
Dyadic Effects of Attachment on Illness Acceptance in Patients with Breast Cancer and Spousal Caregivers: Sense of Coherence as a Mediator




Abstract
1. Introduction
1.1. Associations between Attachment and Illness Acceptance
1.2. Sense of Coherence as a Potential Mediator
1.3. The Present Study
2. Materials and Methods
2.1. Participants and Procedure
2.2. Measures
2.2.1. Attachment
2.2.2. Sense of Coherence
2.2.3. Illness Acceptance
2.3. Statistical Analyses
3. Results
3.1. Descriptive Statistics and Correlational Findings
3.2. Testing Actor–Partner Interdependence Models: Path Analysis
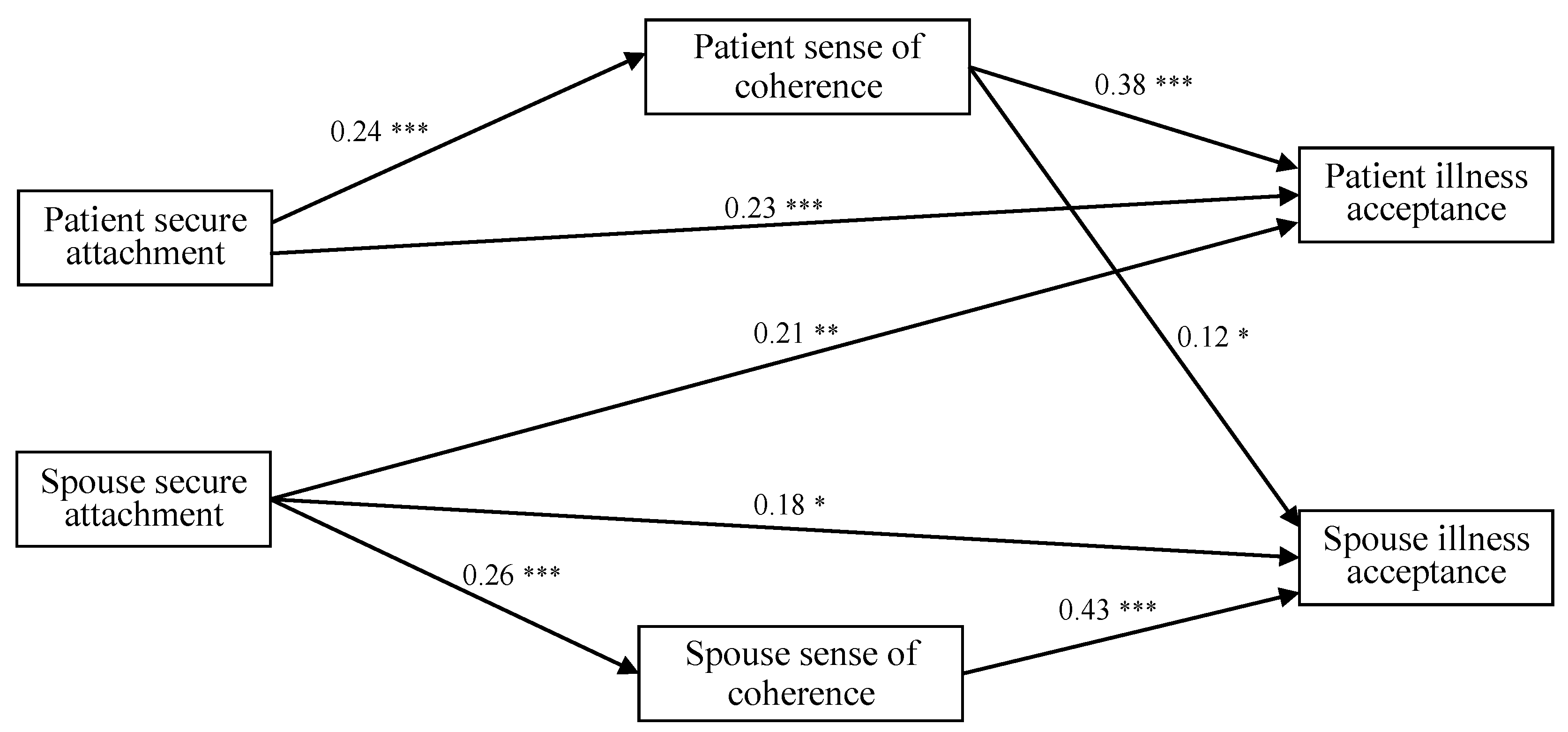
3.2.1. Secure Attachment
