
Therapeutic Hypothermia and Its Role in Preserving Brain Volume in Term Neonates with Perinatal Asphyxia

 , , , and
, , , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Therapeutic Hypothermia Procedure in Newborns with HIE
2.3. Neurodevelopmental Assessment
2.4. Genetic Analysis
2.5. Brain Volume Analysis
2.6. Statistical Analysis
3. Results
3.1. Descriptive Results
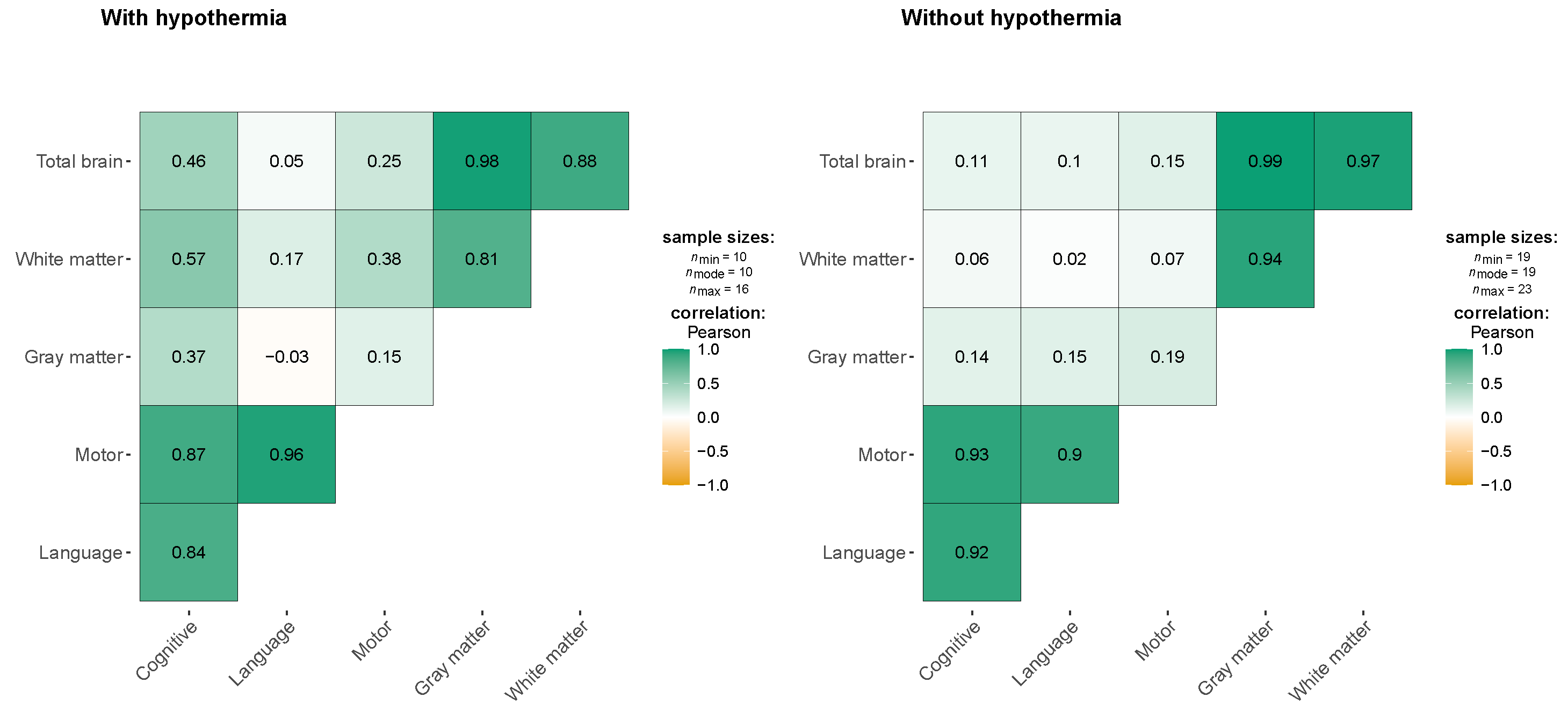
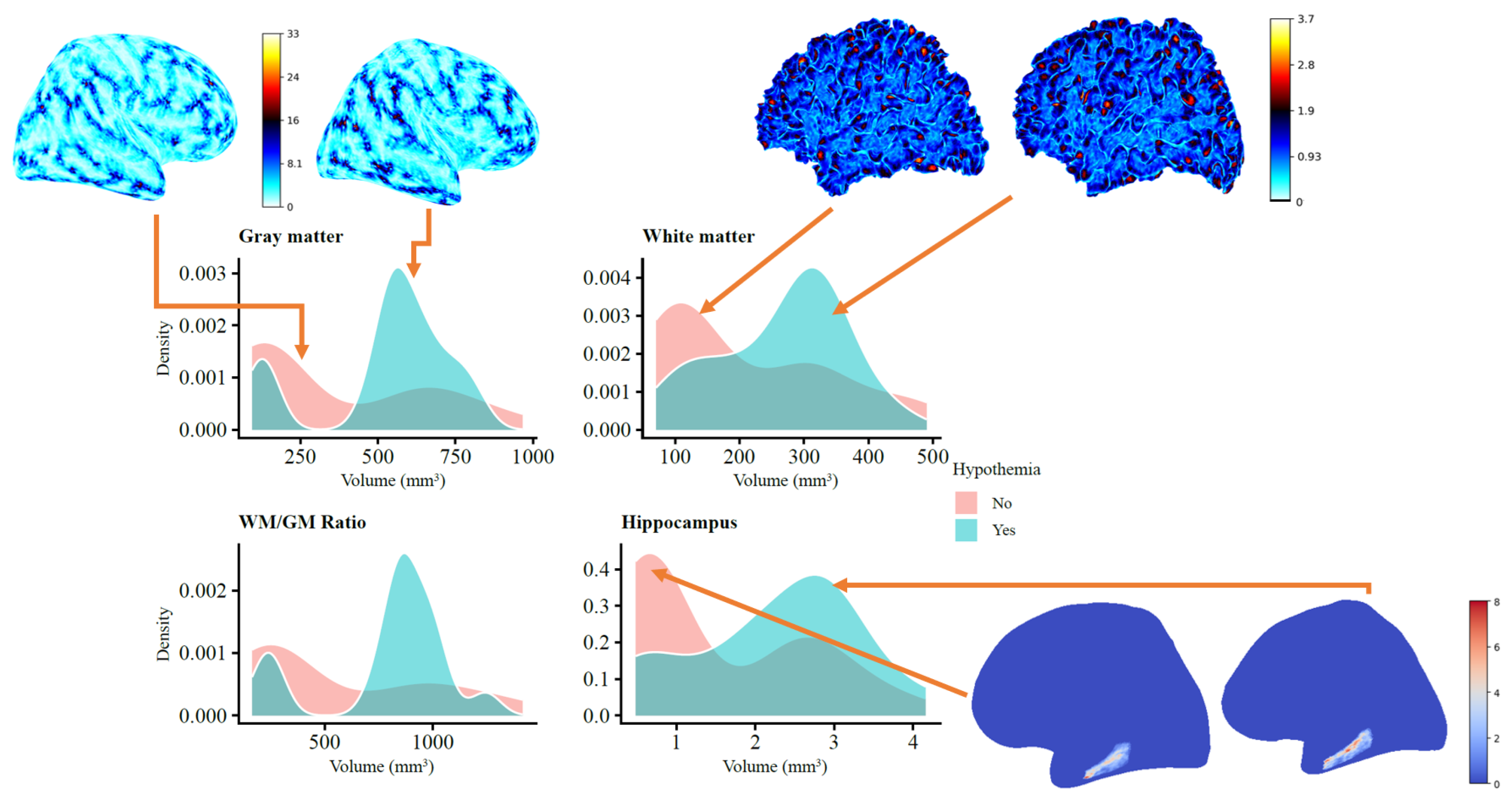
3.2. Hypothermia Effect
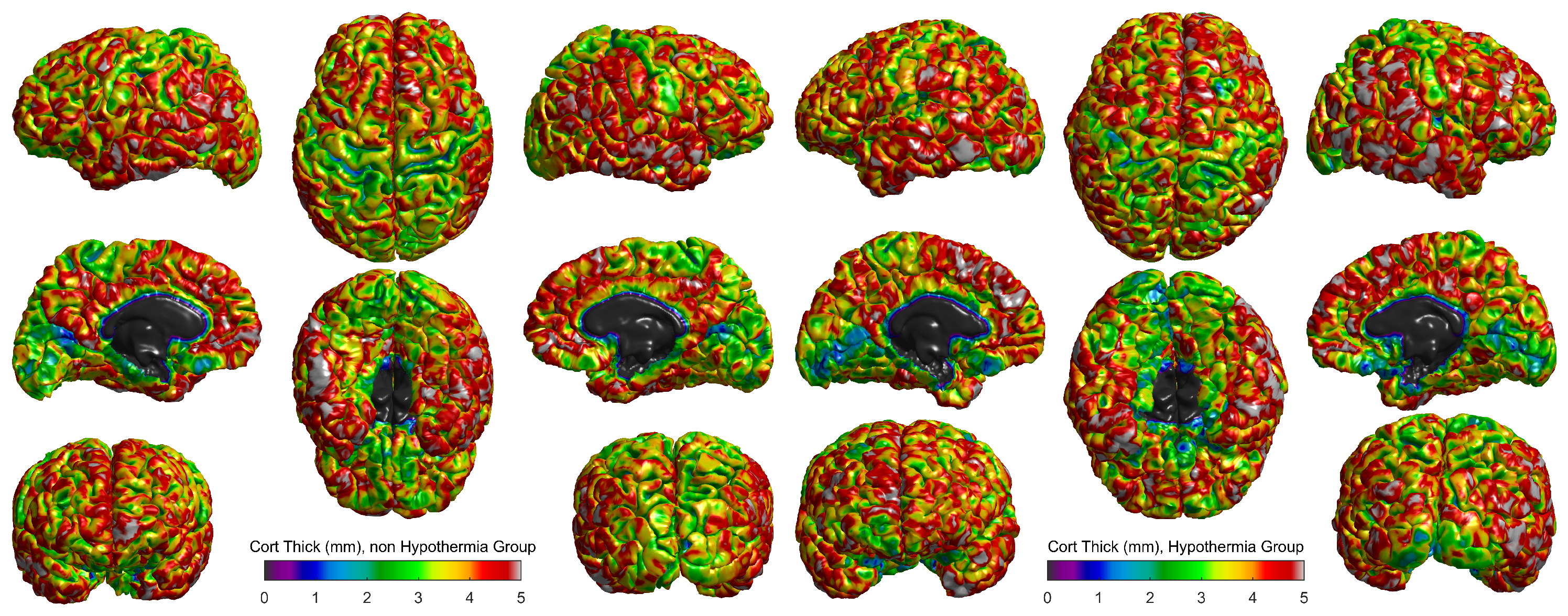
3.3. Cortical Thickness and Structural Differences Between Hypothermia and Non-Hypothermia Groups
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| HIE | hypoxic-ischemic encephalopathy |
| TH | therapeutic hypothermia |
| MRI | magnetic resonance imaging |
| WM | white matter |
| GM | gray matter |
Appendix A

{kind=link}
{kind=link}
{kind=link}
| Characteristic | Hypothermia 1 (Yes, N = 12) | Hypothermia 1 (No, N = 22) | p-Value 2 |
|---|---|---|---|
| Fetal presentation | >0.9 | ||
| Cephalic | 11 (92%) | 20 (91%) | |
| Compound | 0 (0%) | 1 (4.5%) | |
| Breech | 1 (8.3%) | 1 (4.5%) | |
| Birth route | 0.7 | ||
| Cesarean | 4 (33%) | 10 (45%) | |
| Vaginal | 8 (67%) | 12 (55%) | |
| Expulsive | 0.4 | ||
| No | 10 (83%) | 15 (68%) | |
| Yes | 2 (17%) | 7 (32%) | |
| Prolonged labor | >0.9 | ||
| No | 9 (75%) | 15 (68%) | |
| Yes | 3 (25%) | 7 (32%) | |
| Instrumental delivery | 0.2 | ||
| No | 8 (67%) | 20 (91%) | |
| Yes | 4 (33%) | 2 (9.1%) | |
| Urgent cesarean section | 0.7 | ||
| No | 8 (67%) | 13 (59%) | |
| Yes | 4 (33%) | 9 (41%) | |
| Emergent cesarean section | >0.9 | ||
| No | 12 (100%) | 21 (95%) | |
| Yes | 0 (0%) | 1 (4.5%) | |
| Chorioamnionitis | 0.4 | ||
| No | 11 (92%) | 22 (100%) | |
| Yes | 1 (8.3%) | 0 (0%) | |
| Premature rupture of membranes | 0.3 | ||
| No | 12 (100%) | 18 (82%) | |
