
Safety and Efficacy of Atogepant for the Preventive Treatment of Migraines in Adults: A Systematic Review and Meta-Analysis

 ,
,
Abstract
1. Introduction
2. Methods
2.1. Search Strategy
2.2. Eligibility Criteria
2.3. Outcome Measures
2.4. Study Selection, Data Extraction, and Quality Assessment
2.5. Statistical Analysis
3. Results
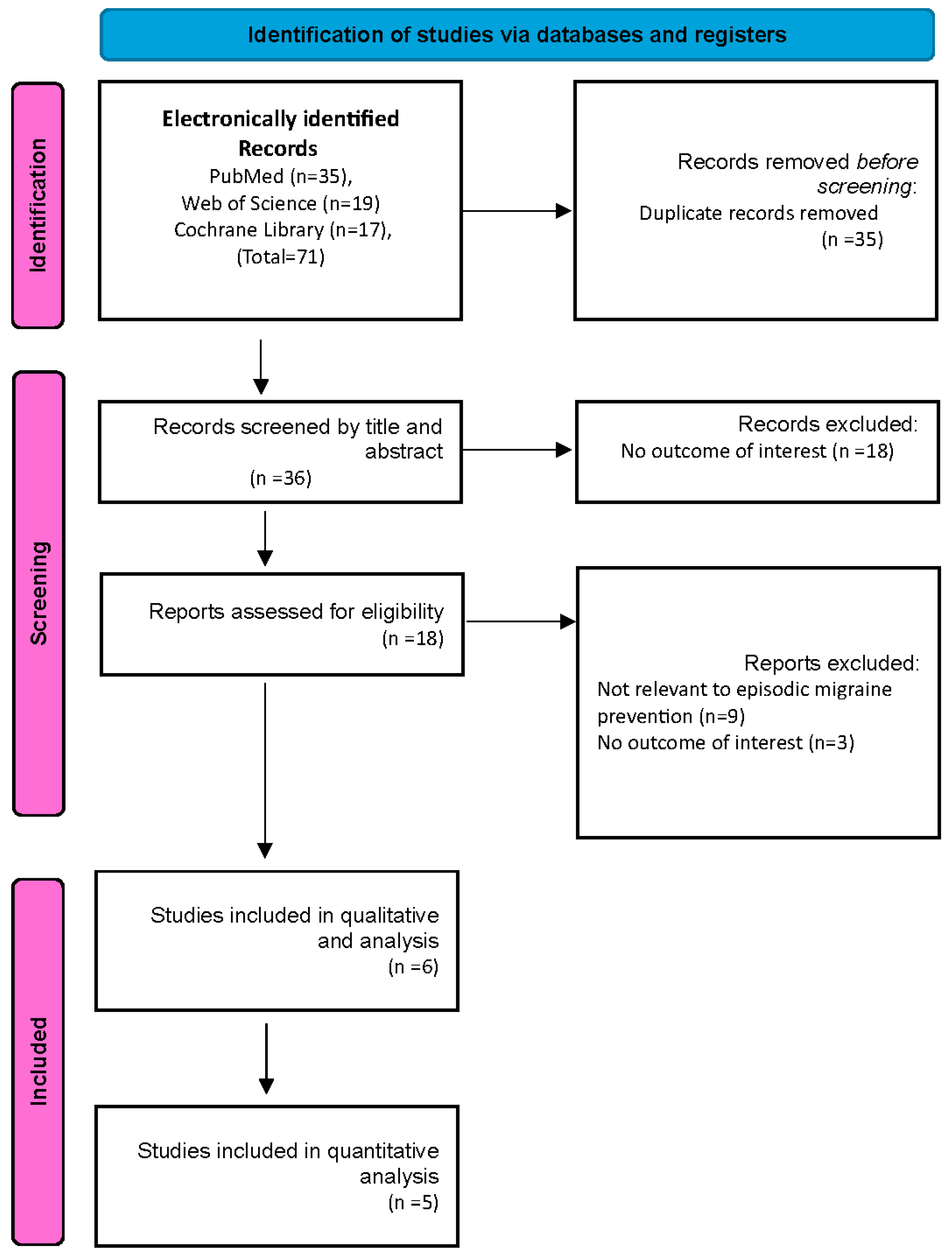
3.1. Search Results
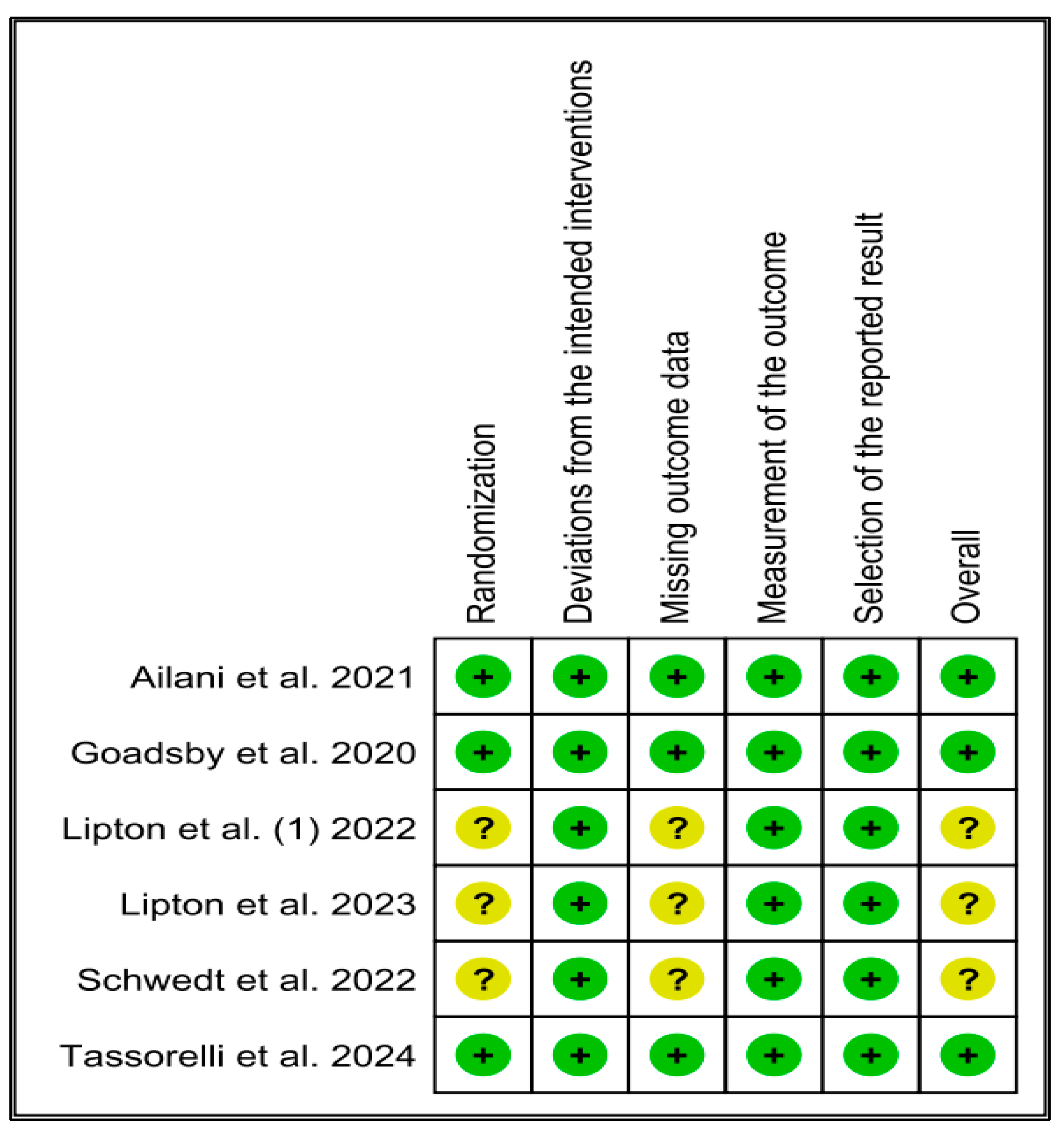
3.2. Quality Assessment
3.3. Characteristics of the Included Studies
3.4. Meta-Analysis
3.5. Mean Monthly Migraine Days Change from Baseline
3.6. Mean Monthly Headache Days Change from Baseline
3.7. Acute Medication Use Days Change from Baseline
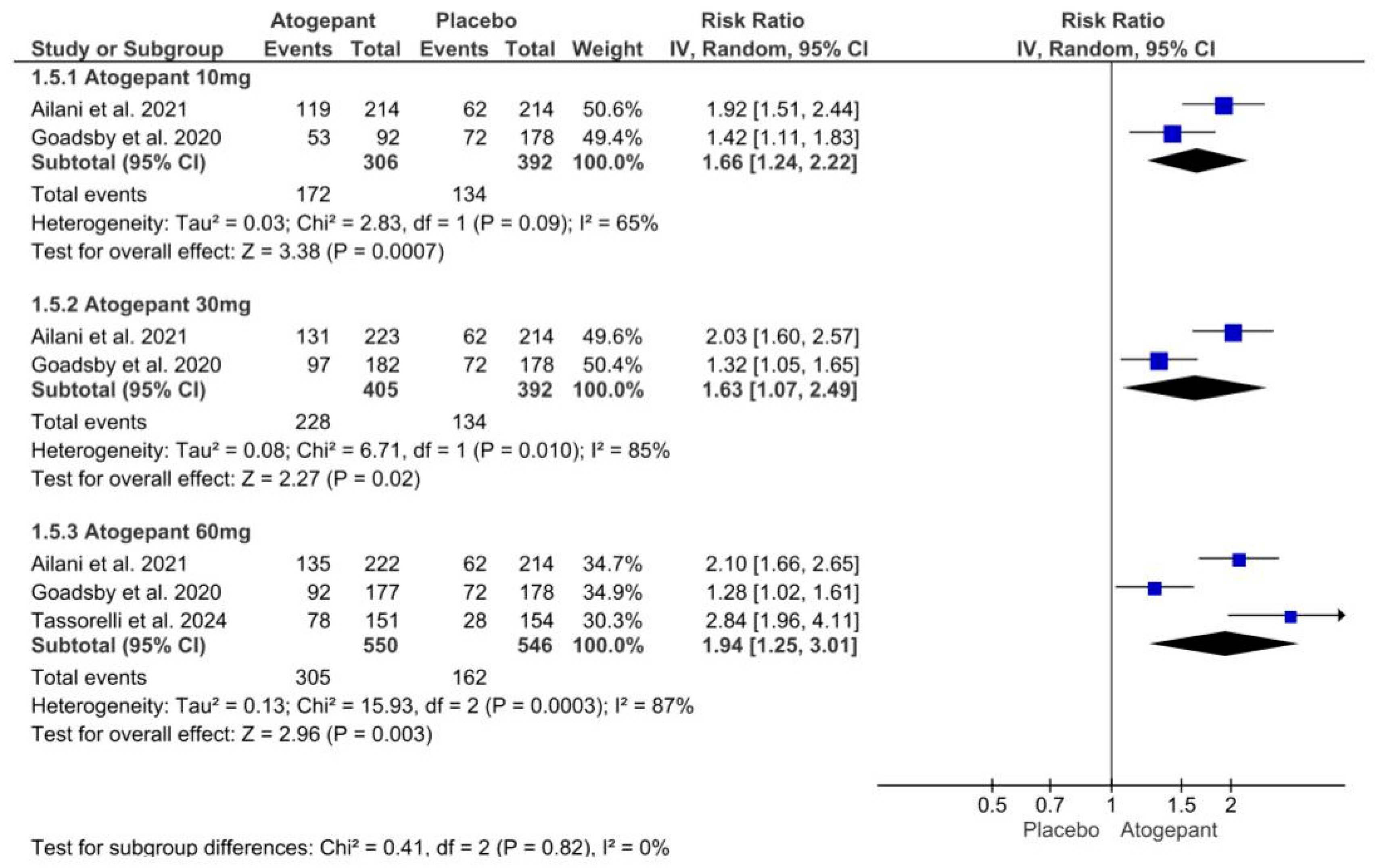
3.8. ≥Outcome of 50% Reduction in Monthly Migraine Days
3.9. Adverse Events
