
Optic Nerve Head and Retinal Changes in Idiopathic Intracranial Hypertension: Correlation with Short-Term Cerebrospinal Fluid Pressure Monitoring

 ,
, 
 ,
,  ,
,  , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Inclusion Criteria
- Clinical evidence suggestive of IIH with or without papilledema:
- -
- High-frequency headache attacks persisting for at least one year refractory to prophylactic therapy;
- -
- High-frequency headache attacks with papilledema, or transient or persistent visual obscuration, and/or blurred vision, or diplopia.
- Normal neurological examination.
- Evidence of bilateral stenosis of the cerebral transverse sinus at MRV [25].
2.2. Exclusion Criteria
- Evidence of central nervous system disease at brain MRI.
- Evidence of current or previous cerebral venous thrombosis revealed by cerebral MRV.
- Treatment with psychoactive, antihypertensive, cardiac, or other drugs interfering with the CSF pressure.
- Comorbidities such as diabetes mellitus, hypertension, cardiovascular and renal diseases, neurological diseases (i.e., tumors, ictus, infectious diseases, epilepsy, multiple sclerosis, previous head or eye injury).
- Eyes with optic disc and retinal pathology (including anterior ischemic optic neuropathy, posterior uveitis, and central retinal vein occlusion), which could bias measurements, and eyes affected by corneal opacity or cataract for which OCT imaging could not be obtained were ruled out from the analysis.
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Headache Classification Committee of the International Headache Society. The International Classification of Headache Disorders, 3rd edition (beta version). Cephalalgia 2013, 33, 629–808. [Google Scholar] [CrossRef] [PubMed]
- Friedman, D.I.; Jacobson, D.M. Diagnostic criteria for idiopathic intracranial hypertension. Neurology 2002, 59, 1492–1495. [Google Scholar] [CrossRef]
- Wang, M.T.; Bhatti, M.T.; Danesh-Meyer, H.V. Idiopathic intracranial hypertension: Pathophysiology, diagnosis and management. J. Clin. Neurosci. 2022, 95, 172–179. [Google Scholar] [CrossRef] [PubMed]
- Raoof, N.; Hoffmann, J. Diagnosis and treatment of idiopathic intracranial hypertension. Cephalalgia 2021, 41, 472–478. [Google Scholar] [CrossRef] [PubMed]
