
Remimazolam Versus Propofol in General Anesthesia of Complex Surgery in Critical and Non-Critical Patients: Meta-Analysis of Randomized Trials

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Searches
2.3. Eligibility Criteria
2.4. Outcomes
2.5. Data Extraction
2.6. Risk of Bias Assessment
2.7. Data Synthesis
3. Results
3.1. Selection of Studies
3.2. Characteristics of Included Studies
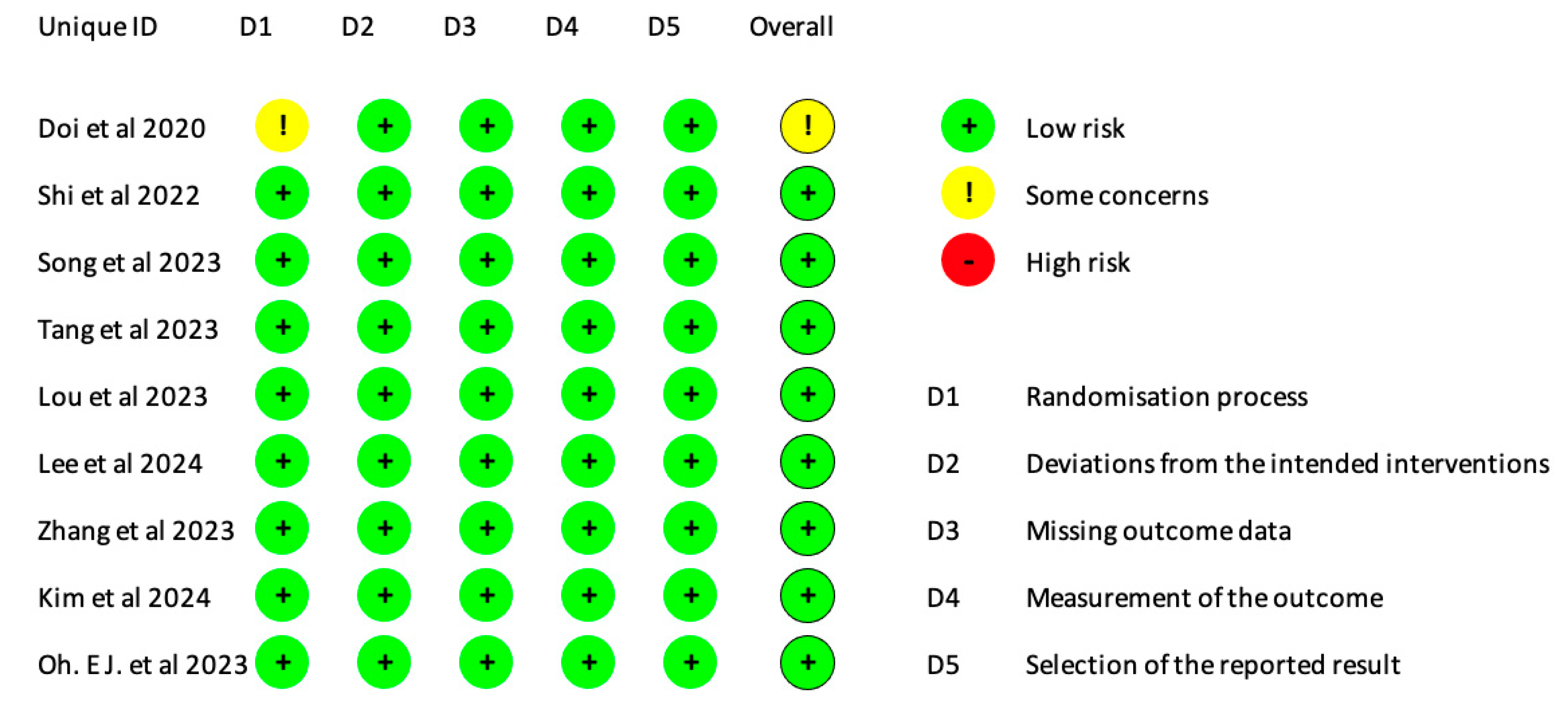
3.3. Risk of Bias Assessment
3.4. Effect of Remimazolam Versus Propofol in the Primary and Secondary Outcomes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lee, M.; Lee, C.; Choi, G.J.; Kang, H. Remimazolam for Procedural Sedation in Older Patients: A Systematic Review and Meta-Analysis with Trial Sequential Analysis. J. Pers. Med. 2024, 14, 276. [Google Scholar] [CrossRef] [PubMed]
- Tang, L.; Sun, Y.; Hao, X.; Sun, X.; Xie, C.; Wang, T.; Hu, C.; Lu, Y.; Liu, X. Effect of general anaesthesia with remimazolam versus propofol on postoperative quality of recovery in patients undergoing ambulatory arthroscopic meniscus repair: A randomised clinical trial. BJA Open 2023, 8, 100237. [Google Scholar] [CrossRef] [PubMed]
- Shimizu, T.; Takasusuki, T.; Yamaguchi, S. Remimazolam Compared to Propofol for Total Intravenous Anesthesia with Remifentanil on the Recovery of Psychomotor Function: A Randomized Controlled Trial. Adv. Ther. 2023, 40, 4395–4404. [Google Scholar] [CrossRef]
- Song, S.W.; Kim, S.; Park, J.-H.; Cho, Y.H.; Jeon, Y.-G. Post-induction hypotension with remimazolam versus propofol in patients routinely administered angiotensin axis blockades: A randomized control trial. BMC Anesthesiol. 2023, 23, 219. [Google Scholar] [CrossRef] [PubMed]
- Kitaura, A.; Tsukimoto, S.; Sakamoto, H.; Hamasaki, S.; Nakao, S.; Nakajima, Y. A retrospective comparative study of anesthesia with remimazolam and remifentanil versus dexmedetomidine and remifentanil for transcatheter aortic valve replacement. Sci. Rep. 2023, 13, 17074. [Google Scholar] [CrossRef] [PubMed]
- Curtin, F. Meta-analysis combining parallel and cross-over trials with random effects. Res. Synth. Methods 2017, 8, 263–274. [Google Scholar] [CrossRef]
- Langan, D.; Higgins, J.P.; Jackson, D.; Bowden, J.; Veroniki, A.A.; Kontopantelis, E.; Viechtbauer, W.; Simmonds, M. A comparison of heterogeneity variance estimators in simulated random-effects meta-analyses. Res. Synth. Methods 2019, 10, 83–98. [Google Scholar] [CrossRef]
- Zhang, Y.; Akl, E.A.; Schünemann, H.J. Using systematic reviews in guideline development: The GRADE approach. Res. Synth. Methods 2019, 10, 312–329. [Google Scholar] [CrossRef]
- Doi, M.; Morita, K.; Takeda, J.; Sakamoto, A.; Yamakage, M.; Suzuki, T. Efficacy and safety of remimazolam versus propofol for general anesthesia: A multicenter, single-blind, randomized, parallel-group, phase IIb/III trial. J. Anesthesia 2020, 34, 543–553. [Google Scholar] [CrossRef]
- Shi, F.; Chen, Y.; Li, H.; Zhang, Y.; Zhao, T. Efficacy and Safety of Remimazolam Tosilate versus Propofol for General Anesthesia in Cirrhotic Patients Undergoing Endoscopic Variceal Ligation. Int. J. Gen. Med. 2022, 15, 583–591. [Google Scholar] [CrossRef]
