

Aspirin at 75 to 81 mg Daily for the Prevention of Preterm Pre-Eclampsia: Systematic Review and Meta-Analysis

 , and
, and
Abstract
1. Introduction
2. Materials and Methods
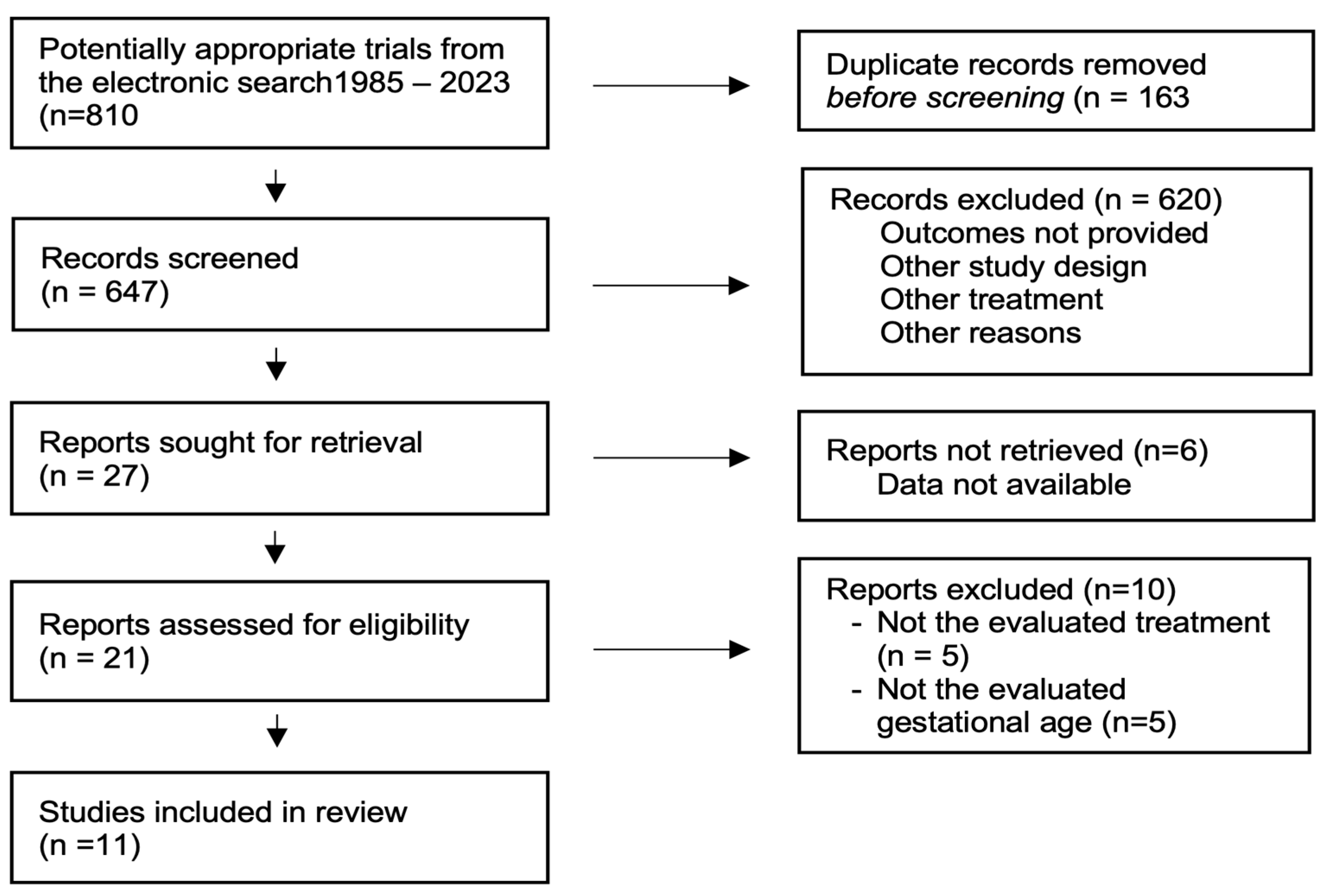
2.1. Study Selection
2.2. Data Extraction
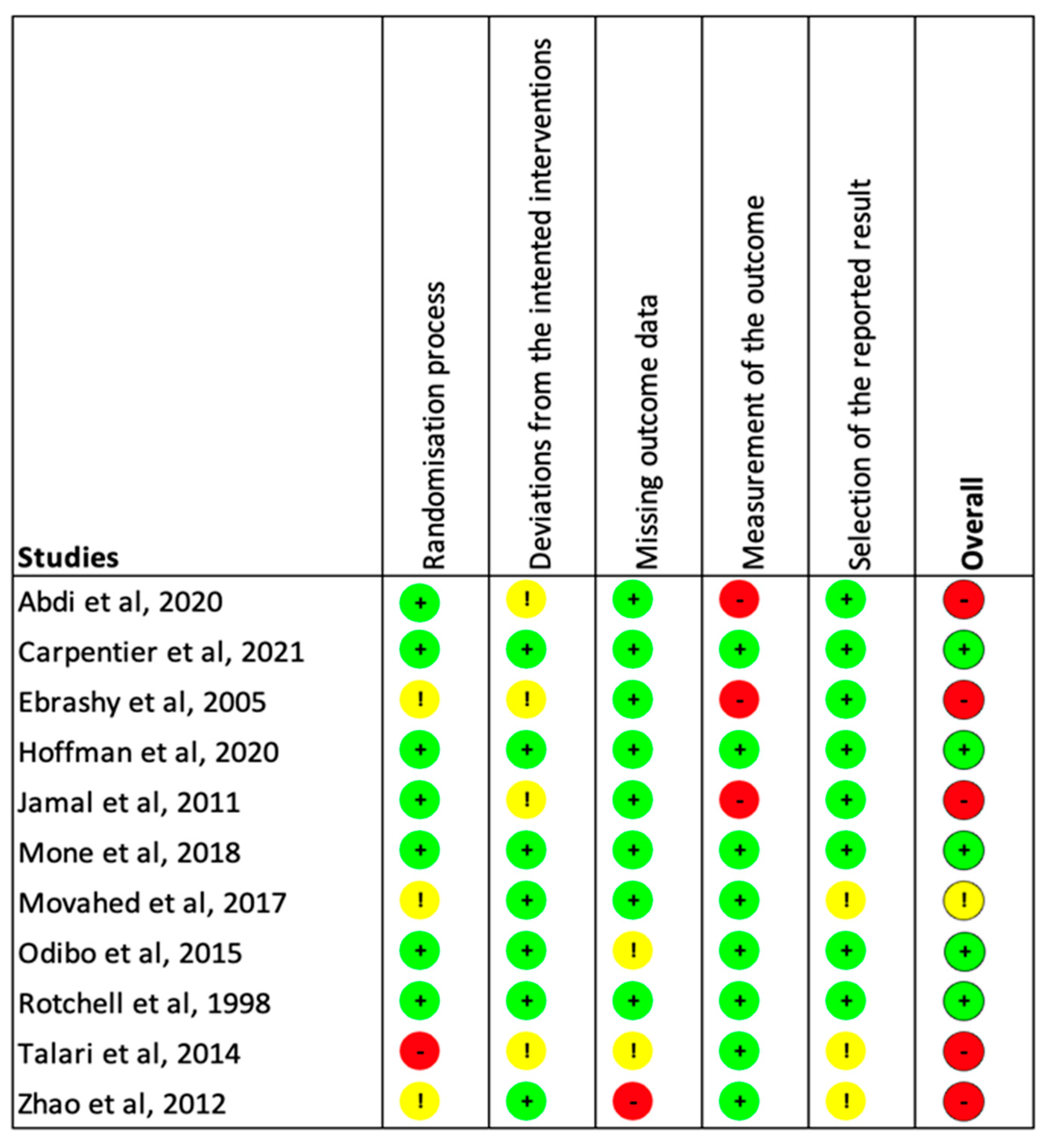
2.3. Assessment of Risk of Bias
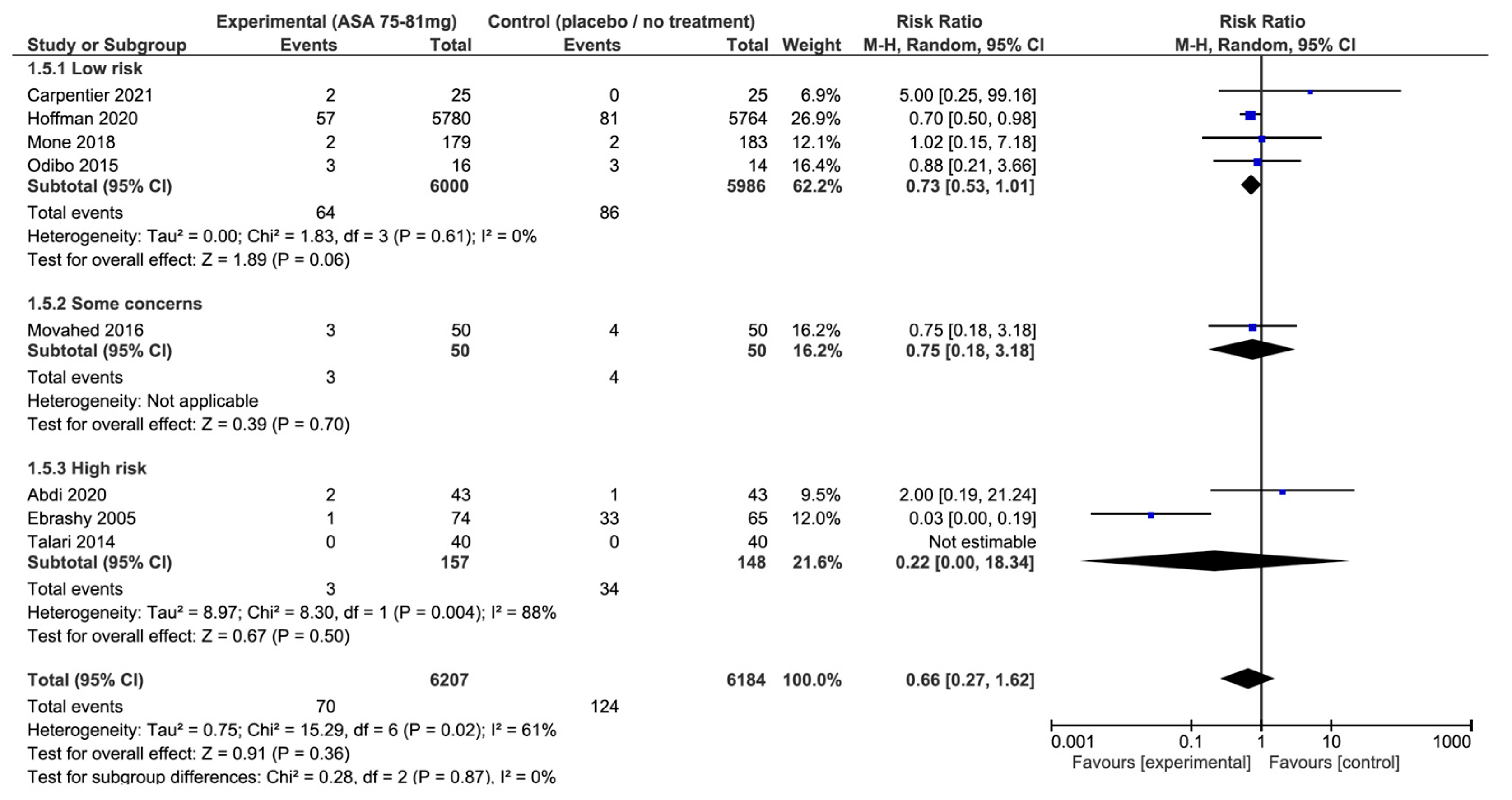
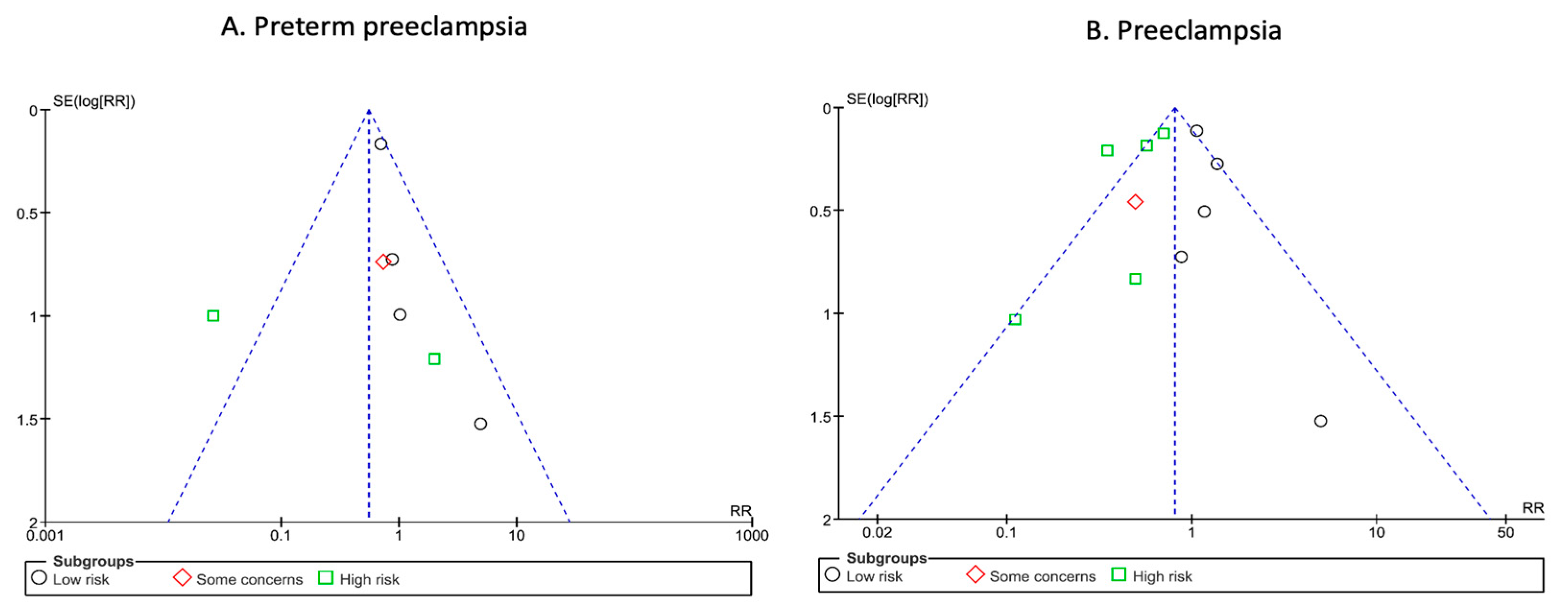
2.4. Data Synthesis and Statistical Analysis
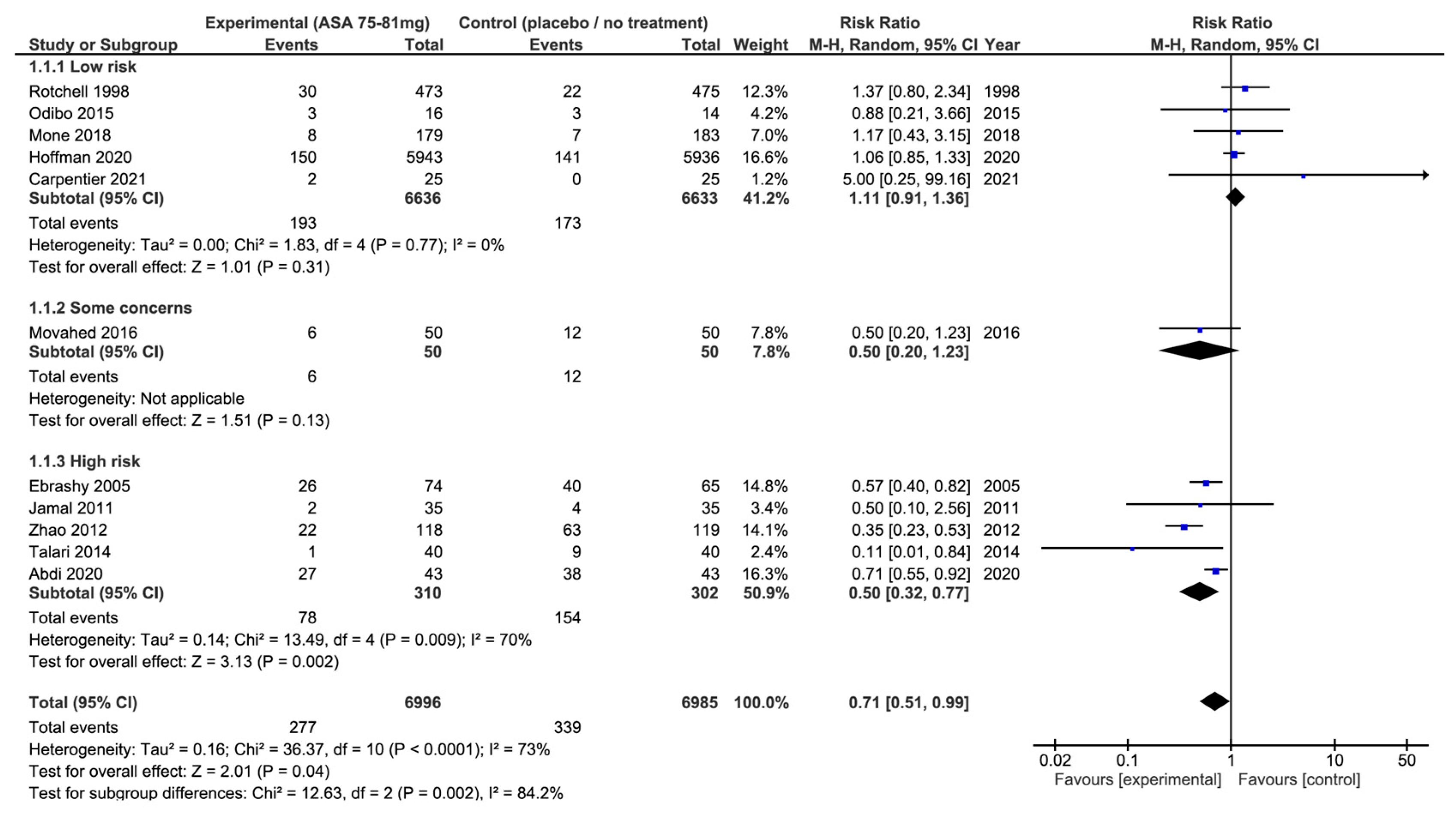
3. Results
4. Discussion
5. Conclusions
6. Future Directions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Gestational Hypertension and Preeclampsia: ACOG Practice Bulletin Summary, Number 222. Obstet. Gynecol. 2020, 135, 1492–1495. [CrossRef]
- Chappell, L.C.; Cluver, C.A.; Kingdom, J.; Tong, S. Pre-eclampsia. Lancet 2021, 398, 341–354. [Google Scholar] [CrossRef]
- Duley, L. The Global Impact of Pre-eclampsia and Eclampsia. Semin. Perinatol. 2009, 33, 130–137. [Google Scholar] [CrossRef] [PubMed]
- Hogan, M.C.; Foreman, K.J.; Naghavi, M.; Ahn, S.Y.; Wang, M.; Makela, S.M.; Lopez, A.D.; Lozano, R.; Murray, C.J. Maternal mortality for 181 countries, 1980–2008: A systematic analysis of progress towards Millennium Development Goal 5. Lancet 2010, 375, 1609–1623. [Google Scholar] [CrossRef] [PubMed]
- Lo, J.O.; Mission, J.F.; Caughey, A.B. Hypertensive disease of pregnancy and maternal mortality. Curr. Opin. Obstet. Gynecol. 2013, 25, 124–132. [Google Scholar] [CrossRef] [PubMed]
- Say, L.; Chou, D.; Gemmill, A.; Tunçalp, Ö.; Moller, A.-B.; Daniels, J.; Gülmezoglu, A.M.; Temmerman, M.; Alkema, L. Global causes of maternal death: A WHO systematic analysis. Lancet Glob. Health 2014, 2, e323–e333. [Google Scholar] [CrossRef] [PubMed]
- Steegers, E.A.P.; von Dadelszen, P.; Duvekot, J.J.; Pijnenborg, R. Pre-eclampsia. Lancet Lond. Engl. 2010, 376, 631–644. [Google Scholar] [CrossRef] [PubMed]