- Caballero, B. The global epidemic of obesity: An overview. Epidemiol. Rev. 2007, 29, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.N.P.; Gillard, J.H.; Owler, B.K.; Harkness, K.; Pickard, J.D. MR venography in idiopathic intracranial hypertension: Unappreciated and misunderstood. J. Neurol. Neurosurg. Psychiatry 2004, 75, 621–625. [Google Scholar] [CrossRef] [PubMed]
- Fera, F.; Bono, F.; Messina, D.; Gallo, O.; Lanza, P.L.; Auteri, W.; Nicoletti, G.; Santoro, G.; Quattrone, A. Comparison of different MR venography techniques for detecting transverse sinus stenosis in idiopathic intracranial hypertension. J. Neurol. 2005, 252, 1021–1025. [Google Scholar] [CrossRef]
- Digre, K.B. Not so benign intracranial hypertension. BMJ 2003, 326, 613–614. [Google Scholar] [CrossRef]
- Kanagalingam, S.; Subramanian, P.S. Update on Idiopathic Intracranial Hypertension. Curr. Treat. Options Neurol. 2018, 20, 24. [Google Scholar] [CrossRef]
- Wang, S.J.; Silberstein, S.D.; Patterson, S.; Young, W.B. Idiopathic intracranial hypertension without papilledema: A case-control study in a headache center. Neurology 1998, 51, 245–249. [Google Scholar]
- Mathew, N.T.; Ravishankar, K.; Sanin, L.C. Coexistence of migraine and idiopathic intracranial hypertension without papilledema. Neurology 1996, 46, 1226–1230. [Google Scholar] [CrossRef]
- Favoni, V.; Pierangeli, G.; Toni, F.; Cirillo, L.; La Morgia, C.; Abu-Rumeileh, S.; Messia, M.; Agati, R.; Cortelli, P.; Cevoli, S. Idiopathic Intracranial Hypertension Without Papilledema (IIHWOP) in Chronic Refractory Headache. Front. Neurol. 2018, 9, 503. [Google Scholar] [CrossRef] [PubMed]
- Mollan, S.P.; Chong, Y.J.; Grech, O.; Sinclair, A.J.; Wakerley, B.R. Current Perspectives on Idiopathic Intracranial Hypertension without Papilloedema. Life 2021, 11, 472. [Google Scholar] [CrossRef]
- Toscano, S.; Fermo, S.L.; Reggio, E.; Chisari, C.G.; Patti, F.; Zappia, M. An update on idiopathic intracranial hypertension in adults: A look at pathophysiology, diagnostic approach and management. J. Neurol. 2021, 268, 3249–3268. [Google Scholar] [CrossRef] [PubMed]
- Liguori, C.; Romigi, A.; Albanese, M.; Marciani, M.G.; Placidi, F.; Friedman, D.; Digre, K.; Liu, G. Revised diagnostic criteria for the pseudotumor cerebri syndrome in adults and children. Neurology 2014, 82, 1752–1753. [Google Scholar] [CrossRef] [PubMed]
