The Association of High-Molecular-Weight Hyaluronic Acid (HMWHA), Alpha Lipoic Acid (ALA), Magnesium, Vitamin B6, and Vitamin D Improves Subchorionic Hematoma Resorption in Women with Threatened Miscarriage: A Pilot Clinical Study



Abstract
1. Introduction
2. Materials and Methods
2.1. Sonographic Visualization of a Subchorionic Hematoma
2.2. Primary and Secondary Outcomes
3. Statistical Analysis
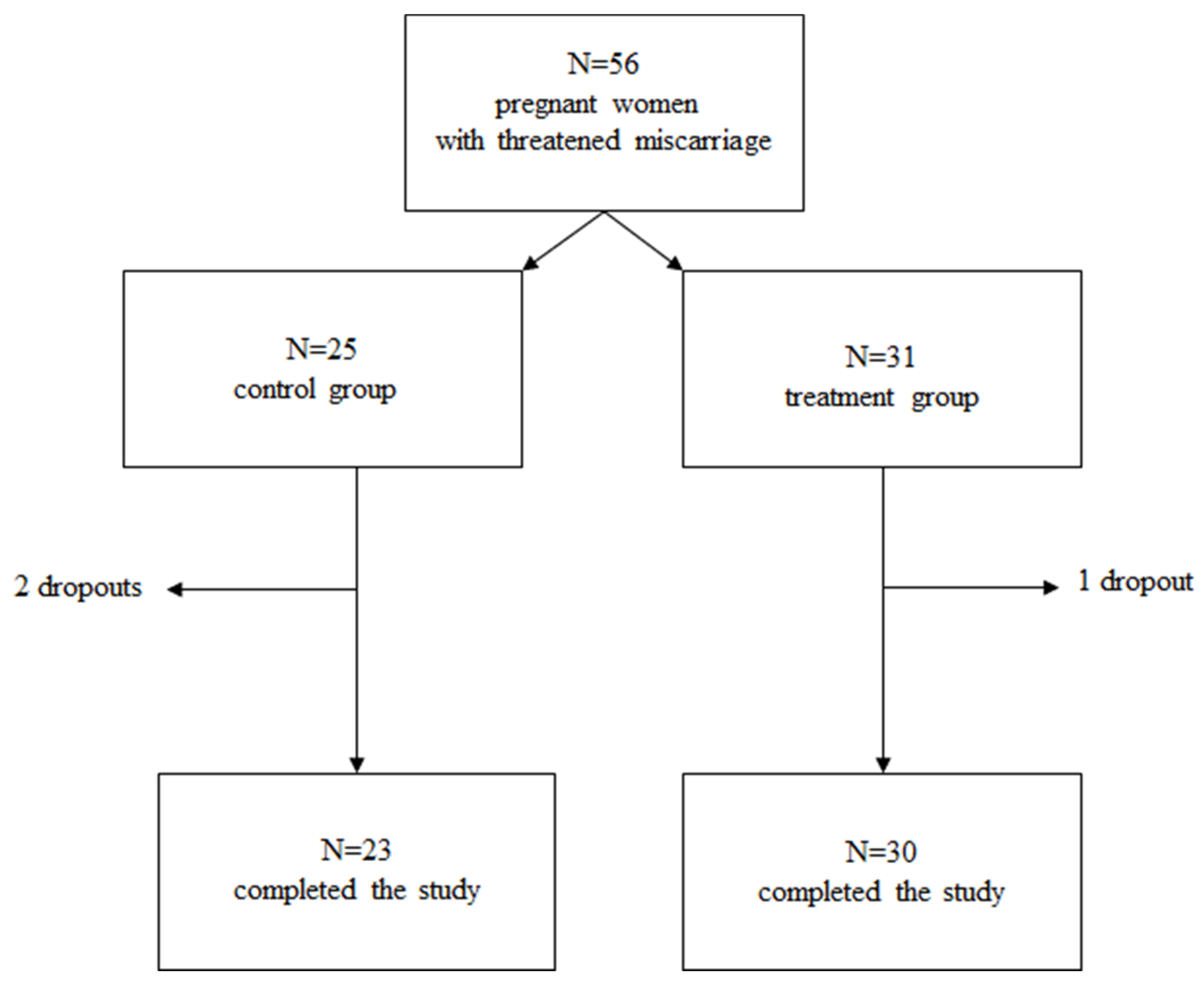
4. Results
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mouri, M.; Hall, H.; Rupp, T.J. Threatened Abortion; StatPearls: Treasure Island, FL, USA, 2022. [Google Scholar]
- Nagy, S.; Bush, M.; Stone, J.; Lapinski, R.H.; Gardó, S. Clinical significance of subchorionic and retroplacental hematomas detected in the first trimester of pregnancy. Obstet. Gynecol. 2003, 102, 94–100. [Google Scholar] [CrossRef]
- Ali, H.Z.; Ismail, S.K. First Trimester Subchorionic Hematoma and Outcome of Pregnancy. Sch. Int. J. Obstet. Gynec. 2021, 4, 297–303. [Google Scholar]
- Pearlstone, M.; Baxi, L. Subchorionic hematoma: A review. Obstet. Gynecol. Surv. 1993, 48, 65–68. [Google Scholar]
- Leite, J.; Ross, P.; Rossi, A.; Jeanty, P. Prognosis of very large first-trimester hematomas. J. Ultrasound Med. 2006, 25, 141–1445. [Google Scholar] [CrossRef] [PubMed]
- Bennett, G.L.; Bromley, B.; Lieberman, E.; Benacerraf, B.R. Subchorionic hemorrhage in first-trimester pregnancies: Prediction of pregnancy outcome with sonography. Radiology 1996, 200, 803–806. [Google Scholar] [CrossRef] [PubMed]
- Parente, E.; Colannino, G.; Picconi, O.; Monastra, G. Safety of oral alpha-lipoic acid treatment in pregnant women: A retrospective observational study. Eur. Rev. Med. Pharmacol. Sci. 2017, 21, 4219–4227. [Google Scholar] [PubMed]
- Palacios, C.; Kostiuk, L.; Peña-Rosas, J.P. Vitamin D supplementation for women during pregnancy. Cochrane Database Syst. Rev. 2019, 7, CD008873. [Google Scholar] [CrossRef] [PubMed]
- Fanni, D.; Gerosa, C.; Nurchi, V.M.; Manchia, M.; Saba, L.; Coghe, F.; Crisponi, G.; Gibo, Y.; Van Eyken, P.; Fanos, V.; et al. The Role of Magnesium in Pregnancy and in Fetal Programming of Adult Diseases. Biol. Trace Elem. Res. 2021, 199, 3647–3657. [Google Scholar] [CrossRef] [PubMed]
- Costantino, M.; Guaraldi, C.; Costantino, D. Resolution of subchorionic hematoma and symptoms of threatened miscarriage using vaginal alpha lipoic acid or progesterone: Clinical evidences. Eur. Rev. Med. Pharmacol. Sci. 2016, 20, 1656–1663. [Google Scholar] [PubMed]
- Porcaro, G.; Brillo, E.; Giardina, I.; Di Iorio, R. Alpha Lipoic Acid (ALA) effects on subchorionic hematoma: Preliminary clinical results. Eur. Rev. Med. Pharmacol. Sci. 2015, 19, 3426–3432. [Google Scholar] [PubMed]