- Poon, L.C.; Shennan, A.; Hyett, J.A.; Kapur, A.; Hadar, E.; Divakar, H.; McAuliffe, F.; da Silva Costa, F.; von Dadelszen, P.; McIntyre, H.D.; et al. The International Federation of Gynecology and Obstetrics (FIGO) Initiative on Preeclampsia (PE): A Pragmatic Guide for First Trimester Screening and Prevention. Int. J. Gynaecol. Obstet. 2019, 145 (Suppl. S1), 1–33. [Google Scholar] [CrossRef] [PubMed]
- Dimitriadis, E.; Rolnik, D.L.; Zhou, W.; Estrada-Gutierrez, G.; Koga, K.; Francisco, R.P.V.; Whitehead, C.; Hyett, J.; Costa, F.d.S.; Nicolaides, K.; et al. Pre-eclampsia. Nat. Rev. Dis. Primer. 2023, 9, 8. [Google Scholar] [CrossRef]
- Ogge, G.; Chaiworapongsa, T.; Romero, R.; Hussein, Y.; Kusanovic, J.P.; Yeo, L.; Kim, C.J.; Hassan, S.S. Placental lesions associated with maternal underperfusion are more frequent in early-onset than in late-onset preeclampsia. J. Perinat. Med. 2011, 39, 641–652. [Google Scholar] [CrossRef]
- Bujold, E.; Roberge, S.; Lacasse, Y.; Bureau, M.; Audibert, F.; Marcoux, S.; Forest, J.-C.; Giguère, Y. Prevention of preeclampsia and intrauterine growth restriction with aspirin started in early pregnancy: A meta-analysis. Obstet. Gynecol. 2010, 116 2 Pt 1, 402–414. [Google Scholar] [CrossRef]
- Bujold, E.; Morency, A.M.; Roberge, S.; Lacasse, Y.; Forest, J.C.; Giguère, Y. Acetylsalicylic acid for the prevention of preeclampsia and intra-uterine growth restriction in women with abnormal uterine artery Doppler: A systematic review and meta-analysis. J. Obstet. Gynecol. Can. JOGC 2009, 31, 818–826. [Google Scholar] [CrossRef]
- Rolnik, D.L.; Wright, D.; Poon, L.C.; O’Gorman, N.; Syngelaki, A.; Paco Matallana, C. Aspirin versus Placebo in Pregnancies at High Risk for Preterm Preeclampsia. N. Engl. J. Med. 2017, 377, 613–622. [Google Scholar] [CrossRef]
- Roberge, S.; Bujold, E.; Nicolaides, K.H. Aspirin for the prevention of preterm and term preeclampsia: Systematic review and metaanalysis. Am. J. Obstet. Gynecol. 2018, 218, 1. [Google Scholar] [CrossRef]
