

Relationship between Upper Limb Functional Assessment and Clinical Tests of Shoulder Mobility and Posture in Individuals Participating in Recreational Strength Training

 , ,
, ,  and
and 
Abstract
1. Introduction
2. Materials and Methods
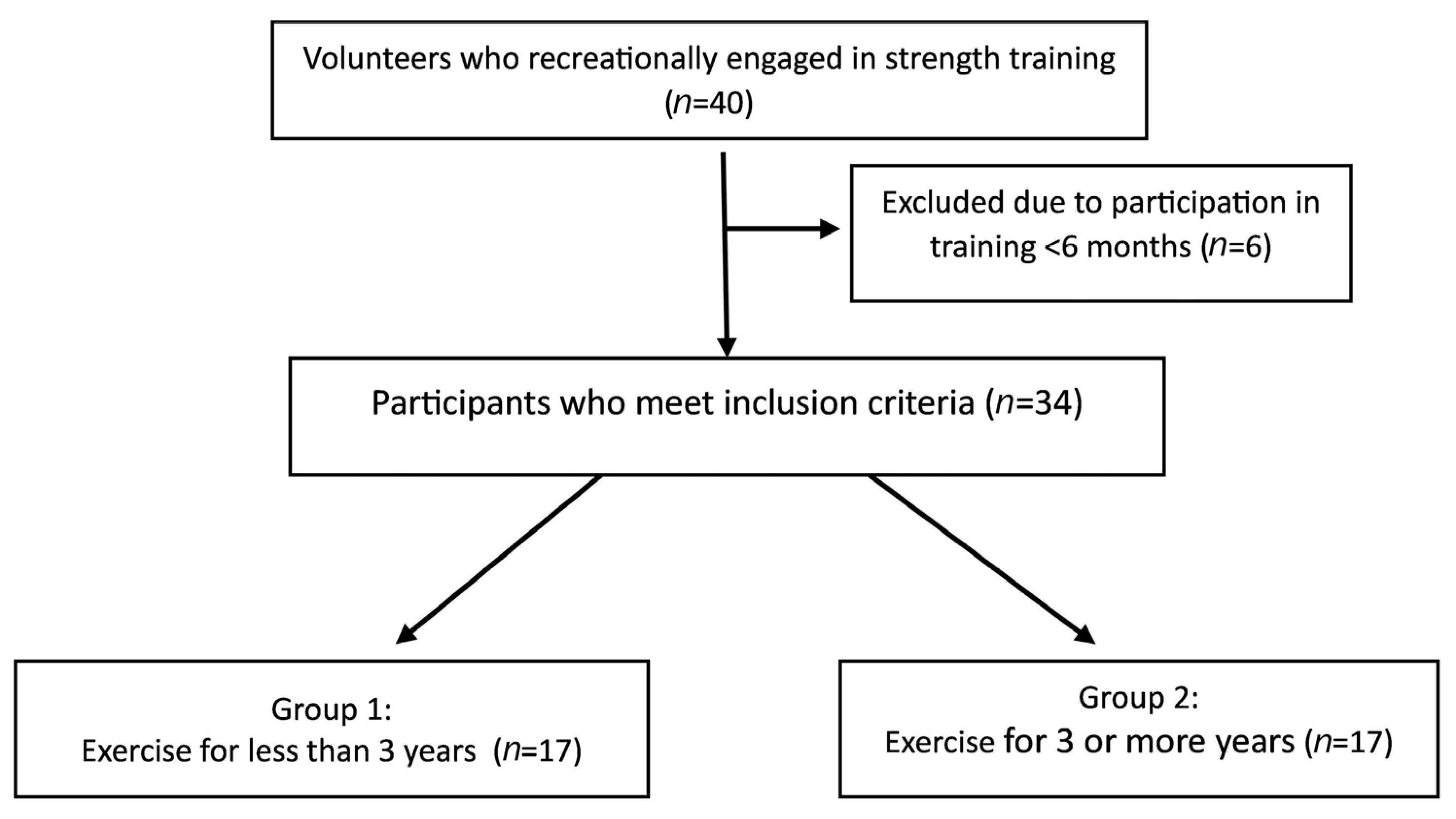
2.1. Subjects
2.2. Procedures
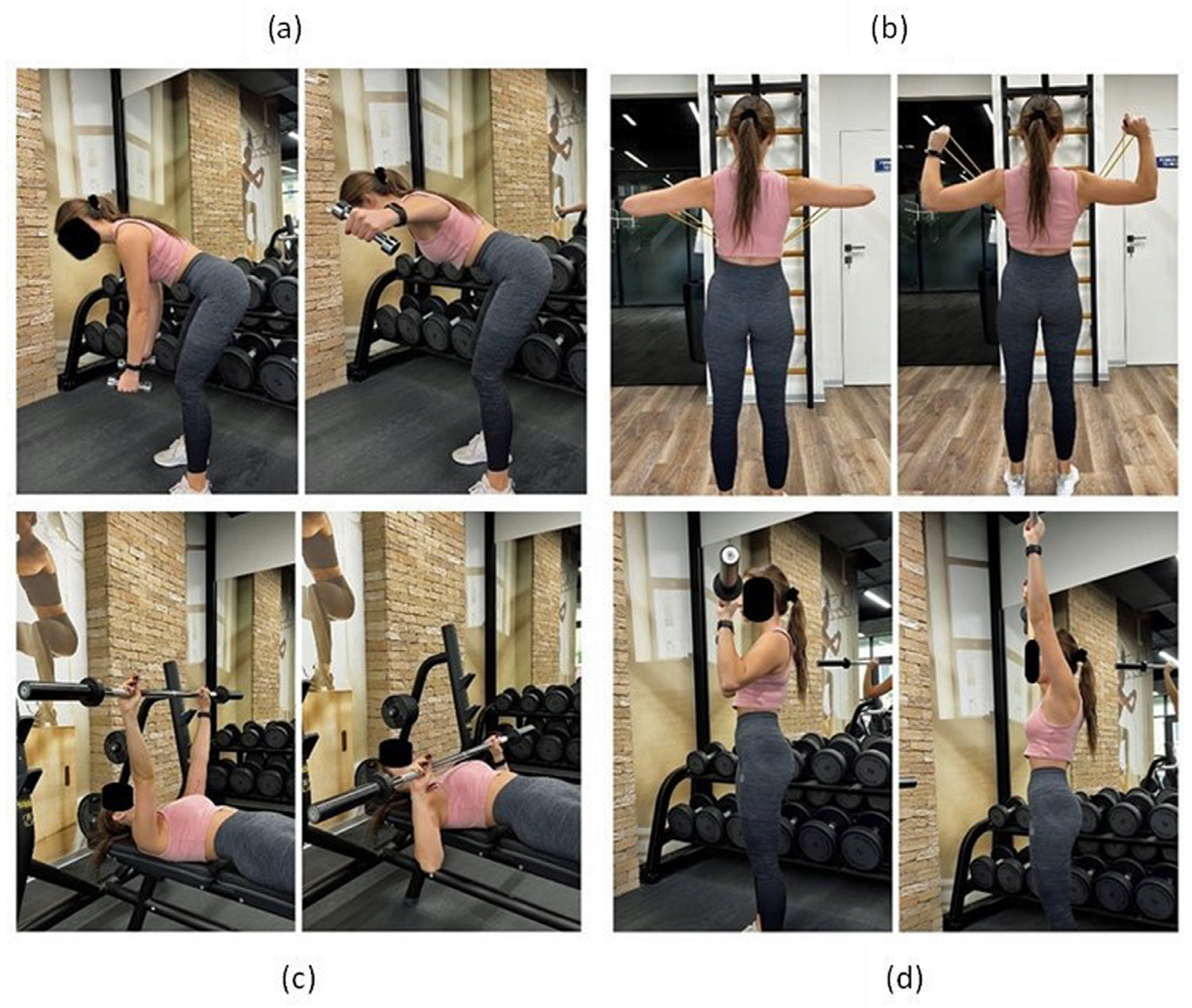
- (a)
- Bend over dumbbell row: an exercise involving the deltoid muscle, latissimus dorsi rhomboids and trapezius [13]. The exercise is performed in 3 sets of 10–15 repetitions. Dumbbell lifting movement is initiated by external rotation of the shoulders and scapula retraction.
- (b)
- Face pull: an exercise aimed at engaging the posterior deltoid, teres minor, trapezius, rhomboid major, and infraspinatus muscles [14]. The exercise is performed in 3 sets of 10–15 repetitions. External rotation movement is initiated by retraction and depression of the scapulae.
- (c)
- Chest press: an exercise involving mainly the pectoralis major muscle. The exercise is performed in 3 sets of 5–10 repetitions of lowering the barbell to the chest.
- (d)
- Military press: an exercise involving anterior and middle supraspinatus muscle and the pectoralis major muscle. The exercise is performed in 3 sets of 8–12 repetitions. The barbell is pressed upwards, with retraction of the head.
2.3. Lateral Scapular Slide Test
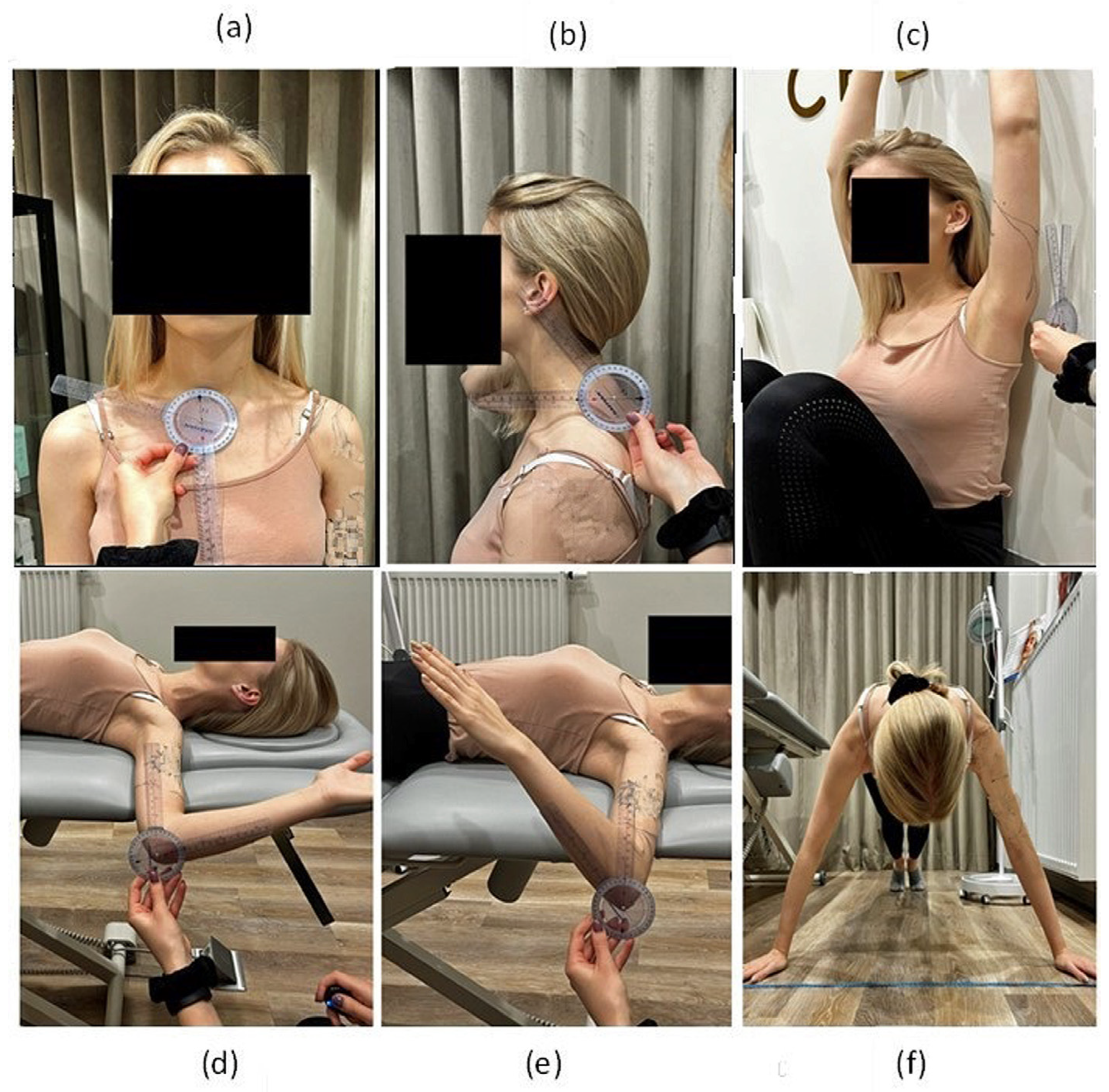
2.4. Assessment of Clavicle Alignment
2.5. Assessment of Head Position
2.6. Shoulder Mobility: Back-to-Wall Shoulder Flexion Test
2.7. Shoulder Mobility: Rotations
2.8. Closed Kinetic Chain Upper Limb Test
2.9. Statistical Analysis
3. Results
4. Discussion
5. Study Limitation
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Jaworski, Ł.; Karpiński, R.; Dobrowolska, A. Biomechanics of the Upper Limb. J. Technol. Exploit. Mech. Eng. 2016, 2, 56–59. [Google Scholar] [CrossRef]
- da Silva, R.T. Sports Injuries of the Upper Limbs. Rev. Bras. Ortop. 2010, 45, 122–131. [Google Scholar] [CrossRef] [PubMed]
- DeCastro, A. Common Upper-Extremity Injuries. Prim Care 2020, 47, 105–114. [Google Scholar] [CrossRef] [PubMed]
- Ootes, D.; Lambers, K.T.; Ring, D.C. The Epidemiology of Upper Extremity Injuries Presenting to the Emergency Department in the United States. Hand 2012, 7, 18–22. [Google Scholar] [CrossRef] [PubMed]
- Knapik, J.J. The Importance of Physical Fitness for Injury Prevention: Part 1. J. Spec. Oper. Med. 2015, 15, 123–127. [Google Scholar] [CrossRef] [PubMed]
- Farley, J.B.; Barrett, L.M.; Keogh, J.W.L.; Woods, C.T.; Milne, N. The Relationship between Physical Fitness Attributes and Sports Injury in Female, Team Ball Sport Players: A Systematic Review. Sports Med. Open 2020, 6, 45. [Google Scholar] [CrossRef] [PubMed]