- Weissmann, B.; Meyer, K.; Sampson, P.; Linker, A. Isolation of oligosaccharides enzymatically produced from hyaluronic acid. J. Biol. Chem. 1954, 208, 417–429. [Google Scholar] [CrossRef]
- Kobayashi, T.; Chanmee, T.; Itano, N. Hyaluronan: Metabolism and Function. Biomolecules 2020, 10, 1525. [Google Scholar] [CrossRef]
- Atkins, E.D.; Sheehan, J.K. Structure for hyaluronic acid. Nat. New Biol. 1972, 235, 253–254. [Google Scholar] [CrossRef]
- Petrey, A.C.; de la Motte, C.A. Hyaluronan, a crucial regulator of inflammation. Front. Immunol. 2014, 5, 101. [Google Scholar] [CrossRef]
- Day, A.J.; de la Motte, C.A. Hyaluronan cross-linking: A protective mechanism in inflammation? Trends Immunol. 2005, 26, 637–643. [Google Scholar] [CrossRef]
- Casale, M.; Moffa, A.; Vella, P.; Sabatino, L.; Capuano, F.; Salvinelli, B.; Lopez, M.A.; Carinci, F.; Salvinelli, F. Hyaluronic acid: Perspectives in dentistry. A systematic review. Int. J. Immunopathol. Pharmacol. 2016, 29, 572–582. [Google Scholar] [CrossRef]
- Fouladi-Nashta, A.A.; Raheem, K.A.; Marei, W.F.; Ghafari, F.; Hartshorne, G.M. Regulation and roles of the hyaluronan system in mammalian reproduction. Reproduction 2017, 153, R43–R58. [Google Scholar] [CrossRef] [PubMed]
- Teklenburg, G.; Salker, M.; Molokhia, M.; Lavery, S.; Trew, G.; Aojanepong, T.; Mardon, H.J.; Lokugamage, A.U.; Rai, R.; Landles, C.; et al. Natural selection of human embryos: Decidualizing endometrial stromal cells serve as sensors of embryo quality upon implantation. PLoS ONE 2010, 5, e10258. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Wang, E.; Huang, S.; Zhu, C.; Zhang, K.; Zhang, J.; Xu, H.; Shu, J. Autoantibodies in association with subchorionic haematoma in early pregnancy. Ann. Med. 2021, 53, 841–847. [Google Scholar] [CrossRef] [PubMed]
- Zhu, R.; Huang, Y.H.; Tao, Y.; Wang, S.C.; Sun Ch Piao, H.L.; Wang, X.Q.; Du, M.R.; Li, D.J. Hyaluronan up-regulates growth and invasion of trophoblasts in an autocrine manner via PI3K/AKT and MAPK/ERK1/2 pathways in early human pregnancy. Placenta 2013, 34, 784–791. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.; Sun, F.; Han, M.; Liu, Y.; Zou, Q.; Wang, F.; Tao, Y.; Li, D.; Du, M.; Li, H.; et al. Trophoblast-derived hyaluronan promotes the regulatory phenotype of decidual macrophages. Reproduction 2019, 157, 189–198. [Google Scholar] [CrossRef]
- Bollyky, P.L.; Wu, R.P.; Falk, B.A.; Lord, J.D.; Long, S.A.; Preisinger, A.; Teng, B.; Holt, G.E.; Standifer, N.E.; Braun, K.R.; et al. ECM components guide IL-10 producing regulatory T-cell (TR1) induction from effector memory T-cell precursors. Proc. Natl. Acad. Sci. USA 2011, 108, 7938–7943. [Google Scholar] [CrossRef]
- Nakamura, K.; Yokohama, S.; Yoneda, M.; Okamoto, S.; Tamaki, Y.; Ito, T.; Okada, M.; Aso, K.; Makino, I. High, but not low, molecular weight hyaluronan prevents T-cell-mediated liver injury by reducing proinflammatory cytokines in mice. J. Gastroenterol. 2004, 39, 346–354. [Google Scholar] [CrossRef]