- Xie, J.S.; Donaldson, L.; Margolin, E.A. Swelling of Atrophic Optic Discs in Idiopathic Intracranial Hypertension. J. Neuroophthalmol. 2023. [Google Scholar] [CrossRef]
- Albrecht, P.; Blasberg, C.; Ringelstein, M.; Müller, A.-K.; Finis, D.; Guthoff, R.; Kadas, E.-M.; Lagreze, W.; Aktas, O.; Hartung, H.-P.; et al. Optical coherence tomography for the diagnosis and monitoring of idiopathic intracranial hypertension. J. Neurol. 2017, 264, 1370–1380. [Google Scholar] [CrossRef]
- Huang-Link, Y.-M.; Al-Hawasi, A.; Oberwahrenbrock, T.; Jin, Y.-P. OCT measurements of optic nerve head changes in idiopathic intracranial hypertension. Clin. Neurol. Neurosurg. 2015, 130, 122–127. [Google Scholar] [CrossRef]
- Kaufhold, F.; Kadas, E.M.; Schmidt, C.; Kunte, H.; Hoffmann, J.; Zimmermann, H.; Oberwahrenbrock, T.; Harms, L.; Polthier, K.; Brandt, A.U.; et al. Optic nerve head quantification in idiopathic intracranial hypertension by spectral domain OCT. PLoS ONE 2012, 7, e36965. [Google Scholar] [CrossRef]
- Anand, A.; Pass, A.; Urfy, M.Z.; Tang, R.; Cajavilca, C.; Calvillo, E.; Suarez, J.I.; Rao, C.P.V.; Bershad, E.M. Optical coherence tomography of the optic nerve head detects acute changes in intracranial pressure. J. Clin. Neurosci. 2016, 29, 73–76. [Google Scholar] [CrossRef]
- Ahuja, S.; Anand, D.; Dutta, T.; Kumar, V.R.; Kar, S.S. Retinal nerve fiber layer thickness analysis in cases of papilledema using optical coherence tomography—A case control study. Clin. Neurol. Neurosurg. 2015, 136, 95–99. [Google Scholar] [CrossRef] [PubMed]
- Thaller, M.; Homer, V.; Hyder, Y.; Yiangou, A.; Liczkowski, A.; Fong, A.W.; Virdee, J.; Piccus, R.; Roque, M.; Mollan, S.P.; et al. The idiopathic intracranial hypertension prospective cohort study: Evaluation of prognostic factors and outcomes. J. Neurol. 2023, 270, 851–863. [Google Scholar] [CrossRef] [PubMed]
- Nichani, P.; Micieli, J.A. Retinal Manifestations of Idiopathic Intracranial Hypertension. Ophthalmol. Retina 2021, 5, 429–437. [Google Scholar] [CrossRef] [PubMed]
- Rizzo, J.L.; Lam, K.V.B.; Wall, M.; Wilson, M.D.; Keltner, J.L. Perimetry, retinal nerve fiber layer thickness and papilledema grade after cerebrospinal fluid shunting in patients with idiopathic intracranial hypertension. J. Neuroophthalmol. 2015, 35, 22–25. [Google Scholar] [CrossRef] [PubMed]