- Luo, W.; Sun, M.; Wan, J.; Zhang, Z.; Huang, J.; Zhang, J.; Xiong, W.; Xia, L.; Xu, P.; Miao, C.; et al. Efficacy and safety of remimazolam tosilate versus propofol in patients undergoing day surgery: A prospective randomized controlled trial. BMC Anesthesiol. 2023, 23, 182. [Google Scholar] [CrossRef] [PubMed]
- Oh, E.J.; Chung, Y.J.; Lee, J.-H.; Kwon, E.J.; Choi, E.A.; On, Y.K.; Min, J.-J. Comparison of propofol vs. remimazolam on emergence profiles after general anesthesia: A randomized clinical trial. J. Clin. Anesthesia 2023, 90, 111223. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.-J.; Kim, J.-Y.; Park, H.-S.; Kim, H.; Ro, Y.-J.; Koh, W.U. Effect of Remimazolam- versus Propofol-Based Total Intravenous General Anesthesia on Intraoperative Hemodynamic Stability for Major Spine Surgery in the Prone Position: A Randomized Controlled Trial. Medicina 2024, 60, 432. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Zhang, J.; Wang, Y.; Bai, X.; Guo, Q.; Liu, W.; Li, H.; Zhu, F.; Wang, X.; Jiang, X.; et al. Effect of remimazolam vs propofol on emergence from general anesthesia in patients undergoing cerebral endovascular procedures: A randomized controlled, non-inferiority trial. J. Clin. Anesthesia 2024, 93, 111356. [Google Scholar] [CrossRef]
- Lee, J.; Han, D.W.; Song, Y.; Lee, J.; Jeon, S.; Kim, M.H. Quality of Postoperative Recovery in Total Intravenous Anesthesia between Remimazolam and Propofol for Intraoperative Neurophysiological Monitoring: A Prospective Double-Blind Randomized Controlled Trial. J. Pers. Med. 2024, 14, 382. [Google Scholar] [CrossRef]
- Yang, J.-J.; Lei, L.; Qiu, D.; Chen, S.; Xing, L.-K.; Zhao, J.-W.; Mao, Y.-Y.; Yang, J.-J. Effect of Remimazolam on Postoperative Delirium in Older Adult Patients Undergoing Orthopedic Surgery: A Prospective Randomized Controlled Clinical Trial. Drug Des. Dev. Ther. 2023, 17, 143–153. [Google Scholar] [CrossRef]
- Wang, L.; Wang, Y.; Ma, L.; Wang, Y.; Mu, X.; Huang, Z.; Zheng, Z.; Nie, H. Cardiopulmonary Adverse Events of Remimazolam versus Propofol During Cervical Conization: A Randomized Controlled Trial. Drug Des. Dev. Ther. 2023, 17, 1233–1243. [Google Scholar] [CrossRef]
- Sneyd, J.R.; Absalom, A.R.; Barends, C.R.; Jones, J.B. Hypotension during propofol sedation for colonoscopy: A retrospective exploratory analysis and meta-analysis. Br. J. Anaesth. 2022, 128, 610–622. [Google Scholar] [CrossRef]
- Zhu, H.; Su, Z.; Zhou, H.; Lu, J.; Wang, X.; Ji, Z.; Chen, S.; Wang, X.; Yao, M.; Lu, Y.; et al. Remimazolam Dosing for Gastroscopy: A Randomized Noninferiority Trial. Anesthesiology 2024, 140, 409–416. [Google Scholar] [CrossRef]
- Zhang, S.; Wang, J.; Ran, R.; Peng, Y.; Xiao, Y. Efficacy and safety of remimazolam tosylate in hysteroscopy: A randomized, single-blind, parallel controlled trial. J. Clin. Pharm. Ther. 2022, 47, 55–60. [Google Scholar] [CrossRef]
- Zhang, X.; Li, S.; Liu, J. Efficacy and safety of remimazolam besylate versus propofol during hysteroscopy: Single-centre randomized controlled trial. BMC Anesthesiol. 2021, 21, 156. [Google Scholar] [CrossRef]
