
Helicobacter pylori Eradication Therapy in Patients with Decreased Renal Function: A Systematic Review



Abstract
1. Introduction
2. Method
2.1. Protocol
2.2. Eligibility Criteria
2.3. Literature Search Strategy
2.4. Literature Search and Selection
2.5. Data Extraction
2.6. Quality Assessment of Included Papers
3. Results
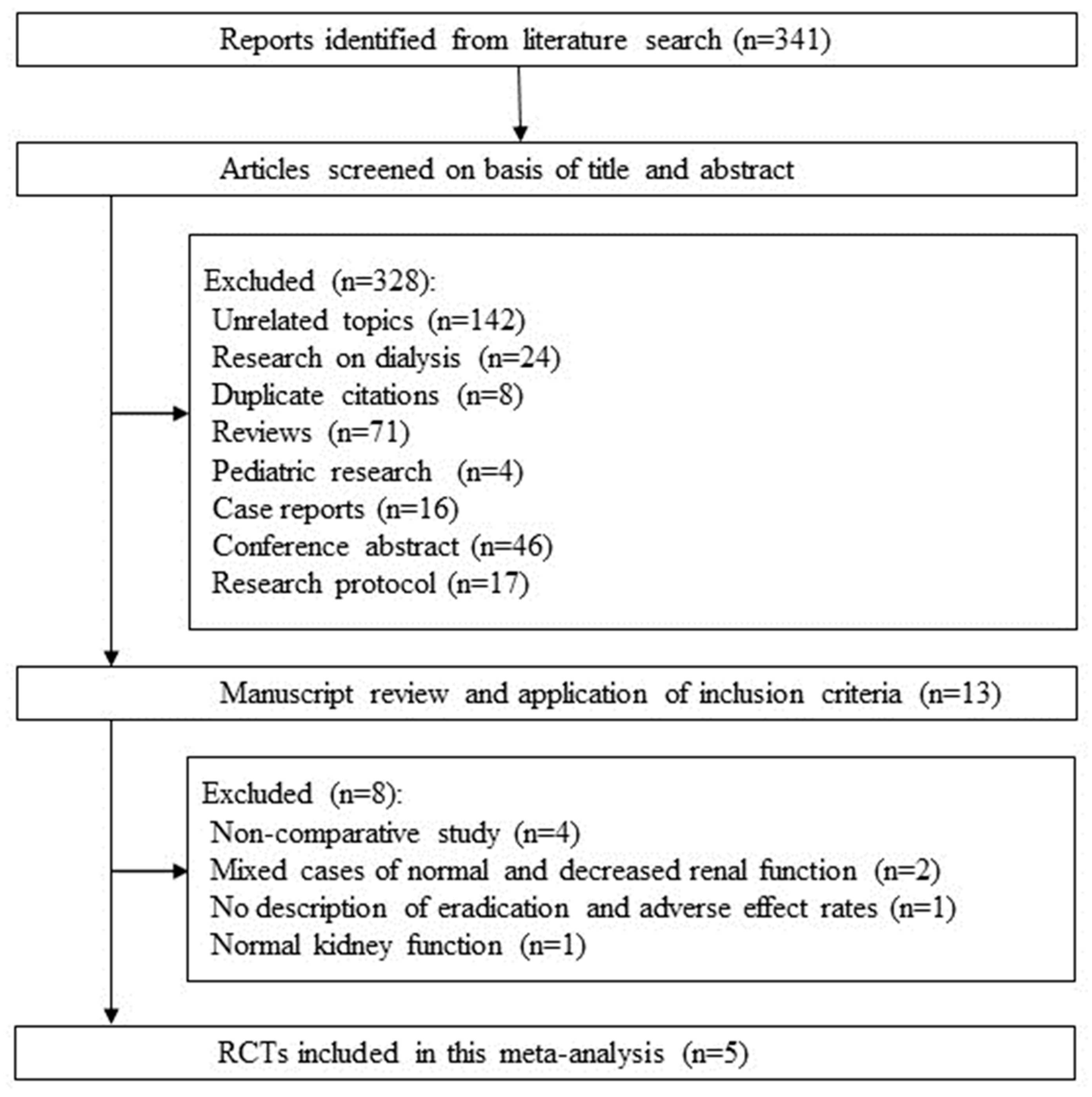
3.1. Literature Selection
3.2. Background and Methods in Included Studies
3.3. Quality Evaluation
3.4. RCTs Comparing the Standard Treatment with Other Treatments in Patients with Decreased Renal Function
3.5. Standard Eradication Treatment for Patients with and without Decreased Renal Function
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kato, M.; Ota, H.; Okuda, M.; Kikuchi, S.; Satoh, K.; Shimoyama, T.; Suzuki, H.; Handa, O.; Furuta, T.; Mabe, K.; et al. Guidelines for the management of Helicobacter pylori infection in Japan: 2016 Revised Edition. Helicobacter 2019, 24, e12597. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, H.; Franceschi, F.; Nishizawa, T.; Gasbarrini, A. Extragastric manifestations of Helicobacter pylori infection. Helicobacter 2011, 16 (Suppl. S1), 65–69. [Google Scholar] [CrossRef]
- Zagari, R.M.; Dajti, E.; Cominardi, A.; Frazzoni, L.; Fuccio, L.; Eusebi, L.H.; Vestito, A.; Lisotti, A.; Galloro, G.; Romano, M.; et al. Standard Bismuth Quadruple Therapy versus Concomitant Therapy for the First-Line Treatment of Helicobacter pylori Infection: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. J. Clin. Med. 2023, 12, 3258. [Google Scholar] [CrossRef] [PubMed]
- Sheu, B.S.; Huang, J.J.; Yang, H.B.; Huang, A.H.; Wu, J.J. The selection of triple therapy for Helicobacter pylori eradication in chronic renal insufficiency. Aliment. Pharmacol. Ther. 2003, 17, 1283–1290. [Google Scholar] [CrossRef] [PubMed]
- Seyyedmajidi, M.; Falaknazi, K.; Mirsattari, D.; Zojaji, H.; Roshani, M.; Lahmi, F.; Orimi, P.G.; Hadizadeh, M.; Zali, M. Correlation between creatinine clearance and Helicobacter pylori infection eradication with sequential and triple therapeutic regimens: A randomised clinical trial. Arab. J. Gastroenterol. 2011, 12, 150–153. [Google Scholar] [CrossRef] [PubMed]
- Alimadadi, M.; Seyyedmajidi, M.; Amirkhanlou, S.; Hafezi, A.A.; Homapour, S.; Vafaeimanesh, J.; Vakili, M.A. Impact of creatinine clearance on Helicobacter pylori eradication rate in patients with peptic ulcer disease. Iran. J. Kidney Dis. 2015, 9, 427–432. [Google Scholar]
- Liang, C.M.; Chiu, C.H.; Wang, H.M.; Tai, W.C.; Yao, C.C.; Tsai, C.E.; Kuo, C.M.; Chiu, Y.C.; Wu, K.L.; Lee, C.H.; et al. First-Line Helicobacter pylori Eradication in Patients with Chronic Kidney Diseases in Taiwan. Biomed. Res. Int. 2017, 2017, 3762194. [Google Scholar] [CrossRef]
- Mak, S.K.; Loo, C.K.; Wong, A.M.; Wong, P.N.; Lo, K.Y.; Tong, G.M.; Lam, E.K.; Wong, A.K. Efficacy of a 1-week course of proton-pump inhibitor-based triple therapy for eradicating Helicobacter pylori in patients with and without chronic renal failure. Am. J. Kidney Dis. 2002, 40, 576–581. [Google Scholar] [CrossRef]