- Bono, F.; Cristiano, D.; Mastrandrea, C.; Latorre, V.; D’Asero, S.; Salvino, D.; Fera, F.; Lavano, A.; Quattrone, A. The upper limit of normal CSF opening pressure is related to bilateral transverse sinus stenosis in headache sufferers. Cephalalgia 2010, 30, 145–151. [Google Scholar] [CrossRef] [PubMed]
- Tewarie, P.; Balk, L.; Costello, F.; Green, A.; Martin, R.; Schippling, S.; Petzold, A. The OSCAR-IB consensus criteria for retinal OCT quality assessment. PLoS ONE 2012, 7, e34823. [Google Scholar] [CrossRef] [PubMed]
- Schippling, S.; Balk, L.; Costello, F.; Albrecht, P.; Balcer, L.; Calabresi, P.; Frederiksen, J.; Frohman, E.; Green, A.; Klistorner, A.; et al. Quality control for retinal OCT in multiple sclerosis: Validation of the OSCAR-IB criteria. Mult. Scler. J. 2015, 21, 163–170. [Google Scholar] [CrossRef]
- Cruz-Herranz, A.; Balk, L.J.; Oberwahrenbrock, T.; Saidha, S.; Martinez-Lapiscina, E.H.; Lagreze, W.A.; Schuman, J.S.; Villoslada, P.; Calabresi, P.; Balcer, L.; et al. The APOSTEL recommendations for reporting quantitative optical coherence tomography studies. Neurology 2016, 86, 2303–2309. [Google Scholar] [CrossRef]
- Bono, F.; Salvino, D.; Tallarico, T.; Cristiano, D.; Condino, F.; Fera, F.; Lanza, P.; Lavano, A.; Quattrone, A. Abnormal pressure waves in headache sufferers with bilateral transverse sinus stenosis. Cephalalgia 2010, 30, 1419–1425. [Google Scholar] [CrossRef]
- Eide, P.K.; Brean, A. Lumbar cerebrospinal fluid pressure waves versus intracranial pressure waves in idiopathic normal pressure hydrocephalus. Br. J. Neurosurg. 2006, 20, 407–414. [Google Scholar] [CrossRef]
- Eide, P.K.; Kerty, E. Static and pulsatile intracranial pressure in idiopathic intracranial hypertension. Clin. Neurol. Neurosurg. 2011, 113, 123–128. [Google Scholar] [CrossRef] [PubMed]
- Boston, R.C.; Sumner, A.E. STATA: A statistical analysis system for examining biomedical data. Adv. Exp. Med. Biol. 2003, 537, 353–369. [Google Scholar] [PubMed]
- Skau, M.; Yri, H.; Sander, B.; Gerds, T.A.; Milea, D.; Jensen, R. Diagnostic value of optical coherence tomography for intracranial pressure in idiopathic intracranial hypertension. Graefes Arch. Clin. Exp. Ophthalmol. 2013, 251, 567–574. [Google Scholar] [CrossRef] [PubMed]