3.2.2. Avoidant Attachment
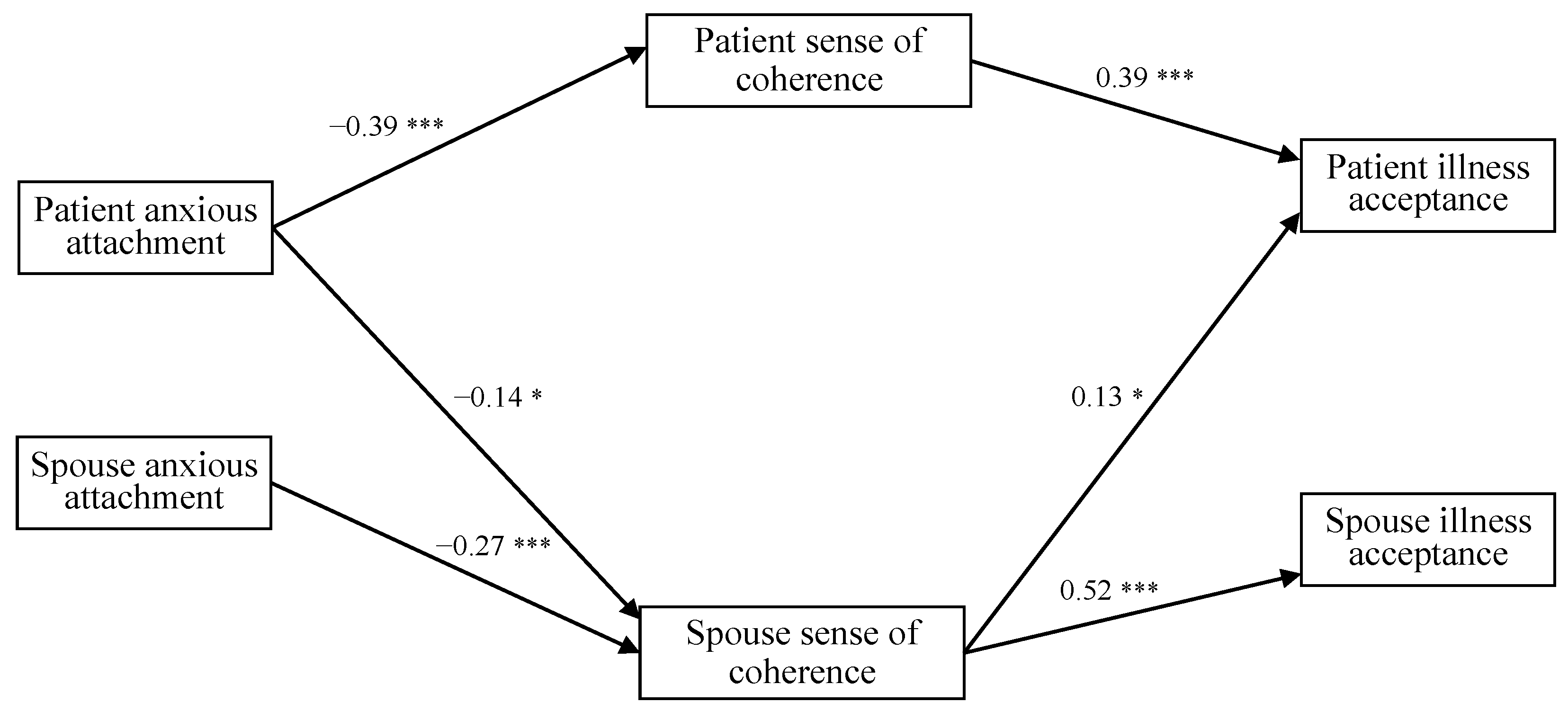
3.2.3. Anxious Attachment
4. Discussion
4.1. Associations Among Attachment, Sense of Coherence, and Illness Acceptance
4.2. Actor–Actor Effects
4.3. Actor–Partner Effects
4.4. Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sedeta, E.T.; Jobre, B.; Avezbakiyev, B. Breast cancer: Global patterns of incidence, mortality, and trends. J. Clin. Oncol. 2023, 41 (Suppl. 16), 10528. [Google Scholar] [CrossRef]
- The Incidence and Mortality of Female Cancers in Poland Are Increasing. Available online: https://www.onkonet.pl/n_n_nowotwory_kobiece_potrzeba_zmian.php (accessed on 9 September 2024).