- Guirelli, A.R.; dos Santos, J.M.; Cabral, E.M.G.; Pinto, J.P.C.; De Lima, G.A.; Felicio, L.R. Relationship between Upper Limb Physical Performance Tests and Muscle Strength of Scapular, Shoulder and Spine Stabilizers: A Cross-Sectional Study. J. Bodyw. Mov. Ther. 2021, 27, 612–619. [Google Scholar] [CrossRef]
- Giuseppe, L.U.; Laura, R.A.; Berton, A.; Candela, V.; Massaroni, C.; Carnevale, A.; Stelitano, G.; Schena, E.; Nazarian, A.; DeAngelis, J.; et al. Scapular Dyskinesis: From Basic Science to Ultimate Treatment. Int. J. Environ. Res. Public Health 2020, 17, 2974. [Google Scholar] [CrossRef]
- Larsen, C.M.; Juul-Kristensen, B.; Lund, H.; Søgaard, K. Measurement Properties of Existing Clinical Assessment Methods Evaluating Scapular Positioning and Function. A Systematic Review. Physiother. Theory Pract. 2014, 30, 453–482. [Google Scholar] [CrossRef]
- Decleve, P.; Attar, T.; Benameur, T.; Gaspar, V.; Van Cant, J.; Cools, A.M. The “Upper Limb Rotation Test”: Reliability and Validity Study of a New Upper Extremity Physical Performance Test. Phys. Ther. Sport 2020, 42, 118–123. [Google Scholar] [CrossRef]
- Hurwitz, E.L.; Morgenstern, H.; Chiao, C. Effects of Recreational Physical Activity and Back Exercises on Low Back Pain and Psychological Distress: Findings From the UCLA Low Back Pain Study. Am. J. Public Health 2005, 95, 1817–1824. [Google Scholar] [CrossRef] [PubMed]
- Škarabot, J.; Balshaw, T.G.; Maeo, S.; Massey, G.J.; Lanza, M.B.; Maden-Wilkinson, T.M.; Folland, J.P. Neural Adaptations to Long-Term Resistance Training: Evidence for the Confounding Effect of Muscle Size on the Interpretation of Surface Electromyography. J. Appl. Physiol. 2021, 131, 702–715. [Google Scholar] [CrossRef] [PubMed]
- Delavier, F.; Gundill, M. The Strength Training Anatomy Workout; Human Kinetics: Champaign, IL, USA, 2011. [Google Scholar]
- Starrett, K.; Cordoza, G. Becoming a Supple Leopard” The Ultimate Guide to Resolving Pain, Preventing Injury, and Optimizing Athletic Performance; Victory Belt Publishing: Las Vegas, NV, USA, 2015; pp. 114–115. [Google Scholar]
- Ozunlu, N.; Tekeli, H.; Baltaci, G. Lateral Scapular Slide Test and Scapular Mobility in Volleyball Players. J. Athl. Train. 2011, 46, 438–444. [Google Scholar] [CrossRef] [PubMed]
- Shadmehr, A.; Bagheri, H.; Ansari, N.N.; Sarafraz, H. The Reliability Measurements of Lateral Scapular Slide Test at Three Different Degrees of Shoulder Joint Abduction. Br. J. Sports Med. 2010, 44, 289–293. [Google Scholar] [CrossRef]
- Wannaprom, N.; Jull, G.; Treleaven, J.; Warner, M.B.; Kamnardsiri, T.; Uthaikhup, S. Clavicular and Scapular, but Not Spinal Kinematics Vary with Scapular Dyskinesis Type during Arm Elevation and Lowering in Persons with Neck Pain. Gait Posture 2022, 97, 48–55. [Google Scholar] [CrossRef] [PubMed]
- Ha, S.; Kwon, O.; Weon, J.; Kim, M.; Kim, S. Reliability and Validity of Goniometric and Photographic Measurements of Clavicular Tilt Angle. Man. Ther. 2013, 18, 367–371. [Google Scholar] [CrossRef] [PubMed]