- Yri, H.M.; Wegener, M.; Sander, B.; Jensen, R. Idiopathic intracranial hypertension is not benign: A long-term outcome study. J. Neurol. 2012, 259, 886–894. [Google Scholar] [CrossRef] [PubMed]
- Jensen, R.H.; Radojicic, A.; Yri, H. The diagnosis and management of idiopathic intracranial hypertension and the associated headache. Ther. Adv. Neurol. Disord. 2016, 9, 317–326. [Google Scholar] [CrossRef] [PubMed]
- Tariq, Y.M.; Li, H.; Burlutsky, G.; Mitchell, P. Retinal nerve fiber layer and optic disc measurements by spectral domain OCT: Normative values and associations in young adults. Eye 2012, 26, 1563–1570. [Google Scholar] [CrossRef]
- Rebolleda, G.; Muñoz-Negrete, F.J. Munoz-Negrete, Follow-up of mild papilledema in idiopathic intracranial hypertension with optical coherence tomography. Investig. Ophthalmol. Vis. Sci. 2009, 50, 5197–5200. [Google Scholar] [CrossRef]
- Savini, G.; Bellusci, C.; Carbonelli, M.; Zanini, M.; Carelli, V.; Sadun, A.A.; Barboni, P. Detection and quantification of retinal nerve fiber layer thickness in optic disc edema using stratus OCT. Arch. Ophthalmol. 2006, 124, 1111–1117. [Google Scholar] [CrossRef]
- Heckmann, J.; Weber, M.; Jünemann, A.; Neundörfer, B.; Mardin, C. Laser scanning tomography of the optic nerve vs CSF opening pressure in idiopathic intracranial hypertension. Neurology 2004, 62, 1221–1223. [Google Scholar] [CrossRef]
- Tang, L.; Kardon, R.H.; Wang, J.-K.; Garvin, M.K.; Lee, K.; Abràmoff, M.D. Quantitative evaluation of papilledema from stereoscopic color fundus photographs. Investig. Ophthalmol. Vis. Sci. 2012, 53, 4490–4497. [Google Scholar] [CrossRef]
- Malhotra, K.; Padungkiatsagul, T.; Moss, H.E. Optical coherence tomography use in idiopathic intracranial hypertension. Ann. Eye Sci. 2020, 5, 7. [Google Scholar] [CrossRef]
- Carey, A.R.; Bosley, T.M.; Miller, N.R.; McCulley, T.J.; Henderson, A.D. Use of En Face Optical Coherence Tomography to Monitor Papilledema in Idiopathic Intracranial Hypertension: A Pilot Study. J. Neuroophthalmol. 2021, 41, 212–216. [Google Scholar] [CrossRef] [PubMed]
- Donnelly, S.J.; Subramanian, P.S. Relationship of intraocular pulse pressure and spontaneous venous pulsations. Am. J. Ophthalmol. 2009, 147, 51–55. [Google Scholar] [CrossRef] [PubMed]