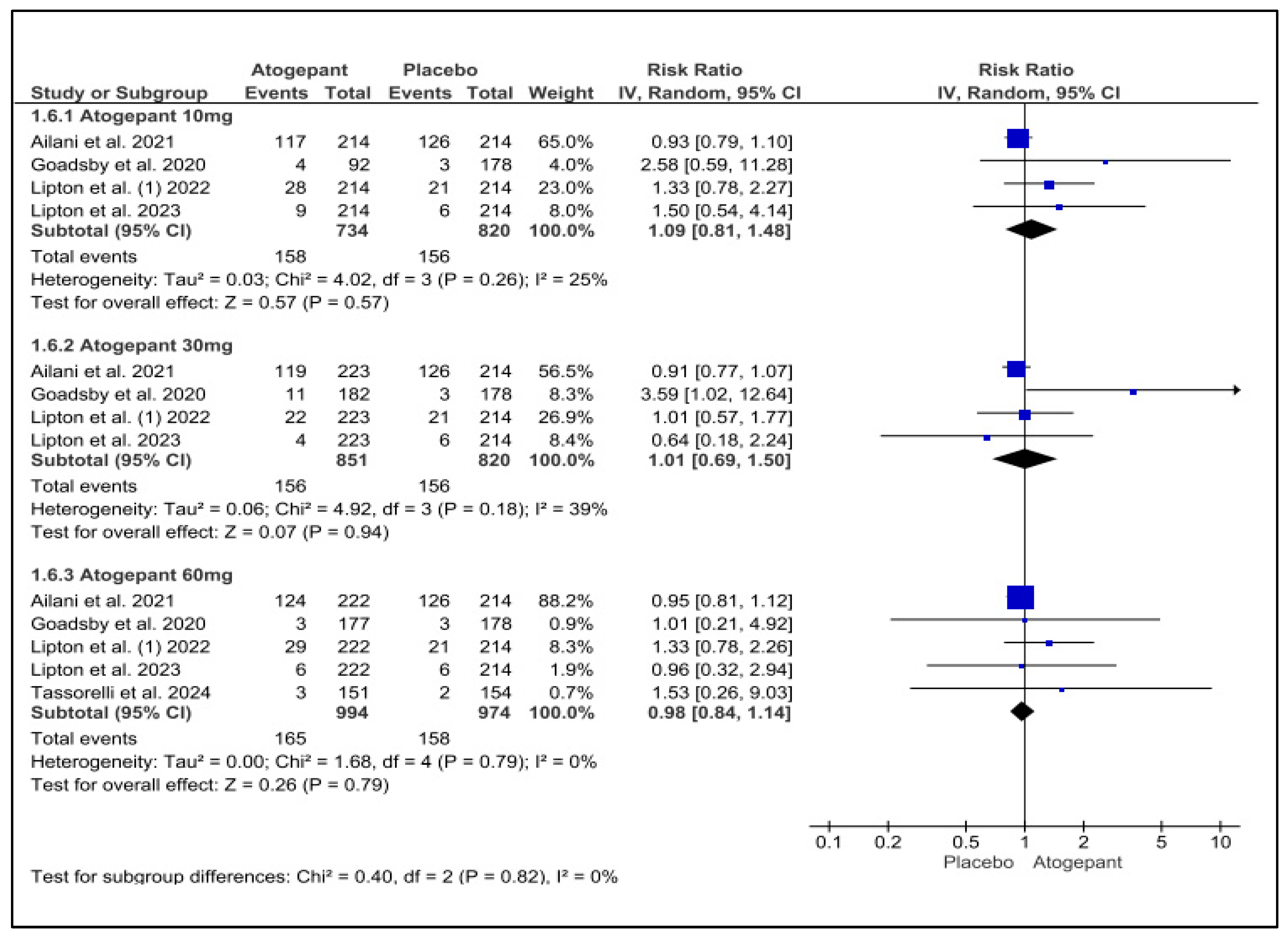
3.10. Any Adverse Events
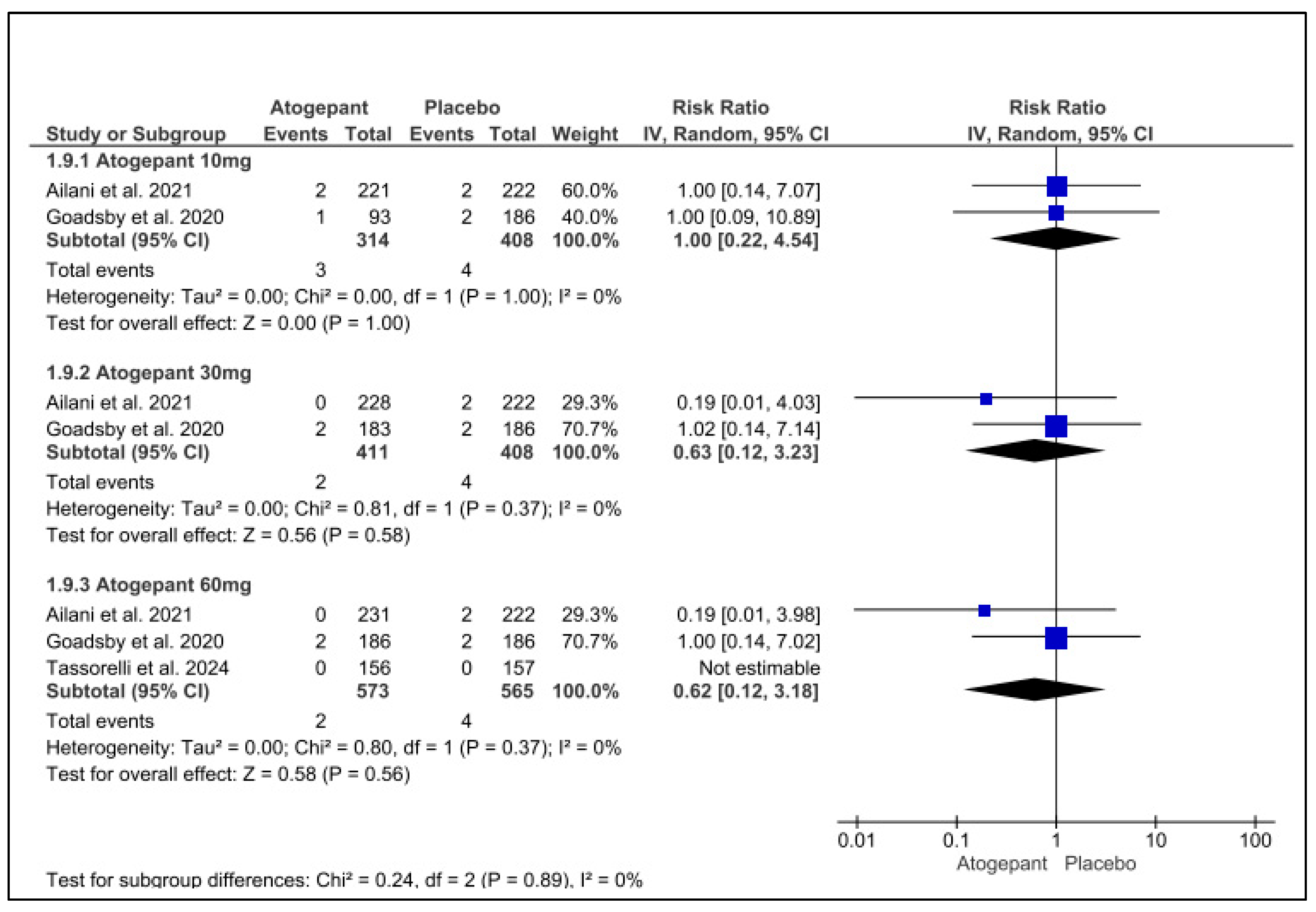
3.11. Serious Adverse Events
3.12. Discontinuation Due to Adverse Events
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lipton, R.B.; Bigal, M.E.; Diamond, M.; Freitag, F.; Reed, M.L.; Stewart, W.F. Migraine prevalence, disease burden, and the need for preventive therapy. Neurology 2007, 68, 343–349. Available online: https://www.neurology.org/doi/10.1212/01.wnl.0000252808.97649.21?url_ver=Z39.88-2003&rfr_id=ori:rid:crossref.org&rfr_dat=cr_pub%20%200pubmed (accessed on 30 June 2024). [CrossRef] [PubMed]
- Steiner, T.J.; Stovner, L.J.; Birbeck, G.L. Migraine: The seventh disabler. J. Headache Pain 2013, 14, 1–3. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3606966/pdf/1129-2377-14-1.pdf (accessed on 30 June 2024). [CrossRef] [PubMed]
