

Retrograde Cricopharyngeal Dysfunction: A Review


{kind=link}
{kind=link}
Abstract
1. Introduction
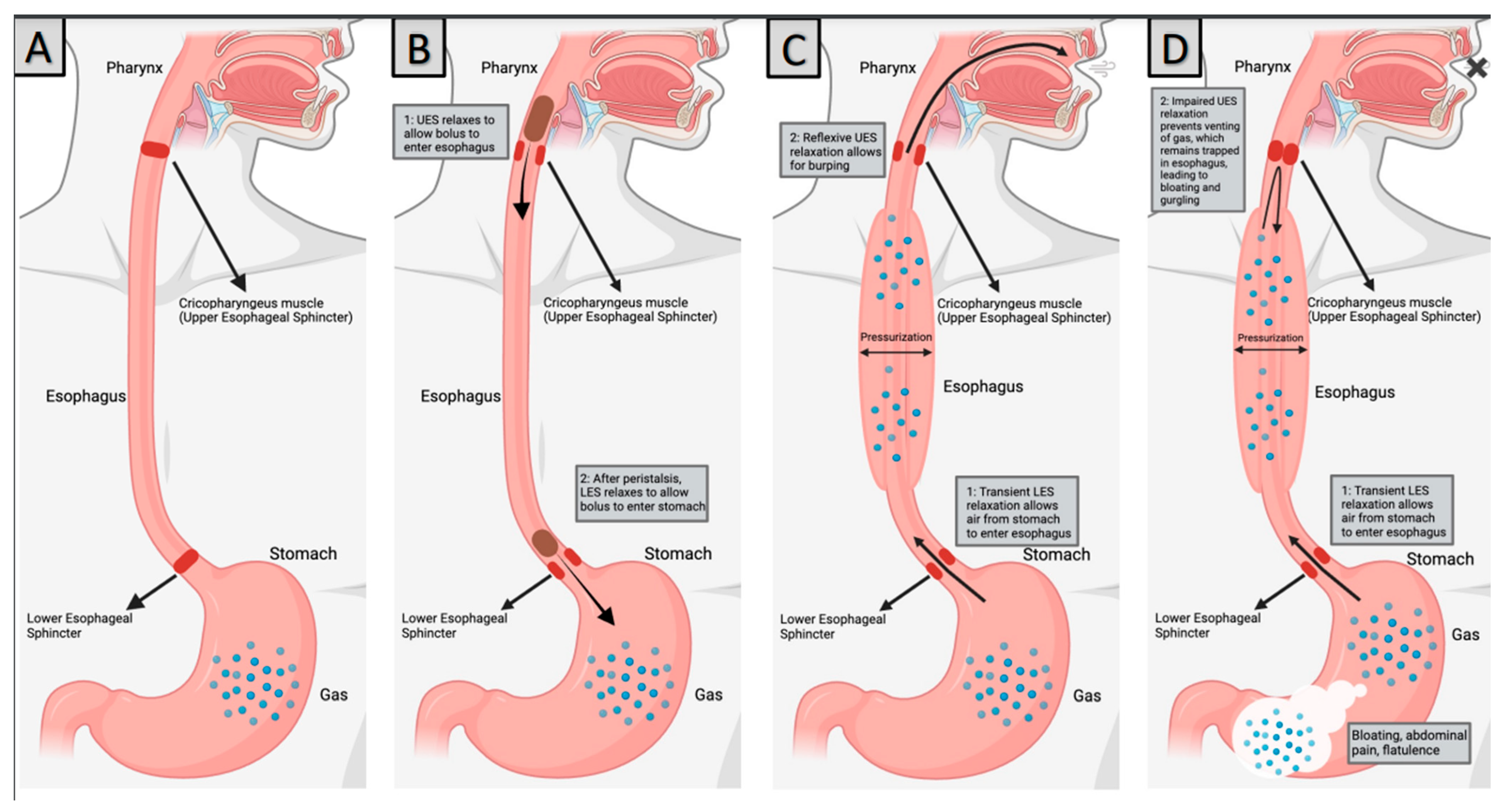
2. Pathophysiology
2.1. The Upper Esophageal Sphincter
2.2. Burping Reflex
2.3. The Role of Behavior?
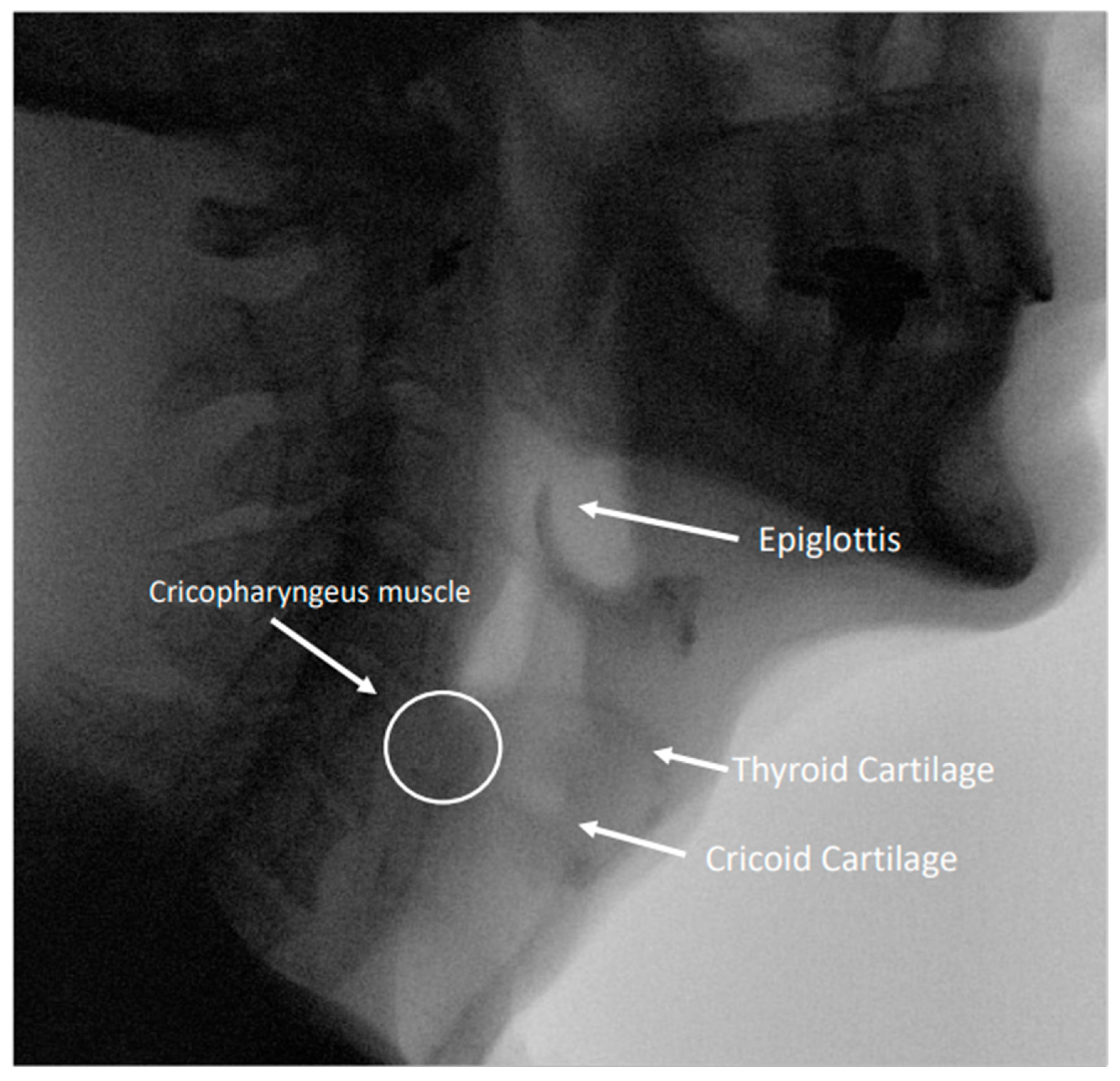
3. Diagnosis
4. Lived Experience of RCPD
5. Treatment
5.1. Botulinum Toxin Injections into the Cricopharyngeus Muscle
5.2. Cricopharyngeal Dilation
5.3. Myotomy
5.4. The Role of Speech–Language Pathologists
6. The Role of Social Media
7. Conclusions
8. Future Directions
Author Contributions
Funding
Conflicts of Interest
References
- Kahrilas, P.J.; Dodds, W.J.; Hogan, W.J. Dysfunction of the belch reflex. Gastroenterology 1987, 93, 818–822. [Google Scholar] [CrossRef]
- Bastian, R.W.; Smithson, M.L. Inability to Belch and Associated Symptoms Due to Retrograde Cricopharyngeus Dysfunction: Diagnosis and Treatment. OTO Open 2019, 3, 2473974X1983455. [Google Scholar] [CrossRef]
- Oude Nijhuis, R.A.B.; Snelleman, J.A.; Oors, J.M.; Kessing, B.F.; Heuveling, D.A.; Schuitenmaker, J.M.; ten Cate, L.; Smout, A.J.P.M.; Bredenoord, A.J. The inability to belch syndrome: A study using concurrent high-resolution manometry and impedance monitoring. Neurogastroenterol. Motil 2022, 34, e14250. [Google Scholar] [CrossRef] [PubMed]
- Karagama, Y. Abelchia: Inability to belch/burp—A new disorder? Retrograde cricopharyngeal dysfunction (RCPD). Eur. Arch. Otorhinolaryngol. 2021, 278, 5087–5091. [Google Scholar] [CrossRef] [PubMed]
- Hoffman, M.R.; Schiffer, B.; Patel, R.A.; Smith, M.E. “I’ve never been able to burp”: Preliminary description of retrograde cricopharyngeal dysfunction in children. Int. J. Pediatr. Otorhinolaryngol. 2022, 161, 111261. [Google Scholar] [CrossRef] [PubMed]
- Sato, H.; Ikarashi, S.; Terai, S. A Rare Case Involving the Inability to Belch. Intern. Med. 2019, 58, 929–931. [Google Scholar] [CrossRef]
