

Pulmonary Embolism Response Teams—Evidence of Benefits? A Systematic Review and Meta-Analysis
 , , , and
, , , and
Abstract
1. Introduction
2. Methods
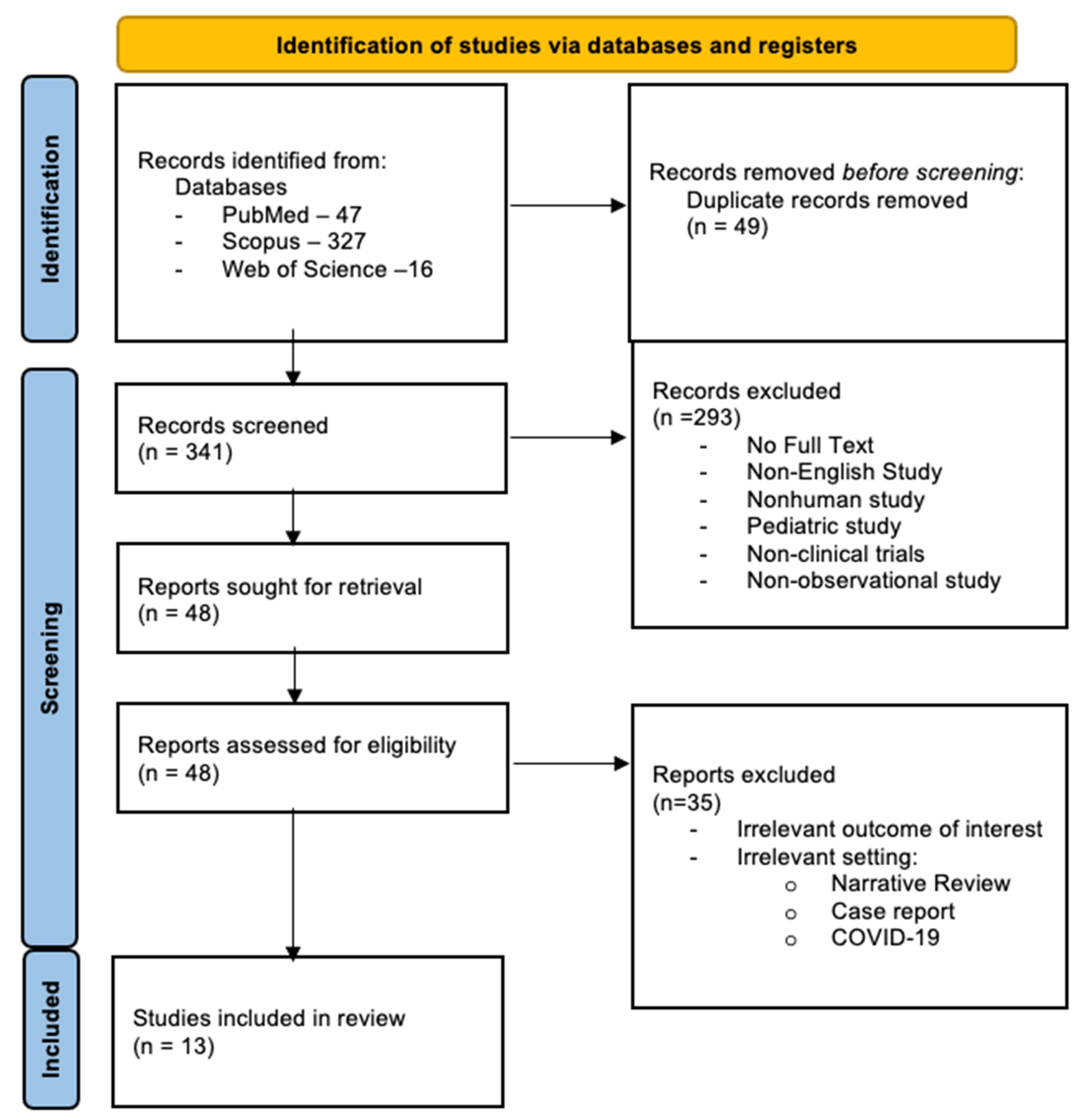
2.1. Study Selection
2.2. Search Criteria
2.3. Study Selection and Data Extraction
2.4. Quality Assessment
2.5. Statistical Analysis
3. Results
3.1. Study Description
3.2. Summary of Studies
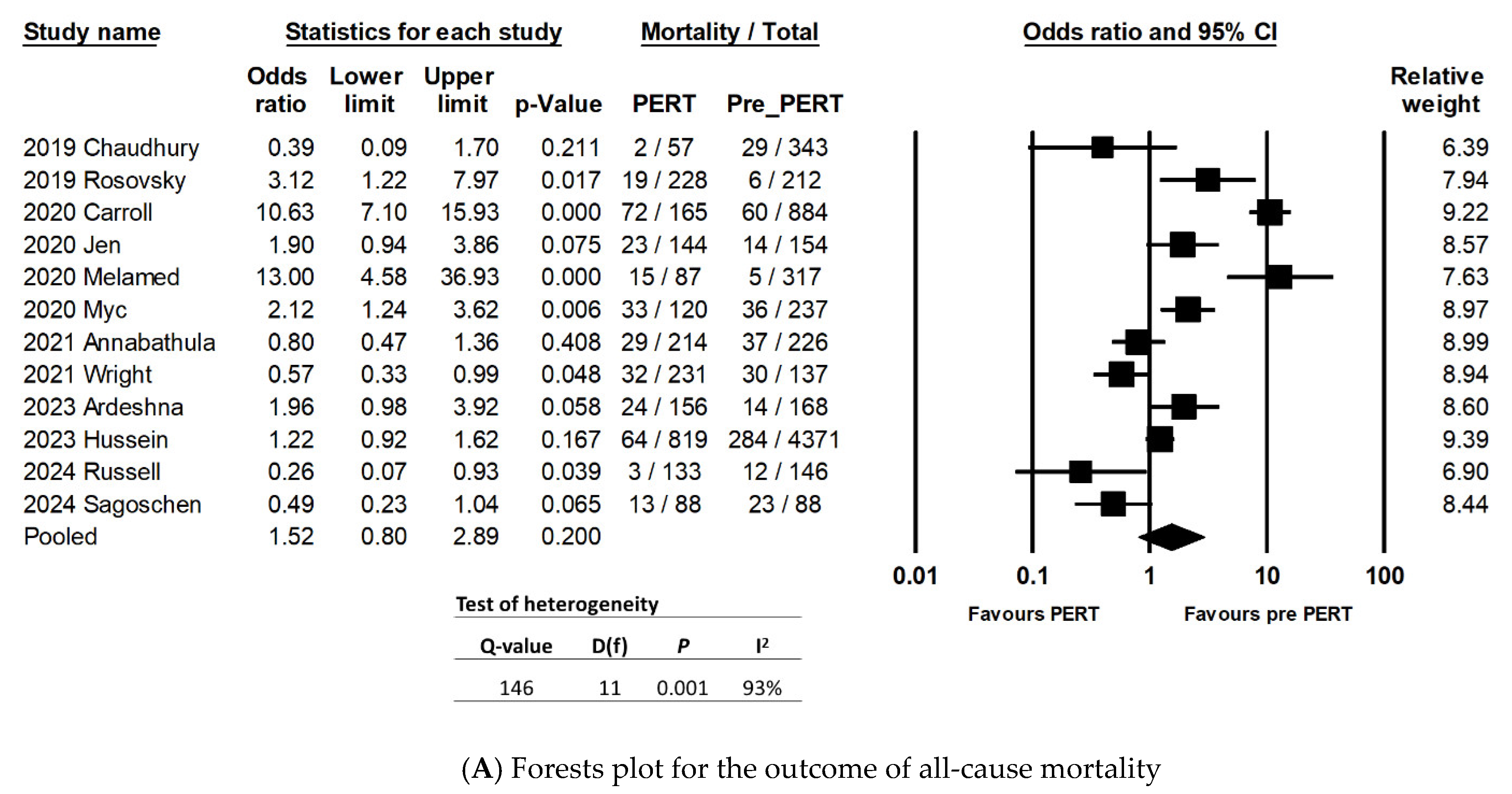
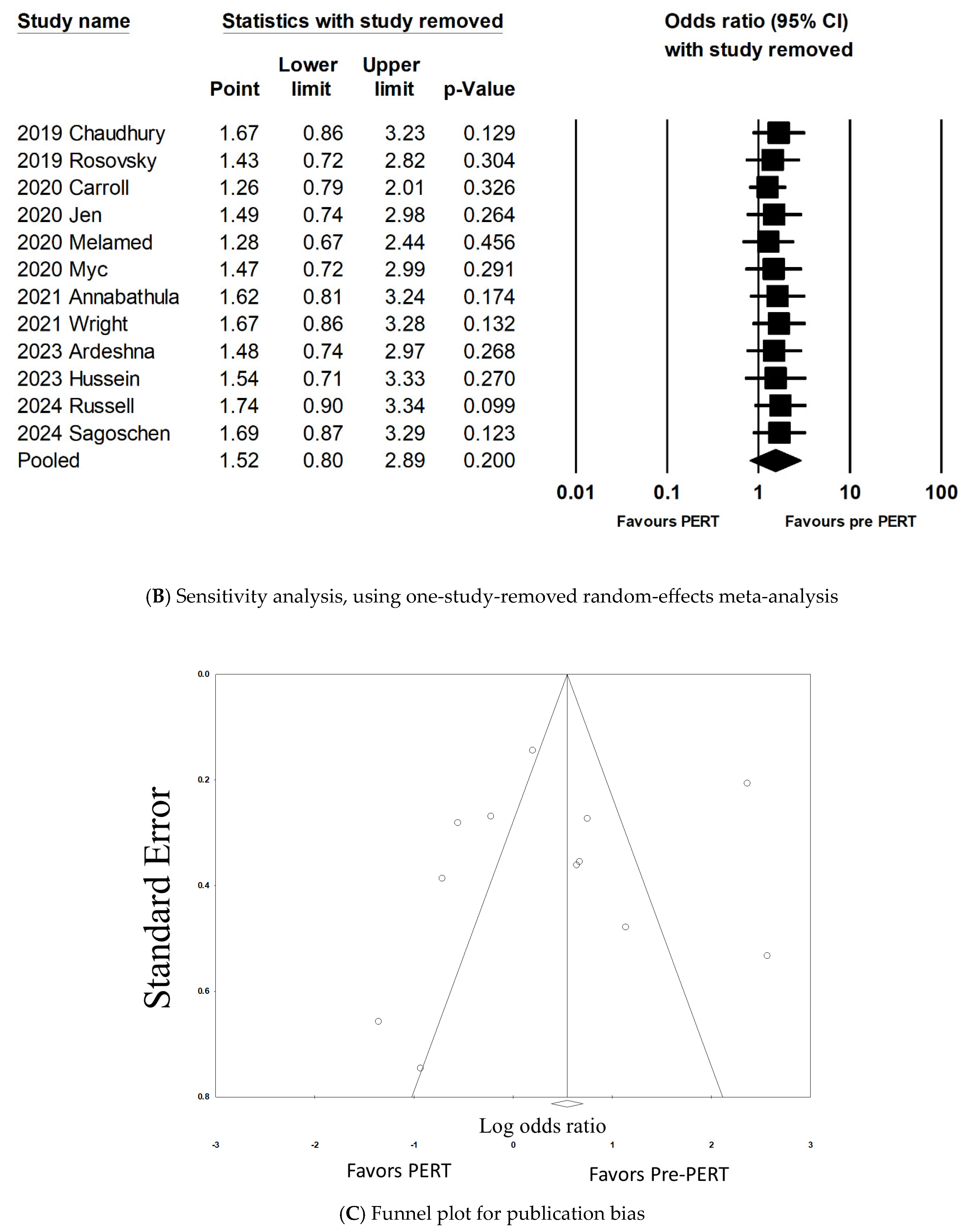
3.3. All-Cause Mortality
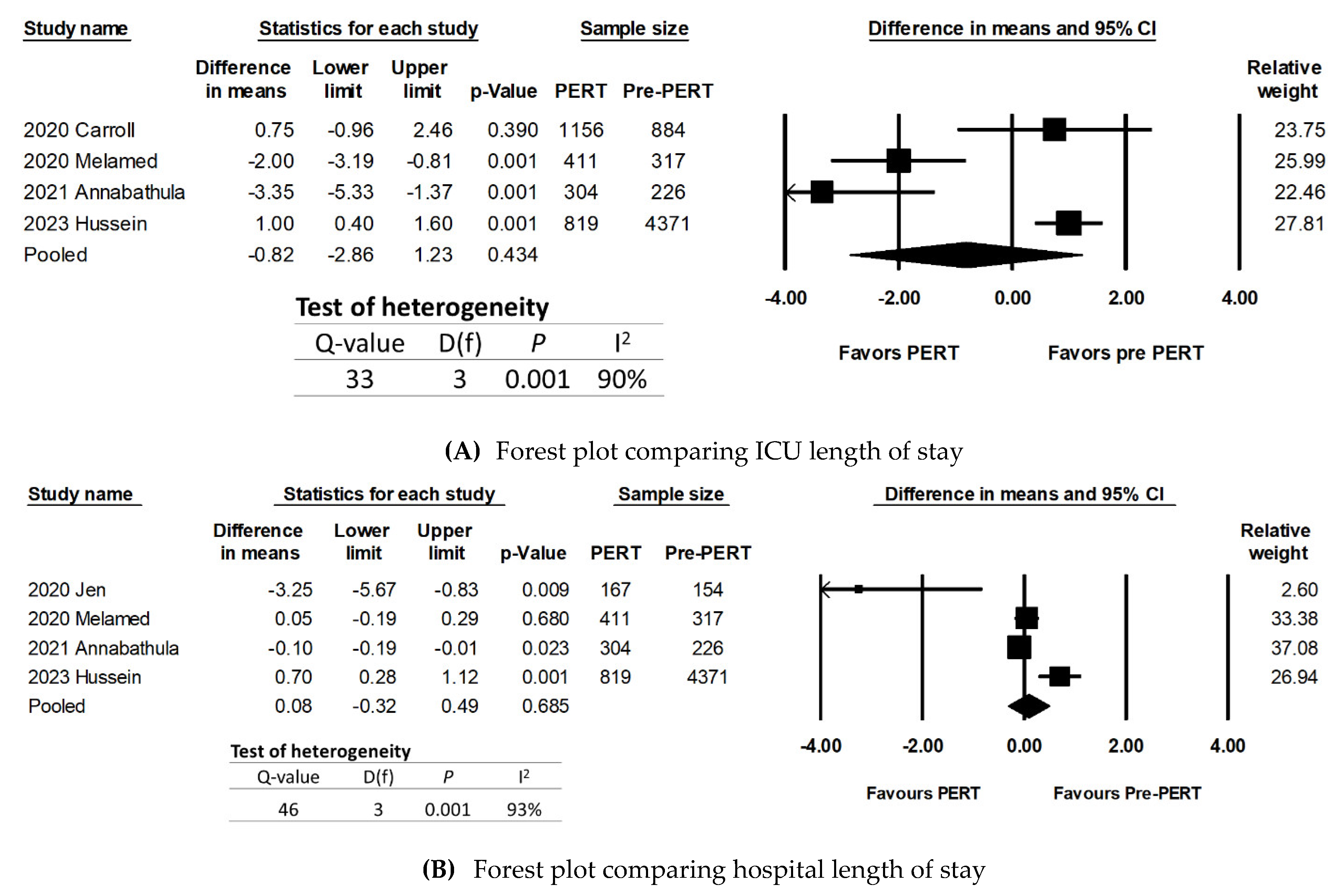
3.4. ICU Length of Stay
3.5. Hospital Length of Stay
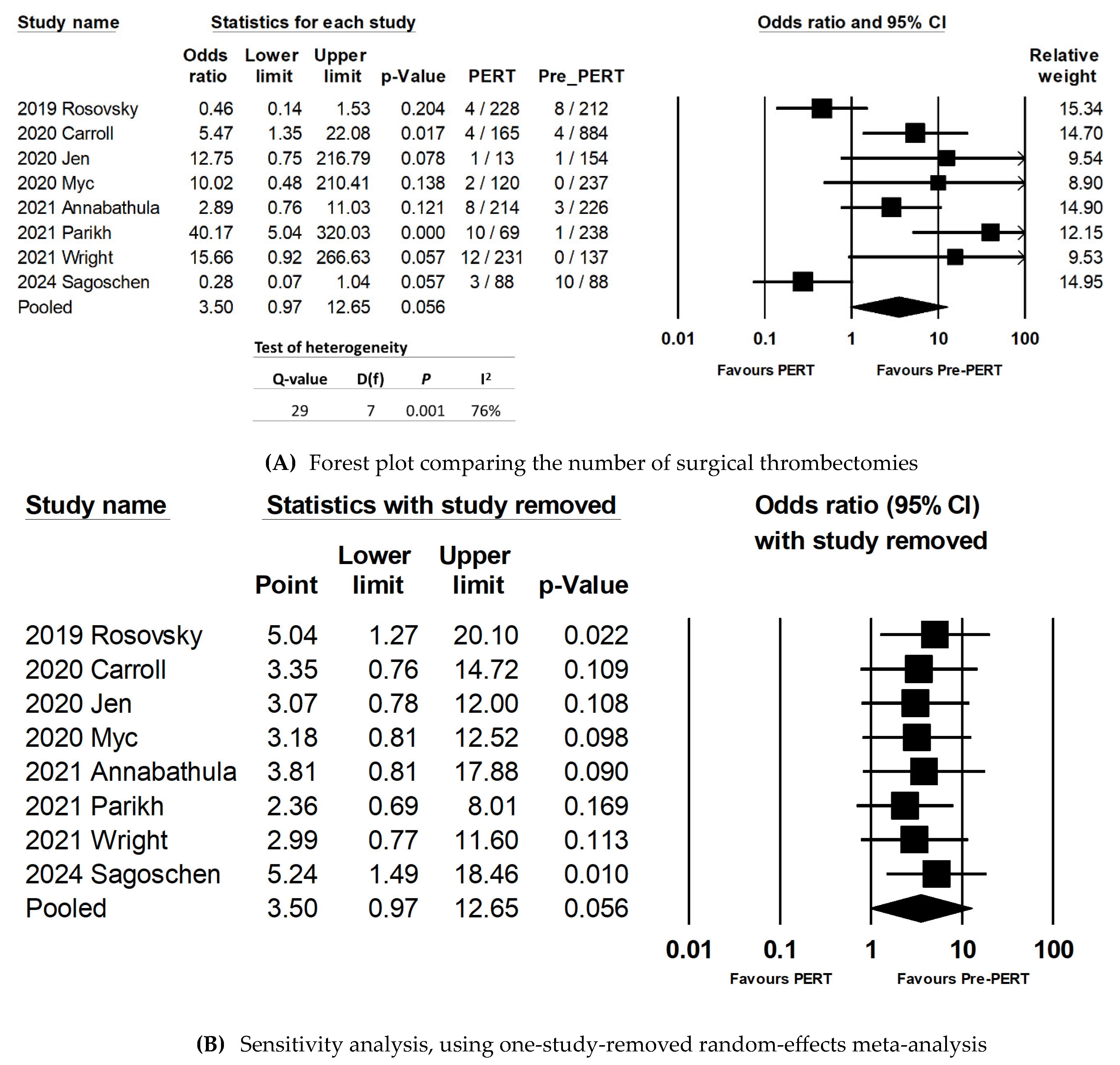
3.6. Rates of Surgical Thrombectomy
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
Appendix A. Search Strategy
Appendix B. Moderator Analyses Subgroups Using Categorical Variables and the Outcome of All-Cause Mortality

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Meta-Analysis | Heterogeneity | ||||||
|---|---|---|---|---|---|---|---|---|
| Number of Studies | Outcome | 95% CI | p | Q-Value | D(f) | p | ||