- Bradford, A.B.; Drean, L.; Sandberg, J.G.; Johnson, L.N. They may disapprove, but I still love you: Attachment behaviors moderate the effect of social disapproval on marital relationship quality. Fam. Process 2020, 59, 1530–1551. [Google Scholar] [CrossRef] [PubMed]
- Bowlby, J. Attachment and Loss: Vol. 1. Attachment, 2nd ed.; Basic Books: New York, NY, USA, 1982. [Google Scholar]
- Bowlby, J. A Secure Base: Parent-Child Attachment and Healthy Human Development; Basic Books: New York, NY, USA, 1988. [Google Scholar]
- Mikulincer, M.; Shaver, P.R. Attachment orientations and emotion regulation. Curr. Opin. Psychol. 2019, 25, 6–10. [Google Scholar] [CrossRef]
- Milbury, K.; Yang, C.; Liao, Z.X.; Tsao, A.S.; Bruera, E. Relationship processes and symptom burden in couples coping with metastatic lung cancer. J. Clin. Oncol. 2018, 36 (Suppl. 34), 169. [Google Scholar] [CrossRef]
- Ramos, K.; Langer, S.L.; Todd, M.; Romano, J.M.; Ghosh, N.; Keefe, F.J.; Baucom, D.H.; Syrjala, K.L.; Porter, L.S. Attachment style, partner communication, and physical well-being among couples coping with cancer. Pers. Relatsh. 2020, 27, 526–549. [Google Scholar] [CrossRef]
- Ramos, K.; Leo, K.; Porter, L.S.; Romano, J.M.; Baucom, B.R.; Langer, S.L. Attachment in couples coping with cancer: Associations with observed communication and long-term health. Int. J. Environ. Res. Public Health 2023, 20, 5249. [Google Scholar] [CrossRef] [PubMed]
- Karveli, S.; Galanis, P.; Mitropoulou, E.M.; Karademas, E.; Markopoulos, C. The role of attachment styles on quality of life and distress among early-stage female breast cancer patients: A systematic review. J. Clin. Psychol. Med. Settings 2023, 30, 724–739. [Google Scholar] [CrossRef]
- Nissen, K.G. Correlates of self-rated attachment in patients with cancer and their caregivers: A systematic review and meta-analysis. Psychooncology 2016, 25, 1017–1027. [Google Scholar] [CrossRef]
- Xiaoyun, C.; Fenglan, L. The relationships among insecure attachment, social support and psychological experiences in family caregivers of cancer inpatients. Eur. J. Oncol. Nurs. 2020, 44, 101691. [Google Scholar] [CrossRef]
- Hiebler-Ragger, M.; Nausner, L.; Blaha, A.; Grimmer, K.; Korlath, S.; Mernyi, M.; Unterrainer, H.F. The supervisory relationship from an attachment perspective: Connections to burnout and sense of coherence in health professionals. Clin. Psychol. Psychother. 2021, 28, 124–136. [Google Scholar] [CrossRef]
- Shalev, D.; Jacobsen, J.C.; Rosenberg, L.B.; Brenner, K.O.; Seaton, M.; Jackson, V.A.; Greer, J.A. (Don’t) Leave Me Alone: Attachment in Palliative Care. J. Palliat. Med. 2022, 25, 9–14. [Google Scholar] [CrossRef] [PubMed]
- Crangle, C.J.; Torbit, L.A.; Ferguson, S.E.; Hart, T.L. Dyadic coping mediates the effects of attachment on quality of life among couples facing ovarian cancer. J. Behav. Med. 2020, 43, 564–575. [Google Scholar] [CrossRef] [PubMed]
- Trejnowska, A.; Goodall, K.; Rush, R.; Ellison, M.; McVittie, C. The relationship between adult attachment and coping with brain tumour: The mediating role of social support. Psychooncology 2020, 29, 729–736. [Google Scholar] [CrossRef]
