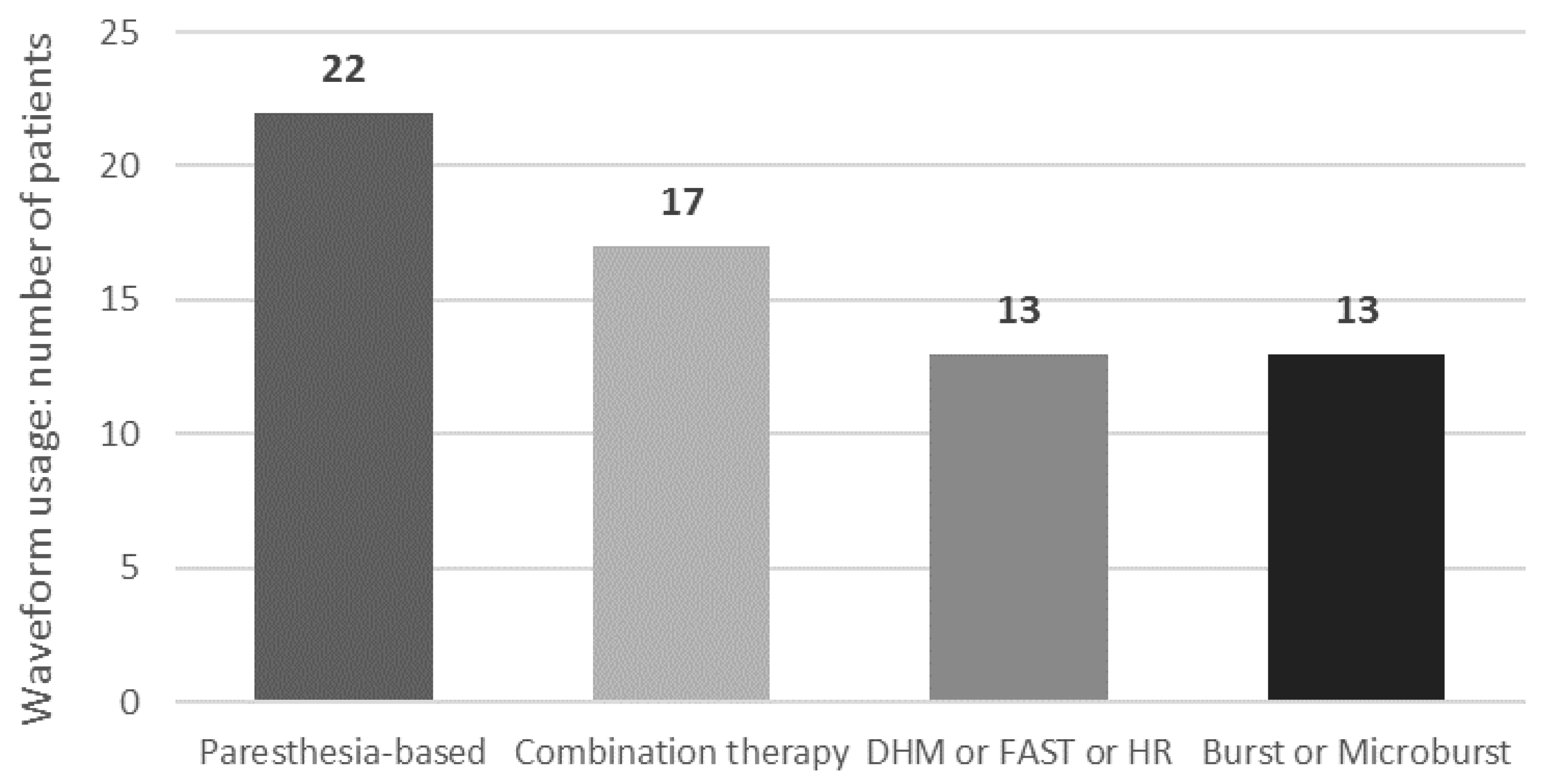
3.3.4. Waveforms Usage
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mansfield, K.E.; Sim, J.; Jordan, J.L.; Jordan, K.P. A systematic review and meta-analysis of the prevalence of chronic widespread pain in the general population. Pain 2016, 157, 55–64. [Google Scholar] [CrossRef]
- Vos, T.; Lim, S.S.; Abbafati, C.; Abbas, K.M.; Abbasi, M.; Abbasifard, M.; Abbasi-Kangevari, M.; Abbastabar, H.; Abd-Allah, F.; Abdelalim, A.; et al. Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1204–1222. [Google Scholar] [CrossRef]
- Cohen, S.P.; Vase, L.; Hooten, W.M. Chronic pain: An update on burden, best practices, and new advances. Lancet 2021, 397, 2082–2097. [Google Scholar] [CrossRef]
- Naiditch, N.; Billot, M.; Moens, M.; Goudman, L.; Cornet, P.; Le Breton, D.; Roulaud, M.; Ounajim, A.; Page, P.; Lorgeoux, B.; et al. Persistent Spinal Pain Syndrome Type 2 (PSPS-T2), a Social Pain? Advocacy for a Social Gradient of Health Approach to Chronic Pain. J. Clin. Med. 2021, 10, 2817. [Google Scholar] [CrossRef] [PubMed]
- Naiditch, N.; Billot, M.; Goudman, L.; Cornet, P.; Roulaud, M.; Ounajim, A.; Page, P.; Lorgeoux, B.; Baron, S.; Nivole, K.; et al. Professional Status of Persistent Spinal Pain Syndrome Patients after Spinal Surgery (PSPS-T2): What Really Matters? A Prospective Study Introducing the Concept of “Adapted Professional Activity” Inferred from Clinical, Psychological and Social Influence. J. Clin. Med. 2021, 10, 5055. [Google Scholar] [CrossRef] [PubMed]
- Shealy, C.N.; Mortimer, J.T.; Reswick, J.B. Electrical inhibition of pain by stimulation of the dorsal columns: Preliminary clinical report. Anesth. Analg. 1967, 46, 489–491. [Google Scholar] [CrossRef] [PubMed]
- Kumar, K.; Taylor, R.S.; Jacques, L.; Eldabe, S.; Meglio, M.; Molet, J.; Thomson, S.; O’Callaghan, J.; Eisenberg, E.; Milbouw, G.; et al. Spinal cord stimulation versus conventional medical management for neuropathic pain: A multicentre randomised controlled trial in patients with failed back surgery syndrome. Pain 2007, 132, 179–188. [Google Scholar] [CrossRef]
- Kumar, K.; Rizvi, S. Cost-effectiveness of spinal cord stimulation therapy in management of chronic pain. Pain Med. 2013, 14, 1631–1649. [Google Scholar] [CrossRef]
- Vallejo, R.; Gupta, A.; Cedeno, D.L.; Vallejo, A.; Smith, W.J.; Thomas, S.M.; Benyamin, R.; Kaye, A.D.; Manchikanti, L. Clinical Effectiveness and Mechanism of Action of Spinal Cord Stimulation for Treating Chronic Low Back and Lower Extremity Pain: A Systematic Review. Curr. Pain Headache Rep. 2020, 24, 70. [Google Scholar] [CrossRef]