- Li, Z.; Yuan, D.; Yu, Y.; Xu, J.; Yang, W.; Chen, L.; Luo, N. Effect of remimazolam vs propofol in high-risk patients undergoing upper gastrointestinal endoscopy: A non-inferiority randomized controlled trial. Trials 2024, 25, 92. [Google Scholar] [CrossRef] [PubMed]
- Yang, L.; Zhang, J.; Xiao, N.; Chen, J.; Liu, H.; He, X.; Xiao, X.; Zhang, F. Clinical Trial Comparing Remimazolam with Propofol During Intravenous Anesthesia: A Prospective Randomised Clinical Trial. Comb. Chem. High Throughput Screen. 2024, 27, 1544–1550. [Google Scholar] [CrossRef] [PubMed]
- Huang, X.; Cao, H.; Zhang, C.; Lan, H.; Gong, X.; Li, R.; Lin, Y.; Xu, B.; Chen, H.; Guan, X. The difference in mean arterial pressure induced by remimazolam compared to etomidate in the presence of fentanyl at tracheal intubation: A randomized controlled trial. Front. Pharmacol. 2023, 14, 1143784. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author, Year | Country | Type and Phase | NCT (Coding del Art) | N° Patients per Arm | Eligibility Criteria | Age (Mean, SD) | Weight (Mean, SD) |
|---|---|---|---|---|---|---|---|
| Doi, M. et al., 2020 [9] | Japan | Multicenter, single-blind, randomized, parallel- group, phase IIb/III trial | JapicCTI number: 121973 | R1: 150 | ≥20 years old body weight of 100 kg or less scheduled for elective surgery ASA I–II. Exclusion Criteria: Emergency surgeries, extracorporeal circulation, spinal/epidural anesthesia, hepatectomy, liver transplant, uncontrolled hypertension, renal (creatinine ≥ 2 mg/dL) or hepatic (AST/ALT ≥ 2.5 × ULN) impairment. | R1: 57.7 (14.7) | W: R1: 61.1 (10) BMI: R1: 23.5 (3), |
| R2: 150 | R2: 56.2 (16) | R2: 60.5 (11.6), BMI: R2: 23 (3.1), | |||||
| P1: 75 | P1: 56.3 (17.6) | P1: 60.8 (10.8), BMI: P: 23.3 (3.4) | |||||
| Kim, 2024 [13] | South Korea | Prospective, randomized, controlled clinical trial | NCT05644483 | R: 47 | Eligibility Criteria: Included patients aged 19–80 years, ASA physical status 1–3, and undergoing major spinal surgery in the prone position. Excluded those with uncontrolled hypertension, significant cardiovascular/liver disease, glaucoma, alcoholism, or BMI < 15 or >35 kg/m2. | R: 67.4 ± 8.0 | R: 61.1 ± 9.0 kg |
| P: 47 | P:67.2 ± 7.5 | P:64.9 ± 9.2 kg | |||||
| Zhang, 2023 [14] | China | Prospective, double-blind, randomized controlled, non-inferiority trial | NCT04950621 | R: 71 | Adults (18+ years) scheduled for cerebral endovascular procedures under general anesthesia. ASA grade IV or higher. Hunt-Hess grade III or higher. BMI < 18 kg/m2 or >30 kg/m2. Previous cerebral endovascular procedures or surgical clipping. | R:56.6 ± 10.2 | R:24.2 ± 2.8 BMI |
| P:71 (69) | P: 56.0 ± 9.9 | P:24.5 ± 2.6 BMI | |||||
| Lee 2024 [15] | South Korea | Prospective, double-blind, randomized controlled trial | NCT04994704 | R:37 | Inclusion Criteria: Individuals aged 20–70 years, ASA I or III, who are undergoing elective spine surgery with intraoperative neurophysiological monitoring. Exclusion Criteria: Addiction or dependence on alcohol or psychotropic substances. Hypersensitivity or tolerance to benzodiazepines. Body mass index (BMI) exceeding 30 kg/m2. | R: 54.2 (Range: 27–66) | R: 65.0 (9.4) |
| P: 36 | P: 50.3 (Range: 33–66) | P:65.5 (11.6) | |||||