- Steiner, T.J.; Stovner, L.J.; Jensen, R.; Uluduz, D.; Katsarava, Z. Migraine remains second among the world’s causes of disability, and first among young women: Findings from GBD2019. Headache Pain 2020, 21, 137–141. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7708887/pdf/10194_2020_Article_1208.pdf (accessed on 30 June 2024). [CrossRef]
- Stewart, W.F.; Ricci, J.A.; Chee, E.; Morganstein, D.; Lipton, R. Lost Productive Time and Cost Due to Common Pain Conditions in the US Workforce. JAMA 2003, 290, 2443–2454. Available online: https://jamanetwork.com/journals/jama/fullarticle/197628#google_vignette (accessed on 30 June 2024). [CrossRef]
- Ashina, M.; Katsarava, Z.; Do, T.P.; Buse, D.C.; Pozo-Rosich, P.; Özge, A.; Krymchantowski, A.V.; Lebedeva, E.R.; Ravishankar, K.; Yu, S.; et al. Migraine: Epidemiology and systems of care. Lancet 2021, 397, 1485–1495. Available online: https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(20)32160-7/abstract (accessed on 30 June 2024). [CrossRef]
- Leonardi, M.; Raggi, A. Burden of migraine: International perspectives. Neurol. Sci. 2013, 34 (Suppl. S1), S117–S118. Available online: https://link.springer.com/article/10.1007/s10072-013-1387-8 (accessed on 30 June 2024). [CrossRef]
- Olesen, J.; Headache Classification Committee of the International Headache Society (IHS). The International Classification of Headache Disorders, 3rd edition. Cephalalgia 2018, 1, 1–211. Available online: https://www.ichd-3.org/wp-content/uploads/2018/01/The-International-Classification-of-Headache-Disorders-3rd-Edition-2018.pdf (accessed on 30 June 2024).
