

Growth Differentiation Factor 15 as a Marker for Chronic Ventricular Pacing


 , , ,
, , ,
Abstract
1. Introduction
2. Materials and Methods
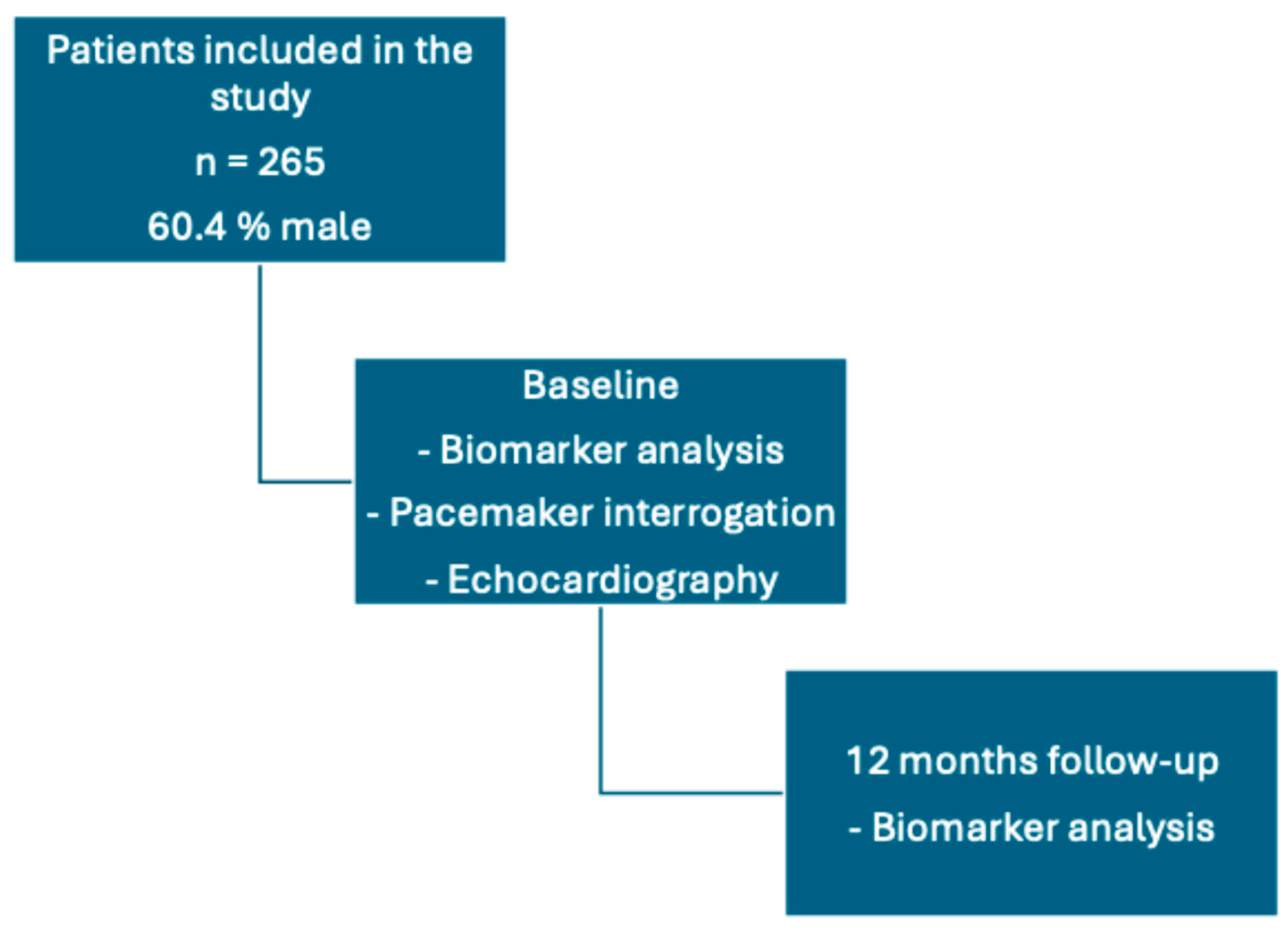
2.1. Study Population