- Bering, E.A., Jr. Circulation of the cerebrospinal fluid. Demonstration of the choroid plexuses as the generator of the force for flow of fluid and ventricular enlargement. J. Neurosurg. 1962, 19, 405–413. [Google Scholar] [CrossRef] [PubMed]
- Portnoy, H.D. The CSF pulse wave in hydrocephalus. Childs Nerv. Syst. 1986, 2, 107–108. [Google Scholar] [CrossRef]
- Yada, K.; Nakagawa, Y.; Tsuru, M. Circulatory disturbance of the venous system during experimental intracranial hypertension. J. Neurosurg. 1973, 39, 723–729. [Google Scholar] [CrossRef]
- Marmarou, A.; Shulman, K.; LaMorgese, J. Compartmental analysis of compliance and outflow resistance of the cerebrospinal fluid system. J. Neurosurg. 1975, 43, 523–534. [Google Scholar] [CrossRef]
- Giliberto, C.; Mostile, G.; Fermo, S.L.; Reggio, E.; Sciacca, G.; Nicoletti, A.; Zappia, M. Vascular parkinsonism or idiopathic NPH? New insights from CSF pressure analysis. Neurol. Sci. 2017, 38, 2209–2212. [Google Scholar] [CrossRef]
- Abegg, M.; Fleischhauer, J.; Landau, K. Unilateral papilledema after trabeculectomy in a patient with intracranial hypertension. Klin. Monbl Augenheilkd. 2008, 225, 441–442. [Google Scholar] [CrossRef]
- Killer, H.E.; Jaggi, G.P.; Flammer, J.; Miller, N.R.; Huber, A.R.; Mironov, A. Cerebrospinal fluid dynamics between the intracranial and the subarachnoid space of the optic nerve. Is. it always bidirectional? Brain 2007, 130 Pt 2, 514–520. [Google Scholar] [CrossRef]
- Von Hanno, T.; Hareide, L.L.; Småbrekke, L.; Morseth, B.; Sneve, M.; Erke, M.G.; Mathiesen, E.B.; Bertelsen, G. Macular Layer Thickness and Effect of BMI, Body Fat, and Traditional Cardiovascular Risk Factors: The Tromso Study. Investig. Ophthalmol. Vis. Sci. 2022, 63, 16. [Google Scholar] [CrossRef] [PubMed]
- Wong, A.C.M.; Chan, C.W.N.; Hui, S.P. Relationship of gender, body mass index, and axial length with central retinal thickness using optical coherence tomography. Eye 2005, 19, 292–297. [Google Scholar] [CrossRef] [PubMed]
- Szewka, A.J.; Bruce, B.B.; Newman, N.J.; Biousse, V. Idiopathic intracranial hypertension: Relation between obesity and visual outcomes. J. Neuroophthalmol. 2013, 33, 4–8. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
| IIHWP (n = 9) | IIHWOP (n = 7) | p Value | |
|---|---|---|---|
| Age (mean ± SD) | 28.5 ± 7.9 | 31.9 ± 10.4 | 0.5 |