- Bastian, R.W.; Hoesli, R.C. Partial Cricopharyngeal Myotomy for Treatment of Retrograde Cricopharyngeal Dysfunction. OTO Open 2020, 4, 2473974X2091764. [Google Scholar] [CrossRef]
- Siddiqui, S.H.; Sagalow, E.S.; Fiorella, M.A.; Jain, N.; Spiegel, J.R. Retrograde Cricopharyngeus Dysfunction: The Jefferson Experience. Laryngoscope 2022, 133, 1081–1085. [Google Scholar] [CrossRef]
- Kahrilas, P.J. Retrograde upper esophageal sphincter function… and dysfunction. Neurogastroenterol. Motil 2022, 34, e14328. [Google Scholar] [CrossRef]
- Lang, I.M.; Shaker, R. Anatomy and Physiology of the Upper Esophageal Sphincter. Am. J. Med. 1997, 103, 50S–55S. [Google Scholar] [CrossRef]
- Wei, P. Botulinum Toxin Injection for the Treatment of Upper Esophageal Sphincter Dysfunction. Toxins 2022, 14, 321. [Google Scholar] [CrossRef] [PubMed]
- Zaino, C.; Jacobson, H.G.; Lepow, H.; Ozturk, C. The pharyngoesophageal sphincter. Radiology 1967, 89, 639–645. [Google Scholar] [CrossRef]
- Adams, C.L.; Lohan, S.; Bruce, A.; Kamalaraj, N.; Gunaratne, S.; White, R. Cricopharyngeal bar and dermatomyositis: A cause of rapidly progressive dysphagia. Int. J. Rheum. Dis. 2021, 24, 125–131. [Google Scholar] [CrossRef] [PubMed]
- Taira, K.; Yamamoto, T.; Mori-Yoshimura, M.; Sajima, K.; Takizawa, H.; Shinmi, J.; Oya, Y.; Nishino, I.; Takahashi, Y. Cricopharyngeal bar on videofluoroscopy: High specificity for inclusion body myositis. J. Neurol. 2021, 268, 1016–1024. [Google Scholar] [CrossRef] [PubMed]
- Miwa, K.; Tsutsumi, M.; Fukino, K.; Eguchi, K.; Okada, R.; Akita, K. An anatomical study of the anterior wall of the hypopharyngeal and the cervical esophageal junction. Auris Nasus Larynx 2020, 47, 849–855. [Google Scholar] [CrossRef]
- Sivarao, D.V.; Goyal, R.K. Functional anatomy and physiology of the upper esophageal sphincter. Am. J. Med. 2000, 108 (Suppl. S4a), 27S–37S. [Google Scholar] [CrossRef]
- DiRe, C.; Shi, G.; Manka, M.; Kahrilas, P.J. Manometric Characteristics of the Upper Esophageal Sphincter Recorded With a Microsleeve. Am. J. Gastroenterol. 2001, 96, 1383–1389. [Google Scholar] [CrossRef]