- Sugimoto, M.; Yamaoka, Y. Review of Helicobacter pylori infection and chronic renal failure. Ther. Apher. Dial. 2011, 15, 1–9. [Google Scholar] [CrossRef]
- Nishizawa, T.; Munkjargal, M.; Ebinuma, H.; Toyoshima, O.; Suzuki, H. Sitafloxacin for Third-Line Helicobacter pylori Eradication: A Systematic Review. J. Clin. Med. 2021, 10, 2722. [Google Scholar] [CrossRef]
- Nishizawa, T.; Nishizawa, Y.; Yahagi, N.; Kanai, T.; Takahashi, M.; Suzuki, H. Effect of supplementation with rebamipide for Helicobacter pylori eradication therapy: A systematic review and meta-analysis. J. Gastroenterol. Hepatol. 2014, 29 (Suppl. S4), 20–24. [Google Scholar] [CrossRef]
- Stang, A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur. J. Epidemiol. 2010, 25, 603–605. [Google Scholar] [CrossRef] [PubMed]
- Singh, A.; Pogorelic, Z.; Agrawal, A.; Munoz, C.M.L.; Kainth, D.; Verma, A.; Jindal, B.; Agarwala, S.; Anand, S. Utility of Ischemia-Modified Albumin as a Biomarker for Acute Appendicitis: A Systematic Review and Meta-Analysis. J. Clin. Med. 2023, 12, 5486. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.; Altman, D.G.; Gotzsche, P.C.; Juni, P.; Moher, D.; Oxman, A.D.; Savovic, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.C.; Chen, S.J.; Huang, P.J.; Huang, H.T.; Cheng, Y.M.; Shih, C.L. Efficacy of Different Energy Levels Used in Focused and Radial Extracorporeal Shockwave Therapy in the Treatment of Plantar Fasciitis: A Meta-Analysis of Randomized Placebo-Controlled Trials. J. Clin. Med. 2019, 8, 1497. [Google Scholar] [CrossRef]
- Mak, S.K.; Loo, C.K.; Wong, P.N.; Lo, K.Y.; Tong, G.M.; Lam, E.K.; Wong, A.K. A retrospective study on efficacy of proton-pump inhibitor-based triple therapy for eradication of Helicobacter pylori in patients with chronic renal failure. Singap. Med. J. 2003, 44, 74–78. [Google Scholar]
- Ikuta, K.; Nakagawa, S.; Yamawaki, C.; Itohara, K.; Hira, D.; Imai, S.; Yonezawa, A.; Nakagawa, T.; Sakuragi, M.; Sato, N.; et al. Use of proton pump inhibitors and macrolide antibiotics and risk of acute kidney injury: A self-controlled case series study. BMC Nephrol. 2022, 23, 383. [Google Scholar] [CrossRef]
- Dede, F.; Ayli, D.; Gonul, I.; Yuksel, O.; Ozturk, R.; Yildiz, A.; Yenigun, E.; Piskinpasa, S.; Turgut, D.; Koc, E.; et al. The effect of Helicobacter pylori eradication on proteinuria in patients with primary glomerulonephritis. Arch. Med. Sci. 2015, 11, 764–769. [Google Scholar] [CrossRef]
- Aljahdli, E.; Almaghrabi, S.J.; Alhejaili, T.L.; Alghamdi, W. Association between Helicobacter pylori Eradication and Kidney Function in Patients with Chronic Gastritis: A Retrospective Single-Center Study. Cureus 2022, 14, e21621. [Google Scholar] [CrossRef]