- Eckermann, J.M.; Pilitsis, J.G.; Vannaboutathong, C.; Wagner, B.J.; Province-Azalde, R.; Bendel, M.A. Systematic Literature Review of Spinal Cord Stimulation in Patients With Chronic Back Pain Without Prior Spine Surgery. Neuromodulation 2021, 25, 648–656. [Google Scholar] [CrossRef]
- Chakravarthy, K.; Malayil, R.; Kirketeig, T.; Deer, T. Burst Spinal Cord Stimulation: A Systematic Review and Pooled Analysis of Real-World Evidence and Outcomes Data. Pain Med. 2019, 20, S47–S57. [Google Scholar] [CrossRef] [PubMed]
- Baranidharan, G.; Edgar, D.; Bretherton, B.; Crowther, T.; Lalkhen, A.G.; Fritz, A.K.; Vajramani, G. Efficacy and Safety of 10 kHz Spinal Cord Stimulation for the Treatment of Chronic Pain: A Systematic Review and Narrative Synthesis of Real-World Retrospective Studies. Biomedicines 2021, 9, 180. [Google Scholar] [CrossRef]
- Rigoard, P.; Billot, M.; Ingrand, P.; Durand-Zaleski, I.; Roulaud, M.; Peruzzi, P.; Dam Hieu, P.; Voirin, J.; Raoul, S.; Page, P.; et al. How Should we Use Multicolumn Spinal Cord Stimulation to Optimize Back Pain Spatial Neural Targeting? A Prospective, Multicenter, Randomized, Double-Blind, Controlled Trial (ESTIMET Study). Neuromodulation 2021, 24, 86–101. [Google Scholar] [CrossRef]
- Veizi, E.; Hayek, S.M.; North, J.; Brent Chafin, T.; Yearwood, T.L.; Raso, L.; Frey, R.; Cairns, K.; Berg, A.; Brendel, J.; et al. Spinal Cord Stimulation (SCS) with Anatomically Guided (3D) Neural Targeting Shows Superior Chronic Axial Low Back Pain Relief Compared to Traditional SCS-LUMINA Study. Pain Med. 2017, 18, 1534–1548. [Google Scholar] [CrossRef] [PubMed]
- Kallewaard, J.W.; Paz-Solis, J.F.; De Negri, P.; Canós-Verdecho, M.A.; Belaid, H.; Thomson, S.J.; Abejón, D.; Vesper, J.; Mehta, V.; Rigoard, P.; et al. Real-World Outcomes Using a Spinal Cord Stimulation Device Capable of Combination Therapy for Chronic Pain: A European, Multicenter Experience. J. Clin. Med. 2021, 10, 4085. [Google Scholar] [CrossRef] [PubMed]
- Metzger, C.S.; Hammond, M.B.; Pyles, S.T.; Washabaugh, E.P., 3rd; Waghmarae, R.; Berg, A.P.; North, J.M.; Pei, Y.; Jain, R. Pain relief outcomes using an SCS device capable of delivering combination therapy with advanced waveforms and field shapes. Expert. Rev. Med. Devices 2020, 17, 951–957. [Google Scholar] [CrossRef]
- Thomson, S.J.; Tavakkolizadeh, M.; Love-Jones, S.; Patel, N.K.; Gu, J.W.; Bains, A.; Doan, Q.; Moffitt, M. Effects of Rate on Analgesia in Kilohertz Frequency Spinal Cord Stimulation: Results of the PROCO Randomized Controlled Trial. Neuromodulation 2018, 21, 67–76. [Google Scholar] [CrossRef]