| Oh EJ, 2023 [12] | South Korea | Prospective, double-blind, randomized trial | KCT 0007132 | R: 50 | Eligibility Criteria: Patients between 19 and 75 years old ASA: I–III Reason for surgery: catheter ablation or atrial arrhythmia Exclusion Criteria: Adverse drug reactions (ADRs), moderate hepatic dysfunction, glaucoma, or metabolic disease. | R: 60 (Range: 54, 65) | BMI R: 26 (24.1, 27.7) |
| P: 50 | P: 60 (Range: 52, 64) | BMI P: 24.7 (22.5, 27.5) | |||||
| Shi F, 2022 [10] | China | Randomized, single-blind, prospective, single-center controlled trial | ChiCTR2100045710 | R: 38 | Eligibility Criteria: Included patients aged 20–80 years scheduled for EVL with recent bleeding history. Excluded those with ASA IV/V, active variceal bleeding, recent alcohol use, hepatic encephalopathy, neurological diseases, hemorrhagic shock, or allergies to benzodiazepine/propofol. | R: 52.74 (4.93) | R: 68.26 (5.11) |
| P: 38 | P: 51.71 (5.48) | P: 66 (5.27) | |||||
| Song SW, 2023 [4] | South Korea | Randomized parallel-group, single-blind controlled trial | KCT0007488 | R: 40 | Eligibility Criteria: Included patients aged 19–65 years with routine ACEI/ARB use and ASA status III or lower. Excluded emergency surgeries, BMI ≥ 35, uncontrolled hypertension, pregnancy, hepatic dysfunction (Class C), and those unable to consent. | R: 58.6 (6.4) | BMI R: 26.6 (4) |
| P: 41 | P: 60.1 (5.2) | BMI P: 26.3 (3.3) | |||||
| Luo W, 2023 [11] | China | Single-center, randomized, placebo-controlled, blinded, parallel trial | ChiCTR2100048904 | R: 39 | Eligibility Criteria: Included adults aged 18–75 years, ASA I–II, BMI 18-<30 kg/m2, undergoing day surgery with LMA. Excluded those with benzodiazepine allergy, recent benzodiazepine/opioid use, alcohol abuse, significant renal/hepatic dysfunction, cardiorespiratory instability, recent drug trial participation, or pregnancy. | R: 43.5 (15.6) | BMI R: 22.7 (3.4) W R: 63.6 (12.6) |
| P: 38 | P: 44.3 (18.1) | BMI P: 23.2 (3,7) W P: 65.9 (13.5) | |||||
| Tang, 2023 [2] | China | ECA, randomly allocated into the remimazolam group (R group) or the propofol group (P group) at a ratio of 1:1 | ChiCTR2100053014 | R: 56 | Eligibility Criteria: Included patients aged 18–65 years, ASA I–II, undergoing arthroscopic meniscus repair. Excluded severe respiratory/circulatory diseases, chronic analgesic/sedative use, alcohol abuse, and inability to understand scales or self-care pre-surgery. | R: 48.5 (Range: 19–62) | BMI: R: 24.7 (2.93) |
| P:58 | P: 50 (Range: 19–64) | BMI P: 23.9 (2.85) |
| Author, Year | INTERVENTION | CONTROL | OUTCOME | ||
|---|---|---|---|---|---|
| Drug | Doses | Description | Description | ||
| Doi, M. et al., 2020 [9] | Remimazolam | Remimazolan—Induction: 6 mg/kg/h or 12 mg/kg/h Remimazolan—Maintenance: 1.0–2.0 mg/kg/h | Induction: Administered at either 6 mg/kg/h or 12 mg/kg/h via continuous intravenous (IV) infusion until loss of consciousness (LoC), typically for up to 2.5 min. If LoC did not occur, the infusion was stopped, and another sedative was used. Maintenance: After induction, remimazolam was maintained at 1 mg/kg/h, adjustable up to a maximum of 2 mg/kg/h, depending on the patient’s