
Cancer and the 10-Year Incidence of Chronic Low Back Pain in 407,314 Adults Followed in General Practices in Germany

 , , , ,
, , , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Ethics Approval and Consent to Participate
2.2. Guidelines
2.3. Database
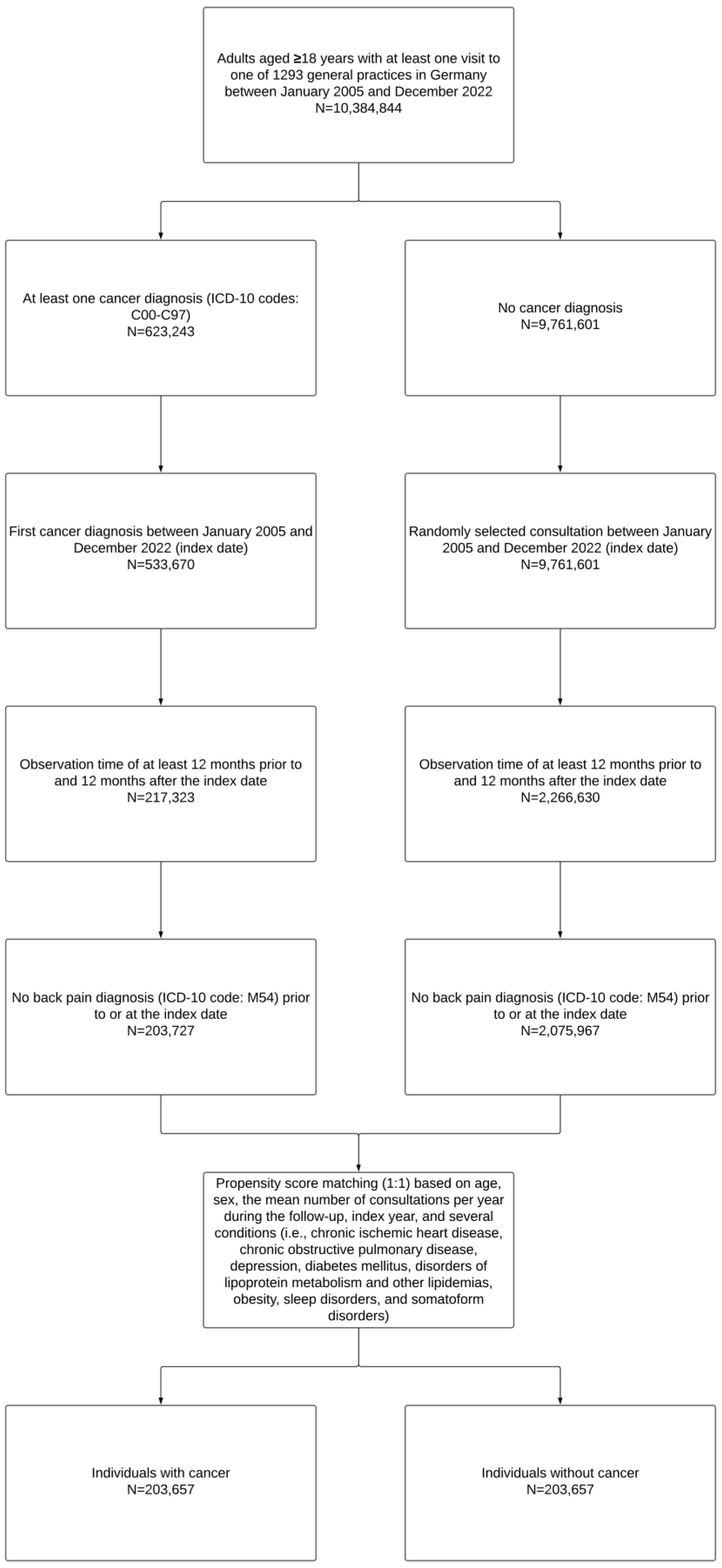
2.4. Study Population
2.5. Study Outcome
2.6. Study Covariates
2.7. Statistical Analyses
3. Results
3.1. Characteristics of the Population
3.2. Cancer and Incident CLBP
4. Discussion
4.1. Main Findings
4.2. Interpretation of the Findings
4.3. Clinical Implications and Directions for Future Research
4.4. Strengths and Limitations
4.5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Paolucci, T.; Attanasi, C.; Cecchini, W.; Marazzi, A.; Capobianco, S.V.; Santilli, V. Chronic Low Back Pain and Postural Rehabilitation Exercise: A Literature Review. J. Pain Res. 2019, 12, 95–107. [Google Scholar] [CrossRef] [PubMed]
- GBD 2021 Low Back Pain Collaborators Global, Regional, and National Burden of Low Back Pain, 1990-2020, Its Attributable Risk Factors, and Projections to 2050: A Systematic Analysis of the Global Burden of Disease Study 2021. Lancet Rheumatol. 2023, 5, e316–e329. [CrossRef] [PubMed]
- Manchikanti, L.; Singh, V.; Falco, F.J.E.; Benyamin, R.M.; Hirsch, J.A. Epidemiology of Low Back Pain in Adults. Neuromodulation 2014, 17 (Suppl. 2), 3–10. [Google Scholar] [CrossRef] [PubMed]
- Heuch, I.; Heuch, I.; Hagen, K.; Sørgjerd, E.P.; Åsvold, B.O.; Zwart, J.-A. Is Chronic Low Back Pain a Risk Factor for Diabetes? The Nord-Trøndelag Health Study. BMJ Open Diabetes Res. Care 2018, 6, e000569. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.-C.; Su, Y.-C.; Luk, H.-N.; Wang, J.-H.; Hsu, C.-Y.; Lin, S.-Z. Increased Risk of Strokes in Patients with Chronic Low Back Pain (CLBP): A Nationwide Population-Based Cohort Study. Clin. Neurol. Neurosurg. 2020, 192, 105725. [Google Scholar] [CrossRef]
- Husky, M.M.; Ferdous Farin, F.; Compagnone, P.; Fermanian, C.; Kovess-Masfety, V. Chronic Back Pain and Its Association with Quality of Life in a Large French Population Survey. Health Qual. Life Outcomes 2018, 16, 195. [Google Scholar] [CrossRef]
- Roseen, E.J.; LaValley, M.P.; Li, S.; Saper, R.B.; Felson, D.T.; Fredman, L. Study of Osteoporotic Fractures Association of Back Pain with All-Cause and Cause-Specific Mortality Among Older Women: A Cohort Study. J. Gen. Intern. Med. 2019, 34, 90–97. [Google Scholar] [CrossRef]
- Natvig, B.; Eriksen, W.; Bruusgaard, D. Low Back Pain as a Predictor of Long-Term Work Disability. Scand J. Public Health 2002, 30, 288–292. [Google Scholar] [CrossRef]
- Montgomery, W.; Sato, M.; Nagasaka, Y.; Vietri, J. The Economic and Humanistic Costs of Chronic Lower Back Pain in Japan. Clinicoecon. Outcomes Res. 2017, 9, 361–371. [Google Scholar] [CrossRef]