- Paz-Solís, J.; Thomson, S.; Jain, R.; Chen, L.; Huertas, I.; Doan, Q. Exploration of High- and Low-Frequency Options for Subperception Spinal Cord Stimulation Using Neural Dosing Parameter Relationships: The HALO Study. Neuromodulation 2022, 25, 94–102. [Google Scholar] [CrossRef]
- Head, J.; Mazza, J.; Sabourin, V.; Turpin, J.; Hoelscher, C.; Wu, C.; Sharan, A. Waves of Pain Relief: A Systematic Review of Clinical Trials in Spinal Cord Stimulation Waveforms for the Treatment of Chronic Neuropathic Low Back and Leg Pain. World Neurosurg. 2019, 131, 264–274.e263. [Google Scholar] [CrossRef]
- Rigoard, P.; Ounajim, A.; Moens, M.; Goudman, L.; Roulaud, M.; Lorgeoux, B.; Baron, S.; Nivole, K.; Many, M.; Lampert, L.; et al. Should we Oppose or Combine Waveforms for Spinal Cord Stimulation in PSPS-T2 Patients? A Prospective Randomized Crossover Trial (MULTIWAVE Study). J. Pain 2023, 24, 2319–2339. [Google Scholar] [CrossRef]
- Kumar, K.; Hunter, G.; Demeria, D. Spinal cord stimulation in treatment of chronic benign pain: Challenges in treatment planning and present status, a 22-year experience. Neurosurgery 2006, 58, 481–496. [Google Scholar] [CrossRef]
- Deer, T.R.; Mekhail, N.; Provenzano, D.; Pope, J.; Krames, E.; Thomson, S.; Raso, L.; Burton, A.; DeAndres, J.; Buchser, E.; et al. The appropriate use of neurostimulation: Avoidance and treatment of complications of neurostimulation therapies for the treatment of chronic pain. Neuromodulation Appropriateness Consensus Committee. Neuromodulation 2014, 17, 571–597, discussion 597–578. [Google Scholar] [CrossRef] [PubMed]
- Aiudi, C.M.; Dunn, R.Y.; Burns, S.M.; Roth, S.A.; Opalacz, A.; Zhang, Y.; Chen, L.; Mao, J.; Ahmed, S.U. Loss of Efficacy to Spinal Cord Stimulator Therapy: Clinical Evidence and Possible Causes. Pain Physician 2017, 20, E1073–E1080. [Google Scholar] [CrossRef]
- Hunter, C.W.; Carlson, J.; Yang, A.; Patterson, D.; Lowry, B.; Mehta, P.; Rowe, J.; Deer, T. BURST(able): A Retrospective, Multicenter Study Examining the Impact of Spinal Cord Stimulation with Burst on Pain and Opioid Consumption in the Setting of Salvage Treatment and “Upgrade”. Pain Physician 2020, 23, E643–E658. [Google Scholar]
- Rigoard, P.; Nivole, K.; Blouin, P.; Monlezun, O.; Roulaud, M.; Lorgeoux, B.; Bataille, B.; Guetarni, F. A novel, objective, quantitative method of evaluation of the back pain component using comparative computerized multi-parametric tactile mapping before/after spinal cord stimulation and database analysis: The “Neuro-Pain’t” software. Neurochirurgie 2015, 61 (Suppl. 1), S99–S108. [Google Scholar] [CrossRef]