- Buse, D.C.; Manack, A.N.; Fanning, K.M.; Serrano, D.; Reed, M.L.; Turkel, C.C.; Lipton, R.B. Chronic migraine prevalence, disability, and sociodemographic factors: Results from the American migraine prevalence and prevention study. Headache 2012, 52, 1456–1470. Available online: https://headachejournal.onlinelibrary.wiley.com/doi/epdf/10.1111/j.1526-4610.2012.02223.x (accessed on 30 June 2024). [CrossRef]
- Lipton, R.B.; Pozo-Rosich, P.; Blumenfeld, A.M.; Dodick, D.W.; McAllister, P.; Li, Y.; Lu, K.; Dabruzzo, B.; Miceli, R.; Severt, L.; et al. Rates of Response to Atogepant for Migraine Prophylaxis among Adults: A Secondary Analysis of a Randomized Clinical Trial. JAMA Netw. Open 2022, 5, E2215499. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9178435/#:~:text=In%20a%20secondary%20analysis%20of%20a%20phase%203%2C,mean%20monthly%20migraine-days%20during%2012%20weeks%20of%20treatment (accessed on 30 June 2024). [CrossRef]
- Katsarava, Z.; Buse, D.C.; Manack, A.N.; Lipton, R.B. Defining the differences between episodic migraine and chronic migraine. Curr. Pain Headache Rep. 2012, 16, 86–92. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3258393/pdf/11916_2011_Article_233.pdf (accessed on 30 June 2024). [CrossRef]
- Ailani, J.; Lipton, R.B.; Goadsby, P.J.; Guo, H.; Miceli, R.; Severt, L.; Finnegan, M.; Trugman, J.M.; ADVANCE Study Group. Atogepant for the Preventive Treatment of Migraine. N. Engl. J. Med. 2021, 385, 695–706. Available online: https://www.nejm.org/doi/pdf/10.1056/NEJMoa2035908 (accessed on 30 June 2024). [CrossRef] [PubMed]
- Tao, X.; Yan, Z.; Meng, J.; Wang, W.; Dai, Q.; Zhou, Q.; Wang, Z.; Wang, Z. The efficacy and safety of atogepant for the prophylactic treatment of migraine: Evidence from randomized controlled trials. J. Headache Pain 2022, 23, 19–31. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8903713/pdf/10194_2022_Article_1391.pdf (accessed on 30 June 2024). [CrossRef] [PubMed]
- Sacco, S.; Lampl, C.; Maassen van den Brink, A.; Caponnetto, V.; Braschinsky, M.; Ducros, A.; Little, P.; Pozo-Rosich, P.; Reuter, U.; Ruiz de la Torre, E.; et al. Burden and Attitude to Resistant and Refractory (BARR) Study Group; Burden and attitude to resistant and refractory migraine: A survey from the European Headache Federation with the endorsement of the European Migraine & Headache Alliance. J. Headache Pain 2021, 22, 39–49. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8130435/pdf/10194_2021_Article_1252.pdf (accessed on 30 June 2024). [PubMed]
- Goadsby, P.J.; Holland, P.R.; Martins-Oliveira, M.; Hoffmann, J.; Schankin, C.; Akerman, S. Pathophysiology of Migraine: A Disorder of Sensory Processing. Physiol. Rev. 2017, 97, 553–622. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5539409/ (accessed on 30 June 2024). [CrossRef]
- Dodick, D.W. Migraine. Lancet 2018, 391, 1315–1330. [Google Scholar] [CrossRef]
- Lattanzi, S.; Trinka, E.; Altamura, C.; Del Giovane, C.; Silvestrini, M.; Brigo, F.; Vernieri, F. Atogepant for the Prevention of Episodic Migraine in Adults: A Systematic Review and Meta-Analysis of Efficacy and Safety. Neurol. Ther. 2022, 11, 1235–1252. Available online: https://link.springer.com/content/pdf/10.1007/s40120-022-00370-8.pdf (accessed on 30 June 2024). [CrossRef]
- Tepper, D. Gepants. Headache: The Journal of Head and Face Pain© 2020 American Headache Society Published by Wiley Periodicals, Inc. 1037–1039. Available online: https://headachejournal.onlinelibrary.wiley.com/doi/epdf/10.1111/head.13791 (accessed on 30 June 2024).
- Tassorelli, C.; Onishchenko, K.; Halker Singh, R.B.; Duan, M.; Dupont-Benjamin, L.; Hemstock, M.; Voller, C.; McAllister, P.; Nahas, S.J.; Gandhi, P.; et al. Comparative efficacy, quality of life, safety, and tolerability of atogepant and rimegepant in migraine prevention: A matching-adjusted indirect comparison analysis. Cephalalgia 2024, 44, 3331024241235156. [Google Scholar] [CrossRef]
- Switzer, M.P.; Robinson, J.E.; Joyner, K.R.; Morgan, K.W. Atogepant for the prevention of episodic migraine in adults. SAGE Open Med. 2022, 10, 20503121221128688. [Google Scholar] [CrossRef]
- Schiffman, E.; Ohrbach, R.; Truelove, E.; Anderson, G.; Goulet, J.-P.; List, T.; Svensson, P.; Gonzalez, Y.; Lobbezoo, F.; Michelotti, A.; et al. The International Classification of Headache Disorders, 3rd edition (beta version). Cephalalgia 2013, 33, 629–808. Available online: https://www.zora.uzh.ch/id/eprint/89115/ (accessed on 30 June 2024).