- Naik, R.; Ingole, P.M. Modified Universal Goniometer for Objective Assessment of Forward Head Posture in Clinical Settings. MGM J. Med. Sci. 2018, 5, 121–124. [Google Scholar] [CrossRef]
- Welch, E.S.; Watson, M.D.; Davies, G.J.; Riemann, B.L. Biomechanical Analysis of the Closed Kinetic Chain Upper Extremity Stability Test in Healthy Young Adults. Phys. Ther. Sport 2020, 45, 120–125. [Google Scholar] [CrossRef]
- Silva, Y.A.; Novaes, W.A.; Dos Passos, M.H.P.; Nascimento, V.Y.S.; Cavalcante, B.R.; Pitangui, A.C.R.; De Araújo, R.C. Reliability of the Closed Kinetic Chain Upper Extremity Stability Test in Young Adults. Phys. Ther. Sport 2019, 38, 17–22. [Google Scholar] [CrossRef]
- Tomczak, M.; Tomczak, E. The Need to Report Effect Size Estimates Revisited. An Overview of Some Recommended Measures of Effect Size. Trends Sport Sci. 2014, 1, 19–25. [Google Scholar]
- Faul, F.; Erdfelder, E.; Lang, A.-G.; Buchner, A. G*Power 3: A Flexible Statistical Power Analysis Program for the Social, Behavioral, and Biomedical Sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef]
- Said, M.A.; Almatar, A.A.; Alibrahim, M.S. Higher Sedentary Behaviors and Lower Levels of Specific Knowledge Are Risk Factors for Physical Activity-Related Injuries in Saudi Adolescents. Int. J. Environ. Res. Public Health 2023, 20, 4610. [Google Scholar] [CrossRef]
- Alzahrani, H.; Mackey, M.; Stamatakis, E.; Zadro, J.R.; Shirley, D. The Association between Physical Activity and Low Back Pain: A Systematic Review and Meta-Analysis of Observational Studies. Sci. Rep. 2019, 9, 8244. [Google Scholar] [CrossRef]
- Aragón-Vela, J.; Solis-Urra, P.; Ruiz-Ojeda, F.J.; Álvarez-Mercado, A.I.; Olivares-Arancibia, J.; Plaza-Diaz, J. Impact of Exercise on Gut Microbiota in Obesity. Nutrients 2021, 13, 3999. [Google Scholar] [CrossRef] [PubMed]
- Yizengaw, M.A.; Mustofa, S.Y.; Ashagrie, H.E.; Zeleke, T.G. Prevalence and Factors Associated with Work-Related Musculoskeletal Disorder among Health Care Providers Working in the Operation Room. Ann. Med. Surg. 2021, 72, 102989. [Google Scholar] [CrossRef] [PubMed]
- Bullo, V.; Gobbo, S.; Sciusco, S.; Cugusi, L.; Di Blasio, A.; Cruz-Díaz, D.; Bortoletto, A.; Priolo, G.; Bocalini, D.S.; Bergamin, M. Resistance Training Improves Physical Fitness and Reduces Pain Perception in Workers with Upper Limb Work-Related Musculoskeletal Disorders: A Pilot Study. Hygiene 2022, 2, 136–145. [Google Scholar] [CrossRef]
- Hägg, G.M. Human Muscle Fibre Abnormalities Related to Occupational Load. Eur. J. Appl. Physiol. 2000, 83, 159–165. [Google Scholar] [CrossRef]
- Rasotto, C.; Bergamin, M.; Simonetti, A.; Maso, S.; Bartolucci, G.B.; Ermolao, A.; Zaccaria, M. Tailored Exercise Program Reduces Symptoms of Upper Limb Work-Related Musculoskeletal Disorders in a Group of Metalworkers: A Randomized Controlled Trial. Man. Ther. 2015, 20, 56–62. [Google Scholar] [CrossRef] [PubMed]