- Hayek, S.M.; Veizi, E.; Hanes, M. Treatment-Limiting Complications of Percutaneous Spinal Cord Stimulator Implants: A Review of Eight Years of Experience From an Academic Center Database. Neuromodulation 2015, 18, 603–608, discussion 608–609. [Google Scholar] [CrossRef]
- Van Buyten, J.P.; Wille, F.; Smet, I.; Wensing, C.; Breel, J.; Karst, E.; Devos, M.; Pöggel-Krämer, K.; Vesper, J. Therapy-Related Explants After Spinal Cord Stimulation: Results of an International Retrospective Chart Review Study. Neuromodulation 2017, 20, 642–649. [Google Scholar] [CrossRef] [PubMed]
- Pope, J.E.; Deer, T.R.; Falowski, S.; Provenzano, D.; Hanes, M.; Hayek, S.M.; Amrani, J.; Carlson, J.; Skaribas, I.; Parchuri, K.; et al. Multicenter Retrospective Study of Neurostimulation With Exit of Therapy by Explant. Neuromodulation 2017, 20, 543–552. [Google Scholar] [CrossRef] [PubMed]
- De Jaeger, M.; Goudman, L.; Putman, K.; De Smedt, A.; Rigoard, P.; Geens, W.; Moens, M. The Added Value of High Dose Spinal Cord Stimulation in Patients with Failed Back Surgery Syndrome after Conversion from Standard Spinal Cord Stimulation. J. Clin. Med. 2020, 9, 3126. [Google Scholar] [CrossRef]
- Courtney, P.; Espinet, A.; Mitchell, B.; Russo, M.; Muir, A.; Verrills, P.; Davis, K. Improved Pain Relief With Burst Spinal Cord Stimulation for Two Weeks in Patients Using Tonic Stimulation: Results From a Small Clinical Study. Neuromodulation 2015, 18, 361–366. [Google Scholar] [CrossRef]
- Sammak, S.E.; Mualem, W.; Michalopoulos, G.D.; Romero, J.M.; Ha, C.T.; Hunt, C.L.; Bydon, M. Rescue therapy with novel waveform spinal cord stimulation for patients with failed back surgery syndrome refractory to conventional stimulation: A systematic review and meta-analysis. J. Neurosurg. Spine 2022, 37, 670–679. [Google Scholar] [CrossRef]
- Haider, N.; Ligham, D.; Quave, B.; Harum, K.E.; Garcia, E.A.; Gilmore, C.A.; Miller, N.; Moore, G.A.; Bains, A.; Lechleiter, K.; et al. Spinal Cord Stimulation (SCS) Trial Outcomes After Conversion to a Multiple Waveform SCS System. Neuromodulation 2018, 21, 504–507. [Google Scholar] [CrossRef]
- Billot, M.; Naiditch, N.; Brandet, C.; Lorgeoux, B.; Baron, S.; Ounajim, A.; Roulaud, M.; Roy-Moreau, A.; de Montgazon, G.; Charrier, E.; et al. Comparison of conventional, burst and high-frequency spinal cord stimulation on pain relief in refractory failed back surgery syndrome patients: Study protocol for a prospective randomized double-blinded cross-over trial (MULTIWAVE study). Trials 2020, 21, 696. [Google Scholar] [CrossRef] [PubMed]