- Roberge, S.; Villa, P.; Nicolaides, K.; Giguère, Y.; Vainio, M.; Bakthi, A.; Ebrashy, A.; Bujold, E. Early administration of low-dose aspirin for the prevention of preterm and term preeclampsia: A systematic review and meta-analysis. Fetal Diagn. Ther. 2012, 31, 141–146. [Google Scholar] [CrossRef]
- Bujold, E.; Roberge, S.; Nicolaides, K. Low-dose aspirin for prevention of adverse outcomes related to abnormal placentation. Prenat. Diagn 2014, 34, 642–648. [Google Scholar] [CrossRef] [PubMed]
- ACOG Committee Opinion No. 743: Low-Dose Aspirin Use During Pregnancy. Obstet. Gynecol. 2018, 132, e44–e52. [CrossRef]
- US Preventive Services Task Force. Aspirin Use to Prevent Preeclampsia and Related Morbidity and Mortality: US Preventive Services Task Force Recommendation Statement. JAMA 2021, 326, 1186–1191. [Google Scholar] [CrossRef] [PubMed]
- Magee, L.A.; Smith, G.N.; Bloch, C.; Côté, A.-M.; Jain, V.; Nerenberg, K.; von Dadelszen, P.; Helewa, M.; Rey, E. Guideline No. 426: Hypertensive Disorders of Pregnancy: Diagnosis, Prediction, Prevention, and Management. J. Obstet. Gynaecol. Can. 2022, 44, 547–571.e1. [Google Scholar] [CrossRef] [PubMed]
- Webster, K.; Fishburn, S.; Maresh, M.; Findlay, S.C.; Chappell, L.C.; Guideline Committee. Diagnosis and management of hypertension in pregnancy: Summary of updated NICE guidance. BMJ 2019, 366, l5119. [Google Scholar] [CrossRef] [PubMed]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. PLoS. Med. 2009, 6, e1000100. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savović, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.C.; et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [PubMed]
- Carpentier, C.; Guerby, P.; Camiré, B.; Tapp, S.; Boutin, A.; Bujold, E. Aspirin Responsiveness at a Dose of 80 mg and Its Impact on Birth Weight when Used in Twin Pregnancies: The GAP Pilot Randomized Trial. Am. J. Perinatol. 2022, 39, 1396–1400. [Google Scholar] [CrossRef] [PubMed]