| Yes | 0 (0%) | 4 (18%) | |
| Oligohydramnios | >0.9 | ||
| No | 11 (92%) | 21 (95%) | |
| Yes | 1 (8.3%) | 1 (4.5%) | |
| Meconium | 0.11 | ||
| No | 11 (92%) | 14 (64%) | |
| Yes | 1 (8.3%) | 8 (36%) | |
| Birth weight (g) | 3100 (2921, 3422) | 3202 (2896, 3404) | 0.8 |
| Height (cm) | 51.00 (49.00, 51.50) | 50.00 (49.00, 52.00) | >0.9 |
| Head circumference (cm) | 34.25 (33.62, 35.00) | 33.00 (32.00, 36.00) | 0.5 |
References
- Lee, A.C.; Kozuki, N.; Blencowe, H.; Vos, T.; Bahalim, A.; Darmstadt, G.L.; Niermeyer, S.; Ellis, M.; Robertson, N.J.; Cousens, S.; et al. Intrapartum-related neonatal encephalopathy incidence and impairment at regional and global levels for 2010 with trends from 1990. Pediatr. Res. 2013, 74, 50–72. [Google Scholar] [CrossRef] [PubMed]
- Shankaran, S. Hypoxic-ischemic encephalopathy and novel strategies for neuroprotection. Clin. Perinatol. 2012, 39, 919–929. [Google Scholar] [CrossRef] [PubMed]
- Lawn, J.E.; Blencowe, H.; Oza, S.; You, D.; Lee, A.C.; Waiswa, P.; Lalli, M.; Bhutta, Z.; Barros, A.J.; Christian, P.; et al. Every Newborn: Progress, priorities, and potential beyond survival. Lancet 2014, 384, 189–205. [Google Scholar] [CrossRef]
- Douglas-Escobar, M.; Weiss, M.D. Hypoxic-ischemic encephalopathy: A review for the clinician. JAMA Pediatr. 2015, 169, 397–403. [Google Scholar] [CrossRef] [PubMed]
- Lacerte, M.; Shapshak, A.H.; Mesfin, F.B. Hypoxic brain injury. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, IL, USA, 2023. [Google Scholar]
- Vannucci, R.C.; Perlman, J.M. Interventions for perinatal hypoxic–ischemic encephalopathy. Pediatrics 1997, 100, 1004–1114. [Google Scholar] [CrossRef] [PubMed]
- Caramelo, I.; Coelho, M.; Rosado, M.; Cardoso, C.M.; Dinis, A.; Duarte, C.B.; Graos, M.; Manadas, B. Biomarkers of hypoxic–ischemic encephalopathy: A systematic review. World J. Pediatr. 2023, 19, 505–548. [Google Scholar] [CrossRef]