2.2. Biomarker Analysis
2.3. Statistical Analysis
3. Results
4. Discussion
- (1)
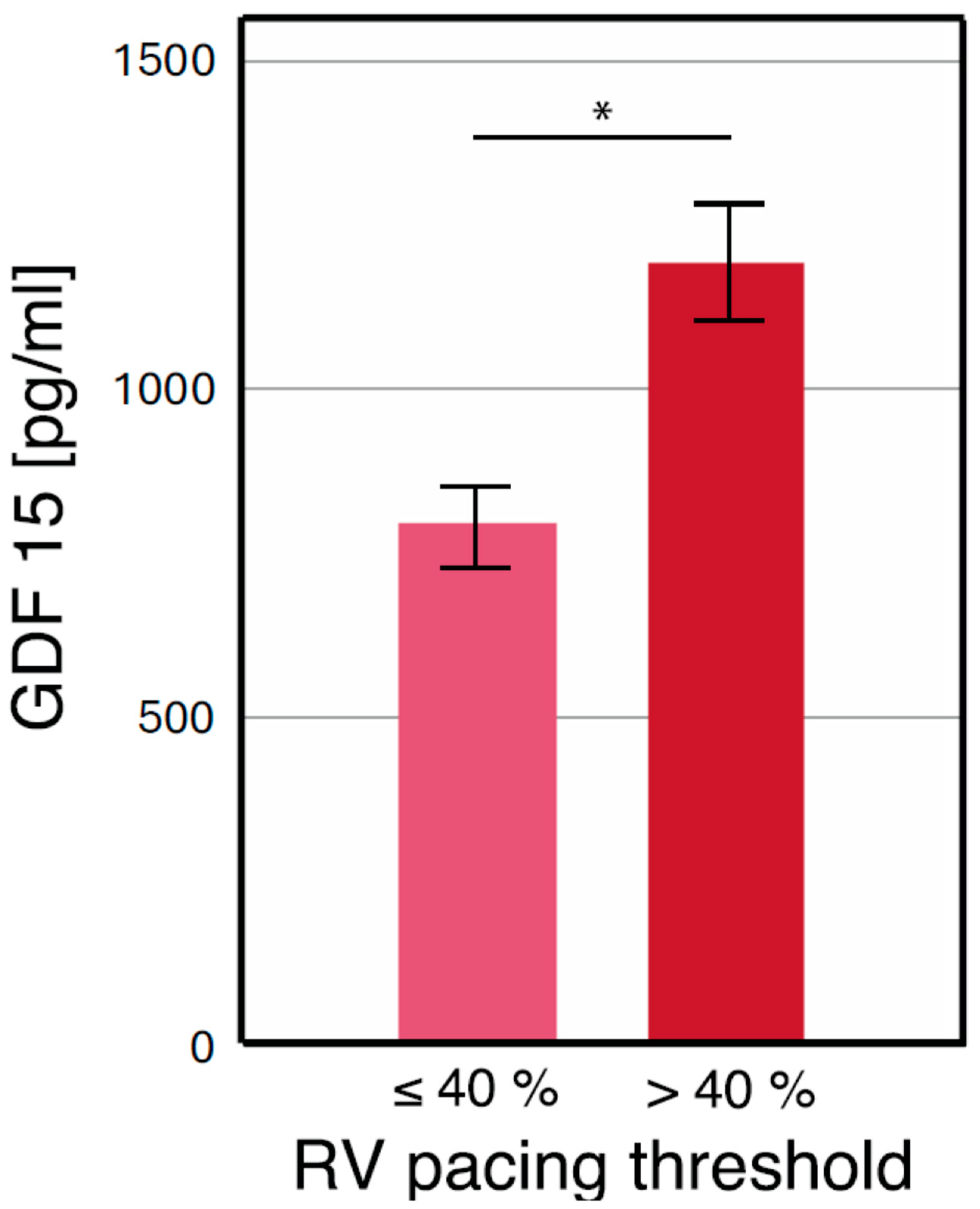
- GDF-15 was significantly increased in patients with increased RVP burden.