| Female (%) | 5(55.5) | 4 (57.14) | - |
| BMI (mean ± SD) | 40.5 ± 4.3 | 32.9 ± 3.7 | 0.002 |
| Visual acuity (LogMAR) (mean ± SD) OD | 0.53 ± 0.21 | 0.061 ± 0.02 | 0.001 |
| OS | 0.51 ± 0.18 | 0.058 ± 0.03 | 0.001 |
| Intraocular pressure (mmhg) | |||
| (mean ± SD) | |||
| OD | 15.2 ± 2 | 13.3 ± 1.6 | 0.07 |
| OS | 13.7 ± 3.7 | 14.9 ± 4 | 0.08 |
| IIHWP | IIHWOP | p Value | |
|---|---|---|---|
| oCSFp (mmH2O) | 348.1 ± 50.4 | 222.2 ± 14.7 | 0.0001 |
| mCSFp (mmH2O) | 370.6 ± 51.4 | 251.6 ± 21.4 | 0.0001 |
| CSF PWA (mmH2O) | 171.2 ± 13.1 | 62.3 ± 13.2 | 0.0001 |
| IIHWP | IIHWOP | p Value | |
|---|---|---|---|
| (n = 9) | (n = 7) | ||
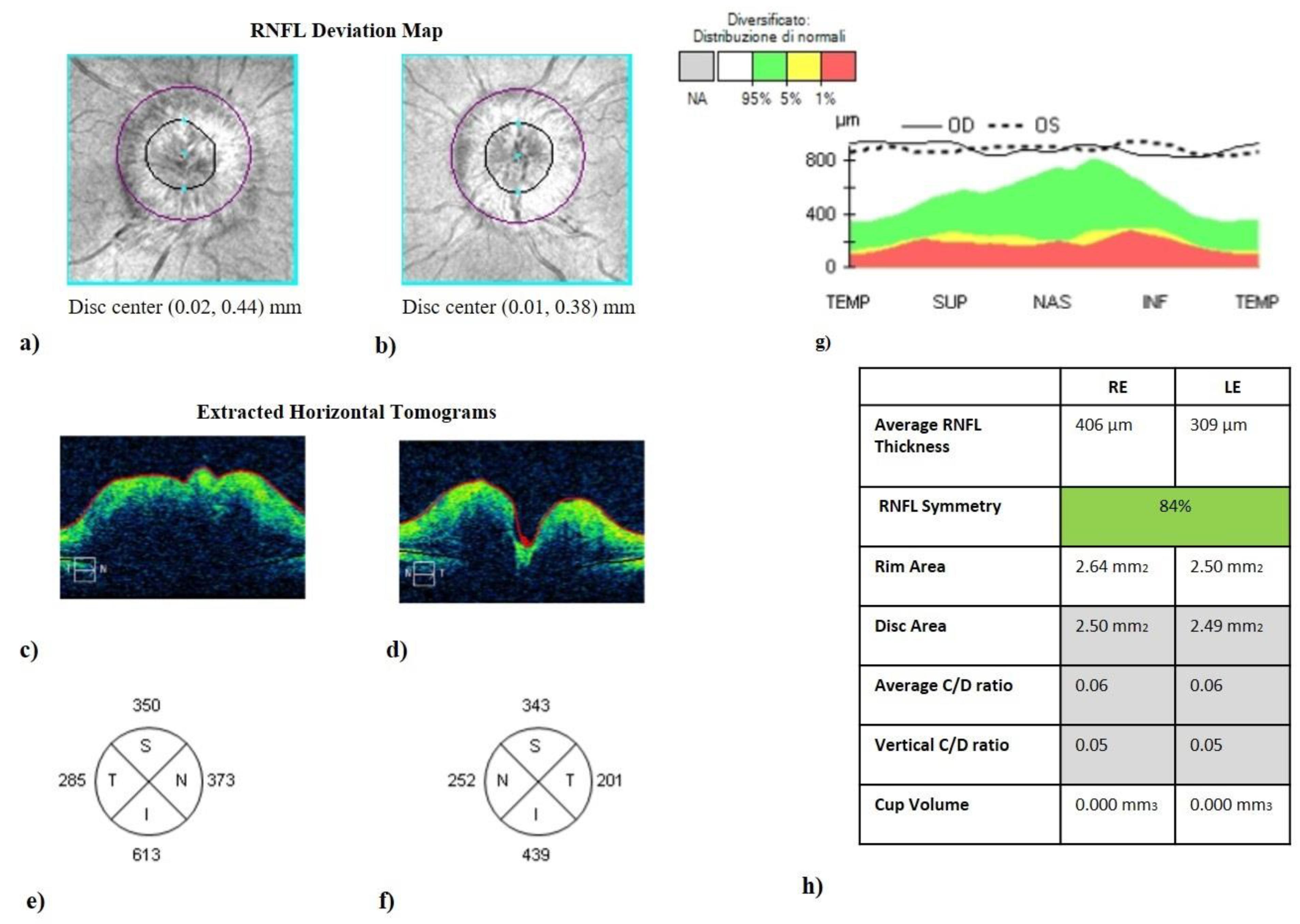
| RNFL (µm) | |||
| OD | 209.4 ± 88.8 | 98.5 ± 5.6 | 0.005 |
| OS | 166.6 ± 54.5 | 98.6 ± 2.3 | 0.006 |
| Superior sector (µm) | |||
| OD | 210.7 ± 95.0 | 119.6 ± 8.0 | 0.03 |
| OS | 177.2 ± 71.9 | 117.9 ± 7.2 | 0.05 |
| Inferior sector (µm) | |||
| OD | 234.2 ± 65.4 | 120.0 ± 9.9 | 0.01 |
| OS | 184.9 ± 53.9 | 123.3 ± 6.6 | 0.01 |
| Nasal sector (µm) | |||
| OD | 140.2 ± 64.3 | 81.7 ± 6.4 | 0.03 |
| OS | 127.1 ± 73.0 | 74.3 ± 6.7 | 0.05 |
| Temporal sector (µm) | |||
| OD | 126.3 ± 36.8 | 69.7 ± 8.3 | 0.001 |
| OS | 113.0 ± 33.0 | 66.4 ± 6.5 | 0.003 |
| Macular volume (µm) | |||
| OD | 10.2 ± 1.0 | 9.8 ± 0.4 | 0.3 |
| OS | 10.9 ± 1.1 | 9.9 ± 0.1 | 0.2 |
| Foveal thickness (µm) | |||
| OD | 253.1 ± 15.0 | 242.6 ± 13.4 | 0.2 |
| OS | 268.8 ± 17.8 | 255.6 ± 12.3 | 0.1 |
| Ganglion cell layer (µm) | |||
| OD | 80.0 ± 2.7 | 81.9 ± 4.8 | 0.3 |
| OS | 81.0 ± 3.5 | 82.6 ± 4.8 | 0.3 |
| C/D ratio | |||
| OD | 0.01 ± 0.03 | 0.06 ± 0.04 | 0.01 |
| OS | 0.02 ± 0.01 | 0.05 ± 0.03 | 0.01 |
| Rim thickness (µm) | |||
| OD | 757.2 ± 158.3 | 580.2 ± 127.4 | 0.03 |
| OS | 750.0 ± 142.5 | 577.8 ± 122.5 | 0.02 |
| Rim area (µm2) | |||
| OD | 1.7 ± 0.2 | 1.4 ± 0.2 | 0.01 |
| OS | 1.7 ± 0.1 | 1.4 ± 0.3 | 0.01 |
| Cup volume (µm3) | |||
| OD | 0.01 ± 0.04 | 0.07 ± 0.03 | 0.005 |
| OS | 0.02 ± 0.03 | 0.08 ± 0.01 | 0.005 |
| RNFL | C/D Ratio | Disc Area | Rim Thickness | Rim Area | Cup Volume | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| OD | OS | OD | OS | OD | OS | OD | OS | OD | OS | OD | OS | |
| oCSFp | 0.58 ° | 0.55 ° | −0.59 ° | −0.61 ° | 0.23 | 0.21 | 0.41 | 0.38 | 0.23 | 0.19 | −0.64 * | −0.63 * |