- She, H.Q.; Sun, Y.F.; Chen, L.; Xiao, Q.X.; Luo, B.Y.; Zhou, H.S.; Zhou, D.; Chang, Q.Y.; Xiong, L.L. Current analysis of hypoxic-ischemic encephalopathy research issues and future treatment modalities. Front. Neurosci. 2023, 17, 1136500. [Google Scholar] [CrossRef]
- Nanyunja, C.; Sadoo, S.; Mambule, I.; Mathieson, S.R.; Nyirenda, M.; Webb, E.L.; Mugalu, J.; Robertson, N.J.; Nabawanuka, A.; Gilbert, G.; et al. Protocol for the birth asphyxia in African newborns (baby BRAiN) study: A neonatal encephalopathy feasibility cohort study. Gates Open Res. 2022, 6, 6–10. [Google Scholar] [CrossRef]
- Sakr, M.; Shah, M.; Balasundaram, P. Neonatal therapeutic hypothermia. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, IL, USA, 2024. [Google Scholar]
- Finder, M.; Boylan, G.B.; Twomey, D.; Ahearne, C.; Murray, D.M.; Hallberg, B. Two-year neurodevelopmental outcomes after mild hypoxic ischemic encephalopathy in the era of therapeutic hypothermia. JAMA Pediatr. 2020, 174, 48–55. [Google Scholar] [CrossRef]
- Ranjan, A.K.; Gulati, A. Advances in therapies to treat neonatal hypoxic-ischemic encephalopathy. J. Clin. Med. 2023, 12, 6653. [Google Scholar] [CrossRef]
- Malik, I.; Shah, F.A.; Ali, T.; Tan, Z.; Alattar, A.; Ullah, N.; Khan, A.u.; Alshaman, R.; Li, S. Potent natural antioxidant carveol attenuates MCAO-stress induced oxidative, neurodegeneration by regulating the Nrf-2 pathway. Front. Neurosci. 2020, 14, 659. [Google Scholar] [CrossRef] [PubMed]
- Schock, R.B. Re:“Therapeutic Hypothermia for Hypoxic–Ischemic Brain Injury Is More Effective in Newborn Infants Than in Older Patients: Review and Hypotheses” by Whitelaw and Thoresen. Ther. Hypothermia Temp. Manag. 2024, 14, 1. [Google Scholar] [CrossRef] [PubMed]