- Simunic, M.; Ljutic, D.; Mise, S.; Pesutic-Pisac, V.; Tonkic, M.; Hozo, I. Helicobacter pylori eradication for the treatment of dyspeptic symptoms in chronic renal failure. Ann. Saudi Med. 2005, 25, 425–427. [Google Scholar] [CrossRef]
- Wang, J.W.; Hsu, C.N.; Tai, W.C.; Ku, M.K.; Hung, T.H.; Tseng, K.L.; Yuan, L.T.; Nguang, S.H.; Liang, C.M.; Yang, S.C.; et al. The Association of Helicobacter pylori Eradication with the Occurrences of Chronic Kidney Diseases in Patients with Peptic Ulcer Diseases. PLoS ONE 2016, 11, e0164824. [Google Scholar] [CrossRef]
- Hsu, C.H.; Hu, H.Y.; Huang, N.; Chang, S.S. Early eradication has a lower risk of peptic ulcer bleeding in Helicobacter pylori-infected chronic kidney disease patients. Eur. J. Intern. Med. 2016, 33, 112–117. [Google Scholar] [CrossRef]
- Sun, Y.; Yang, X.; Li, F.; Song, L.; Li, J. Effect of anti-helicobacter pylori treatment on early diabetic kidney disease. World Chin. J. Dig. 2015, 23, 1202–1207. [Google Scholar] [CrossRef]
- Murakami, K.; Sakurai, Y.; Shiino, M.; Funao, N.; Nishimura, A.; Asaka, M. Vonoprazan, a novel potassium-competitive acid blocker, as a component of first-line and second-line triple therapy for Helicobacter pylori eradication: A phase III, randomised, double-blind study. Gut 2016, 65, 1439–1446. [Google Scholar] [CrossRef]
- Sue, S.; Suzuki, Y.; Sasaki, T.; Kaneko, H.; Irie, K.; Komatsu, K.; Maeda, S. Prospective Study of Vonoprazan-Based First-Line Triple Therapy with Amoxicillin and Metronidazole for Clarithromycin-Resistant Helicobacter pylori. J. Clin. Med. 2023, 12, 5443. [Google Scholar] [CrossRef]
- Furuta, T.; Yamade, M.; Higuchi, T.; Takahashi, S.; Ishida, N.; Tani, S.; Tamura, S.; Iwaizumi, M.; Hamaya, Y.; Osawa, S.; et al. Expectations for the Dual Therapy with Vonoprazan and Amoxicillin for the Eradication of H. pylori. J. Clin. Med. 2023, 12, 3110. [Google Scholar] [CrossRef]
- Sue, S.; Suzuki, N.; Shibata, W.; Sasaki, T.; Yamada, H.; Kaneko, H.; Tamura, T.; Ishii, T.; Kondo, M.; Maeda, S. First-Line Helicobacter pylori Eradication with Vonoprazan, Clarithromycin, and Metronidazole in Patients Allergic to Penicillin. Gastroenterol. Res. Pract. 2017, 2017, 2019802. [Google Scholar] [CrossRef]
- Malfertheiner, P.; Megraud, F.; O’morain, C.A.; Gisbert, J.P.; Kuipers, E.J.; Axon, A.T.; Bazzoli, F.; Gasbarrini, A.; Atherton, J.; Graham, D.Y.; et al. Management of Helicobacter pylori infection-the Maastricht V/Florence Consensus Report. Gut 2017, 66, 6–30. [Google Scholar] [CrossRef] [PubMed]
- Ono, S.; Kato, M.; Nakagawa, S.; Mabe, K.; Sakamoto, N. Vonoprazan improves the efficacy of Helicobacter pylori eradication therapy with a regimen consisting of clarithromycin and metronidazole in patients allergic to penicillin. Helicobacter 2017, 22, e12374. [Google Scholar] [CrossRef] [PubMed]
- Adachi, K.; Kato, S.; Koshino, A.; Nagao, K.; Sugiyama, T.; Yoshimine, T.; Yamaguchi, Y.; Izawa, S.; Ohashi, W.; Ebi, M.; et al. A Vonoprazan, Clarithromycin, and Metronidazole Regimen as Helicobacter pylori Eradication Therapy for Patients with Penicillin Allergy in Light of Clarithromycin Resistance. Intern. Med. 2023, 62, 2301–2306. [Google Scholar] [CrossRef] [PubMed]