- Nativ-Zeltzer, N.; Belafsky, P.C.; Bayoumi, A.; Kuhn, M.A. Volitional control of the upper esophageal sphincter with high-resolution manometry driven biofeedback. Laryngoscope Investig. Otolaryngol. 2019, 4, 264–268. [Google Scholar] [CrossRef]
- Kahrilas, P.J.; Dodds, W.J.; Dent, J.; Wyman, J.B.; Hogan, W.J.; Arndorfer, R.C. Upper esophageal sphincter function during belching. Gastroenterology 1986, 91, 133–140. [Google Scholar] [CrossRef]
- Pandolfino, J.E.; Ghosh, S.K.; Zhang, Q.; Han, A.; Kahrilas, P.J. Upper sphincter function during transient lower oesophageal sphincter relaxation (tLOSR); it is mainly about microburps. Neurogastroenterol. Motil. 2007, 19, 203–210. [Google Scholar] [CrossRef]
- Alotaibi, F.Z. Retrograde cricopharyngeal dysfunction (R-CPD): What do we know so far? World J. Otorhinolaryngol.-Head Neck Surg. 2023, wjo2.127. [Google Scholar] [CrossRef]
- Hoesli, R.C.; Wingo, M.L.; Bastian, R.W. The Long-term Efficacy of Botulinum Toxin Injection to Treat Retrograde Cricopharyngeus Dysfunction. OTO Open 2020, 4, 2473974X2093834. [Google Scholar] [CrossRef] [PubMed]
- Wajsberg, B.; Hoesli, R.C.; Wingo, M.L.; Bastian, R.W. Efficacy and Safety of Electromyography-Guided Injection of Botulinum Toxin to Treat Retrograde Cricopharyngeus Dysfunction. OTO Open 2021, 5, 2473974X2198958. [Google Scholar] [CrossRef]
- Miller, M.; Lina, I.; Akst, L. Experiences of Patients Living with Retrograde Cricopharyngeal Dysfunction. Laryngoscope 2023. [Google Scholar] [CrossRef]
- Chandrasekhara, V.; Koh, J.; Lattimer, L.; Dunbar, K.B.; Ravich, W.J.; Clarke, J.O. Endoscopic balloon catheter dilatation via retrograde or static technique is safe and effective for cricopharyngeal dysfunction. WJGE 2017, 9, 183. [Google Scholar] [CrossRef] [PubMed]
- Watson, N.A.; Siddiqui, Z.; Miller, B.J.; Karagama, Y.; Gibbins, N. Non-aesthetic uses of botulinum toxin in the head and neck. Eur. Arch. Otorhinolaryngol. 2021, 278, 4147–4154. [Google Scholar] [CrossRef] [PubMed]