- Korf, J.M.; McCullough, L.D.; Caretti, V. A narrative review on treatment strategies for neonatal hypoxic ischemic encephalopathy. Transl. Pediatr. 2023, 12, 1552. [Google Scholar] [CrossRef] [PubMed]
- Serrano-Tabares, C.; Uribe-Murillo, A.; Villegas, J.D.; Maya, M.A.; Maya, M.I.; RodrÃguez-Padilla, L.M. Organic Behavior Characterization in Patients with Hypoxic Ischemic Encephalopathy Who Have Received Hypothermia. Open Access J. Neurol. Neurosurg. 2018, 9, 16–23. [Google Scholar]
- Gutierrez, M.; Uribe, A.; Tabares, C. Dismantling a Myth: The Correlation between Ammonium Levels and Severity of Hypoxic-Ischemic Encephalopathy. Could it be an Effect of Hypothermia. J. Neurol Stroke 2015, 3, 00091. [Google Scholar]
- Kurisu, K.; Kim, J.Y.; You, J.; Yenari, M.A. Therapeutic hypothermia and neuroprotection in acute neurological disease. Curr. Med. Chem. 2019, 26, 5430–5455. [Google Scholar] [CrossRef]
- Sun, Y.J.; Zhang, Z.Y.; Fan, B.; Li, G.Y. Neuroprotection by therapeutic hypothermia. Front. Neurosci. 2019, 13, 586. [Google Scholar] [CrossRef]
- Rutherford, M.; Pennock, J.; Schwieso, J.; Cowan, F.; Dubowitz, L. Hypoxic-ischaemic encephalopathy: Early and late magnetic resonance imaging findings in relation to outcome. Arch. Dis. -Child.-Fetal Neonatal Ed. 1996, 75, F145–F151. [Google Scholar] [CrossRef]
- Weeke, L.C.; Groenendaal, F.; Mudigonda, K.; Blennow, M.; Lequin, M.H.; Meiners, L.C.; van Haastert, I.C.; Benders, M.J.; Hallberg, B.; de Vries, L.S. A novel magnetic resonance imaging score predicts neurodevelopmental outcome after perinatal asphyxia and therapeutic hypothermia. J. Pediatr. 2018, 192, 33–40. [Google Scholar] [CrossRef]
- Zöllei, L.; Iglesias, J.E.; Ou, Y.; Grant, P.E.; Fischl, B. Infant FreeSurfer: An automated segmentation and surface extraction pipeline for T1-weighted neuroimaging data of infants 0–2 years. Neuroimage 2020, 218, 116946. [Google Scholar] [CrossRef]