condition, until the end of the surgery. Recovery: In cases where awakening was delayed, flumazenil was administered to expedite recovery. | Propofol—Induction: 2.0–2.5 mg/kg Propofol—Maintenance: 4–10 mg/kg/h Induction: Administered as a slow bolus of 2.0–2.5 mg/kg until LoC, which was expected to occur within 1 min. Maintenance: Continued infusion at 4–10 mg/kg/h, adjustable based on the patient’s condition until the end of surgery. Recovery: Patients were monitored for spontaneous recovery or given additional medication as needed. | Primary outcomes: (1) intraoperative awakening or recall, (2) the need for rescue sedative medication, and (3) body movement Secondary outcomes: (1) responding to verbal stimuli, (2) adequate recovery of respiratory function, (3) stable blood pressure (BP) and heart rate (HR), and (4) recovery of muscle strength |
| Kim, 2024 [13] | Remimazolam | Induction: 6 mg/kg/h. Maintenance: 1–2 mg/kg/h. | Induction with remimazolam was performed at a rate of 6 mg/kg/h. For anesthesia maintenance, the Remimazolam infusion was adjusted between 1–2 mg/kg/h to maintain a patient state index between 25 and 50 | Propofol—Induction: Target-controlled infusion (TCI) using a Schneider pharmacokinetic model, with an effect-site concentration of 2.0 µg/mL and maintenance of 2–3 µg/mL. The propofol infusion rate was increased by 0.5 µg/mL every 30 s until loss of consciousness. | Primary outcomes: incidence of hypotensive episodes during the first hour after prone positioning Secondary outcomes included the incidence of severe hypotension and the total amount of inotropic or vasopressor medication |
| Zhang, 2023 [14] | Remimazolam | Induction: IV injection remimazolam 0.1 mg kg−1. Maintained with remimazolam 0.3–0.7 mg kg−1 h−1 | After loss of consciousness upon anesthesia induction, Sufentanil (0.2–0.3 mg kg−1) and rocuronium (0.6–0.9 mg kg−1) were given to facilitate endotracheal intubation. Remifentanil was infused intravenously at 0.1–0.3 μg kg−1 h−1 during anesthesia maintenance. Rocuronium was injected intermittently as needed. | Induced with intravenous injection of propofol 1–1.5 mg kg−1 and maintained with propofol 4–10 mg kg−1 h−1. Also received Sufentanil and rocuronium for intubation and remifentanil for maintenance, with mechanical ventilation to maintain a Bispectral Index (BIS) between 40 and 60. | The primary outcome was time to emergence, defined as the interval from discontinuation of study drugs to eye opening upon verbal command (mITT): 16.1 ± 10.4 min in the remimazolam group vs. 19.0 ± 11.2 min in the propofol group. Secondary outcomes included the time to loss of consciousness (LoC); episode of hypotension (remimazolam group had lower rate of hypotensive episodes during anesthesia induction (11.3% vs. 25.4% in the propofol group, RR = 0.44 [95% CI: 0.21, 0.96], P = 0.03)); intraoperative use of vasoactive drugs; incidence of postoperative delirium (POD) during emergence; major complications prior to patient discharge; length of hospital stay and Glasgow Coma Scale (GCS) at discharge; the level of lactate in arterial blood, serum IL-6, TNF-α, and S100β at the end of the surgery; mRS at 30 and 90 days after surgery. |