- Abdi, N.; Rozrokh, A.; Alavi, A.; Zare, S.; Vafaei, H.; Asadi, N.; Kasraeian, M.; Hessami, K. The effect of aspirin on preeclampsia, intrauterine growth restriction and preterm delivery among healthy pregnancies with a history of preeclampsia. J. Chin. Med. Assoc. JCMA 2020, 83, 852–857. [Google Scholar] [CrossRef] [PubMed]
- Hoffman, M.K.; Goudar, S.S.; Kodkany, B.S.; Metgud, M.; Somannavar, M.; Okitawutshu, J.; Lokangaka, A.; Tshefu, A.; Bose, C.L.; Mwapule, A.; et al. Low-Dose Aspirin for the Prevention of Preterm Delivery in Nulliparous Women with a Singleton Pregnancy: A Randomised Multi-country Placebo Controlled Trial. Lancet Lond. Engl. 2020, 395, 285–293. [Google Scholar] [CrossRef]
- Jamal, A.; Milani, F.; Al-Yasin, A. Evaluation of the effect of metformin and aspirin on utero placental circulation of pregnant women with PCOS. Iran. J. Reprod. Med. 2012, 10, 265–270. [Google Scholar]
- Ebrashy, A.; Ibrahim, M.; Marzook, A.; Yousef, D. Usefulness of aspirin therapy in high-risk pregnant women with abnormal uterine artery Doppler ultrasound at 14–16 weeks pregnancy: Randomized controlled clinical trial. Croat. Med. J. 2005, 46, 826–831. [Google Scholar]
- Zhao, Y.M.; Xiao, L.P.; Hu, H.; Yang, X.N.; Xu, Y.Q.; Guo, L.M. Low-dose aspirin prescribed at bed time for the prevention of pre-eclampsia in high-risk pregnant women. Reprod. Contracept. 2012, 32, 355–359. [Google Scholar]
- Odibo, A.O.; Goetzinger, K.R.; Odibo, L.; Tuuli, M.G. Early prediction and aspirin for prevention of pre-eclampsia (EPAPP) study: A randomized controlled trial. Ultrasound Obstet. Gynecol. 2015, 46, 414–418. [Google Scholar] [CrossRef]
- Talari, H.; Mesdaghinia, E.; Abedzadeh Kalahroudi, M. Aspirin and preeclampsia prevention in patients with abnormal uterine artery blood flow. Iran. Red. Crescent Med. J. 2014, 16, e17175. [Google Scholar] [CrossRef][Green Version]