- Chawla, D. Therapeutic hypothermia for neonatal encephalopathy in developing countries: Current evidence. Clin. Epidemiol. Glob. Health 2024, 26, 101507. [Google Scholar] [CrossRef]
- Thayyil, S.; Pant, S.; Montaldo, P.; Shukla, D.; Oliveira, V.; Ivain, P.; Bassett, P.; Swamy, R.; Mendoza, J.; Moreno-Morales, M.; et al. Hypothermia for moderate or severe neonatal encephalopathy in low-income and middle-income countries (HELIX): A randomised controlled trial in India, Sri Lanka, and Bangladesh. Lancet Glob. Health 2021, 9, e1273–e1285. [Google Scholar] [CrossRef] [PubMed]
- Balasundaram, P.; Id, A. Bayley Scales of Infant and Toddler Development; Updated 24 November 2021; StatPearls Publishing: Treasure Island, IL, USA, 2022. [Google Scholar]
- Misser, S.K.; Barkovich, A.J.; Lotz, J.W.; Archary, M. A pictorial review of the pathophysiology and classification of the magnetic resonance imaging patterns of perinatal term hypoxic ischemic brain injury–What the radiologist needs to know…. SA J. Radiol. 2020, 24, 1915. [Google Scholar] [CrossRef] [PubMed]
- Rivero-Arias, O.; Eddama, O.; Azzopardi, D.; Edwards, A.D.; Strohm, B.; Campbell, H. Hypothermia for perinatal asphyxia: Trial-based resource use and costs at 6–7 years. Arch. Dis. -Child.-Fetal Neonatal Ed. 2019, 104, F285–F292. [Google Scholar] [CrossRef]
| Hypothermia | ||||
|---|---|---|---|---|
| Characteristic | Yes, N = 12 1 | No, N = 22 1 | Overall, N = 34 1 | p-Value 2 |
| Sex | ||||
| Female | 0.6 | |||
| Male | ||||
| Gestational age (weeks) | 39.20 (38.8–39.2) | 39.35 (38.0–40.0) | 39.20 (38.2–40.00) | 0.8 |
| Mother’s age (years) | 26.0 (24.0–30.2) | 29.5 (24.5–33.8) | 28.0 (24.0–33.0) | 0.3 |
| Prenatal control | 11 (92%) | 22 (100%) | 33 (97%) | 0.4 |
| Characteristic | Yes, N = 12 | No, N = 22 | Overall, N = 34 | p-Value |
|---|---|---|---|---|
| Pre-eclampsia | 0.5 | |||