- Doruk, C.; Pitman, M.J. Lateral Transcervical In-office Botulinum Toxin Injection for Retrograde Cricopharyngeal Dysfunction. Laryngoscope 2023, 134, 283–286. [Google Scholar] [CrossRef]
- Pavesi, L.; Balzano, C.; Mauramati, S.; Giudice, C.; Fresia, M.; Todisco, M.; Alfonsi, E.; Cosentino, G. Retrograde Cricopharyngeus Dysfunction effectively treated with low dose botulinum toxin. A case report from Italy. Front. Neurol. 2023, 14, 1238304. [Google Scholar] [CrossRef]
- Kelly, E.A.; Koszewski, I.J.; Jaradeh, S.S.; Merati, A.L.; Blumin, J.H.; Bock, J.M. Botulinum Toxin Injection for the Treatment of Upper Esophageal Sphincter Dysfunction. Ann. Otol. Rhinol. Laryngol. 2013, 122, 100–108. [Google Scholar] [CrossRef]
- Ertekin, C.; Aydogdu, I. Electromyography of human cricopharyngeal muscle of the upper esophageal sphincter. Muscle Nerve 2002, 26, 729–739. [Google Scholar] [CrossRef]
- Verhulst, J.; Amé, P.; Guatterie, M.; Barat, M.; Traissac, L. A retrospective study of 91 injections of botulinus toxin into the upper sphincter of the oesophagus. Rev. Laryngol. Otol. Rhinol. (Bord) 2003, 124, 315–320. [Google Scholar]
- Suzukia, Y.; Sano, N.; Shinonaga, C.; Fukuda, M.; Hyodo, M.; Morimoto, T. Successful botulinum toxin treatment of dysphagia in a spinal muscular atrophy type 2 patient. Brain Dev. 2007, 29, 662–665. [Google Scholar] [CrossRef] [PubMed]
- Restivo, D.A.; Marchese-Ragona, R.; Patti, F.; Solaro, C.; Maimone, D.; Zappalá, G.; Pavone, A. Botulinum toxin improves dysphagia associated with multiple sclerosis: BoNT/A for dysphagia in MS. Eur. J. Neurol. 2011, 18, 486–490. [Google Scholar] [CrossRef]
- Wei, P.; Xu, Y.; Zhang, Z.; Zhang, S.; Lv, Z. Treatment for upper esophageal sphincter dysfunction in a patient with poststroke dysphagia: A case report. Medicine 2019, 98, e14988. [Google Scholar] [CrossRef] [PubMed]
- Xie, M.; Wen, H.; Dou, Z. Case report: A case of novel treatment for retrograde cricopharyngeal dysfunction. Front. Neurol. 2022, 13, 1005655. [Google Scholar] [CrossRef]