- Rotchell, Y.E.; Cruickshank, J.K.; Gay, M.P.; Griffiths, J.; Stewart, A.; Farrell, B.; Ayers, S.; Hennis, A.; Grant, A.; Duley, L.; et al. Barbados Low Dose Aspirin Study in Pregnancy (BLASP): A randomised trial for the prevention of pre-eclampsia and its complications. Br. J. Obstet. Gynaecol. 1998, 105, 286–292. [Google Scholar] [CrossRef]
- Movahed, F.; Lalooha, F.; Moinodin, R.; Dabbaghi Ghale, T.; Rezaee Majd, Z.; Yazdi, Z. The effect of aspirin in the prevention of preeclampsia in women with abnormal uterine artery doppler ultrasonography findings. J. Adv. Med. Biomed. Res. 2017, 25, 11–19. [Google Scholar]
- Mone, F.; Mulcahy, C.; McParland, P.; Breathnach, F.; Downey, P.; McCormack, D.; Culliton, M.; Stanton, A.; Cody, F.; Morrison, J.J.; et al. Trial of feasibility and acceptability of routine low-dose aspirin versus Early Screening Test indicated aspirin for pre-eclampsia prevention (TEST study): A multicentre randomised controlled trial. BMJ Open 2018, 8, e022056. [Google Scholar] [CrossRef]
- Van Doorn, R.; Mukhtarova, N.; Flyke, I.P.; Lasarev, M.; Kim, K.; Hennekens, C.H.; Hoppe, K.K. Dose of aspirin to prevent preterm preeclampsia in women with moderate or high-risk factors: A systematic review and meta-analysis. PLoS ONE 2021, 16, e0247782. [Google Scholar] [CrossRef]
- Roberge, S.; Nicolaides, K.; Demers, S.; Hyett, J.; Chaillet, N.; Bujold, E. The role of aspirin dose on the prevention of preeclampsia and fetal growth restriction: Systematic review and meta-analysis. Am. J. Obstet. Gynecol. 2017, 216, 110–120.e6. [Google Scholar] [CrossRef]
- Ghesquiere, L.; Guerby, P.; Marchant, I.; Kumar, N.; Zare, M.; Foisy, M.-A.; Roberge, S.; Bujold, E. Comparing aspirin 75 to 81 mg vs 150 to 162 mg for prevention of preterm preeclampsia: Systematic review and meta-analysis. Am. J. Obstet. Gynecol. MFM 2023, 5, 101000. [Google Scholar] [CrossRef]
- Sinha, N.; Singh, S.; Agarwal, M.; Manjhi, P.K.; Kumar, R.; Singh, S.K.; Priya, A. A Randomized Controlled Study Comparing the Efficacy of 75 mg Versus 150 mg Aspirin for the Prevention of Preeclampsia in High-Risk Pregnant Women. Cureus 2023, 15, e39752. [Google Scholar] [CrossRef] [PubMed]