- Tao, L.; Lv, J.; Tan, X.; Hu, X.; Fu, L.; Li, J. Relationships between attachment style, emotional self-disclosure, and quality of life among young breast cancer survivors: A cross-sectional study. Semin. Oncol. Nurs. 2024, 40, 151526. [Google Scholar] [CrossRef]
- Krok, D.; Zarzycka, B.; Telka, E. The interplay of religious and nonreligious meaning-making on psychological well-being in gastrointestinal cancer patients. Int. J. Psychol. Relig. 2021, 31, 276–287. [Google Scholar] [CrossRef]
- Hinz, A.; Schulte, T.; Ernst, J.; Mehnert-Theuerkauf, A.; Finck, C.; Wondie, Y.; Ernst, M. Sense of coherence, resilience, and habitual optimism in cancer patients. Int. J. Clin. Health Psychol. 2023, 23, 100358. [Google Scholar] [CrossRef] [PubMed]
- Antonovsky, A. Health, Stress and Coping; Jossey-Bass: San Francisco, CA, USA, 1979. [Google Scholar]
- Eriksson, M. The sense of coherence: The concept and its relationship to health. In The Handbook of Salutogenesis, 2nd ed.; Mittelmark, M.B., Bauer, G.F., Vaandrager, L., Pelikan, J.M., Sagy, S., Eriksson, M., Lindström, B., Magistretti, C.M., Eds.; Springer: Cham, Switzerland, 2022; pp. 61–68. [Google Scholar]
- Pasek, M.; Dębska, G.; Wojtyna, E. Perceived social support and the sense of coherence in patient–caregiver dyad versus acceptance of illness in cancer patients. J. Clin. Nurs. 2017, 26, 4985–4993. [Google Scholar] [CrossRef]
- Krok, D.; Telka, E. Spousal support and illness acceptance in breast cancer patients: The mediating function of meaning in life and sense of coherence. Fam. Forum 2022, 12, 271–292. [Google Scholar] [CrossRef]
- Ying, Y.W.; Lee, P.A.; Tsai, J.L. Attachment, sense of coherence, and mental health among Chinese American college students: Variation by migration status. Int. J. Intercult. Relat. 2007, 31, 531–544. [Google Scholar] [CrossRef]
- Antonovksy, A. Unraveling the Mystery of Health: How People Manage Stress and Stay Well; Jossey-Bass: San Francisco, CA, USA, 1987. [Google Scholar]
- Ying, Y.W.; Lee, P.A.; Tsai, J.L. Predictors of depressive symptoms in Chinese American college students: Parent and peer attachment, college challenges and sense of coherence. Am. J. Orthopsychiatry 2007, 77, 316–323. [Google Scholar] [CrossRef]
- Plopa, M. Kwestionariusz Stylów Przywiązaniowych (KSP) [The Attachment Styles Questionnaire]; Pracownia Testów Psychologicznych: Warszawa, Poland, 2008. [Google Scholar]
- Ainsworth, M.D.S. The Bowlby-Ainsworth attachment theory. Behav. Brain Sci. 1978, 1, 436–438. [Google Scholar] [CrossRef]
- Antonovsky, A. The structure and properties of the sense of coherence scale. Soc. Sci. Med. 1993, 36, 725–733. [Google Scholar] [CrossRef] [PubMed]
- Janowski, K.; Steuden, S.; Pietrzak, A.; Krasowska, D.; Kaczmarek, Ł.; Gradus, I.; Chodorowska, G. Social support and adaptation to the disease in men and women with psoriasis. Arch. Dermatol. Res. 2012, 304, 421–432. [Google Scholar] [CrossRef]
- Soper, D.S. A-Priori Sample Size Calculator for Structural Equation Models. Available online: https://www.danielsoper.com/statcalc/calculator.aspx?id=89 (accessed on 25 July 2024).