- Ashman, A.; Dale, O.T.; Baldwin, D.L. Management of isolated cricopharyngeal dysfunction: Systematic review. J. Laryngol. Otol. 2016, 130, 611–615. [Google Scholar] [CrossRef] [PubMed]
- Jones, C.A.; Knigge, M.A.; McCulloch, T.M. Speech Pathologist Practice Patterns for Evaluation and Management of Suspected Cricopharyngeal Dysfunction. Dysphagia 2014, 29, 332–339. [Google Scholar] [CrossRef]
- Goldstein, A.N.; Paredes-Echeverri, S.; Finkelstein, S.A.; Guthrie, A.J.; Perez, D.L.; Freeburn, J.L. Speech and language therapy: A treatment case series of 20 patients with functional speech disorder. NRE 2023, 53, 227–238. [Google Scholar] [CrossRef]
- Anbar, R.D.; Spence, N.A. Hypnosis in the treatment of retrograde cricopharyngeus dysfunction: A case report. Am. J. Clin. Hypn. 2023. [Google Scholar] [CrossRef]
- Wajsberg, B.; Hoesli, R.C.; Wingo, M.L.; Richardson, B.E.; Bastian, R.W. Retrograde Cricopharyngeus Dysfunction: An Orphan Disease? Am. J. Gastroenterol. 2022, 117, 1539. [Google Scholar] [CrossRef]
- Moorhead, S.A.; Hazlett, D.E.; Harrison, L.; Carroll, J.K.; Irwin, A.; Hoving, C. A new dimension of health care: Systematic review of the uses, benefits, and limitations of social media for health communication. J. Med. Internet. Res. 2013, 15, e85. [Google Scholar] [CrossRef] [PubMed]
- Silver, J.A.; Roy, C.F.; Young, J.; Kost, K.M. Retrograde cricopharyngeus dysfunction: A Canadian experience fueled by social media. Ear Nose Throat J. 2023, 1455613231162203. [Google Scholar] [CrossRef]
- Verma, S.P.; Goshtasbi, K.; Berry, L.D.; Anderson, C.; Francis, D.O.; Gelbard, A. Utilization and Influence of Online Support Communities in Idiopathic Subglottic Stenosis Patients. Laryngoscope 2021, 131, 1821–1827. [Google Scholar] [CrossRef] [PubMed]
- Oh, L.; Phan, K.; Jufas, N.E.; Patel, N.P. Assessing the Quality of Patient Information for Vestibular Schwannoma on the Open Source Video Sharing Platform YouTube. Otol. Neurotol. 2022, 43, e316–e322. [Google Scholar] [CrossRef] [PubMed]