| Outcome: all-cause mortality | ||||||||
| Study design | Prospective | 1 | 0.49 | 0.23–1.04 | 0.065 | NA | NA | NA |
| Retrospective | 11 | 1.69 | 0.8–3.29 | 0.12 | 135 | 10 | 0.001 | |
| Study settings | ED | 8 | 2.56 | 1.19–5.5 | 0.016 | 110 | 7 | 0.001 |
| ED/Inpatient | 4 | 0.58 | 0.37–0.89 | 0.014 | 3 | 3 | 0.33 | |
| Study sample size | <350 patients | 3 | 0.67 | 0.2–2.13 | 0.5 | 10 | 2 | 0.006 |
| 351–700 patients | 5 | 1.36 | 0.74–2.53 | 0.33 | 19 | 4 | 0.001 | |
| >701 patients | 4 | 3.02 | 0.66–13.8 | 0.15 | 89 | 3 | 0.001 | |
| Outcome: surgical thrombectomy | ||||||||
| Study design | Prospective | 2 | 3.11 | 0.02–410 | 0.65 | 16 | 1 | 0.001 |
| Retrospective | 6 | 3.51 | 1.06–11.6 | 0.04 | 12 | 5 | 0.029 | |
| Study settings | ED | 6 | 6.38 | 1.28–31.6 | 0.023 | 19 | 5 | 0.002 |
| ED/Inpatient | 2 | 0.89 | 0.089–8.90 | 0.921 | 6 | 1 | 0.015 | |
| Study sample size | <350 patients | 3 | 4.7 | 0.14–154 | 0.39 | 18 | 2 | 0.001 |
| 351–700 patients | 4 | 2.6 | 0.52–12.9 | 0.24 | 9 | 3 | 0.033 | |