- Westland, J.C. Lower bounds on sample size in structural equation modeling. Electron. Commer. Res. Appl. 2010, 9, 476–487. [Google Scholar] [CrossRef]
- Hayes, A.F.; Preacher, K.J. Conditional process modeling: Using structural equation modeling to examine contingent causal processes. In Structural Equation Modeling: A Second Course, 2nd ed.; Hancock, G.R., Mueller, R.O., Eds.; IAP Information Age Publishing: Charlotte, NC, USA, 2013; pp. 219–266. [Google Scholar]
- Cassidy, T.; McLaughlin, M. Caring for a child with cancer: The role of attachment, self-compassion and social support. Child Care Pract. 2024, 30, 305–317. [Google Scholar] [CrossRef]
- Snyder, K.S.; Luchner, A.F.; Tantleff-Dunn, S. Adverse childhood experiences and insecure attachment: The indirect effects of dissociation and emotion regulation difficulties. Psychol. Trauma 2024, 16 (Suppl. 1), 20–27. [Google Scholar] [CrossRef]
- Krok, D.; Telka, E.; Kocur, D. Perceived and received social support and illness acceptance among breast cancer patients: The serial mediation of meaning-making and fear of recurrence. Ann. Behav. Med. 2024, 58, 147–155. [Google Scholar] [CrossRef]
- Leo, K.; Langer, S.L.; Porter, L.S.; Ramos, K.; Romano, J.M.; Baucom, D.H.; Baucom, B.R. Couples communication and cancer: Sequences and trajectories of behavioral affective processes in relation to intimacy. J. Fam. Psychol. 2024, 38, 246–256. [Google Scholar] [CrossRef]
- Asaba, K.; Okawa, A. Moderating effect of sense of coherence on the relationship between symptom distress and health-related quality of life in patients receiving cancer chemotherapy. Support Care Cancer 2021, 29, 4651–4662. [Google Scholar] [CrossRef]
- Chen, M.; Gong, J.; Cao, Q.; Luo, X.; Li, J.; Li, Q. A literature review of the relationship between dyadic coping and dyadic outcomes in cancer couples. Eur. J. Oncol. Nurs. 2021, 54, 102035. [Google Scholar] [CrossRef]
- George-Levi, S.; Vilchinsky, N.; Tolmacz, R.; Khaskiaa, A.; Mosseri, M.; Hod, H. “It takes two to take”: Caregiving style, relational entitlement, and medication adherence. J. Fam. Psychol. 2016, 30, 743–751. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
| Variables | 1. | 2. | 3. | 4. | 5. | 6. | 7. | 8. |
|---|---|---|---|---|---|---|---|---|
| 1. Secure attachment | – | −0.53 *** | −0.44 *** | 0.18 * | 0.24 ** | 0.20 ** | 0.24 ** | 0.37 *** |
| 2. Avoidant attachment | −0.40 *** | – | 0.48 *** | −0.19 * | −0.23 ** | −0.23 ** | −0.24 ** | −0.30 *** |
| 3. Anxious attachment | −0.39 *** | 0.44 *** | – | −0.35 *** | −0.37 *** | −0.29 *** | −0.39 *** | −0.30 *** |
| 4. Comprehensibility | 0.25 *** | −0.15 | −0.29 *** | – | 0.68 *** | 0.49 *** | 0.86 *** | 0.35 *** |
| 5. Manageability | 0.19 * | −0.25 *** | −0.32 *** | 0.70 *** | – | 0.73 *** | 0.89 *** | 0.41 *** |