- Hakeem, L.A.; Bello, Y.O.; Obajimi, G.O.; Onifade, A.F.A.; Ahmed, B.; Arowojolu, A.O.; Morhason-Bello, I.O. Inflammatory cytokines in maternal serum between women with threatened miscarriage and normal pregnancy. Int. J. Gynaecol. Obstet. 2024, 164, 255–261. [Google Scholar] [CrossRef]
- Shay, K.P.; Moreau, R.; Smith, E.; Smith, A.R.; Hagen, T.M. Alpha-lipoic acid as a dietary supplement: Molecular mechanisms and therapeutic potential. Biochim. Biophys. Acta 2009, 1790, 1149–1160. [Google Scholar] [CrossRef]
- Goraca, A.; Huk-Kolega, H.; Piechota, A.; Kleniewska, P.; Ciejka, E.; Skibska, B. Lipoic acid-biological activity, and therapeutic potential. Pharmacol. Rep. 2011, 63, 849–858. [Google Scholar] [CrossRef] [PubMed]
- Monastra, G.; De Grazia, S.; De Luca, L.; Vittorio, S.; Unfer, V. Vitamin D: A steroid hormone with progesterone-like activity. Eur. Rev. Med. Pharmacol. Sci. 2018, 22, 2502–2512. [Google Scholar] [CrossRef]
- Vernon, W.B. The role of magnesium in nucleic-acid and protein metabolism. Magnesium 1988, 7, 234–248. [Google Scholar] [PubMed]
- Falsaperla, R.; Saporito, M.; Di Stefano, V.; Mauceri, L.; Quattrocchi, E.; Musolino, A.; Corsello, G. Pyridoxine supplementation during pregnancy, lactation and the first months of life: A review of the literature. Curr. Pediatr. Res. 2017, 21, 613–619. [Google Scholar]
- Unfer, V.; Tilotta, M.; Kaya, C.; Noventa, M.; Török, P.; Alkatout, I.; Gitas, G.; Bilotta, G.; Laganà, A.S. Absorption, distribution, metabolism, and excretion of hyaluronic acid during pregnancy: A matter of molecular weight. Expert Opin. Drug Metab. Toxicol. 2021, 17, 823–840. [Google Scholar] [CrossRef] [PubMed]
- Balogh, L.; Polyak, A.; Mathe, D.; Kiraly, R.; Thuroczy, J.; Terez, M.; Janoki, G.; Ting, Y.; Bucci, L.R.; Schauss, A.G. Absorption, uptake and tissue affinity of high-molecular-weight hyaluronan after oral administration in rats and dogs. J. Agric. Food Chem. 2008, 56, 10582–10593. [Google Scholar] [CrossRef]
- Kawada, C.; Yoshida, T.; Yoshida, H.; Matsuoka, R.; Sakamoto, W.; Odanaka, W.; Sato, T.; Yamasaki, T.; Kanemitsu, T.; Masuda, Y.; et al. Ingested hyaluronan moisturizes dry skin. Nutr. J. 2014, 13, 70. [Google Scholar] [CrossRef]
- Sato, Y.; Joumura, T.; Takekuma, Y.; Sugawara, M. Transfer of orally administered hyaluronan to the lymph. Eur. J. Pharm. Biopharm. 2020, 154, 210–213. [Google Scholar] [CrossRef]
- De Souza, A.B.; Chaud, M.; Santana, M.H.A. Hyaluronic acid behavior in oral administration and perspectives for nanotechnology-based formulations: A review. Carbohydr. Polym. 2019, 15, 115001. [Google Scholar] [CrossRef]