- Seo, H.J.; Kim, S.Y.; Lee, Y.J.; Park, J.E. RoBANS 2: A Revised Risk of Bias Assessment Tool for Nonrandomized Studies of Interventions. Korean J. Fam. Med. 2023, 44, 249–260. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10522469/pdf/kjfm-23-0034.pdf (accessed on 30 June 2024). [CrossRef]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. Available online: https://www.bmj.com/content/bmj/366/bmj.l4898.full.pdf (accessed on 30 June 2024). [CrossRef] [PubMed]
- Higgins, J.P.T.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 2002, 21, 1539–1558. Available online: https://pubmed.ncbi.nlm.nih.gov/12111919/ (accessed on 30 June 2024). [CrossRef] [PubMed]
- Book Series, C.; Higgins, J.P.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions; The Cochrane Collaboration®: London, UK, 2008. [Google Scholar]
- Schwedt, T.J.; Lipton, R.B.; Ailani, J.; Silberstein, S.D.; Tassorelli, C.; Guo, H.; Lu, K.; Dabruzzo, B.; Miceli, R.; Severt, L.; et al. Time course of efficacy of atogepant for the preventive treatment of migraine: Results from the randomized, double-blind ADVANCE trial. Cephalalgia 2022, 42, 3–11. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8739573/pdf/10.1177_03331024211042385.pdf (accessed on 30 June 2024). [CrossRef] [PubMed]
- Goadsby, P.J.; Dodick, D.W.; Ailani, J.; Trugman, J.M.; Finnegan, M.; Lu, K.; Szegedi, A. Safety, tolerability, and efficacy of orally administered atogepant for the prevention of episodic migraine in adults: A double-blind, randomised phase 2b/3 trial. Lancet Neurol. 2020, 19, 727–737. Available online: https://www.thelancet.com/journals/laneur/article/PIIS1474-4422(20)30234-9/abstract (accessed on 30 June 2024). [CrossRef]
- Lipton, R.B.; Pozo-Rosich, P.; Blumenfeld, A.M.; Li, Y.; Severt, L.; Stokes, J.T.; Creutz, L.; Gandhi, P.; Dodick, D. Effect of Atogepant for Preventive Migraine Treatment on Patient-Reported Outcomes in the Randomized, Double-blind, Phase 3 ADVANCE Trial. Neurology 2023, 100, E764–E777. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9984220/pdf/WNL-2022-201407.pdf (accessed on 30 June 2024). [CrossRef]
- Tassorelli, C.; Nagy, K.; Pozo-Rosich, P.; Lanteri-Minet, M.; Sacco, S.; Nežádal, T.; Guo, H.; De Abreu Ferreira, R.; Forero, G.; Trugman, J.M. Safety and efficacy of atogepant for the preventive treatment of episodic migraine in adults for whom conventional oral preventive treatments have failed (ELEVATE): A randomised, placebo-controlled, phase 3b trial. Lancet Neurol. 2024, 23, 382–392. Available online: https://www.thelancet.com/journals/laneur/article/PIIS1474-4422(24)00025-5/abstract (accessed on 30 June 2024). [CrossRef]
- Lipton, R.B.; Nahas, S.J.; Pozo-Rosich, P.; Bilchik, T.; McAllister, P.; Finnegan, M.; Liu, Y.; Chalermpalanupap, N.; Dabruzzo, B.; Dodick, D.W. Sustained response to atogepant in episodic migraine: Post hoc analyses of a 12-week randomized trial and a 52-week long-term safety trial. J. Headache Pain 2024, 25, 83–94. [Google Scholar] [CrossRef]
- Cohen, F.; Yuan, H.; Silberstein, S.D. Calcitonin Gene-Related Peptide (CGRP)-Targeted Monoclonal Antibodies and Antagonists in Migraine: Current Evidence and Rationale. BioDrugs 2022, 36, 341–358. [Google Scholar] [CrossRef]
- Hou, M.; Luo, X.; He, S.; Yang, X.; Zhang, Q.; Jin, M.; Zhang, P.; Li, Y.; Bi, X.; Li, J.; et al. Efficacy and safety of atogepant, a small molecule CGRP receptor antagonist, for the preventive treatment of migraine: A systematic review and meta-analysis. J. Headache Pain 2024, 25, 116–132. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11264921/pdf/10194_2024_Article_1822.pdf (accessed on 30 June 2024). [CrossRef]
- Lopes, L.M.; de Almeida, A.M.; Pasqualotto, E.; Sudo, R.Y.; Leite, M.G.; Souza, M.E.C.; de Moraes, F.C.A.; Siebel, V.M.; Figueiredo, N. Efficacy and Safety of Atogepant for Preventing Chronic and Episodic Migraines: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Curr. Treat. Options Neurol. 2024, 26, 411–419. Available online: https://link.springer.com/article/10.1007/s11940-024-00803-9 (accessed on 30 June 2024). [CrossRef]
- Feigin, V.L.; Nichols, E.; Alam, T.; Bannick, M.S.; Beghi, E.; Blake, N.; Culpepper, W.J.; Dorsey, E.R.; Elbaz, A.; Ellenbogen, R.G.; et al. Global, regional, and national burden of neurological disorders, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2019, 18, 459–480. Available online: https://research.wur.nl/en/publications/global-regional-and-national-burden-of-neurological-disorders-199 (accessed on 30 June 2024). [CrossRef] [PubMed]
- Lampl, C.; Maassen Van Den Brink, A.; Deligianni, C.I.; Gil-Gouveia, R.; Jassal, T.; Sanchez-del-Rio, M.; Reuter, U.; Uluduz, D.; Versijpt, J.; Zeraatkar, D.; et al. The comparative effectiveness of migraine preventive drugs: A systematic review and network meta-analysis. J. Headache Pain 2023, 24, 56–70. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10197489/pdf/10194_2023_Article_1594.pdf (accessed on 30 June 2024). [CrossRef] [PubMed]
- Charles, A.C.; Digre, K.B.; Goadsby, P.J.; Robbins, M.S.; Hershey, A. American Headache Society.; Calcitonin gene-related peptide-targeting therapies are a first-line option for the prevention of migraine: An American Headache Society position statement update. Headache 2024, 64, 333–341. Available online: https://headachejournal.onlinelibrary.wiley.com/doi/epdf/10.1111/head.14692 (accessed on 30 June 2024). [CrossRef] [PubMed]
- National Institute for Health and Care Excellence (NICE). Atogepant for Preventing Migraine Technology Appraisal Guidance. 2024. Available online: https://www.nice.org.uk/guidance/ta973/resources/atogepant-for-preventing-migraine-pdf-82615848254917 (accessed on 30 June 2024).