- Sundstrup, E.; Jakobsen, M.D.; Brandt, M.; Jay, K.; Aagaard, P.; Andersen, L.L. Strength Training Improves Fatigue Resistance and Self-Rated Health in Workers with Chronic Pain: A Randomized Controlled Trial. BioMed Res. Int. 2016, 2016, 4137918. [Google Scholar] [CrossRef] [PubMed]
- Melo, F.C.M.; de Lima, K.K.F.; Silveira, A.P.K.F.; de Azevedo, K.P.M.; Dos Santos, I.K.; de Medeiros, H.J.; Leitão, J.C.; Knackfuss, M.I. Physical Training and Upper-Limb Strength of People With Paraplegia: A Systematic Review. J. Sport Rehabil. 2019, 28, 288–293. [Google Scholar] [CrossRef]
- Neira, V.E.; Niemietz, T.D.; Farrell, J.W. The Effects of Exercise Training on Upper Extremity Function for Persons with Multiple Sclerosis: A Systematic Review. J. Rehabil. Med. Clin. Commun. 2022, 5, 2306. [Google Scholar] [CrossRef] [PubMed]
- Angulo, J.; El Assar, M.; Álvarez-Bustos, A.; Rodríguez-Mañas, L. Physical Activity and Exercise: Strategies to Manage Frailty. Redox Biol. 2020, 35, 101513. [Google Scholar] [CrossRef] [PubMed]
- Jacobs, P.L.; Nash, M.S.; Rusinowski, J.W. Circuit Training Provides Cardiorespiratory and Strength Benefits in Persons with Paraplegia. Med. Sci. Sports Exerc. 2001, 33, 711–717. [Google Scholar] [CrossRef] [PubMed]
- Perret, C.; De Jaegher, J.; Velstra, I.-M. Feasibility of an Upper Limb Strength Training Program in Persons with Spinal Cord Injury during Primary Rehabilitation—An Uncontrolled Interventional Study. Int. J. Environ. Res. Public Health 2022, 19, 14743. [Google Scholar] [CrossRef] [PubMed]
- Bye, E.A.; Harvey, L.A.; Gambhir, A.; Kataria, C.; Glinsky, J.V.; Bowden, J.L.; Malik, N.; Tranter, K.E.; Lam, C.P.; White, J.S.; et al. Strength Training for Partially Paralysed Muscles in People with Recent Spinal Cord Injury: A within-Participant Randomised Controlled Trial. Spinal Cord 2017, 55, 460–465. [Google Scholar] [CrossRef] [PubMed]
- Afonso, J.; Ramirez-Campillo, R.; Moscão, J.; Rocha, T.; Zacca, R.; Martins, A.; Milheiro, A.A.; Ferreira, J.; Sarmento, H.; Clemente, F.M. Strength Training versus Stretching for Improving Range of Motion: A Systematic Review and Meta-Analysis. Healthcare 2021, 9, 427. [Google Scholar] [CrossRef] [PubMed]
- Morton, S.K.; Whitehead, J.R.; Brinkert, R.H.; Caine, D.J. Resistance Training vs. Static Stretching: Effects on Flexibility and Strength. J. Strength Cond. Res. 2011, 25, 3391. [Google Scholar] [CrossRef]
- Barlow, J.C.; Benjamin, B.W.; Birt, P.J.; Hughes, C.J. Shoulder Strength and Range-Of-Motion Characteristics in Bodybuilders. J. Strength Cond. Res. 2002, 16, 367. [Google Scholar]
- Nuzzo, J.L. The Case for Retiring Flexibility as a Major Component of Physical Fitness. Sports Med. 2020, 50, 853–870. [Google Scholar] [CrossRef]