- Rigoard, P.; Ounajim, A.; Goudman, L.; Banor, T.; Héroux, F.; Roulaud, M.; Babin, E.; Bouche, B.; Page, P.; Lorgeoux, B.; et al. The Challenge of Converting “Failed Spinal Cord Stimulation Syndrome” Back to Clinical Success, Using SCS Reprogramming as Salvage Therapy, through Neurostimulation Adapters Combined with 3D-Computerized Pain Mapping Assessment: A Real Life Retrospective Study. J. Clin. Med. 2022, 11, 272. [Google Scholar] [CrossRef] [PubMed]
- Andrade, P.; Heiden, P.; Visser-Vandewalle, V.; Matis, G. 1.2 kHz High-Frequency Stimulation as a Rescue Therapy in Patients With Chronic Pain Refractory to Conventional Spinal Cord Stimulation. Neuromodulation 2021, 24, 540–545. [Google Scholar] [CrossRef] [PubMed]
- Li, S.; Farber, J.P.; Linderoth, B.; Chen, J.; Foreman, R.D. Spinal Cord Stimulation with “Conventional Clinical” and Higher Frequencies on Activity and Responses of Spinal Neurons to Noxious Stimuli: An Animal Study. Neuromodulation 2018, 21, 440–447. [Google Scholar] [CrossRef] [PubMed]
- Rubinstein, J.T. Axon termination conditions for electrical stimulation. IEEE Trans. Biomed. Eng. 1993, 40, 654–663. [Google Scholar] [CrossRef] [PubMed]
- Metzger, C.S.; Hammond, M.B.; Paz-Solis, J.F.; Newton, W.J.; Thomson, S.J.; Pei, Y.; Jain, R.; Moffitt, M.; Annecchino, L.; Doan, Q. A novel fast-acting sub-perception spinal cord stimulation therapy enables rapid onset of analgesia in patients with chronic pain. Expert. Rev. Med. Devices 2021, 18, 299–306. [Google Scholar] [CrossRef] [PubMed]
- Gilbert, J.E.; Titus, N.; Zhang, T.; Esteller, R.; Grill, W.M. Surround Inhibition Mediates Pain Relief by Low Amplitude Spinal Cord Stimulation: Modeling and Measurement. Eneuro 2022, 9, ENEURO.0058-22.2022. [Google Scholar] [CrossRef] [PubMed]
- Boonstra, A.M.; Stewart, R.E.; Köke, A.J.; Oosterwijk, R.F.; Swaan, J.L.; Schreurs, K.M.; Schiphorst Preuper, H.R. Cut-Off Points for Mild, Moderate, and Severe Pain on the Numeric Rating Scale for Pain in Patients with Chronic Musculoskeletal Pain: Variability and Influence of Sex and Catastrophizing. Front. Psychol. 2016, 7, 1466. [Google Scholar] [CrossRef]
- D’Souza, R.S.; Her, Y.F. Stimulation holiday rescues analgesia after habituation and loss of efficacy from 10-kilohertz dorsal column spinal cord stimulation. Reg. Anesth. Pain. Med. 2022, 47, 722–727. [Google Scholar] [CrossRef]
- Patel, S.K.; Gozal, Y.M.; Saleh, M.S.; Gibson, J.L.; Karsy, M.; Mandybur, G.T. Spinal cord stimulation failure: Evaluation of factors underlying hardware explantation. J. Neurosurg. Spine 2019, 32, 133–138. [Google Scholar] [CrossRef]