- Raja, A.; Asim, R.; Shuja, M.H.; Raja, S.; Saleh Muhammad, T.; Bajaj, S.; Ansari, A.H.; Ali, H.; Magsi, I.A.; Faridi, M.H.; et al. Atogepant for Migraine Prevention: A Meta-Analysis of Safety and Efficacy in Adults. Front. Neurol. 2024, 15, 1468961. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Goadsby et al., 2020 [26] | Schwedt et al., 2022 [25] | ||||||
|---|---|---|---|---|---|---|---|---|
| Placebo | Atogepant 10 mg Once Daily | Atogepant 30 mg Once Daily | Atogepant 60 mg Once Daily | Placebo | Atogepant 10 mg Once Daily | Atogepant 30 mg Once Daily | Atogepant 60 mg Once Daily | |
| Total sample size | 186 | 93 | 183 | 186 | 222 | 221 | 228 | 231 |
| Modified intention to treat population | 178 | 92 | 182 | 177 | 214 | 214 | 223 | 222 |
| Age, years | 40.5 (11.7) | 39.4 (12.4) | 41.0 (13.6) | 40.4 (11.7) | 40.3 (12.8) | 41.4 (12.1) | 42.1 (11.7) | 42.5 (12.4) |
| Female sex | 154 (83%) | 82 (88%) | 166 (91%) | 156 (84%) | 198 (89.2%) | 200 (90.5%) | 204 (89.5%) | 199 (86.1%) |
| White race | 137 (74%) | 69 (74%) | 145 (79%) | 133 (72%) | 194 (87.4%) | 181 (81.9%) | 185 (81.1%) | 192 (83.1%) |
| Black race | 45 (24%) | 20 (22%) | 29 (16%) | 44 (24%) | N/A | N/A | N/A | N/A |
| Other races | 4 (2%) | 4 (4%) | 9 (5%) | 9 (5%) | 199 (89.6%) | 200 (90.5%) | 209 (91.7%) | 217 (93.9%) |
| Body mass index, kg/m | 30.4 (7.6) | 29.9 (7.3) | 30.0 (7.1) | 30.0 (7.8) | 30.8 (8.7) | 30.4 (7.6) | 31.2 (7.6) | 29.9 (7.3) |
| Monthly migraine days | 7.8 (2.5) | 7.6 (2.5) | 7.6 (2.4) | 7.7 (2.6) | 7.5 (2.4) | 7.5 (2.5) | 7.9 (2.3) | 7.8 (2.3) |
| Migraine with aura | 45 (24%) | 21 (23%) | 37 (20%) | 36 (19%) | N/A | N/A | N/A | N/A |
| Migraine without aura | 94 (51%) | 48 (52%) | 93 (51%) | 96 (52%) | N/A | N/A | N/A | N/A |
| Monthly headache days | 9.1 (2.7) | 8.9 (2.7) | 8.7 (2.5) | 8.9 (2.8) | 8.4 (2.6) | 8.4 (2.8) | 8.8 (2.6) | 9.0 (2.6) |
| Monthly acute medication use days | 6.6 (3.2) | 6.2 (3.3) | 6.6 (3.0) | 6.8 (3.3) | 6.5 (3.2) | 6.6 (3.0) | 6.7 (3.0) | 6.9 (3.2) |
| Variable | Tassorelli et al., 2024 [28] | Ailani et al., 2021 [11] | ||||||
| Placebo | Atogepant 10 mg Once Daily | Atogepant 30 mg Once Daily | Atogepant 60 mg Once Daily | Placebo | Atogepant 10 mg Once Daily | Atogepant 30 mg Once Daily | Atogepant 60 mg Once Daily | |
| Total sample size | 157 | N/A | N/A | 156 | 222 | 221 | 228 | 231 |
| Modified intention to treat population | 154 | N/A | N/A | 151 | 214 | 214 | 223 | 222 |
| Age, years | 43.4 (10.3) | N/A | N/A | 40.9 (10.7) | 40.3 (12.8) | 41.4 (12.0) | 42.1 (11.7) | 42.5 (12.4) |
| Female sex | 141 (90%) | N/A | N/A | 139 (89%) | 198 (89.2%) | 200 (90.5%) | 204 (89.5%) | 199 (86.1%) |
| White race | 151 (96%) | N/A | N/A | 149 (96%) | 194 (87.4%) | 181 (81.9%) | 185 (81.1%) | 192 (83.1%) |
| Black race | 4 (3%) | N/A | N/A | 3 (2%) | 24 (10.8%) | 34 (15.4%) | 38 (16.7%) | 28 (12.1%) |
| Other races | 2 (1%) | N/A | N/A | 2 (1%) | 4 (1.8%) | 6 (2.8%) | 5 (2.1%) | 10 (4.3%) |
| Body mass index, kg/m | 26.2 (5.2) | N/A | N/A | 25.6 (4.9) | 30.8 (8.7) | 30.3 (7.6) | 31.1 (7.6) | 29.9 (7.3) |
| Monthly migraine days | N/A | N/A | N/A | N/A | 7.7 (2.6) | 7.2 (2.5) | 7.3 (2.4) | 7.3 (2.4) |
| Migraine with aura | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N/A |
| Migraine without aura | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N/A |
| Monthly headache days | N/A | N/A | N/A | N/A | 9.5 (2.8) | 9.3 (2.7) | 9.2 (2.7) | 9.1 (2.7) |
| Monthly acute medication use days | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N/A |
| Variable | Lipton et al., 2023 [27] | Lipton et al., 2022 [9] | ||||||
| Placebo | Atogepant 10 mg Once Daily | Atogepant 30 mg Once Daily | Atogepant 60 mg Once Daily | Placebo | Atogepant 10 mg Once Daily | Atogepant 30 mg Once Daily | Atogepant 60 mg Once Daily | |
| Total sample size | 222 | 221 | 228 | 231 | 222 | 221 | 228 | 231 |
| Modified intention to treat population | 214 | 214 | 223 | 222 | 214 | 214 | 223 | 222 |
| Age, years | 40.3 (12.9) | 41.5 (12.0) | 42.2 (11.7) | 42.8 (12.3) | 40.3 (12.8) | 41.4 (12.1) | 42.1 (11.7) | 42.5 (12.4) |