| >701 patients | 1 | 3.46 | 1.35–22.1 | 0.017 | NA | NA | NA |
References
- CDC. CDC Data and Statistics on Venous Thromboembolism. Available online: https://www.cdc.gov/blood-clots/index.html. (accessed on 7 February 2024).
- Freund, Y.; Cohen-Aubart, F.; Bloom, B. Acute Pulmonary Embolism: A Review. JAMA 2022, 328, 1336–1345. [Google Scholar] [CrossRef]
- Cuomo, J.R.; Arora, V.; Wilkins, T. Management of Acute Pulmonary Embolism with a Pulmonary Embolism Response Team. J. Am. Board Fam. Med. 2021, 34, 402–408. [Google Scholar] [CrossRef] [PubMed]
- Licha, C.R.M.; McCurdy, C.M.; Maldonado, S.M.; Lee, L.S. Current Management of Acute Pulmonary Embolism. Ann. Thorac. Cardiovasc. Surg. 2020, 26, 65–71. [Google Scholar] [CrossRef] [PubMed]
- Ortel, T.L.; Neumann, I.; Ageno, W.; Beyth, R.; Clark, N.P.; Cuker, A.; Hutten, B.A.; Jaff, M.R.; Manja, V.; Schulman, S.; et al. American Society of Hematology 2020 guidelines for management of venous thromboembolism: Treatment of deep vein thrombosis and pulmonary embolism. Blood Adv. 2020, 4, 4693–4738. [Google Scholar] [CrossRef]