- Rey, E.; Rivard, G.E. Is testing for aspirin response worthwhile in high-risk pregnancy? Eur. J. Obstet. Gynecol. Reprod. Biol. 2011, 157, 38–42. [Google Scholar] [CrossRef] [PubMed]
- Dumont, A.; Flahault, A.; Beaufils, M.; Verdy, E.; Uzan, S. Effect of aspirin in pregnant women is dependent on increase in bleeding time. Am. J. Obstet. Gynecol. 1999, 180 1 Pt 1, 135–140. [Google Scholar] [CrossRef] [PubMed]
- Caron, N.; Rivard, G.-E.; Michon, N.; Morin, F.; Pilon, D.; Moutquin, J.-M.; Rey, É. Low-dose ASA response using the PFA-100 in women with high-risk pregnancy. J. Obstet. Gynaecol. Can. JOGC 2009, 31, 1022–1027. [Google Scholar] [CrossRef] [PubMed]
- Askie, L.M.; Duley, L.; Henderson-Smart, D.J.; Stewart, L.A.; PARIS Collaborative Group. Antiplatelet agents for prevention of pre-eclampsia: A meta-analysis of individual patient data. Lancet Lond. Engl. 2007, 369, 1791–1798. [Google Scholar] [CrossRef]
- Duley, L.; Meher, S.; Hunter, K.E.; Seidler, A.L.; Askie, L.M. Antiplatelet agents for preventing pre-eclampsia and its complications. Cochrane Database Syst. Rev. 2019, 2019, CD004659. [Google Scholar] [CrossRef] [PubMed]
- Mendoza, M.; Bonacina, E.; Garcia-Manau, P.; López, M.; Caamiña, S.; Vives, À.; Lopez-Quesada, E.; Ricart, M.; Maroto, A.; de Mingo, L.; et al. Aspirin Discontinuation at 24 to 28 Weeks’ Gestation in Pregnancies at High Risk of Preterm Preeclampsia: A Randomized Clinical Trial. JAMA 2023, 329, 542–550. [Google Scholar] [CrossRef] [PubMed]
- Ghesquiere, L.; Demuth, B.; Bujold, E. Optimal dose of aspirin for the prevention of preterm preeclampsia. Am. J. Obstet. Gynecol. 2023, 229, 574–575. [Google Scholar] [CrossRef] [PubMed]