- Dosage Recommendations for Main Drugs in Renal Impairment, 37th Edition. Jpn. Soc. Nephrol. Pharmacother. 2014, pp. 27–33. Available online: http://jsnp.kenkyuukai.jp/images/sys/information/20140408235329-AE791D6696DA986E554DBFF97DD91687B61C00ACA99BDE895CF2B7B52237FF28.pdf (accessed on 28 February 2014).
- Aloy, B.; Launay-Vacher, V.; Bleibtreu, A.; Bortolotti, P.; Faure, E.; Filali, A.; Gauzit, R.; Gilbert, M.; Lesprit, P.; Mahieu, R.; et al. Antibiotics and chronic kidney disease: Dose adjustment update for infectious disease clinical practice. Med. Mal. Infect. 2020, 50, 323–331. [Google Scholar] [CrossRef]
- Malfertheiner, P.; Megraud, F.; Rokkas, T.; Gisbert, J.P.; Liou, J.M.; Schulz, C.; Gasbarrini, A.; Hunt, R.H.; Leja, M.; O’Morain, C.; et al. Management of Helicobacter pylori infection: The Maastricht VI/Florence consensus report. Gut 2022, 71, 1724–1762. [Google Scholar] [CrossRef]
- Zamani, M.; Alizadeh-Tabari, S.; Zamani, V.; Shokri-Shirvani, J.; Derakhshan, M.H. Worldwide and Regional Efficacy Estimates of First-line Helicobacter pylori Treatments: A Systematic Review and Network Meta-Analysis. J. Clin. Gastroenterol. 2022, 56, 114–124. [Google Scholar] [CrossRef]
- Pelepenko, L.E.; Janini, A.C.P.; Gomes, B.P.; de-Jesus-Soares, A.; Marciano, M.A. Effects of Bismuth Exposure on the Human Kidney—A Systematic Review. Antibiotics 2022, 11, 1741. [Google Scholar] [CrossRef]
- Pan, W.; Zhang, H.; Wang, L.; Zhu, T.; Chen, B.; Fan, J. Association between Helicobacter pylori infection and kidney damage in patients with peptic ulcer. Ren. Fail. 2019, 41, 1028–1034. [Google Scholar] [CrossRef]


{kind=link}
| First Author | Study Design | Subjects | Comparison Group | Control Group | Outcomes | NOS |
|---|---|---|---|---|---|---|
| Sheu [4] | Randomized controlled trial | H. pylori-infected cases with renal dysfunction | PPI + MNZ + CAM | PPI + AMPC + CAM | Eradication rate, renal impairment | - |
| Seyyedmajidi [5] | Randomized controlled trial | H. pylori-infected cases with renal dysfunction | PPI + AMPC + CPFX + furazolidone | PPI + AMPC + CAM | Eradication rate | - |
| Alimadadi [6] | Case-control study | H. pylori-infected cases | PPI + AMPC + CAM in cases with decreased renal function | PPI + AMPC + CAM in cases with normal renal function | Eradication rate | 7 |
| Liang [7] | Case-control study | H. pylori-infected cases | PPI + AMPC + CAM in cases with decreased renal function | PPI + AMPC + CAM in cases with normal renal function | Eradication rate, adverse event | 7 |
| Mak [8] | Case-control study | H. pylori-infected cases | PPI + AMPC + CAM in cases with decreased renal function | PPI + AMPC + CAM in cases with normal renal function | Eradication rate, renal impairment | 6 |