- Rose, M.B.; Noonan, T. Glenohumeral Internal Rotation Deficit in Throwing Athletes: Current Perspectives. Open Access J. Sports Med. 2018, 9, 69–78. [Google Scholar] [CrossRef]
- Molina-Garcia, P.; Mora-Gonzalez, J.; Migueles, J.H.; Rodriguez-Ayllon, M.; Esteban-Cornejo, I.; Cadenas-Sanchez, C.; Plaza-Florido, A.; Gil-Cosano, J.J.; Pelaez-Perez, M.A.; Garcia-Delgado, G.; et al. Effects of Exercise on Body Posture, Functional Movement, and Physical Fitness in Children With Overweight/Obesity. J. Strength Cond. Res. 2020, 34, 2146. [Google Scholar] [CrossRef] [PubMed]
- Ruivo, R.M.; Pezarat-Correia, P.; Carita, A.I. Effects of a Resistance and Stretching Training Program on Forward Head and Protracted Shoulder Posture in Adolescents. J. Manip. Physiol. Ther. 2017, 40, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Tucci, H.T.; Martins, J.; Sposito, G.d.C.; Camarini, P.M.F.; de Oliveira, A.S. Closed Kinetic Chain Upper Extremity Stability Test (CKCUES Test): A Reliability Study in Persons with and without Shoulder Impingement Syndrome. BMC Musculoskelet. Disord. 2014, 15, 1. [Google Scholar] [CrossRef] [PubMed]
- Hrysomallis, C. Effectiveness of Strengthening and Stretching Exercises for the Postural Correction of Abducted Scapulae: A Review. J. Strength Cond. Res. 2010, 24, 567. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Variable | Group | Mean | Std. Dev. | Median | Min–Max | Statistics | |
|---|---|---|---|---|---|---|---|
| Z | p | ||||||
| Age [years] | Beginner | 27.53 | 6.02 | 25 | 22–40 | −1.69 | 0.09 |
| Experienced | 30.12 | 5.01 | 29 | 22–39 | |||
| Heigh [cm] | Beginner | 175.59 | 8.92 | 176 | 159–193 | 0.33 | 0.74 |
| Experienced | 175.06 | 9.66 | 173 | 162–193 | |||
| Body mass [kg] | Beginner | 69.47 | 11.54 | 68 | 50–90 | −0.26 | 0.80 |
| Experienced | 72.24 | 16.36 | 65 | 50–98 | |||
| BMI [kg/m2] | Beginner | 22.46 | 2.85 | 21.56 | 18.82–28.08 | −0.84 | 0.40 |
| Experienced | 23.26 | 2.95 | 22.86 | 18.82–27.78 | |||
| Variable | Group | Mean | Std. Dev. | Median | Min | Max | Statistics | |
|---|---|---|---|---|---|---|---|---|
| Z | p | |||||||
| Scapula crest-dom-rest [cm] | Beginner | 5.90 | 1.09 | 5.75 | 4.50 | 8.00 | −1.42 | 0.16 |
| Experienced | 6.50 | 1.22 | 6.50 | 4.75 | 9.00 | |||
| Scapula crest-dom-hips [cm] | Beginner | 5.34 | 1.19 | 5.00 | 3.75 | 8.00 | −0.83 | 0.41 |
| Experienced | 5.65 | 1.18 | 5.50 | 3.50 | 7.75 | |||
| Scapula crest-dom-abduction [cm] | Beginner | 3.87 | 0.90 | 4.00 | 2.50 | 6.00 | −0.76 | 0.45 |
| Experienced | 4.29 | 1.43 | 4.25 | 2.00 | 6.75 | |||
| Scapula crest-ndom-rest [cm] | Beginner | 5.68 | 1.23 | 5.50 | 4.00 | 8.00 | −1.09 | 0.28 |
| Experienced | 6.19 | 1.24 | 6.00 | 4.00 | 8.50 | |||
| Scapula crest-ndom-hips [cm] | Beginner | 5.07 | 1.16 | 5.00 | 3.50 | 7.00 | −0.92 | 0.36 |
| Experienced | 5.43 | 0.84 | 5.25 | 4.00 | 7.00 | |||