- Green, C.R.; Hart-Johnson, T.; Loeffler, D.R. Cancer-Related Chronic Pain: Examining Quality of Life in Diverse Cancer Survivors. Cancer 2011, 117, 1994–2003. [Google Scholar] [CrossRef]
- Vistad, I.; Cvancarova, M.; Kristensen, G.B.; Fosså, S.D. A Study of Chronic Pelvic Pain after Radiotherapy in Survivors of Locally Advanced Cervical Cancer. J. Cancer Surviv. 2011, 5, 208–216. [Google Scholar] [CrossRef] [PubMed]
- Schou Bredal, I.; Smeby, N.A.; Ottesen, S.; Warncke, T.; Schlichting, E. Chronic Pain in Breast Cancer Survivors: Comparison of Psychosocial, Surgical, and Medical Characteristics between Survivors with and without Pain. J. Pain Symptom. Manage 2014, 48, 852–862. [Google Scholar] [CrossRef] [PubMed]
- Jiang, C.; Wang, H.; Wang, Q.; Luo, Y.; Sidlow, R.; Han, X. Prevalence of Chronic Pain and High-Impact Chronic Pain in Cancer Survivors in the United States. JAMA Oncol. 2019, 5, 1224–1226. [Google Scholar] [CrossRef] [PubMed]
- Sanford, N.N.; Sher, D.J.; Butler, S.S.; Xu, X.; Ahn, C.; Aizer, A.A.; Mahal, B.A. Prevalence of Chronic Pain among Cancer Survivors in the United States, 2010–2017. Cancer 2019, 125, 4310–4318. [Google Scholar] [CrossRef] [PubMed]
- Cox-Martin, E.; Anderson-Mellies, A.; Borges, V.; Bradley, C. Chronic Pain, Health-Related Quality of Life, and Employment in Working-Age Cancer Survivors. J. Cancer Surviv. 2020, 14, 179–187. [Google Scholar] [CrossRef]
- Poço Gonçalves, J.; Veiga, D.; Araújo, A. Chronic Pain, Functionality and Quality of Life in Cancer Survivors. Br. J. Pain 2021, 15, 401–410. [Google Scholar] [CrossRef]
- Yin, M.; Wang, C.; Gu, K.; Bao, P.; Shu, X.-O. Chronic Pain and Its Correlates among Long-Term Breast Cancer Survivors. J. Cancer Surviv. 2023, 17, 460–467. [Google Scholar] [CrossRef]
- Burton, A.W.; Fanciullo, G.J.; Beasley, R.D.; Fisch, M.J. Chronic Pain in the Cancer Survivor: A New Frontier. Pain Med. 2007, 8, 189–198. [Google Scholar] [CrossRef]
- Neil, S.E.; Gotay, C.C.; Campbell, K.L. Physical Activity Levels of Cancer Survivors in Canada: Findings from the Canadian Community Health Survey. J. Cancer Surviv. 2014, 8, 143–149. [Google Scholar] [CrossRef]
- Alzahrani, H.; Mackey, M.; Stamatakis, E.; Zadro, J.R.; Shirley, D. The Association between Physical Activity and Low Back Pain: A Systematic Review and Meta-Analysis of Observational Studies. Sci. Rep. 2019, 9, 8244. [Google Scholar] [CrossRef]
- Jacob, L.; Rathmann, W.; Koyanagi, A.; Haro, J.M.; Kostev, K. Association between Type 2 Diabetes and Chronic Low Back Pain in General Practices in Germany. BMJ Open Diabetes Res. Care 2021, 9, e002426. [Google Scholar] [CrossRef] [PubMed]