- (2)
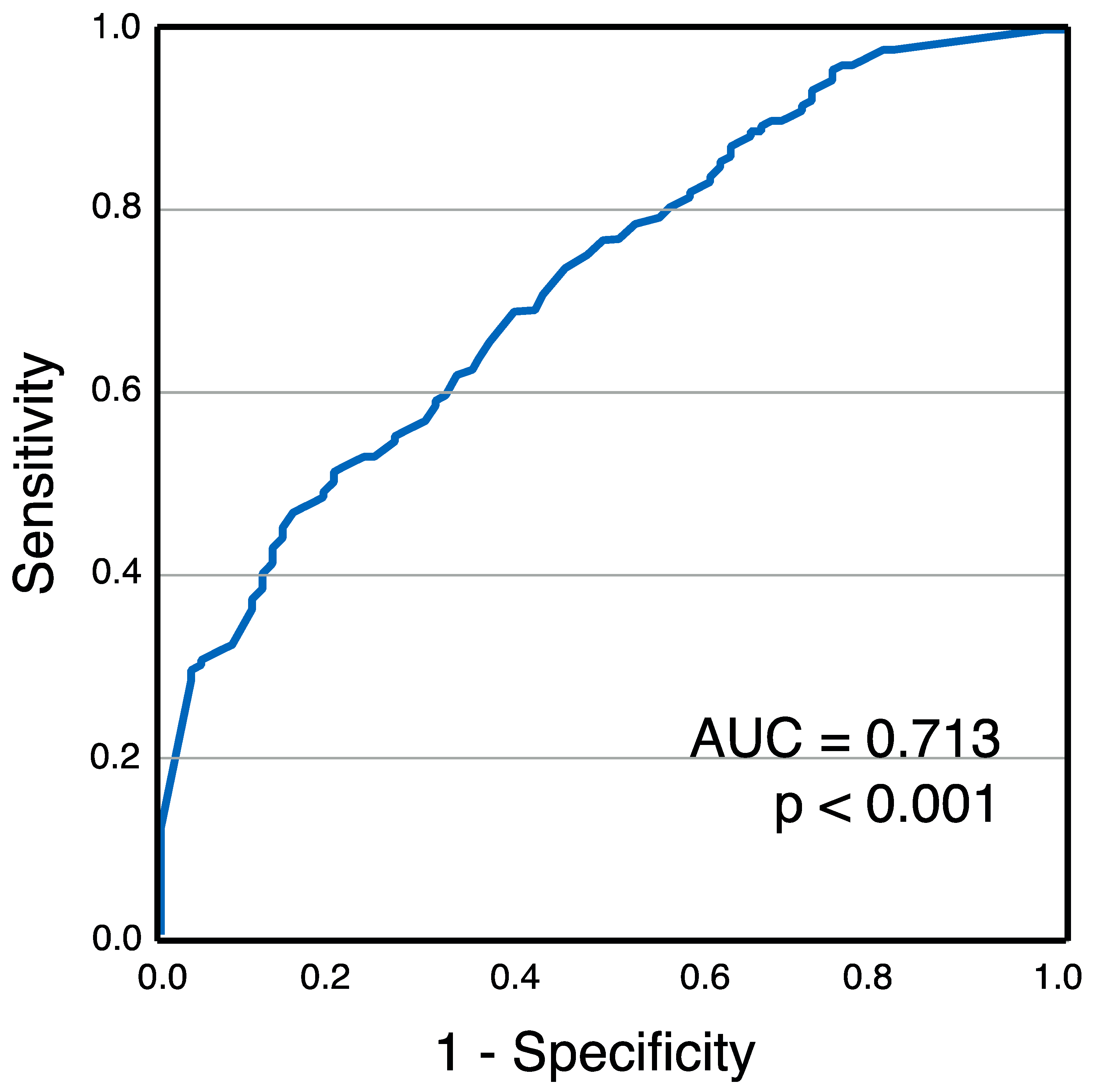
- GDF-15 could be identified as a potential biomarker for RV pacing.