| Scapula crest-ndom-abduction [cm] | Beginner | 4.00 | 1.54 | 4.00 | 2.50 | 9.00 | −0.40 | 0.69 |
| Experienced | 4.09 | 1.31 | 4.00 | 2.00 | 6.25 | |||
| Scapula crest—Difference -rest [cm] | Beginner | 0.75 | 0.49 | 0.75 | 0.00 | 2.00 | 0.30 | 0.77 |
| Experienced | 0.78 | 0.71 | 0.50 | 0.00 | 3.00 | |||
| Scapula crest—Difference -hips [cm] | Beginner | 0.79 | 0.64 | 0.50 | 0.00 | 2.50 | 0.97 | 0.33 |
| Experienced | 0.51 | 0.30 | 0.50 | 0.00 | 1.00 | |||
| Scapula crest—Difference -abduction [cm] | Beginner | 0.54 | 0.75 | 0.25 | 0.00 | 3.00 | −0.56 | 0.57 |
| Experienced | 0.47 | 0.32 | 0.50 | 0.00 | 1.00 | |||
| Lower angle-dom-rest [cm] | Beginner | 8.76 | 1.40 | 9.00 | 6.00 | 11.00 | 0.71 | 0.48 |
| Experienced | 8.44 | 1.37 | 8.50 | 6.50 | 10.50 | |||
| Lower angle-dom-hips [cm] | Beginner | 8.96 | 1.57 | 8.75 | 7.00 | 12.50 | −0.05 | 0.96 |
| Experienced | 8.79 | 1.35 | 8.50 | 6.00 | 11.00 | |||
| Lower angle-dom-abduction [cm] | Beginner | 8.87 | 1.67 | 9.00 | 6.00 | 12.00 | −0.26 | 0.79 |
| Experienced | 8.96 | 1.80 | 9.00 | 5.00 | 12.25 | |||
| Lower angle-ndom-rest [cm] | Beginner | 8.15 | 1.32 | 8.00 | 5.50 | 10.75 | −0.14 | 0.89 |
| Experienced | 8.35 | 1.36 | 8.00 | 6.00 | 11.00 | |||
| Lower angle-ndom-hips [cm] | Beginner | 8.60 | 1.49 | 8.25 | 6.50 | 11.50 | −0.36 | 0.72 |
| Experienced | 8.71 | 1.48 | 8.50 | 6.50 | 12.00 | |||
| Lower angle-ndom-abduction [cm] | Beginner | 9.09 | 1.43 | 9.00 | 6.50 | 11.00 | 0.26 | 0.80 |
| Experienced | 8.87 | 1.90 | 9.00 | 5.00 | 11.75 | |||
| Lower angle- Difference -rest [cm] | Beginner | 0.97 | 0.86 | 0.75 | 0.25 | 3.50 | 1.35 | 0.18 |
| Experienced | 0.59 | 0.38 | 0.50 | 0.00 | 1.50 | |||
| Lower angle- Difference -hips [cm] | Beginner | 0.97 | 0.86 | 0.50 | 0.00 | 3.00 | 1.12 | 0.26 |
| Experienced | 0.59 | 0.45 | 0.50 | 0.00 | 1.50 | |||
| Lower angle- Difference -abduction [cm] | Beginner | 1.04 | 1.02 | 1.00 | 0.00 | 3.00 | 0.19 | 0.85 |
| Experienced | 0.79 | 0.84 | 0.50 | 0.00 | 2.75 | |||
| Head posture in standing [°] | Beginner | 47.35 | 5.98 | 48.00 | 36.00 | 59.00 | −1.42 | 0.16 |
| Experienced | 50.26 | 4.80 | 49.00 | 40.00 | 61.50 | |||
| Head posture in sitting [°] | Beginner | 46.71 | 7.00 | 47.00 | 36.00 | 60.00 | −1.12 | 0.26 |
| Experienced | 48.71 | 6.02 | 50.00 | 38.00 | 65.00 | |||
| Clavicle position dom [°] | Beginner | 110.03 | 6.06 | 110.00 | 99.00 | 120.50 | 1.95 | 0.05 |
| Experienced | 105.50 | 6.09 | 105.00 | 95.00 | 119.00 | |||
| Clavicle position ndom [°] | Beginner | 109.35 | 4.38 | 110.00 | 101.00 | 116.00 | 0.97 | 0.33 |
| Experienced | 107.38 | 5.38 | 106.00 | 99.50 | 116.00 | |||
| Clavicle difference [°] | Beginner | 3.38 | 3.09 | 2.00 | 0.50 | 11.00 | −0.33 | 0.74 |
| Experienced | 4.00 | 4.30 | 3.00 | 0.00 | 17.50 | |||
| Variable | Group | Mean | Std. Dev. | Median | Min | Max | Statistics | |