| No | 12 (100%) | 19 (86%) | 31 (91%) | |
| Yes | 0 (0%) | 3 (14%) | 3 (8.8%) | |
| Chronic hypertension | ||||
| No | 12 (100%) | 22 (100%) | 34 (100%) | |
| Smoking during pregnancy | >0.9 | |||
| No | 12 (100%) | 21 (95%) | 33 (97%) | |
| Yes | 0 (0%) | 1 (4.5%) | 1 (2.9%) | |
| Previous cesarean section | ||||
| No | 12 (100%) | 22 (100%) | 34 (100%) | |
| Epidural anesthesia | 0.2 | |||
| No | 8 (67%) | 19 (86%) | 27 (79%) | |
| Yes | 4 (33%) | 3 (14%) | 7 (21%) | |
| Intra-uterine growth retardation | ||||
| No | 12 (100%) | 22 (100%) | 34 (100%) | |
| TORCH | ||||
| No | 12 (100%) | 22 (100%) | 34 (100%) | |
| Medication during pregnancy | 0.3 | |||
| No | 10 (83%) | 21 (95%) | 31 (91%) | |
| Yes | 2 (17%) | 1 (4.5%) | 3 (8.8%) | |
| Maternal infections | >0.9 | |||
| No | 12 (100%) | 21 (95%) | 33 (97%) | |
| Yes | 0 (0%) | 1 (4.5%) | 1 (2.9%) | |
| Gestational diabetes | ||||
| No | 12 (100%) | 22 (100%) | 34 (100%) | |
| Primiparity | 0.5 | |||
| No | 7 (58%) | 10 (45%) | 17 (50%) | |
| Yes | 5 (42%) | 12 (55%) | 17 (50%) | |
| Fentanyl use | 0.4 | |||
| No | 11 (92%) | 22 (100%) | 33 (97%) | |
| Yes | 1 (8.3%) | 0 (0%) | 1 (2.9%) | |
| Other | 0.7 | |||
| No | 7 (58%) | 15 (68%) | 22 (65%) | |
| Yes | 5 (42%) | 7 (32%) | 12 (35%) |
| Brain Structure | Coefficient | Std. Error | Effect (Coefficient) | t Value | p Value | AIC |
|---|---|---|---|---|---|---|
| Gray matter | 1.314 | 0.530 | 3.7 | 2.478 | 0.025 | 395.508 |
| White matter | 0.798 | 0.321 | 2.2 | 2.483 | 0.025 | 341.883 |
| WM/GM ratio | 1.086 | 0.443 | 3.0 | 2.452 | 0.026 | 412.594 |
| Left cerebellum | 0.037 | 0.050 | 1.0 | 0.749 | 0.464 | 161.359 |
| Right cerebellum | 0.077 | 0.082 | 1.1 | 0.937 | 0.363 | 188.329 |
| Total cerebellum | 0.061 | 0.075 | 1.1 | 0.819 | 0.425 | 224.077 |
| Caudate | 0.526 | 0.331 | 1.7 | 1.587 | 0.132 | 104.479 |
| Putamen | 0.146 | 0.078 | 1.2 | 1.868 | 0.080 | 40.092 |