| Lee 2024 [15] | Remimazolam | Remimazolam—Induction: 6–12 mg/kg/h Remimazolam—Maintenance 1–2 mg/kg/h | Induction with remimazolam at a rate of 6–12 mg/kg/h until loss of consciousness, followed by maintenance at 1.0–2.0 mg/kg/h. Concurrent administration of remifentanil using target-controlled infusion (TCI) based on the Minto model. | Propofol—Induction: 3.0 ng/mL−1. Induction using propofol at a targeted concentration of 3.0 ng/mL, followed by maintenance using the same target-controlled infusion method. Remifentanil was also administered similarly to the remimazolam group. | The primary outcome of our study was the total QoR-15 (Quality of Recovery) score measured on postoperative day (POD) 1. Secondary outcomes: We investigated hemodynamic parameters such as MAP, heart rate, peripheral oxygen saturation, and PSI values. |
| Oh EJ, 2023 [12] | Remimazolam | Remimazolan–Induction: 6 mg/kg/h Remimazolan–Maintenance: 1.0 y 2.0 mg/kg/h | Remimazolam Group: Patients received continuous infusion of remimazolam at 6 mg/kg/h for induction, adjusted to 1.0–2.0 mg/kg/h for maintenance. Maintenance: In both groups, remifentanil was infused at a rate of 0.05–0.20 μg/kg/min for analgesia. Rocuronium was used to achieve neuromuscular blockade. | Propofol Group: Patients received target-controlled infusion (TCI) of propofol at an effect-site concentration of 5.0 μg/mL for induction, adjusted to 3.0–5.0 μg/mL for maintenance. Maintenance: In both groups, remifentanil was infused at a rate of 0.05–0.20 μg/kg/min for analgesia. Rocuronium was used to achieve neuromuscular blockade. | Outcomes assessed Primary: obeying verbal commands Secondary: -Bispectral Index (BIS) -Time until laryngeal mask airway removal -RASS -Adverse events |
| Shi F, 2022 [10] | Remimazolam | Remimazolan–Induction: 0.2 mg/kg Remimazolan–Maintenance: 1 mg/kg/h | Induction: Remimazolam tosylate was administered as a slow bolus of 0.2 mg/kg. Maintenance: Following induction, remimazolam was continuously infused at a rate of 1.0–2.0 mg/kg/h during the procedure. Anesthesia Monitoring: All patients were monitored for vital signs, including mean arterial blood pressure (MAP), heart rate (HR), pulse oxygen saturation (SpO2), end-tidal CO2 partial pressure (PetCO2), and Bispectral Index (BIS). The depth of anesthesia was assessed using the Modified Observer’s Assessment of Alertness/Sedation (MOAA/S) scale. Recovery: At the end of the surgery, flumazenil was administered to patients in the remimazolam group to reverse the effects of the anesthetic and facilitate faster recovery. The same volume of saline was given to patients in the propofol group. | Propofol Group (Group P): Induction: Propofol was administered at 2 mg/kg. Maintenance: Continuous infusion of propofol was maintained at a rate of 4–10 mg/kg/h. Anesthesia Monitoring: All patients were monitored for vital signs, including mean arterial blood pressure (MAP), heart rate (HR), pulse oxygen saturation (SpO2), end-tidal CO2 partial pressure (PetCO2), and Bispectral Index (BIS). The depth of anesthesia was assessed using the Modified Observer’s Assessment of Alertness/Sedation (MOAA/S) scale. | Outcomes assessed Primary: success of the surgical procedure/MOAA Secondary: -Anesthetic time -Vital signs: MAP, heart rate -Hypotension -Adverse events after surgery: Hypotension, nausea and vomiting -Patient and operator satisfaction |