| First Author | Random Sequence Generation | Allocation Concealment | Blinding of Participants and Personnel | Blinding of Outcome Assessment | Adequate Assessment of Incomplete Outcome | Selective Reporting Avoided | No Other Bias |
|---|---|---|---|---|---|---|---|
| Sheu [4] | Unclear | Unclear | High risk | Low risk | Low risk | Low risk | Low risk |
| Seyyedmajidi [5] | Unclear | Unclear | High risk | Low risk | Low risk | Low risk | Low risk |
| First Author | Subjects | Treatments | Duration | Eradication Rate (PP) | Renal Impairment |
|---|---|---|---|---|---|
| Sheu [4] | Serum Cr > 1.5 mg/dL Non-dialysis | LPZ(30 mg) + MNZ(500 mg) + CAM(500 mg) bid | 7 days | 92.5% (37/40) | 2% (1/44) |
| LPZ(30 mg) + AMPC(750 mg) + CAM(500 mg) bid | 7 days | 76.3% (29/38) * | 18% (8/44) * | ||
| Seyyedmajidi [5] | CCr < 60 mg/min Non-dialysis | Sequential therapy: OPZ (20 mg) + AMPC (1000 mg) + CPFX (500 mg: first half) + furazolidone (200 mg: second half) bid | 14 days | 83.7% (31/37) | - |
| OPZ(20 mg) + AMPC(1000 mg) + CAM(500 mg) bid | 14 days | 77.8% (28/36) | - |
| First Author | Duration | Treatment Groups | Antibiotic Dose Adjustment | Eradication Rate (PP) | Adverse Events |
|---|---|---|---|---|---|
| Alimadadi [6] | 14 days | Decreased renal function | Half dose for CCr ≦ 30 mL/min | 81.2% (43/53) | - |
| Normal renal function | None | 83.0% (44/53) | - | ||
| Liang [7] | 7 days | Decreased renal function | Half dose for end-stage renal disease | 85.1% (97/114) | 3.1% (4/130) # |
| Normal renal function | None | 85.7% (538/628) | 4.6% (29/628) | ||
| Mak [8] | 7 days | Decreased renal function | None | 90.5% (19/21) ## | CCr did not change before and after eradication |
| Normal renal function | None | 85.7% (18/21) | - | ||
| Seyyedmajidi [5] | 14 days | Decreased renal function | Half dose for end-stage renal disease | 77.8% (28/36) | - |
| Normal renal function | None | 76.0% (19/25) | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nishizawa, T.; Sano, M.; Toyoshima, O.; Suzuki, H. Helicobacter pylori Eradication Therapy in Patients with Decreased Renal Function: A Systematic Review. J. Clin. Med. 2024, 13, 850. https://doi.org/10.3390/jcm13030850
Nishizawa T, Sano M, Toyoshima O, Suzuki H. Helicobacter pylori Eradication Therapy in Patients with Decreased Renal Function: A Systematic Review. Journal of Clinical Medicine. 2024; 13(3):850. https://doi.org/10.3390/jcm13030850
Chicago/Turabian StyleNishizawa, Toshihiro, Masaya Sano, Osamu Toyoshima, and Hidekazu Suzuki. 2024. "Helicobacter pylori Eradication Therapy in Patients with Decreased Renal Function: A Systematic Review" Journal of Clinical Medicine 13, no. 3: 850. https://doi.org/10.3390/jcm13030850
APA StyleNishizawa, T., Sano, M., Toyoshima, O., & Suzuki, H. (2024). Helicobacter pylori Eradication Therapy in Patients with Decreased Renal Function: A Systematic Review. Journal of Clinical Medicine, 13(3), 850. https://doi.org/10.3390/jcm13030850