- Rolnik, D.L.; Syngelaki, A.; O’Gorman, N.; Wright, D.; Poon, L.C.; Nicolaides, K.H. ASPRE trial: Effects of aspirin on mean arterial blood pressure and uterine artery pulsatility index trajectories in pregnancy. Ultrasound Obstet. Gynecol. 2023, 61, 691–697. [Google Scholar] [CrossRef] [PubMed]
- Tan, M.Y.; Syngelaki, A.; Poon, L.C.; Rolnik, D.L.; O’Gorman, N.; Delgado, J.L.; Akolekar, R.; Konstantinidou, L.; Tsavdaridou, M.; Galeva, S.; et al. Screening for pre-eclampsia by maternal factors and biomarkers at 11–13 weeks’ gestation. Ultrasound Obstet. Gynecol. 2018, 52, 186–195. [Google Scholar] [CrossRef] [PubMed]
- Yu, C.K.H.; Papageorghiou, A.T.; Parra, M.; Palma Dias, R.; Nicolaides, K.H. Fetal Medicine Foundation Second Trimester Screening Group. Randomized controlled trial using low-dose aspirin in the prevention of pre-eclampsia in women with abnormal uterine artery Doppler at 23 weeks’ gestation. Ultrasound Obstet. Gynecol. 2003, 22, 233–239. [Google Scholar] [CrossRef] [PubMed]
- Jiang, Y.; Chen, Z.; Chen, Y.; Wei, L.; Gao, P.; Zhang, J.; Zhou, X.; Zhu, S.; Zhang, H.; Du, Y.; et al. Low dose aspirin use during pregnancy may be a potential risk for postpartum hemorrhage and increased blood loss: A systematic review and meta-analysis. Am. J. Obstet. Gynecol. MFM 2023, 5, 100878. [Google Scholar] [CrossRef]
- Ghesquiere, L.; Demuth, B.; Bujold, E. Reply: Current optimal dose of aspirin for the prevention of preterm preeclampsia. Am. J. Obstet. Gynecol. MFM 2023, 5, 101099. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| First Author (Year) | Country | N | Inclusion Criteria | Aspirin Dose | Control | GA * at Start (Weeks) | Primary Outcome |
|---|---|---|---|---|---|---|---|
| Carpentier (2022) [23] | Canada | 95 | Twin pregnancy | 80 mg | Placebo | 8 to 14 | Birth weight |
| Abdi (2020) [24] | Iran | 90 | Previous history of PE | 80 mg | Placebo | 12 to 15 | PE, IUGR, PTB * |
| Hoffman (2020) [25] | Several countries | 11,976 | Nulliparous women | 81 mg | Placebo | 6 to 14 | PTB |