- (3)
- GDF-15 is an emerging biomarker associated with a variety of cardiovascular pathologies, including heart failure and myocardial stress. The correlation between elevated GDF-15 levels and a right ventricular (RV) pacing >40 suggests that GDF-15 may serve as a valuable marker in the context of PiCM.
4.1. Mechanistic Insights
4.2. Potential Clinical Implications
- (1)
- Early Detection: Utilizing GDF-15 levels as a biomarker could facilitate the early identification of patients at risk for PiCM. Patients presenting with a high RVP burden and elevated GDF-15 levels might be more closely monitored for early signs of ventricular dysfunction, enabling timely intervention.
- (2)
- Risk Stratification: GDF-15 could potentially be integrated into risk stratification models for patients requiring pacemakers. Higher GDF-15 levels in conjunction with elevated pacing burden could identify a subgroup of patients at greater risk for adverse outcomes, thus tailoring follow-up schedules and management strategies accordingly.
- (3)
- Guiding Therapy: For patients with high GDF-15 levels and elevated RVP burden, clinicians might consider alternative pacing strategies, such as CRT or His-bundle pacing, to mitigate the risk of developing PiCM. These alternatives can preserve more natural ventricular contraction patterns, potentially reducing myocardial stress and preventing adverse remodeling.
- (4)
- Monitoring Disease Progression: Serial measurements of GDF-15 could be useful in monitoring the progression of PiCM. Rising GDF-15 levels might indicate worsening myocardial stress and dysfunction, prompting adjustments in pacing strategies or the initiation of heart failure therapies.
- (5)
- Research Implications: Further research is warranted to explore the causal relationships between GDF-15 levels, RVP burden, and the development of PiCM. Longitudinal studies could help establish the predictive value of GDF-15 and elucidate the underlying mechanisms linking pacing-induced myocardial stress with biomarker elevation.
- (1)
- Establishing definitive GDF-15 thresholds that predict adverse outcomes in pacemaker patients.
- (2)
- Evaluating the impact of CRT upgrades in patients identified by elevated GDF-15 levels and high RVP burden.
- (3)
- Investigating the long-term benefits of CRT upgrades guided by GDF-15, including improvements in heart failure symptoms, hospitalization rates, and mortality. The use of GDF-15 as a biomarker to guide CRT upgrades represents another promising future direction in the management of pacemaker patients. This approach could lead to more personalized, timely, and effective interventions, ultimately enhancing patient care and outcomes.
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Glikson, M.; Nielsen, J.C. 2021 ESC Guidelines on cardiac pacing and cardiac resynchronization therapy. Eur. Heart J. 2021, 42, 3427–3520. [Google Scholar] [CrossRef]
- Shantha, G.; Brock, J. Anatomical location of leadless pacemaker and the risk of pacing-induced cardiomyopathy. J. Cardiovasc. Electrophysiol. 2023, 34, 1418–1426. [Google Scholar] [CrossRef]