- Yang, K.; Liu, Z.; Thong, M.S.Y.; Doege, D.; Arndt, V. Higher Incidence of Diabetes in Cancer Patients Compared to Cancer-Free Population Controls: A Systematic Review and Meta-Analysis. Cancers 2022, 14, 1808. [Google Scholar] [CrossRef]
- Greenlee, H.; Shi, Z.; Sardo Molmenti, C.L.; Rundle, A.; Tsai, W.Y. Trends in Obesity Prevalence in Adults With a History of Cancer: Results From the US National Health Interview Survey, 1997 to 2014. J. Clin. Oncol. 2016, 34, 3133–3140. [Google Scholar] [CrossRef] [PubMed]
- Zhang, T.-T.; Liu, Z.; Liu, Y.-L.; Zhao, J.-J.; Liu, D.-W.; Tian, Q.-B. Obesity as a Risk Factor for Low Back Pain: A Meta-Analysis. Clin. Spine Surg. 2018, 31, 22–27. [Google Scholar] [CrossRef]
- Croft, P.R.; Papageorgiou, A.C.; Ferry, S.; Thomas, E.; Jayson, M.I.; Silman, A.J. Psychologic Distress and Low Back Pain. Evidence from a Prospective Study in the General Population. Spine 1995, 20, 2731–2737. [Google Scholar] [CrossRef]
- Deimling, G.T.; Kahana, B.; Bowman, K.F.; Schaefer, M.L. Cancer Survivorship and Psychological Distress in Later Life. Psychooncology 2002, 11, 479–494. [Google Scholar] [CrossRef] [PubMed]
- Rathmann, W.; Bongaerts, B.; Carius, H.-J.; Kruppert, S.; Kostev, K. Basic Characteristics and Representativeness of the German Disease Analyzer Database. Int. J. Clin. Pharmacol. Ther. 2018, 56, 459–466. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.; Kim, H.J.; Lonjon, G.; Zhu, Y. Written on behalf of AME Big-Data Clinical Trial Collaborative Group Balance Diagnostics after Propensity Score Matching. Ann. Transl. Med. 2019, 7, 16. [Google Scholar] [CrossRef] [PubMed]
- Garbe, C.; Forsea, A.-M.; Amaral, T.; Arenberger, P.; Autier, P.; Berwick, M.; Boonen, B.; Bylaite, M.; Del Marmol, V.; Dreno, B.; et al. Skin Cancers Are the Most Frequent Cancers in Fair-Skinned Populations, but We Can Prevent Them. Eur. J. Cancer 2024, 204, 114074. [Google Scholar] [CrossRef]
- Wehner, M.R.; Cidre Serrano, W.; Nosrati, A.; Schoen, P.M.; Chren, M.-M.; Boscardin, J.; Linos, E. All-Cause Mortality in Patients with Basal and Squamous Cell Carcinoma: A Systematic Review and Meta-Analysis. J. Am. Acad. Dermatol. 2018, 78, 663–672.e3. [Google Scholar] [CrossRef]
- Siegel, R.L.; Giaquinto, A.N.; Jemal, A. Cancer Statistics, 2024. CA Cancer J. Clin. 2024, 74, 12–49. [Google Scholar] [CrossRef] [PubMed]
- Cortés-Ibáñez, F.O.; Jaramillo-Calle, D.A.; Vinke, P.C.; Byambasukh, O.; Corpeleijn, E.; Sijtsma, A.; Eulenburg, C.; Vonk, J.M.; de Bock, G.H. Comparison of Health Behaviours between Cancer Survivors and the General Population: A Cross-Sectional Analysis of the Lifelines Cohort. J. Cancer Surviv. 2020, 14, 377–385. [Google Scholar] [CrossRef] [PubMed]