- Jaff, M.R.; McMurtry, M.S.; Archer, S.L.; Cushman, M.; Goldenberg, N.; Goldhaber, S.Z.; Jenkins, J.S.; Kline, J.A.; Michaels, A.D.; Thistlethwaite, P.; et al. Management of massive and submassive pulmonary embolism, iliofemoral deep vein thrombosis, and chronic thromboembolic pulmonary hypertension: A scientific statement from the American Heart Association. Circulation 2011, 123, 1788–1830. [Google Scholar] [CrossRef]
- Vedantham, S.; Piazza, G.; Sista, A.K.; Goldenberg, N.A. Guidance for the use of thrombolytic therapy for the treatment of venous thromboembolism. J. Thromb. Thrombolysis 2016, 41, 68–80. [Google Scholar] [CrossRef]
- Rivera-Lebron, B.N.; Rali, P.M.; Tapson, V.F. The PERT Concept: A Step-by-Step Approach to Managing Pulmonary Embolism. Chest 2021, 159, 347–355. [Google Scholar] [CrossRef]
- Provias, T.; Dudzinski, D.M.; Jaff, M.R.; Rosenfield, K.; Channick, R.; Baker, J.; Weinberg, I.; Donaldson, C.; Narayan, R.; Rassi, A.N.; et al. The Massachusetts General Hospital Pulmonary Embolism Response Team (MGH PERT): Creation of a multidisciplinary program to improve care of patients with massive and submassive pulmonary embolism. Hosp. Pract. 2014, 42, 31–37. [Google Scholar] [CrossRef]
- Todoran, T.M.; Giri, J.; Barnes, G.D.; Rosovsky, R.P.; Chang, Y.; Jaff, M.R.; Rosenfield, K.; Kabrhel, C. PERT Consortium Treatment of submassive and massive pulmonary embolism: A clinical practice survey from the second annual meeting of the Pulmonary Embolism Response Team Consortium. J. Thromb. Thrombolysis 2018, 46, 39–49. [Google Scholar] [CrossRef]
- Rosovsky, R.; Zhao, K.; Sista, A.; Rivera-Lebron, B.; Kabrhel, C. Pulmonary embolism response teams: Purpose, evidence for efficacy, and future research directions. Res. Pract. Thromb. Haemost. 2019, 3, 315–330. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Wells, G.A.; Shea, B.; O’Connell, D.; Pereson, J.; Welch, V.; Losos, M.; Tugwell, P. Ottawa Hospital Research Institute. Available online: https://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 8 February 2024).