| 6. Meaningfulness | 0.25 *** | −0.19 * | −0.16 * | 0.56 *** | 0.63 *** | – | 0.82 *** | 0.44 *** |
| 7. Sense of coherence | 0.26 *** | −0.22 ** | −0.30 *** | 0.89 *** | 0.89 *** | 0.80 *** | − | 0.45 *** |
| 8. Illness acceptance | 0.30 *** | −0.19 * | −0.17 * | 0.40 *** | 0.47 *** | 0.51 ** | 0.52 *** | − |
| Patients’ mean (SD) | 6.00 (0.86) | 1.79 (0.89) | 2.69 (1.06) | 4.39 (0.81) | 5.24 (0.81) | 5.56 (0.83) | 5.01 (0.71) | 3.42 (0.66) |
| Spouses’ mean (SD) | 6.14 (0.67) | 1.67 (0.81) | 2.83 (1.05) | 4.23 (0.89) | 5.04 (0.82) | 5.64 (0.76) | 4.90 (0.73) | 3.53 (0.60) |
| Effect Type | Model Pathways | Estimate | 95% CI |
|---|---|---|---|
| Actor–actor effects Actor–partner effects | PT secure attachment → PT sense of coherence → PT illness acceptance | 0.09 | (0.04, 0.16) |
| PT avoidant attachment → PT sense of coherence → PT illness acceptance | −0.09 | (−0.15, −0.04) | |
| PT anxious attachment → PT sense of coherence → PT illness acceptance | −0.17 | (−0.25, −0.10) | |
| PT anxious attachment → SP sense of coherence → PT illness acceptance | −0.15 | (−0.21, −0.11) | |
| SP secure attachment → SP sense of coherence → SP illness acceptance | 0.11 | (0.05, 0.19) | |
| SP avoidant attachment → SP sense of coherence → SP illness acceptance | −0.11 | (−0.20, −0.03) | |
| SP anxious attachment → SP sense of coherence → SP illness acceptance | −0.14 | (−0.22, −0.07) | |
| PT secure attachment → PT sense of coherence → SP illness acceptance | 0.03 | (0.01, 0.07) | |
| SP avoidant attachment → SP sense of coherence → PT illness acceptance | −0.03 | (−0.07, −0.01) | |
| PT anxious attachment → SP sense of coherence → SP illness acceptance | −0.07 | (−0.14, −0.01) | |
| SP anxious attachment → SP sense of coherence → PT illness acceptance | −0.04 | (−0.08, −0.01) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Krok, D.; Telka, E.; Moroń, M. Dyadic Effects of Attachment on Illness Acceptance in Patients with Breast Cancer and Spousal Caregivers: Sense of Coherence as a Mediator. J. Clin. Med. 2024, 13, 6425. https://doi.org/10.3390/jcm13216425
Krok D, Telka E, Moroń M. Dyadic Effects of Attachment on Illness Acceptance in Patients with Breast Cancer and Spousal Caregivers: Sense of Coherence as a Mediator. Journal of Clinical Medicine. 2024; 13(21):6425. https://doi.org/10.3390/jcm13216425
Chicago/Turabian StyleKrok, Dariusz, Ewa Telka, and Marcin Moroń. 2024. "Dyadic Effects of Attachment on Illness Acceptance in Patients with Breast Cancer and Spousal Caregivers: Sense of Coherence as a Mediator" Journal of Clinical Medicine 13, no. 21: 6425. https://doi.org/10.3390/jcm13216425
APA StyleKrok, D., Telka, E., & Moroń, M. (2024). Dyadic Effects of Attachment on Illness Acceptance in Patients with Breast Cancer and Spousal Caregivers: Sense of Coherence as a Mediator. Journal of Clinical Medicine, 13(21), 6425. https://doi.org/10.3390/jcm13216425