| mCSFp | 0.62 # | 0.60 # | −0.55 ° | −0.53 ° | 0.18 | 0.15 | 0.71 * | 0.68 * | 0.43 | 0.38 | −0.55 ° | −0.57 ° |
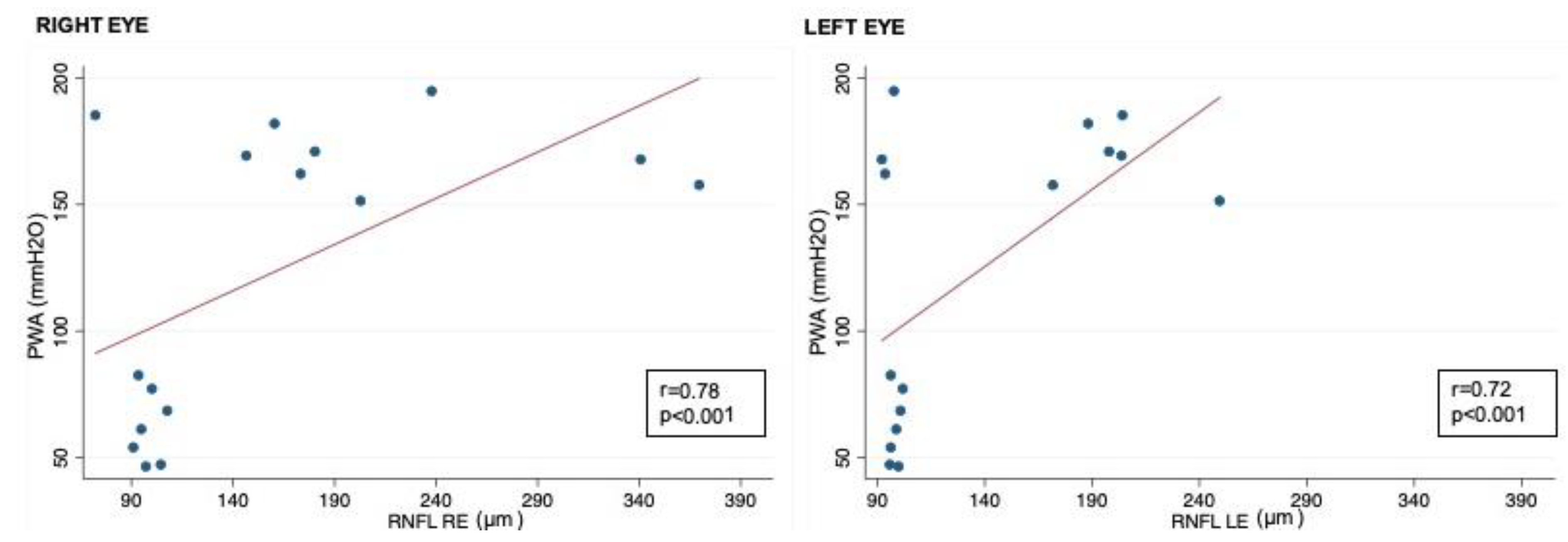
| CSFPWA | 0.78 * | 0.72 * | −0.65 # | −0.63 # | 0.17 | 0.16 | 0.72 * | 0.71 * | 0.41 | 0.40 | −0.78 * | −0.72 * |
| RNFL | C/D Ratio | Disc Area | Rim Thickness | Rim Area | Cup Volume | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| OD | OS | OD | OS | OD | OS | OD | OS | OD | OS | OD | OS | |
| VA OD | 0.74 * | / | −0.60 # | / | 0.19 | / | 0.33 | / | 0.21 | / | −0.65 * | |
| VA OS | / | 0.71 * | / | −0.61 # | / | 0.20 | / | 0.31 | / | 0.17 | −0.61 * | |
| oCSFp | mCSFp | CSF PWA | |
|---|---|---|---|
| VA OD | 0.40 | 0.64 # | 0.64 * |
| VA OS | 0.42 | 0.62 # | 0.66 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Toro, M.D.; Castellino, N.; Russo, A.; Scollo, D.; Avitabile, T.; Rejdak, R.; Rejdak, M.; Cimino, V.; Costagliola, C.; Carnevali, A.; et al. Optic Nerve Head and Retinal Changes in Idiopathic Intracranial Hypertension: Correlation with Short-Term Cerebrospinal Fluid Pressure Monitoring. J. Clin. Med. 2024, 13, 562. https://doi.org/10.3390/jcm13020562
Toro MD, Castellino N, Russo A, Scollo D, Avitabile T, Rejdak R, Rejdak M, Cimino V, Costagliola C, Carnevali A, et al. Optic Nerve Head and Retinal Changes in Idiopathic Intracranial Hypertension: Correlation with Short-Term Cerebrospinal Fluid Pressure Monitoring. Journal of Clinical Medicine. 2024; 13(2):562. https://doi.org/10.3390/jcm13020562
Chicago/Turabian StyleToro, Mario Damiano, Niccolò Castellino, Andrea Russo, Davide Scollo, Teresio Avitabile, Robert Rejdak, Magdalena Rejdak, Vincenzo Cimino, Ciro Costagliola, Adriano Carnevali, and et al. 2024. "Optic Nerve Head and Retinal Changes in Idiopathic Intracranial Hypertension: Correlation with Short-Term Cerebrospinal Fluid Pressure Monitoring" Journal of Clinical Medicine 13, no. 2: 562. https://doi.org/10.3390/jcm13020562
APA StyleToro, M. D., Castellino, N., Russo, A., Scollo, D., Avitabile, T., Rejdak, R., Rejdak, M., Cimino, V., Costagliola, C., Carnevali, A., & Chisari, C. G. (2024). Optic Nerve Head and Retinal Changes in Idiopathic Intracranial Hypertension: Correlation with Short-Term Cerebrospinal Fluid Pressure Monitoring. Journal of Clinical Medicine, 13(2), 562. https://doi.org/10.3390/jcm13020562