- Hozo, S.P.; Djulbegovic, B.; Hozo, I. Estimating the mean and variance from the median, range, and the size of a sample. BMC Med. Res. Methodol. 2005, 5, 13. [Google Scholar] [CrossRef] [PubMed]
- Parikh, M.; Chahine, N.M.; Hammad, T.A.; Tefera, L.; Li, J.; Carman, T.; Schilz, R.; Shishehbor, M.H. Predictors and potential advantages of PERT and advanced therapy use in acute pulmonary embolism. Catheter. Cardiovasc. Interv. 2021, 97, 1430–1437. [Google Scholar] [CrossRef] [PubMed]
- Sagoschen, I.; Scibior, B.; Farmakis, I.T.; Keller, K.; Graafen, D.; Griemert, E.-V.; Vosseler, M.; Treede, H.; Münzel, T.; Knorr, M.; et al. A multidisciplinary pulmonary embolism response team (PERT): First experience from a single center in Germany. Clin. Res. Cardiol. 2024, 113, 581–590. [Google Scholar] [CrossRef] [PubMed]
- Chaudhury, P.; Gadre, S.K.; Schneider, E.; Renapurkar, R.D.; Gomes, M.; Haddadin, I.; Heresi, G.A.; Tong, M.Z.; Bartholomew, J.R. Impact of Multidisciplinary Pulmonary Embolism Response Team Availability on Management and Outcomes. Am. J. Cardiol. 2019, 124, 1465–1469. [Google Scholar] [CrossRef]
- Carroll, B.J.; Beyer, S.E.; Mehegan, T.; Dicks, A.; Pribish, A.; Locke, A.; Godishala, A.; Soriano, K.; Kanduri, J.; Sack, K.; et al. Changes in Care for Acute Pulmonary Embolism Through a Multidisciplinary Pulmonary Embolism Response Team. Am. J. Med. 2020, 133, 1313–1321.e6. [Google Scholar] [CrossRef]
- Jen, W.-Y.; Kristanto, W.; Teo, L.; Phua, J.; Yip, H.S.; MacLaren, G.; Teoh, K.; Sim, T.B.; Loh, J.; Ong, C.C.; et al. Assessing the Impact of a Pulmonary Embolism Response Team and Treatment Protocol on Patients Presenting with Acute Pulmonary Embolism. Heart Lung Circ. 2020, 29, 345–353. [Google Scholar] [CrossRef]
- Melamed, R.; St. Hill, C.A.; Engstrom, B.I.; Tierney, D.M.; Smith, C.S.; Agboto, V.K.; Weise, B.E.; Eckman, P.M.; Skeik, N. Effects of a Consensus-Based Pulmonary Embolism Treatment Algorithm and Response Team on Treatment Modality Choices, Outcomes, and Complications. Clin. Appl. Thromb. 2020, 26, 1076029620928420. [Google Scholar] [CrossRef]
- Myc, L.A.; Solanki, J.N.; Barros, A.J.; Nuradin, N.; Nevulis, M.G.; Earasi, K.; Richardson, E.D.; Tsutsui, S.C.; Enfield, K.B.; Teman, N.R.; et al. Adoption of a dedicated multidisciplinary team is associated with improved survival in acute pulmonary embolism. Respir. Res. 2020, 21, 159. [Google Scholar] [CrossRef]
- Annabathula, R.; Dugan, A.; Bhalla, V.; Davis, G.A.; Smyth, S.S.; Gupta, V.A. Value-based assessment of implementing a Pulmonary Embolism Response Team (PERT). J. Thromb. Thrombolysis 2021, 51, 217–225. [Google Scholar] [CrossRef]
- Wright, C.; Goldenberg, I.; Schleede, S.; McNitt, S.; Gosev, I.; Elbadawi, A.; Pietropaoli, A.; Barrus, B.; Chen, Y.L.; Mazzillo, J.; et al. Effect of a Multidisciplinary Pulmonary Embolism Response Team on Patient Mortality. Am. J. Cardiol. 2021, 161, 102–107. [Google Scholar] [CrossRef] [PubMed]