| Female sex | 190 (88.8%) | 193 (90.2%) | 199 (89.2%) | 191 (86.0%) | 198 (89.2%) | 200 (90.5%) | 204 (89.5%) | 199 (86.1%) |
| White race | 188 (87.9%) | 176 (82.2%) | 181 (81.2%) | 184 (82.9%) | 194 (87.4%) | 181 (81.9%) | 185 (81.1%) | 192 (83.1%) |
| Black race | 22 (10.3%) | 32 (15.0%) | 37 (16.6%) | 27 (12.2%) | 24 (10.8%) | 34 (15.4%) | 38 (16.7%) | 28 (12.1%) |
| Other races | 4 (1.8%) | 6 (2.8%) | 5 (2.2%) | 11 (5%) | 4 (1.8%) | 6 (2.8%) | 5 (2.1%) | 11 (4.7%) |
| Body mass index, kg/m | N/A | N/A | N/A | N/A | 30.8 (8.7%) | 30.4 (7.6%) | 31.2 (7.6%) | 29.9 (7.3%) |
| Monthly migraine days baseline | 7.5 (2.4) | 7.5 (2.5) | 7.9 (2.3) | 7.8 (2.3) | 7.5 (2.4) | 7.5 (2.5) | 7.9 (2.3) | 7.8 (2.3) |
| Migraine with aura | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N/A |
| Migraine without aura | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N/A |
| Monthly headache days | 8.4 (2.6) | 8.4 (2.8) | 8.8 (2.6) | 9.0 (2.6) | N/A | N/A | N/A | N/A |
| Monthly acute medication use days | 6.5 (3.2) | 6.6 (3.0) | 6.7 (3.0) | 6.9 (3.2) | N/A | N/A | N/A | N/A |
| Study Reference | Placebo | Atogepant 10 mg Once Daily | Atogepant 30 mg Once Daily | Atogepant 60 mg Once Daily | |
|---|---|---|---|---|---|
| Any treatment-related TEAE | Lipton et al.’s (2022) [9] | 20/222 (9%) | 51/221 (23.1%) | 34/228 (14.9%) | 45/231 (19.5%) |
| Constipation | 1/222 (5%) | 17/221 (7.7%) | 16/228 (7%) | 16/231 (6.9%) | |
| Nausea | 4/222 (1.8%) | 11/221 (5%) | 10/228 (4.4%) | 14/231 (6.1%) | |
| Any treatment-related TEAE | Ailani et al. (2021) [11] | 20/222 (9%) | 51/221 (23.1%) | 34/228 (14.9%) | 45/231 (19.5%) |
| Constipation | 1/222 (0.5%) | 17/221 (7.7%) | 16/228 (7%) | 16/231 (6.9%) | |
| Upper respiratory tract infection | 10/222 (4.5%) | 9/221 (4.1%) | 13/228 (5.7%) | 9/231 (3.9%) | |
| Nausea | 4/222 (1.8%) | 11/221 (5%) | 10/228 (4.4%) | 14/231 (6.1%) | |
| Any treatment-related TEAE | Schwedt et al. (2022) [25] | 56.80% | N/A | N/A | N/A |
| Nausea | N/A | N/A | N/A | N/A | |
| Constipation | N/A | N/A | N/A | N/A | |
| Fatigue | N/A | N/A | N/A | N/A | |
| Any treatment-related TEAE | Goadsby et al. (2020) [26] | 30/186 (16%) | 17/93 (18%) | 39/183 (21%) | 42/186 (23%) |
| Nausea | 5/186 (3%) | 3/93 (3%) | 10/183 (5%) | 11/186 (6%) | |
| Constipation | 2/186 (1%) | 1/93 (1%) | 10/183 (5%) | 8/186 (4%) | |
| Fatigue | 4/186 (2%) | 1/93 (1%) | 2/183 (1%) | 4/186 (2%) | |
| Any treatment-related TEAE | Lipton et al. (2023) [27] | N/A | N/A | N/A | N/A |
| Nausea | N/A | N/A | N/A | N/A | |
| Constipation | N/A | N/A | N/A | N/A | |
| Fatigue | N/A | N/A | N/A | N/A | |
| Any treatment-related TEAE | Tassorelli et al. (2024) [28] | 14/157 (9%) | N/A | N/A | 31/156 (20%) |
| Constipation | 3/157 (2%) | N/A | N/A | 13/156 (8%) | |
| Nausea | 3/157 (2%) | N/A | N/A | 8/156 (5%) | |
| Decreased appetite | 0 | N/A | N/A | 5/156 (3%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alrasheed, A.S.; Almaqboul, T.M.; Alshamrani, R.A.; AlMohish, N.M.; Alabdali, M.M. Safety and Efficacy of Atogepant for the Preventive Treatment of Migraines in Adults: A Systematic Review and Meta-Analysis. J. Clin. Med. 2024, 13, 6713. https://doi.org/10.3390/jcm13226713
Alrasheed AS, Almaqboul TM, Alshamrani RA, AlMohish NM, Alabdali MM. Safety and Efficacy of Atogepant for the Preventive Treatment of Migraines in Adults: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine. 2024; 13(22):6713. https://doi.org/10.3390/jcm13226713
Chicago/Turabian StyleAlrasheed, Abdulrahim Saleh, Taif Mansour Almaqboul, Reem Ali Alshamrani, Noor Mohammad AlMohish, and Majed Mohammad Alabdali. 2024. "Safety and Efficacy of Atogepant for the Preventive Treatment of Migraines in Adults: A Systematic Review and Meta-Analysis" Journal of Clinical Medicine 13, no. 22: 6713. https://doi.org/10.3390/jcm13226713
APA StyleAlrasheed, A. S., Almaqboul, T. M., Alshamrani, R. A., AlMohish, N. M., & Alabdali, M. M. (2024). Safety and Efficacy of Atogepant for the Preventive Treatment of Migraines in Adults: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine, 13(22), 6713. https://doi.org/10.3390/jcm13226713