| Jamal (2012) [26] | Iran | 70 | PCOS before pregnancy, no diabetes mellitus or hypertension. | 80 mg | No treatment | 6 to 12 | UtA * Doppler at 20 weeks |
| Ebrashy (2005) [27] | Croatie | 139 | High risk for HDP or IUGR and abnormal UtA Doppler | 75 mg | No treatment | 14 to 16 | PE, IUGR, PTB |
| Zhao (2012) [28] | Chine | 237 | High risk for HDP or IUGR | 75 mg | Placebo | 13 to 16 | PE, HDP |
| Odibo (2015) [29] | USA | 30 | High risk for HDP | 81 mg | Placebo | 11 to 14 | PE |
| Talari (2014) [30] | Iran | 80 | Abnormal UtA Doppler | 80 mg | Placebo | 12 to 16 | PE |
| Rotchell (1998) [31] | Barbados | 948 | Pregnancy before 32 weeks | 75 mg | Placebo | <16 | PE |
| Movahed (2017) [32] | Iran | 100 | Abnormal UtA Doppler | 80 mg | Placebo | 11 to 14 | PE, IUGR, PTB |
| Mone (2018) [33] | Dublin | 546 | Nulliparous | 75 mg | No treatment | 11 to 14 | Completion of research protocol |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Demuth, B.; Pellan, A.; Boutin, A.; Bujold, E.; Ghesquière, L. Aspirin at 75 to 81 mg Daily for the Prevention of Preterm Pre-Eclampsia: Systematic Review and Meta-Analysis. J. Clin. Med. 2024, 13, 1022. https://doi.org/10.3390/jcm13041022
Demuth B, Pellan A, Boutin A, Bujold E, Ghesquière L. Aspirin at 75 to 81 mg Daily for the Prevention of Preterm Pre-Eclampsia: Systematic Review and Meta-Analysis. Journal of Clinical Medicine. 2024; 13(4):1022. https://doi.org/10.3390/jcm13041022
Chicago/Turabian StyleDemuth, Brielle, Ariane Pellan, Amélie Boutin, Emmanuel Bujold, and Louise Ghesquière. 2024. "Aspirin at 75 to 81 mg Daily for the Prevention of Preterm Pre-Eclampsia: Systematic Review and Meta-Analysis" Journal of Clinical Medicine 13, no. 4: 1022. https://doi.org/10.3390/jcm13041022
APA StyleDemuth, B., Pellan, A., Boutin, A., Bujold, E., & Ghesquière, L. (2024). Aspirin at 75 to 81 mg Daily for the Prevention of Preterm Pre-Eclampsia: Systematic Review and Meta-Analysis. Journal of Clinical Medicine, 13(4), 1022. https://doi.org/10.3390/jcm13041022