| Song SW, 2023 [4] | Remimazolam | Remimazolan–Induction: 6 mg/kg/h Remimazolan–Maintenance: 1 mg/kg/h | Remimazolam Group (Group R): Patients received a saline placebo followed by remimazolam at 6 mg/kg/h for induction and 1 mg/kg/h for maintenance. The infusion rate of remimazolam was adjusted if the Bispectral Index (BIS) exceeded 60. Maintenance: In both groups, remifentanil was infused at 0.25 µg/kg/min. Rocuronium was used for neuromuscular blockade, and orotracheal intubation was performed after two and a half minutes. | Propofol Group (Group P): Patients received propofol at 2 mg/kg for induction, followed by an infusion of remimazolam at 0.1 mg/kg/h for blinding purposes. Maintenance: In both groups, remifentanil was infused at 0.25 µg/kg/min. Rocuronium was used for neuromuscular blockade, and orotracheal intubation was performed after two and a half minutes. | Primary outcome was the incidence of hypotension following anesthesia induction. Secondary outcomes were heart rate, mean, systolic, and diastolic blood pressure (MBP, SBP, and DBP), and Bispectral Index (BIS). |
| Luo W, 2023 [11] | Remimazolam | Remimazolan—Induction: 0.3 mg/kg, Remimazolan—Maintenance: 1–3 mg/kg/h | RT Group: Received remimazolam tosylate at 0.3 mg/kg intravenously. If loss of consciousness (LoC) did not occur within 3 min, an additional dose of 0.1 mg/kg was administered. RT Group: Anesthesia was maintained with remimazolam tosylate at 1–3 mg/kg/h. Additional Medications: Sufentanil (0.2–0.4 µg/kg) was administered during induction, and rocuronium (0.2–0.4 mg/kg) was used for muscle paralysis before inserting a laryngeal mask airway (LMA). Monitoring and Adjustments: The depth of anesthesia was monitored using the Bispectral Index (BIS). Hypotension (SBP < 80% of baseline) was treated with ephedrine or phenylephrine, and sinus bradycardia (HR < 40 beats/min) was treated with atropine. | Induction: Patients in the propofol group received an intravenous bolus of propofol at a dose of 2.0–2.5 mg/kg. If loss of consciousness (LoC) did not occur within 3 min, an additional dose of 1.0 mg/kg of propofol was administered. Maintenance: After induction, anesthesia was maintained with a continuous infusion of propofol at a rate of 6–12 mg/kg/h. Remifentanil was concurrently administered at a rate of 0.05–0.15 µg/kg/min to provide analgesia during surgery. Monitoring: The depth of anesthesia was monitored using the Bispectral Index (BIS) to ensure it stayed within the desired range (typically between 40 and 60). Vital signs, including systolic blood pressure (SBP), diastolic blood pressure (DBP), heart rate (HR), and oxygen saturation (SpO2), were continuously monitored. | Outcomes assessed Primary: -Induction time -Alert time Secondary: -Success rate -BIS -MOAA -Adverse events (hypotension, bradycardia, hypoxia) |