- Hansen, I.M.; Ebbesen, M.F.; Kaspersen, L.; Thomsen, T.; Bienk, K.; Cai, Y.; Malle, B.M.; Howard, K.A. Hyaluronic Acid Molecular Weight-Dependent Modulation of Mucin Nanostructure for Potential Mucosal Therapeutic Applications. Mol. Pharm. 2017, 14, 2359–2367. [Google Scholar] [CrossRef]
- Koropatkin, N.M.; Cameron, E.A.; Martens, E.C. How glycan metabolism shapes the human gut microbiota. Nat. Rev. Microbiol. 2012, 10, 323–335. [Google Scholar] [CrossRef]
- Abreu, M.T. Toll-like receptor signalling in the intestinal epithelium: How bacterial recognition shapes intestinal function. Nat. Rev. Immunol. 2010, 10, 131–144. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.; de la Motte, C.A. The Role of Hyaluronan Treatment in Intestinal Innate Host Defense. Front. Immunol. 2020, 11, 569. [Google Scholar] [CrossRef]
- Parente, E.; Colannino, G.; Bilotta, G.; Espinola, M.S.B.; Proietti, S.; Oliva, M.M.; Neri, I.; Aragona, C.; Unfer, V. Effect of Oral High Molecular Weight Hyaluronic Acid (HMWHA), Alpha Lipoic Acid (ALA), Magnesium, Vitamin B6 and Vitamin D Supplementation in Pregnant Women: A Retrospective Observational Pilot Study. Clin. Pract. 2023, 13, 1123–1129. [Google Scholar] [CrossRef] [PubMed]
- Mahendroo, M. Cervical hyaluronan biology in pregnancy, parturition and preterm birth. Matrix Biol. 2019, 78–79, 24–31. [Google Scholar] [CrossRef] [PubMed]
- Akgul, Y.; Word, R.A.; Ensign, L.M.; Yamaguchi, Y.; Lydon, J.; Hanes, J.; Mahendroo, M. Hyaluronan in cervical epithelia protects against infection-mediated preterm birth. J. Clin. Investig. 2014, 124, 5481–5489. [Google Scholar] [CrossRef] [PubMed]
- Zhao, G.; Zhou, X.; Fang, T.; Hou, Y.; Hu, Y. Hyaluronic acid promotes the expression of progesterone receptor membrane component 1 via epigenetic silencing of miR-139-5p in human and rat granulosa cells. Biol. Reprod. 2014, 91, 116. [Google Scholar] [CrossRef] [PubMed]
- Wu, W.; Shi, S.; Huang, H.J.; Balducci, J.; Garfield, R.E. Changes in PGRMC1, a potential progesterone receptor, in human myometrium during pregnancy and labour at term and preterm. Mol. Hum. Reprod. 2011, 17, 233–242. [Google Scholar] [CrossRef] [PubMed]
- Feng, L.; Antczak, B.; Lan, L.; Grotegut, C.A.; Thompson, J.L.; Allen, T.K.; Murtha, A.P. Progesterone receptor membrane component 1 (PGRMC1) expression in fetal membranes among women with preterm premature rupture of the membranes (PPROM). Placenta 2014, 35, 331–333. [Google Scholar] [CrossRef]
- Feng, L.; Allen, T.; Marinello, W.P.; Murtha, A.P. Roles of Progesterone Receptor Membrane Component 1 in Oxidative Stress-Induced Aging in Chorion Cells. Reprod. Sci. 2019, 26, 394–403. [Google Scholar] [CrossRef]
- Lyzikova, Y.A.; Zinovkin, D.; Pranjol, M.Z.I. Increase in FoxP3, CD56 immune cells and decrease in glands PGRMC1 expression in the endometrium are associated with recurrent miscarriages. Eur. J. Obstet. Gynecol. Reprod. Biol. 2020, 245, 121–126. [Google Scholar] [CrossRef]