- Love-Jones, S.; Thomson, S.; Rauck, R.; Group, R.; Woon, R.; Jain, R. ESRA19-0159 A prospective global registry of real-world outcomes using spinal cord stimulation systems for chronic pain. Reg. Anesth. Pain Med. 2019, 44, A77. [Google Scholar] [CrossRef]
- Deer, T.; Skaribas, I.; McJunkin, T.; Nelson, C.; Salmon, J.; Darnule, A.; Braswell, J.; Russo, M.; Fernando Gomezese, O. Results From the Partnership for Advancement in Neuromodulation Registry: A 24-Month Follow-Up. Neuromodulation 2016, 19, 179–187. [Google Scholar] [CrossRef]
- Kapural, L.; Sayed, D.; Kim, B.; Harstroem, C.; Deering, J. Retrospective Assessment of Salvage to 10 kHz Spinal Cord Stimulation (SCS) in Patients Who Failed Traditional SCS Therapy: RESCUE Study. J. Pain. Res. 2020, 13, 2861–2867. [Google Scholar] [CrossRef] [PubMed]
- Cordero Tous, N.; Sánchez Corral, C.; Ortiz García, I.M.; Jover Vidal, A.; Gálvez Mateos, R.; Olivares Granados, G. High-frequency spinal cord stimulation as rescue therapy for chronic pain patients with failure of conventional spinal cord stimulation. Eur. J. Pain 2021, 25, 1603–1611. [Google Scholar] [CrossRef] [PubMed]
- North, J.; Loudermilk, E.; Lee, A.; Sachdeva, H.; Kaiafas, D.; Washabaugh, E.; Sheth, S.; Scowcroft, J.; Mekhail, N.; Lampert, B.; et al. Outcomes of a Multicenter, Prospective, Crossover, Randomized Controlled Trial Evaluating Subperception Spinal Cord Stimulation at ≤1.2 kHz in Previously Implanted Subjects. Neuromodulation 2020, 23, 102–108. [Google Scholar] [CrossRef] [PubMed]
- Rigoard, P.; Ounajim, A.; Goudman, L.; Louis, P.Y.; Slaoui, Y.; Roulaud, M.; Naiditch, N.; Bouche, B.; Page, P.; Lorgeoux, B.; et al. A Novel Multi-Dimensional Clinical Response Index Dedicated to Improving Global Assessment of Pain in Patients with Persistent Spinal Pain Syndrome after Spinal Surgery, Based on a Real-Life Prospective Multicentric Study (PREDIBACK) and Machine Learning Techniques. J. Clin. Med. 2021, 10, 4910. [Google Scholar] [CrossRef] [PubMed]
- Goudman, L.; Rigoard, P.; Billot, M.; De Smedt, A.; Roulaud, M.; Consortium, D.; Moens, M. Spinal Cord Stimulation–Naïve Patients vs. Patients with Failed Previous Experiences with Standard Spinal Cord Stimulation: Two Distinct Entities or One Population? Neuromodulation 2023, 26, 157–163. [Google Scholar] [CrossRef] [PubMed]
- Leplus, A.; Voirin, J.; Cuny, E.; Onno, M.; Billot, M.; Rigoard, P.; Fontaine, D. Is Spinal Cord Stimulation Still Effective After One or More Surgical Revisions? Neuromodulation 2023, 26, 1102–1108. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Characteristics | Patients |