- Ardeshna, N.S.; Song, M.; Hyder, S.N.; Grace, K.A.; O’Hare, C.; Schaeffer, W.J.; Stover, M.; Greineder, C.F.; Barnes, G.D. Effect of pulmonary embolism response team on advanced therapies administered: The University of Michigan experience. Thromb. Res. 2023, 221, 73–78. [Google Scholar] [CrossRef] [PubMed]
- Hussein, E.A.; Semaan, D.B.; Phillips, A.R.; Andraska, E.A.; Rivera-Lebron, B.N.; Chaer, R.A.; Eslami, M.H.; Sridharan, N. Pulmonary embolism response team for hospitalized patients with submassive and massive pulmonary embolism: A single-center experience. J. Vasc. Surg. Venous Lymphat. Disord. 2023, 11, 741–747.e2. [Google Scholar] [CrossRef] [PubMed]
- Russell, N.; Sayfo, S.; George, T.; Gable, D. Effect of a pulmonary embolism response team on the management and outcomes of patients with acute pulmonary embolism. J. Vasc. Surg. 2024, 80, A17. [Google Scholar] [CrossRef]
- Rosovsky, R.; Chang, Y.; Rosenfield, K.; Channick, R.; Jaff, M.R.; Weinberg, I.; Sundt, T.; Witkin, A.; Rodriguez-Lopez, J.; Parry, B.A.; et al. Changes in treatment and outcomes after creation of a pulmonary embolism response team (PERT), a 10-year analysis. J. Thromb. Thrombolysis 2019, 47, 31–40. [Google Scholar] [CrossRef]
| Study (Year, Author) | Total NOS Score | Setting | Number of Patients | No of PERT Activations | Study Type | Mean Age (Pre-PERT/Post-PERT) | % Female (Pre-PERT/Post-PERT) | Mortality (Pre-PERT/Post-PERT) | Thrombolytic (Pre-PERT/Post-PERT) | IVC Filter (Pre-PERT/Post-PERT) | Surgical/Mechanical Thrombectomy (Pre-PERT/Post-PERT) | CDT (Pre-PERT/Post-PERT) | Any Anticoagulation (Pre-PERT/Post-PERT) | DOAC (Pre-PERT/Post-PERT) | ECMO (Pre-PERT/Post-PERT) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 2019, Chaudhury et al. [17] | 8 | ED/inpatient | 769 | 57 | Retrospective Cohort Study | 58.1 | 49.3 | 29 | 4 | 76 | 4 | 1 | 318 | 50 | 0 |
| Pre PERT: 343 | 57.2 | 47.9 | 20 | 14 | 70 | 3 | 6 | 410 | 50 | 2 | |||||
| Post PERT: 426 | |||||||||||||||
| 2019, Rosovsky et al. [11] | 6 | ED | 440 | 228 | Retrospective Cohort Study | 59 | 52 | 6 | 10 | 9 | 10 | ||||
| Pre PERT: 212 | 61 | 47 | 19 | 12 | 4 | 31 | |||||||||
| Post PERT: 228 | |||||||||||||||
| 2020, Carroll et al. [18] | 8 | ED | 2042 | 165 | Retrospective Cohort Study | 62.3 | 52.3 | 60 | 34 | 95 | 4 | 10 | 836 | 6 | 4 |
| Pre PERT: 884 | 63.6 | 53.9 | 72 | 24 | 80 | 4 | 35 | 1088 | 30 | 5 | |||||
| Post PERT: 1158 | |||||||||||||||
| 2020, Jen et al. [19] | 8 | ED | 321 | 167 | Retrospective Cohort Study | 61.1 | 51.9 | 14 | 2 | 1 | 9 | ||||
| Pre PERT: 154 | 60.3 | 51.5 | 23 | 6 | 1 | 4 | 25 | 1 | |||||||
| Post PERT: 167 | |||||||||||||||
| 2020, Melamed et al. [20] | 8 | ED | 728 | 87 | Retrospective Cohort Study | 62.4 | 52.4 | 5 | 8 | 9 | |||||
| Pre PERT: 317 | 62.4 | 47.7 | 15 | 90 | 12 | ||||||||||
| Post PERT: 411 | |||||||||||||||
| 2020, Myc et al. [21] | 7 | ED | 554 | 120 | Retrospective Cohort Study | 62 | 48 | 36 | 0 | 53 | 0 | 7 | 113 | 0 | |
| Pre PERT: 237 | 63.5 | 48.3 | 33 | 5 | 41 | 2 | 26 | 200 | 4 | ||||||
| Post PERT: 317 | |||||||||||||||
| 2021, Annabathula et al. [22] | 8 | ED/inpatient | 530 | 214 | Retrospective Cohort Study | 59.5 | 58.4 | 37 | 10 | 3 | 46 | 221 | 23 | 12 | |