- Choi, S.R.; Choi, H.; Jo, E.; Choi, H.Y.; Jung, S.; Jang, S.; Choi, S.J.; Hwang, S.O. Decreased expression of progesterone receptor membrane component 1 in fetal membranes with chorioamnionitis among women with preterm birth. Arch. Gynecol. Obstet. 2020, 301, 949–954. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
| Control Group (n = 25) | Treatment Group (n = 31) | p Value | |
|---|---|---|---|
| Age (years) | 32.0 ± 2.5 | 32.6 ± 3.8 | 0.46 |
| Weight (kg) | 61.2 ± 6.8 | 61.2 ± 7.3 | 0.99 |
| Gestational age (weeks) | 8.3 ± 1.0 | 8.6 ± 0.9 | 0.41 |
| Parity | 11 (44%) | 16 (52%) | 0.60 |
| Previous cesarean section | 3 (12%) | 4 (13%) | 1.00 |
| Previous miscarriage | 8 (32%) | 9 (29%) | 1.00 |
| Symptoms | T0 | T1 | T2 | |||
|---|---|---|---|---|---|---|
| Ctrl Group n (%) | Treat. Group n (%) | Ctrl Group n (%) | Treat. Group n (%) | Ctrl Group n (%) | Treat. Group n (%) | |
| Vag. bleed. | 15 (65%) | 14 (47%) | 10 (43%) # | 1(3%) *** ### | 2 (8.7%) ### | 0 |
| Abd. pain | 23 (100%) | 30 (100%) | 14 (61%) ## | 9 (30%) * ### | 7 (30%) ### | 1 (3%) ** ### |
| Uter. Contr. | 23 (100%) | 30 (100%) | 21 (91%) | 12 (40%) *** ### | 12 (52%) ### | 0 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Porcaro, G.; Laganà, A.S.; Neri, I.; Aragona, C. The Association of High-Molecular-Weight Hyaluronic Acid (HMWHA), Alpha Lipoic Acid (ALA), Magnesium, Vitamin B6, and Vitamin D Improves Subchorionic Hematoma Resorption in Women with Threatened Miscarriage: A Pilot Clinical Study. J. Clin. Med. 2024, 13, 706. https://doi.org/10.3390/jcm13030706
Porcaro G, Laganà AS, Neri I, Aragona C. The Association of High-Molecular-Weight Hyaluronic Acid (HMWHA), Alpha Lipoic Acid (ALA), Magnesium, Vitamin B6, and Vitamin D Improves Subchorionic Hematoma Resorption in Women with Threatened Miscarriage: A Pilot Clinical Study. Journal of Clinical Medicine. 2024; 13(3):706. https://doi.org/10.3390/jcm13030706
Chicago/Turabian StylePorcaro, Giuseppina, Antonio Simone Laganà, Isabella Neri, and Cesare Aragona. 2024. "The Association of High-Molecular-Weight Hyaluronic Acid (HMWHA), Alpha Lipoic Acid (ALA), Magnesium, Vitamin B6, and Vitamin D Improves Subchorionic Hematoma Resorption in Women with Threatened Miscarriage: A Pilot Clinical Study" Journal of Clinical Medicine 13, no. 3: 706. https://doi.org/10.3390/jcm13030706
APA StylePorcaro, G., Laganà, A. S., Neri, I., & Aragona, C. (2024). The Association of High-Molecular-Weight Hyaluronic Acid (HMWHA), Alpha Lipoic Acid (ALA), Magnesium, Vitamin B6, and Vitamin D Improves Subchorionic Hematoma Resorption in Women with Threatened Miscarriage: A Pilot Clinical Study. Journal of Clinical Medicine, 13(3), 706. https://doi.org/10.3390/jcm13030706