|---|---|---|---|---|---|---|---|---|
| Z | p | |||||||
| Back-to-wall shoulder test dom [°] | Beginner | 19.71 | 12.39 | 20.00 | 0.00 | 50.00 | 3.37 | <0.001 * ES = 0.58 (large) |
| Experienced | 6.41 | 6.64 | 5.00 | 0.00 | 20.00 | |||
| Back-to-wall shoulder test ndom [°] | Beginner | 18.65 | 12.95 | 20.00 | 0.00 | 46.00 | 3.06 | 0.002 * ES = 0.52 (large) |
| Experienced | 5.59 | 5.39 | 5.00 | 0.00 | 14.00 | |||
| Back-to-wall shoulder test diff [°] | Beginner | 6.00 | 5.41 | 4.50 | 0.00 | 20.00 | 2.06 | 0.04 * ES = 0.35 (moderate) |
| Experienced | 2.76 | 2.88 | 2.00 | 0.00 | 9.50 | |||
| Internal rotation dom [°] | Beginner | 57.15 | 11.98 | 53.00 | 37.50 | 76.50 | 0.95 | 0.34 |
| Experienced | 52.24 | 12.45 | 51.00 | 29.50 | 72.00 | |||
| Internal rotation ndom [°] | Beginner | 60.65 | 10.63 | 60.50 | 40.00 | 76.00 | 1.29 | 0.20 |
| Experienced | 55.82 | 11.75 | 57.00 | 35.50 | 75.00 | |||
| Internal rotation difference [°] | Beginner | 6.79 | 7.68 | 5.00 | 1.00 | 35.00 | −0.90 | 0.37 |
| Experienced | 8.47 | 6.73 | 5.00 | 2.50 | 24.00 | |||
| External rotation dom [°] | Beginner | 86.32 | 10.10 | 85.00 | 70.00 | 105.00 | −1.74 | 0.08 |
| Experienced | 94.38 | 13.84 | 94.50 | 71.50 | 131.50 | |||
| External rotation ndom [°] | Beginner | 87.53 | 12.06 | 87.00 | 65.00 | 115.00 | −1.98 | 0.047 * ES = 0.34 (moderate) |
| Experienced | 94.76 | 10.91 | 95.00 | 72.00 | 116.00 | |||
| External rotation difference [°] | Beginner | 6.68 | 5.74 | 6.00 | 0.00 | 21.00 | −0.03 | 0.97 |
| Experienced | 6.50 | 4.61 | 5.00 | 1.50 | 15.50 | |||
| Closed kinetic chain test [repetitions} | Beginner | 22.12 | 2.78 | 22.00 | 18.50 | 30.00 | −2.16 | 0.03 * ES = 0.37 (moderate) |
| Experienced | 25.65 | 5.10 | 24.00 | 19.00 | 35.00 | |||
| Variable | Group 1 (Beginner) | Group 2 | ||
|---|---|---|---|---|
| Spearman r | p-Value | Spearman r | p-Value | |
| Scapula crest-dom-rest | 0.31 | 0.22 | 0.56 (strong) | 0.02 * |
| Scapula crest-dom-hips | 0.08 | 0.75 | 0.67 (strong) | <0.01 * |
| Scapula crest-dom-abduction | −0.05 | 0.86 | 0.61 (strong) | 0.01 * |
| Scapula crest-ndom-rest | 0.42 | 0.09 | 0.68 (strong) | <0.01 * |
| Scapula crest-ndom-hips | 0.41 | 0.10 | 0.67 (strong) | <0.01 * |
| Scapula crest-ndom-abduction | 0.30 | 0.24 | 0.49 (strong) | 0.048 * |
| Lower angle-dom-rest | 0.48 | 0.05 | 0.27 | 0.29 |
| Lower angle-dom-hips | 0.32 | 0.22 | 0.28 | 0.27 |
| Lower angle-dom-abduction | 0.51 (strong) | 0.04 * | 0.30 | 0.25 |
| Lower angle-ndom-rest | 0.33 | 0.19 | 0.46 | 0.06 |
| Lower angle-ndom-hips | 0.38 | 0.13 | 0.27 | 0.29 |
| Lower angle-ndom-abduction | 0.34 | 0.18 | 0.24 | 0.35 |
| Scapula crest—Difference 1 | 0.30 | 0.24 | −0.14 | 0.58 |
| Scapula crest—Difference 2 | 0.22 | 0.39 | 0.02 | 0.94 |
| Scapula crest—Difference 3 | −0.07 | 0.80 | −0.13 | 0.62 |
| Lower angle- Difference 1 | 0.21 | 0.41 | 0.03 | 0.91 |