| Pre PERT: 226 | 58.1 | 53 | 29 | 7 | 8 | 55 | 298 | 145 | 12 | ||||||
| Post PERT: | |||||||||||||||
| 2021, Parikh et al. [15] | 9 | ED | 307 | 69 | Prospective Cohort Study | 60.1 | |||||||||
| 2021, Wright et al. [23] | 8 | ED | 368 | 231 | Retrospective Cohort Study | 63.2 | 48 | 33 | 11 | 9 | 0 | 1 | 134 | 1 | |
| Pre PERT: 137 | 63.9 | 46 | 46 | 23 | 14 | 12 | 10 | 227 | 2 | ||||||
| Post PERT: 231 | |||||||||||||||
| 2023, Ardeshna et al. [24] | 8 | ED | 644 | 156 | Retrospective Cohort Study | 58 | 53 | 14.28 | 2 | 9 | 14 | 156 | 5 | ||
| Pre PERT: 168 | 59 | 51 | 24 | 8 | 15 | 10 | 447.44 | 9.52 | |||||||
| Post PERT: 476 | |||||||||||||||
| 2023, Hussein et al. [25] | 8 | ED | 5190 | 819 | Retrospective Cohort Study | 62.6 | 52.6 | ||||||||
| Pre PERT: 4371 | 59.8 | 47 | |||||||||||||
| Post PERT: 819 | |||||||||||||||
| 2024 Russell et al. [26] | 7 | ED/inpatient | 279 | 133 | Retrospective Cohort Study | 63 | 48 | 12 | 7 | ||||||
| Pre PERT: 146 | 61 | 41 | 3 | 6 | 21 | 48 | 132 | ||||||||
| Post PERT: 133 | |||||||||||||||
| 2024 Sagoschen et al. [16] | 8 | ED/inpatient | 176 | 88 | Prospective Cohort Study | 67 | 50 | 23 | 12 | 10 | |||||
| Pre PERT: 88 | 68 | 49 | 13 | 8 | 3 | ||||||||||
| Post PERT: 88 |
| Variables | Number of Studies | Corr. Coeff. (95% CI) | p | R2 | I2 |
|---|---|---|---|---|---|
| PERT age | 12 | 0.04 (−0.15 to 0.23) | 0.72 | 0.2 | 89% |
| PERT number of females | 0.17 (0.004 to 0.34) | 0.045 | |||
| PERT thrombolysis | 10 | 0.03 (−0.0002 to 0.06) | 0.051 | 0.19 | 92% |
| PERT IVC filter | 5 | 0.04 (0.02 to 0.057) | 0.001 | 0.88 | 65% |
| PERT surgical thrombectomy | 7 | 0.01 (−0.04 to 0.07) | 0.66 | 0.23 | 93% |
| PERT catheter-directed thrombolysis | −0.15 (−0.3 to −0.001) | 0.048 | |||
| PERT number of anticoagulations | 6 | 0.003 (0.0027 to 0.0039) | 0.001 | 1 | 0% |
| PERT number of ECMO | 5 | −0.04 (−0.37 to 0.3) | 0.84 | 0 | 96% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bryan, A.; Tran, Q.K.; Ahari, J.; Mclaughlin, E.; Boone, K.; Pourmand, A. Pulmonary Embolism Response Teams—Evidence of Benefits? A Systematic Review and Meta-Analysis. J. Clin. Med. 2024, 13, 7623. https://doi.org/10.3390/jcm13247623
Bryan A, Tran QK, Ahari J, Mclaughlin E, Boone K, Pourmand A. Pulmonary Embolism Response Teams—Evidence of Benefits? A Systematic Review and Meta-Analysis. Journal of Clinical Medicine. 2024; 13(24):7623. https://doi.org/10.3390/jcm13247623
Chicago/Turabian StyleBryan, Amelia, Quincy K. Tran, Jalil Ahari, Erin Mclaughlin, Kirsten Boone, and Ali Pourmand. 2024. "Pulmonary Embolism Response Teams—Evidence of Benefits? A Systematic Review and Meta-Analysis" Journal of Clinical Medicine 13, no. 24: 7623. https://doi.org/10.3390/jcm13247623
APA StyleBryan, A., Tran, Q. K., Ahari, J., Mclaughlin, E., Boone, K., & Pourmand, A. (2024). Pulmonary Embolism Response Teams—Evidence of Benefits? A Systematic Review and Meta-Analysis. Journal of Clinical Medicine, 13(24), 7623. https://doi.org/10.3390/jcm13247623