- Blanchard, C.M.; Denniston, M.M.; Baker, F.; Ainsworth, S.R.; Courneya, K.S.; Hann, D.M.; Gesme, D.H.; Reding, D.; Flynn, T.; Kennedy, J.S. Do Adults Change Their Lifestyle Behaviors after a Cancer Diagnosis? Am. J. Health Behav. 2003, 27, 246–256. [Google Scholar] [CrossRef] [PubMed]
- Xu, H.-R.; Zhang, Y.-H.; Ngo, T.L.; Yang, Q.-H.; Du, S.-H.; Wang, X.-Q. Association between Smoking and Incident Back Pain: A Prospective Cohort Study with 438 510 Participants. J. Glob. Health 2023, 13, 04152. [Google Scholar] [CrossRef]
- Khan, N.F.; Watson, E.; Rose, P.W. Primary Care Consultation Behaviours of Long-Term, Adult Survivors of Cancer in the UK. Br. J. Gen. Pract. 2011, 61, 197–199. [Google Scholar] [CrossRef]
- Fidjeland, H.L.; Vistad, I.; Gjelstad, S.; Brekke, M. Exploring Why Patients with Cancer Consult GPs: A 1-Year Data Extraction. BJGP Open 2019, 3, bjgpopen19X101663. [Google Scholar] [CrossRef]
- Nieminen, L.K.; Pyysalo, L.M.; Kankaanpää, M.J. Prognostic Factors for Pain Chronicity in Low Back Pain: A Systematic Review. Pain Rep. 2021, 6, e919. [Google Scholar] [CrossRef]
- Fredheim, O.M.; Skurtveit, S.; Handal, M.; Hjellvik, V. A Complete National Cohort Study of Prescriptions of Analgesics and Benzodiazepines to Cancer Survivors in Norway 10 Years after Diagnosis. Pain 2019, 160, 852–859. [Google Scholar] [CrossRef]
- Zhang, F.-M.; Song, C.-H.; Guo, Z.-Q.; Yu, Z.; Weng, M.; Zhou, F.-X.; Liu, M.; Cong, M.-H.; Li, T.; Li, Z.-N.; et al. Sarcopenia Prevalence in Patients with Cancer and Association with Adverse Prognosis: A Nationwide Survey on Common Cancers. Nutrition 2023, 114, 112107. [Google Scholar] [CrossRef]
- Iwahashi, S.; Hashida, R.; Matsuse, H.; Higashi, E.; Bekki, M.; Iwanaga, S.; Hara, K.; Higuchi, T.; Hirakawa, Y.; Kubota, A.; et al. The Impact of Sarcopenia on Low Back Pain and Quality of Life in Patients with Osteoporosis. BMC Musculoskelet. Disord. 2022, 23, 142. [Google Scholar] [CrossRef]
- Caetano Dos Santos, F.L.; Wojciechowska, U.; Michalek, I.M.; Didkowska, J. Survival of Patients with Cancers of the Female Genital Organs in Poland, 2000-2019. Sci. Rep. 2023, 13, 8473. [Google Scholar] [CrossRef] [PubMed]
- Bi, J.-H.; Tuo, J.-Y.; Xiao, Y.-X.; Tang, D.-D.; Zhou, X.-H.; Jiang, Y.-F.; Ji, X.-W.; Tan, Y.-T.; Yuan, H.-Y.; Xiang, Y.-B. Observed and Relative Survival Trends of Lung Cancer: A Systematic Review of Population-Based Cancer Registration Data. Thorac. Cancer 2024, 15, 142–151. [Google Scholar] [CrossRef] [PubMed]
- Steffens, D.; Maher, C.G.; Pereira, L.S.M.; Stevens, M.L.; Oliveira, V.C.; Chapple, M.; Teixeira-Salmela, L.F.; Hancock, M.J. Prevention of Low Back Pain: A Systematic Review and Meta-Analysis. JAMA Intern. Med. 2016, 176, 199–208. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Cai, D.; Hong, S. Prevalence and Prognosis of Bone Metastases in Common Solid Cancers at Initial Diagnosis: A Population-Based Study. BMJ Open 2023, 13, e069908. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Variable | People with Cancer (n = 203,657) | People Without Cancer (n = 203,657) | Standardized Mean Difference a |