- Rossi, N.A.; French, K.R.; Evans, C.L.; Ohlstein, J.F.; Neve, L.D.; Daram, S.; Young, D.L.; McKinnon, B.J.; Pine, H.S. Trending Tubes: A Social Media Analysis of Tympanostomy Tubes in Children. OTO Open 2022, 6. [Google Scholar] [CrossRef]
- Rossi, N.A.; George, S.S.; Patel, K.P.; Reddy, D.N.; Ohlstein, J.F.; McKinnon, B.J.; Siddiqui, F.N.; Lees, K.A. Qualitative analysis of sinus surgery posts on popular social media platforms. Am. J. Otolaryngol. 2022, 43, 103388. [Google Scholar] [CrossRef]
- AlBahlal, A.; Alosaimi, N.; Bawadood, M.; AlHarbi, A.; AlSubhi, F. The Effect and Implication of Social Media Platforms on Plastic Cosmetic Surgery: A Cross-sectional Study in Saudi Arabia From 2021 to 2022. Aesthetic Surg. J. Open Forum 2023, 5, ojad002. [Google Scholar] [CrossRef]
- Moffatt, D.C.; Lahaye, J.J.; Corona, K.K.; Rossi, N.A.; Joshi, R.; Resto, V.; McKinnon, B.J.; Coblens, O.M. Laryngectomy: Social media analysis of patient perception. Head Neck 2023, 45, 464–472. [Google Scholar] [CrossRef]
- Reddy, R.; Cheng, H.; Jufas, N.; Patel, N. Assessing the Quality of Patient Information for Cholesteatoma on the Video Sharing Platform YouTube. Otol. Neurotol. 2023, 44, e230–e234. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Miller, M.E.; Lina, I.; Akst, L.M. Retrograde Cricopharyngeal Dysfunction: A Review. J. Clin. Med. 2024, 13, 413. https://doi.org/10.3390/jcm13020413
Miller ME, Lina I, Akst LM. Retrograde Cricopharyngeal Dysfunction: A Review. Journal of Clinical Medicine. 2024; 13(2):413. https://doi.org/10.3390/jcm13020413
Chicago/Turabian StyleMiller, Mattea E., Ioan Lina, and Lee M. Akst. 2024. "Retrograde Cricopharyngeal Dysfunction: A Review" Journal of Clinical Medicine 13, no. 2: 413. https://doi.org/10.3390/jcm13020413
APA StyleMiller, M. E., Lina, I., & Akst, L. M. (2024). Retrograde Cricopharyngeal Dysfunction: A Review. Journal of Clinical Medicine, 13(2), 413. https://doi.org/10.3390/jcm13020413