| Tang, 2023 [2] | Remimazolam | Remimazolam–Induction: 6 mg/kg/h Remimazolam–Maintenance: 0.4–2 mg/kg/h | Induction: Patients in the R Group received remimazolam besylate at an intravenous infusion rate of 6 mg/kg/h for the induction of anesthesia. Maintenance: After induction, anesthesia was maintained by adjusting the remimazolam dose within a range of 0.4–2 mg/kg/h to achieve the desired depth of anesthesia, monitored using the Bispectral Index (BIS), which was targeted between 40 and 60. Remifentanil was also administered at a rate of 0.1–0.3 µg/kg/min to provide analgesia during the surgery. Procedure: Following the loss of consciousness (LOC), cisatracurium (0.2 mg/kg) was administered to facilitate the placement of a laryngeal mask airway (LMA). Volume-controlled mechanical ventilation was adjusted to maintain an end-tidal CO2 (EtCO2) concentration between 4.66 and 5.99 kPa. | Induction: Patients in the Propofol Group received propofol through plasma target-controlled infusion (TCI). The initial target concentration was set at 2 µg/mL and could be increased up to 3.5 µg/mL to achieve the desired level of anesthesia. Maintenance: After induction, anesthesia was maintained by adjusting the propofol concentration within the range of 1–3 µg/mL to maintain a Bispectral Index (BIS) between 40 and 60, ensuring appropriate depth of anesthesia. Remifentanil was administered at a rate of 0.1–0.3 µg/kg/min to provide analgesia during surgery. Procedure: Once loss of consciousness (LOC) was achieved, cisatracurium (0.2 mg/kg) was administered to facilitate the placement of a laryngeal mask airway (LMA). Volume-controlled mechanical ventilation was adjusted to maintain an end-tidal CO2 (EtCO2) concentration between 4.66 and 5.99 kPa. | Primary outcome: QoR-15 score Secondary outcomes: LOC BIS 60 Extubation time RSS Adverse events |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Muñoz-Carrillo, J.L.; Rodríguez-Cortes, N.; Lévano, S.T.; Moran-Mariños, C.; Barboza, J.J. Remimazolam Versus Propofol in General Anesthesia of Complex Surgery in Critical and Non-Critical Patients: Meta-Analysis of Randomized Trials. J. Clin. Med. 2024, 13, 7791. https://doi.org/10.3390/jcm13247791
Muñoz-Carrillo JL, Rodríguez-Cortes N, Lévano ST, Moran-Mariños C, Barboza JJ. Remimazolam Versus Propofol in General Anesthesia of Complex Surgery in Critical and Non-Critical Patients: Meta-Analysis of Randomized Trials. Journal of Clinical Medicine. 2024; 13(24):7791. https://doi.org/10.3390/jcm13247791
Chicago/Turabian StyleMuñoz-Carrillo, José Luis, Natalie Rodríguez-Cortes, Sandra Trujillo Lévano, Cristian Moran-Mariños, and Joshuan J. Barboza. 2024. "Remimazolam Versus Propofol in General Anesthesia of Complex Surgery in Critical and Non-Critical Patients: Meta-Analysis of Randomized Trials" Journal of Clinical Medicine 13, no. 24: 7791. https://doi.org/10.3390/jcm13247791
APA StyleMuñoz-Carrillo, J. L., Rodríguez-Cortes, N., Lévano, S. T., Moran-Mariños, C., & Barboza, J. J. (2024). Remimazolam Versus Propofol in General Anesthesia of Complex Surgery in Critical and Non-Critical Patients: Meta-Analysis of Randomized Trials. Journal of Clinical Medicine, 13(24), 7791. https://doi.org/10.3390/jcm13247791