- Shen, L.; Jhund, P.S. Prior Pacemaker Implantation and Clinical Outcomes in Patients With Heart Failure and Preserved Ejection Fraction. JACC Heart Fail. 2019, 7, 418–427. [Google Scholar] [CrossRef]
- Khazanie, P.; Hellkamp, A.S. Permanent pacemaker use among patients with heart failure and preserved ejection fraction: Findings from the Acute Decompensated Heart Failure National Registry (ADHERE) National Registry. Am. Heart J. 2018, 198, 123–128. [Google Scholar] [CrossRef]
- Tayal, B.; Fruelund, P. Incidence of heart failure after pacemaker implantation: A nationwide Danish Registry-based follow-up study. Eur. Heart J. 2019, 40, 3641–3648. [Google Scholar] [CrossRef] [PubMed]
- Merchant, F.M.; Mittal, S. Pacing induced cardiomyopathy. J. Cardiovasc. Electrophysiol. 2020, 31, 286–292. [Google Scholar] [CrossRef] [PubMed]
- Khurshid, S.; Epstein, A.E. Incidence and predictors of right ventricular pacing-induced cardiomyopathy. Heart Rhythm 2014, 11, 1619–1625. [Google Scholar] [CrossRef] [PubMed]
- Kiehl, E.L.; Makki, T. Incidence and predictors of right ventricular pacing-induced cardiomyopathy in patients with complete atrioventricular block and preserved left ventricular systolic function. Heart Rhythm 2016, 13, 2272–2278. [Google Scholar] [CrossRef] [PubMed]
- Somma, V.; Ha, F.J.; Palmer, S. A systematic review and meta-analysis of definition, prevalence, risk factors, and management. Heart Rhythm 2023, 20, 282–290. [Google Scholar] [CrossRef] [PubMed]
- Abbas, J.; Zulqarnain, M. Incidence and predictors of pacemaker-induced cardiomyopathy with right ventricular pacing: A systematic review. Expert Rev. Cardiovasc. Ther. 2022, 20, 267–273. [Google Scholar] [CrossRef]
- Arnold, M.; Richards, M. Avoiding unnecessary ventricular pacing is associated with reduced incidence of heart failure hospitalizations and persistent atrial fibrillation in pacemaker patients. Europace 2023, 25, euad065. [Google Scholar] [CrossRef] [PubMed]
- Chung, M.K.; Patton, K.K. 2023 HRS/APHRS/LAHRS guideline on cardiac physiologic pacing for the avoidance and mitigation of heart failure. Heart Rhythm 2023, 20, e17–e91. [Google Scholar] [CrossRef] [PubMed]
- Heidenreich, P.A.; Bozkurt, B. 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 2022, 145, e895–e1032. [Google Scholar] [CrossRef]
- May, B.M.; Pimentel, M. GDF-15 as a Biomarker in Cardiovascular Disease. Arq. Bras. Cardiol. 2021, 116, 494–500. [Google Scholar] [PubMed]
- Meijers, W.C.; Bayes-Genis, A. Circulating heart failure biomarkers beyond natriuretic peptides: Review from the Biomarker Study Group of the Heart Failure Association (HFA), European Society of Cardiology (ESC). Eur. J. Heart Fail. 2021, 23, 1610–1632. [Google Scholar] [CrossRef] [PubMed]
- Cheng, J.M.; Akkerhuis, K.M. Biomarkers of heart failure with normal ejection fraction: A systematic review. Eur. J. Heart Fail. 2013, 15, 1350–1362. [Google Scholar] [CrossRef] [PubMed]
- Siddiqui, J.A.; Pothuraju, R. Pathophysiological role of growth differentiation factor 15 (GDF15) in obesity, cancer, and cachexia. Cytokine Growth Factor Rev. 2022, 64, 71–83. [Google Scholar] [CrossRef] [PubMed]
- Wang, T.; Liu, J.; McDonald, C. GDF15 is a heart-derived hormone that regulates body growth. EMBO Mol. Med. 2017, 9, 1150–1164. [Google Scholar] [CrossRef] [PubMed]