| Lower angle- Difference 2 | −0.16 | 0.54 | 0.21 | 0.43 |
| Lower angle- Difference 3 | 0.10 | 0.70 | 0.08 | 0.75 |
| Head posture in standing | −0.13 | 0.61 | −0.04 | 0.89 |
| Head posture in sitting | −0.11 | 0.67 | 0.08 | 0.77 |
| Clavicle position dom | 0.07 | 0.79 | 0.23 | 0.37 |
| Clavicle position ndom | 0.06 | 0.83 | −0.08 | 0.76 |
| Clavicle difference | 0.05 | 0.84 | −0.01 | 0.96 |
| Back-to-wall shoulder test dom | 0.26 | 0.32 | 0.13 | 0.63 |
| Back-to-wall shoulder test ndom | 0.28 | 0.27 | 0.23 | 0.38 |
| Back-to-wall shoulder test difference | −0.25 | 0.34 | −0.52 (strong) | 0.03 * |
| Internal rotation dom | −0.33 | 0.19 | −0.23 | 0.38 |
| Internal rotation ndom | −0.18 | 0.48 | −0.07 | 0.78 |
| Internal rotation difference | −0.09 | 0.73 | 0.04 | 0.89 |
| External rotation dom | 0.30 | 0.24 | −0.22 | 0.40 |
| External rotation ndom | 0.50 (strong) | 0.04* | −0.38 | 0.13 |
| External rotation difference | 0.14 | 0.58 | −0.36 | 0.15 |
| Variables | β | SE β | B | SE B | t | p-Value | Statistics |
|---|---|---|---|---|---|---|---|
| Intercept | - | - | 18.55 | 17.49 | 1.06 | 0.29 | R = 0.78 R2 = 0.60 SE = 0.34 |
| Sex | −0.18 | 0.17 | −0.17 | 0.17 | −1.00 | 0.32 | |
| Back-to-wall shoulder test ndom | −0.67 | 0.13 | −0.03 | 0.006 | −4.92 | <0.001 * | |
| Internal rotation dom | −0.38 | 0.13 | −0.02 | 0.005 | −2.83 | <0.01 * | |
| Closed kinetic chain test | 0.40 | 0.17 | 0.04 | 0.02 | 2.27 | 0.03 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zawadka, M.; Gaweł, M.; Tomczyk-Warunek, A.; Turżańska, K.; Blicharski, T. Relationship between Upper Limb Functional Assessment and Clinical Tests of Shoulder Mobility and Posture in Individuals Participating in Recreational Strength Training. J. Clin. Med. 2024, 13, 1028. https://doi.org/10.3390/jcm13041028
Zawadka M, Gaweł M, Tomczyk-Warunek A, Turżańska K, Blicharski T. Relationship between Upper Limb Functional Assessment and Clinical Tests of Shoulder Mobility and Posture in Individuals Participating in Recreational Strength Training. Journal of Clinical Medicine. 2024; 13(4):1028. https://doi.org/10.3390/jcm13041028
Chicago/Turabian StyleZawadka, Magdalena, Marta Gaweł, Agnieszka Tomczyk-Warunek, Karolina Turżańska, and Tomasz Blicharski. 2024. "Relationship between Upper Limb Functional Assessment and Clinical Tests of Shoulder Mobility and Posture in Individuals Participating in Recreational Strength Training" Journal of Clinical Medicine 13, no. 4: 1028. https://doi.org/10.3390/jcm13041028
APA StyleZawadka, M., Gaweł, M., Tomczyk-Warunek, A., Turżańska, K., & Blicharski, T. (2024). Relationship between Upper Limb Functional Assessment and Clinical Tests of Shoulder Mobility and Posture in Individuals Participating in Recreational Strength Training. Journal of Clinical Medicine, 13(4), 1028. https://doi.org/10.3390/jcm13041028