| Thalamus | 0.119 | 0.064 | 1.1 | 1.870 | 0.080 | 50.563 |
| Globus pallidus | 0.332 | 0.195 | 1.4 | 1.702 | 0.108 | 15.003 |
| Hippocampus | 1.218 | 0.519 | 3.4 | 2.347 | 0.032 | 90.461 |
| Amygdala | 0.624 | 0.310 | 1.9 | 2.012 | 0.061 | 0.863 |
| Accumbens | 0.384 | 0.214 | 1.5 | 1.792 | 0.092 | −39.749 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
García Arias, H.F.; Porras-Hurtado, G.L.; Estrada-Álvarez, J.M.; Cardona-Ramirez, N.; Restrepo-Restrepo, F.; Serrano, C.; Cárdenas-Peña, D.; Orozco-Gutiérrez, Á.Á. Therapeutic Hypothermia and Its Role in Preserving Brain Volume in Term Neonates with Perinatal Asphyxia. J. Clin. Med. 2024, 13, 7121. https://doi.org/10.3390/jcm13237121
García Arias HF, Porras-Hurtado GL, Estrada-Álvarez JM, Cardona-Ramirez N, Restrepo-Restrepo F, Serrano C, Cárdenas-Peña D, Orozco-Gutiérrez ÁÁ. Therapeutic Hypothermia and Its Role in Preserving Brain Volume in Term Neonates with Perinatal Asphyxia. Journal of Clinical Medicine. 2024; 13(23):7121. https://doi.org/10.3390/jcm13237121
Chicago/Turabian StyleGarcía Arias, Hernán Felipe, Gloria Liliana Porras-Hurtado, Jorge Mario Estrada-Álvarez, Natalia Cardona-Ramirez, Feliza Restrepo-Restrepo, Carolina Serrano, David Cárdenas-Peña, and Álvaro Ángel Orozco-Gutiérrez. 2024. "Therapeutic Hypothermia and Its Role in Preserving Brain Volume in Term Neonates with Perinatal Asphyxia" Journal of Clinical Medicine 13, no. 23: 7121. https://doi.org/10.3390/jcm13237121
APA StyleGarcía Arias, H. F., Porras-Hurtado, G. L., Estrada-Álvarez, J. M., Cardona-Ramirez, N., Restrepo-Restrepo, F., Serrano, C., Cárdenas-Peña, D., & Orozco-Gutiérrez, Á. Á. (2024). Therapeutic Hypothermia and Its Role in Preserving Brain Volume in Term Neonates with Perinatal Asphyxia. Journal of Clinical Medicine, 13(23), 7121. https://doi.org/10.3390/jcm13237121