- Wang, D.; Day, E.A. GDF15: Emerging biology and therapeutic applications for obesity and cardiometabolic disease. Nat. Rev. Endocrinol. 2021, 17, 592–607. [Google Scholar] [CrossRef]
- Xiao, Q.A.; He, Q. GDF-15, a future therapeutic target of glucolipid metabolic disorders and cardiovascular disease. Biomed. Pharmacother. 2022, 146, 112582. [Google Scholar] [CrossRef] [PubMed]
- Sharma, A.; Stevens, S.R. Prognostic Utility of Growth Differentiation Factor-15 in Patients With Chronic Heart Failure. J. Am. Coll. Cardiol. 2007, 50, 1054–1060. [Google Scholar]
- Rabkin, S.W.; Tang, J.K.K. The utility of growth differentiation factor-15, galectin-3, and sST2 as biomarkers for the diagnosis of heart failure with preserved ejection fraction and compared to heart failure with reduced ejection fraction: A systematic review. Heart Fail. Rev. 2021, 26, 799–812. [Google Scholar] [CrossRef] [PubMed]
- Sawalha, K.; Norgard, N.B.; Drees, B.M.; López-Candales, A. Growth Differentiation Factor 15 (GDF-15), a New Biomarker in Heart Failure Management. Curr. Heart Fail. Rep. 2023, 20, 287–299. [Google Scholar] [CrossRef]
- Gavaghan, C. Pacemaker Induced Cardiomyopathy: An Overview of Current Literature. Curr. Cardiol. Rev. 2022, 18, e010921196020. [Google Scholar] [CrossRef] [PubMed]
- Daley, W.R.; Kaczmarek, R.G. The Epidemiology of Cardiac Pacemakers in the Older US Population. J. Am. Geriatr. Soc. 2015, 46, 1016–1019. [Google Scholar] [CrossRef]
- Bannehr, M.; Edlinger, C.; Lichtenauer, M.; Wernly, B.; Hauptmann, L.; Paar, V.; Hoppe, U.; Motloch, L.J.; Butter, C.; Schernthaner, C. Growth differentiation factor 15 as marker for chronic right ventricular pacing. Clin. Res. Cardiol. 2023, 112, 1005. [Google Scholar] [CrossRef]
- Lichtenauer, M.; Jirak, P.; Wernly, B.; Paar, V.; Rohm, I.; Jung, C.; Schernthaner, C.; Kraus, J.; Motloch, L.J.; Yilmaz, A.; et al. A comparative analysis of novel cardiovascular biomarkers in patients with chronic heart failure. Eur. J. Intern. Med. 2017, 44, 31–38. [Google Scholar] [CrossRef] [PubMed]
- Castiglione, V.; Aimo, A.; Vergaro, G.; Saccaro, L.; Passino, C.; Emdin, M. Biomarkers for the diagnosis and management of heart failure. Heart Fail. Rev. 2022, 27, 625–643. [Google Scholar] [CrossRef] [PubMed]
- Gaggin, H.K.; Januzzi, J.L., Jr. Biomarkers and diagnostics in heart failure. Biochim. Biophys. Acta 2013, 1832, 2442–2450. [Google Scholar] [CrossRef] [PubMed]
- Malikides, O.; Simantirakis, E.; Zacharis, E.; Fragkiadakis, K.; Kochiadakis, G.; Marketou, M. Cardiac Remodeling and Ventricular Pacing: From Genes to Mechanics. Genes 2024, 15, 671. [Google Scholar] [CrossRef] [PubMed]
- Spragg, D.D.; Kass, D.A. Pathobiology of left ventricular dyssynchrony and resynchronization. Prog. Cardiovasc. Dis. 2006, 49, 26–41. [Google Scholar] [CrossRef] [PubMed]
- Schwinger, R.H.G. Pathophysiology of heart failure. Cardiovasc. Diagn. Ther. 2021, 11, 263–276. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Overall n = 265 | VP < 40% n = 89 | VP ≥ 40% n = 176 | p-Value | |
|---|---|---|---|---|
| Sex male [%] | 60.4 | 50.6 | 67.4 | 0.011 |
| Age [years] | 72.1 ± 11.4 | 68.9 ± 13.7 | 73.7 ± 9.7 | 0.005 |