|---|---|---|---|
| Age (in years) | |||
| Mean (standard deviation) | 66.2 (14.6) | 66.0 (13.8) | −0.014 |
| ≤50 | 27,501 (13.5) | 29,129 (14.3) | |
| 51–60 | 37,039 (18.2) | 36,890 (18.1) | |
| 61–70 | 52,377 (25.7) | 48,739 (23.9) | |
| 71–80 | 58,582 (28.8) | 55,229 (27.1) | |
| >80 | 28,158 (13.8) | 33,670 (16.5) | |
| Sex | |||
| Female | 104,509 (51.3) | 105,431 (51.8) | −0.005 |
| Male | 99,148 (48.7) | 98,226 (48.2) | |
| Consultations per year during the follow-up, mean (standard deviation) | 8.7 (3.8) | 8.8 (3.8) | −0.026 |
| Index year | |||
| 2005–2007 | 13,463 (6.6) | 14,437 (7.1) | −0.047 |
| 2008–2010 | 22,718 (11.2) | 20,232 (9.9) | |
| 2011–2013 | 33,299 (16.4) | 30,136 (14.8) | |
| 2014–2016 | 41,611 (20.4) | 40,529 (19.9) | |
| 2017–2019 | 49,816 (24.5) | 52,109 (25.6) | |
| 2020–2022 | 42,750 (21.0) | 46,214 (22.7) | |
| Chronic conditions | |||
| Chronic ischemic heart disease | 30,330 (14.9) | 29,863 (14.7) | −0.002 |
| Chronic obstructive pulmonary disease | 19,206 (9.4) | 18,921 (9.3) | −0.001 |
| Depression | 32,252 (15.8) | 32,422 (15.9) | 0.001 |
| Diabetes mellitus | 43,060 (21.1) | 43,934 (21.6) | 0.004 |
| Disorders of lipoprotein metabolism and other lipidemias | 58,974 (29.0) | 59,035 (29.0) | 0.000 |
| Obesity | 17,842 (8.8) | 17,537 (8.6) | −0.001 |
| Sleep disorders | 22,946 (11.3) | 22,493 (11.0) | −0.002 |
| Somatoform disorders | 19,376 (9.5) | 18,943 (9.3) | −0.002 |
| Variable | People with Cancer (n = 203,657) | People Without Cancer (n = 203,657) | p-Value a |
|---|---|---|---|
| Atrial fibrillation and flutter | 16,767 (8.2) | 17,128 (8.4) | 0.041 |
| Disorders of the thyroid gland | 44,290 (21.7) | 43,434 (21.3) | 0.001 |
| Essential hypertension | 96,458 (47.4) | 99,908 (49.1) | <0.001 |
| Gastritis and duodenitis | 31,304 (15.4) | 31,935 (15.7) | 0.006 |
| Gastro-esophageal reflux disease | 26,824 (13.2) | 25,736 (12.6) | <0.001 |
| Heart failure | 16,103 (7.9) | 16,317 (8.0) | 0.215 |
| Osteoarthritis of the knee | 22,464 (11.0) | 21,398 (10.5) | <0.001 |
| Varicose veins of the lower extremities | 17,649 (8.7) | 17,062 (8.4) | 0.001 |
| Variable | Patients with Cancer (n = 203,657) |
|---|---|
| Breast cancer | 29,969 (14.7) |
| Cancer of bronchus and lung | 8360 (4.1) |
| Cancer of esophagus or stomach | 4291 (2.1) |
| Cancer of female genital organs | 9114 (4.5) |
| Colorectal cancer | 17,536 (8.6) |
| Malignant neoplasms of ill-defined, other secondary, and unspecified sites | 14,544 (7.1) |