|---|---|
| Sex—female, n (%) | 27 (46.5) |
| Age (years), mean ± SD | 58.3 ± 9.5, n = 52 |
| Pain location prior to IPG conversion, n (%) (multiple locations may be reported) | Low back/legs, 33 (57.0) Lower limbs, 25 (43.1) |
| Pain prior to any SCS implant, mean ± SD | 7.8 ± 1.9, n = 47 |
| Pain prior to IPG conversion, mean ± SD ALL patients Rescue group Sustain group | 6.6 ± 2.5, n = 56 7.3 ± 1.7, n = 49 1.5 ± 1.2, n = 7 |
| Follow-up duration (years), mean ± SD [range in years] With previous IPG With new IPG | 5.6 ± 4.1 [0.02–8.25], n = 58 1.4 ± 1.4 [0.04–18.98], n = 50 |
| Waveform used priori conversion | |
| Paresthesia-based | n = 39 |
| Paresthesia-free | n = 15 |
| Device-Related Information | Patients |
|---|---|
| Patients prior to conversion, type of adaptors used n (%) M8/M1 adaptor S8 adaptor No adaptor | 44 (75.9) 9 (15.5) 5 (8.6) |
| Patients after conversion, type of IPG implanted, n (%) Spectra Wavewriter Wavewriter Alpha Precision Spectra Precision Montage Precision Novi Precision Plus Not reported | 29 (50.0) 12 (20.7) 11 (18.9) 3 (5.2) 1 (1.7) 1 (1.7) 1 (1.7) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rigoard, P.; Billot, M.; Bougeard, R.; Llopis, J.E.; Raoul, S.; Matis, G.; Vesper, J.; Belaïd, H. Improved Outcomes and Therapy Longevity after Salvage Using a Novel Spinal Cord Stimulation System for Chronic Pain: Multicenter, Observational, European Case Series. J. Clin. Med. 2024, 13, 1079. https://doi.org/10.3390/jcm13041079
Rigoard P, Billot M, Bougeard R, Llopis JE, Raoul S, Matis G, Vesper J, Belaïd H. Improved Outcomes and Therapy Longevity after Salvage Using a Novel Spinal Cord Stimulation System for Chronic Pain: Multicenter, Observational, European Case Series. Journal of Clinical Medicine. 2024; 13(4):1079. https://doi.org/10.3390/jcm13041079
Chicago/Turabian StyleRigoard, Philippe, Maxime Billot, Renaud Bougeard, Jose Emilio Llopis, Sylvie Raoul, Georgios Matis, Jan Vesper, and Hayat Belaïd. 2024. "Improved Outcomes and Therapy Longevity after Salvage Using a Novel Spinal Cord Stimulation System for Chronic Pain: Multicenter, Observational, European Case Series" Journal of Clinical Medicine 13, no. 4: 1079. https://doi.org/10.3390/jcm13041079
APA StyleRigoard, P., Billot, M., Bougeard, R., Llopis, J. E., Raoul, S., Matis, G., Vesper, J., & Belaïd, H. (2024). Improved Outcomes and Therapy Longevity after Salvage Using a Novel Spinal Cord Stimulation System for Chronic Pain: Multicenter, Observational, European Case Series. Journal of Clinical Medicine, 13(4), 1079. https://doi.org/10.3390/jcm13041079