| Body mass index [kg/m2] | 27.3 ± 4.8 | 27.9 ± 5.7 | 26.9 ± 4.4 | 0.145 |
| Hypertension [%] | 81.5 | 74.2 | 82.0 | 0.150 |
| Type II diabetes [%] | 21.2 | 15.7 | 22.5 | 0.414 |
| Coronary artery disease [%] | 26.4 | 21.3 | 29.8 | 0.188 |
| Chronic kidney disease [%] | 23.0 | 13.5 | 27.0 | 0.013 |
| Atrial fibrillation [%] | 63.4 | 46.1 | 71.9 | <0.001 |
| Echocardiographic parameters | ||||
| Left ventricular ejection fraction [%] | 54.3 ± 5.8 | 56.6 ± 4.5 | 53.1 ± 6.2 | <0.001 |
| Left ventricular end-diastolic diameter [mm] | 46.2 ± 6.1 | 44.9 ± 5.0 | 46.9 ± 6.6 | 0.009 |
| Left atrial volume [mL] | 75.8 ± 36.9 | 62.3 ± 25.1 | 82.7 ± 40.0 | <0.001 |
| Right atrial volume [mL] | 49.7 ± 23.8 | 40.6 ± 10.7 | 54.2 ± 26.9 | <0.001 |
| Pacemaker parameters | ||||
| Indication for pacemaker implantation | <0.001 | |||
| Sick sinus syndrome | 20.6 | 42.7 | 9.6 | |
| Bradycardia–tachycardia syndrome (incl. brady AF) | 16.4 | 10.0 | 18.6 | |
| AV-Block II | 19.6 | 13.6 | 23.1 | |
| AV-Block III | 42.8 | 33.7 | 47.6 | |
| Other (cardioinhibitory syncope, sinus syndrome) | 0.7 | 0 | 1.1 | |
| Pacemaker type | <0.001 | |||
| Single-chamber pacemaker [%] | 19.6 | 5.6 | 25.8 | |
| Dual-chamber pacemaker [%] | 80.4 | 94.4 | 74.2 | |
| Pacemaker mode | <0.001 | |||
| DDD | 66.2 | 71.9 | 63.3 | |
| VVI | 22.6 | 6.7 | 30.5 | |
| AAI-DDD | 10.2 | 20.3 | 5.1 | |
| DDI | 1.0 | 1.0 | 1.1 | |
| Mode switch [%] | 1.0 IQR 1.82 | 1 IQR 0.09 | 1 IQR 5.15 | 0.209 |
| Activation of sensor | 38.3 | 46.1 | 34.3 | 0.082 |
| Ventricular pacing [%] | 62.5 ± 441.1 | 8.3 ± 10.3 | 89.6 ± 16.7 | <0.001 |
| Atrial pacing [%] | 28.4 ± 34.9 | 35.6 ± 37.2 | 24.5 ± 33.2 | 0.019 |
| Baseline | Follow-Up | p-Value | |
|---|---|---|---|
| GDF-15 [pg/mL] | 988.2 ± 497.5 | 1324.4 ± 810 | 0.001 |
| NT-proBNP [pg/mL] | 957.6 ± 2303.9 | 1377.8 ± 3449.5 | 0.001 |
| eGFR [mL/min] | 61.1 ± 11.3 | 59.4 ± 13.4 | 0.02 |
| Hemoglobin [g/dL] | 13.8 ± 1.6 | 13.7 ± 1.7 | 0.102 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Edlinger, C.; Bannehr, M.; Lichtenauer, M.; Paar, V.; Jankowska, P.; Hauptmann, L.; Hoppe, U.C.; Butter, C.; Schernthaner, C. Growth Differentiation Factor 15 as a Marker for Chronic Ventricular Pacing. J. Clin. Med. 2024, 13, 7748. https://doi.org/10.3390/jcm13247748
Edlinger C, Bannehr M, Lichtenauer M, Paar V, Jankowska P, Hauptmann L, Hoppe UC, Butter C, Schernthaner C. Growth Differentiation Factor 15 as a Marker for Chronic Ventricular Pacing. Journal of Clinical Medicine. 2024; 13(24):7748. https://doi.org/10.3390/jcm13247748
Chicago/Turabian StyleEdlinger, Christoph, Marwin Bannehr, Michael Lichtenauer, Vera Paar, Paulina Jankowska, Laurenz Hauptmann, Uta C. Hoppe, Christian Butter, and Christiana Schernthaner. 2024. "Growth Differentiation Factor 15 as a Marker for Chronic Ventricular Pacing" Journal of Clinical Medicine 13, no. 24: 7748. https://doi.org/10.3390/jcm13247748
APA StyleEdlinger, C., Bannehr, M., Lichtenauer, M., Paar, V., Jankowska, P., Hauptmann, L., Hoppe, U. C., Butter, C., & Schernthaner, C. (2024). Growth Differentiation Factor 15 as a Marker for Chronic Ventricular Pacing. Journal of Clinical Medicine, 13(24), 7748. https://doi.org/10.3390/jcm13247748