| Malignant neoplasms of lymphoid, hematopoietic, and related tissue | 15,411 (7.6) |
| Prostate cancer | 23,082 (11.3) |
| Skin cancer | 45,409 (22.3) |
| Urinary tract cancer | 13,882 (6.8) |
| Cancer of other sites | 22,059 (10.8) |
| Population | Hazard Ratio (95% Confidence Interval) | p-Value |
|---|---|---|
| Overall population | 0.87 (0.86–0.89) | <0.001 |
| By age (in years) | ||
| ≤50 | 0.87 (0.83–0.92) | <0.001 |
| 51–60 | 0.78 (0.75–0.82) | <0.001 |
| 61–70 | 0.83 (0.80–0.87) | <0.001 |
| 71–80 | 0.98 (0.94–1.02) | 0.313 |
| >80 | 1.12 (1.04–1.19) | 0.001 |
| By sex | ||
| Female | 0.88 (0.86–0.91) | <0.001 |
| Male | 0.86 (0.84–0.89) | <0.001 |
| By cancer diagnosis | ||
| Breast cancer | 0.76 (0.72–0.80) | <0.001 |
| Cancer of bronchus and lung | 1.01 (0.92–1.12) | 0.799 |
| Cancer of esophagus or stomach | 0.86 (0.75–0.99) | 0.039 |
| Cancer of female genital organs | 1.07 (0.97–1.18) | 0.165 |
| Colorectal cancer | 0.83 (0.77–0.89) | <0.001 |
| Malignant neoplasms of ill-defined, other secondary, and unspecified sites | 0.96 (0.89–1.04) | 0.329 |
| Malignant neoplasms of lymphoid, hematopoietic, and related tissue | 0.88 (0.81–0.95) | <0.001 |
| Prostate cancer | 0.80 (0.75–0.86) | <0.001 |
| Skin cancer | 0.94 (0.90–0.98) | 0.004 |
| Urinary tract cancer | 0.90 (0.83–0.97) | 0.008 |
| Cancer of other sites | 0.86 (0.81–0.91) | <0.001 |
| By metastasis | ||
| Absence of metastasis | 0.88 (0.86–0.90) | <0.001 |
| Presence of metastasis | 1.04 (0.93–1.15) | 0.510 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kostev, K.; Latourte, A.; Yon, D.K.; Haro, J.M.; Richette, P.; Beaudreuil, J.; Jacob, L. Cancer and the 10-Year Incidence of Chronic Low Back Pain in 407,314 Adults Followed in General Practices in Germany. J. Clin. Med. 2024, 13, 6969. https://doi.org/10.3390/jcm13226969
Kostev K, Latourte A, Yon DK, Haro JM, Richette P, Beaudreuil J, Jacob L. Cancer and the 10-Year Incidence of Chronic Low Back Pain in 407,314 Adults Followed in General Practices in Germany. Journal of Clinical Medicine. 2024; 13(22):6969. https://doi.org/10.3390/jcm13226969
Chicago/Turabian StyleKostev, Karel, Augustin Latourte, Dong Keon Yon, Josep Maria Haro, Pascal Richette, Johann Beaudreuil, and Louis Jacob. 2024. "Cancer and the 10-Year Incidence of Chronic Low Back Pain in 407,314 Adults Followed in General Practices in Germany" Journal of Clinical Medicine 13, no. 22: 6969. https://doi.org/10.3390/jcm13226969
APA StyleKostev, K., Latourte, A., Yon, D. K., Haro, J. M., Richette, P., Beaudreuil, J., & Jacob, L. (2024). Cancer and the 10-Year Incidence of Chronic Low Back Pain in 407,314 Adults Followed in General Practices in Germany. Journal of Clinical Medicine, 13(22), 6969. https://doi.org/10.3390/jcm13226969