

Clinical Utility of Baseline Brain Natriuretic Peptide Levels on Health Status Outcomes after Catheter Ablation for Atrial Fibrillation in Individuals without Heart Failure

 , , , and
, , , and
Abstract
1. Introduction
2. Methods
2.1. Data Source
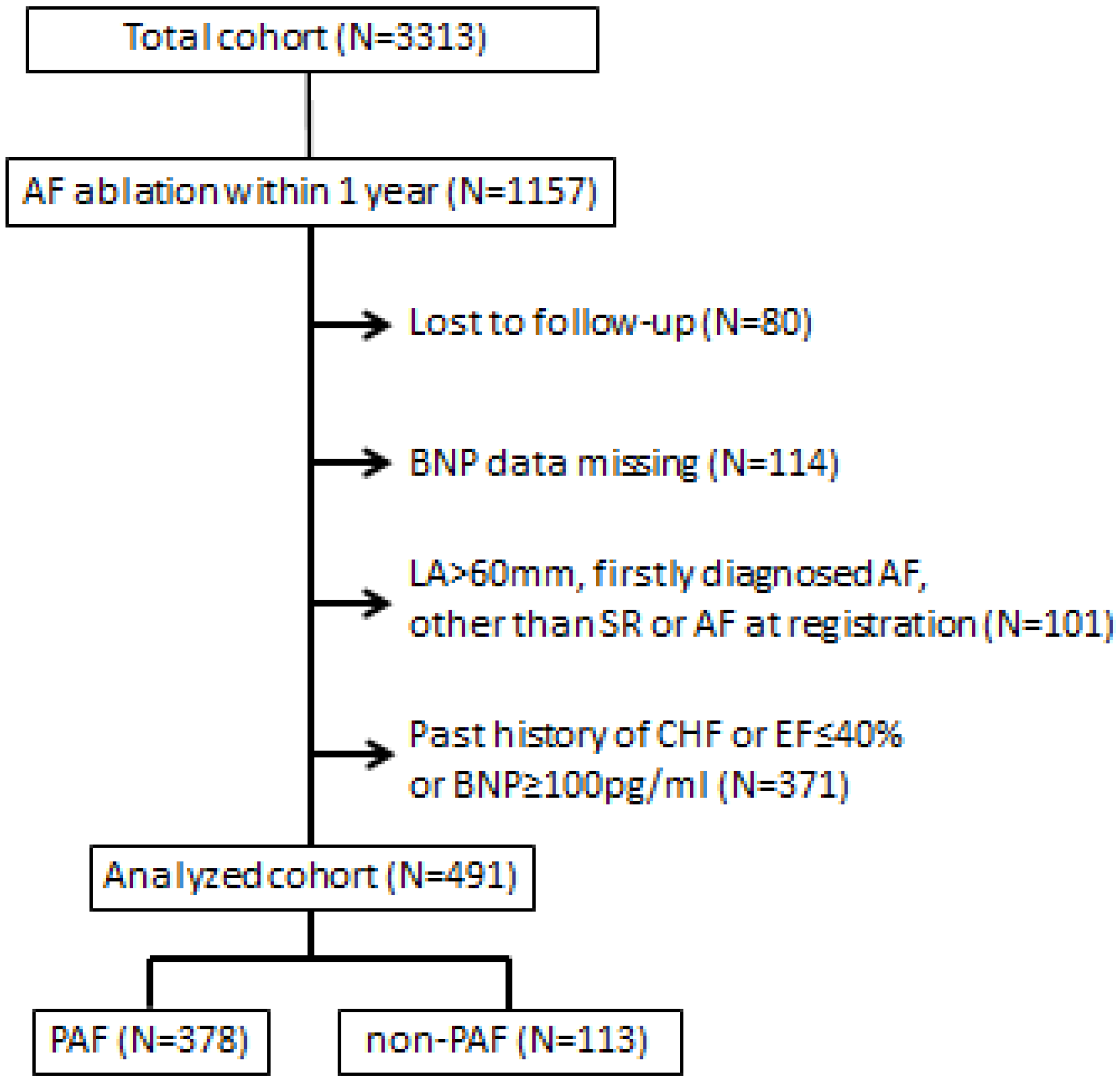
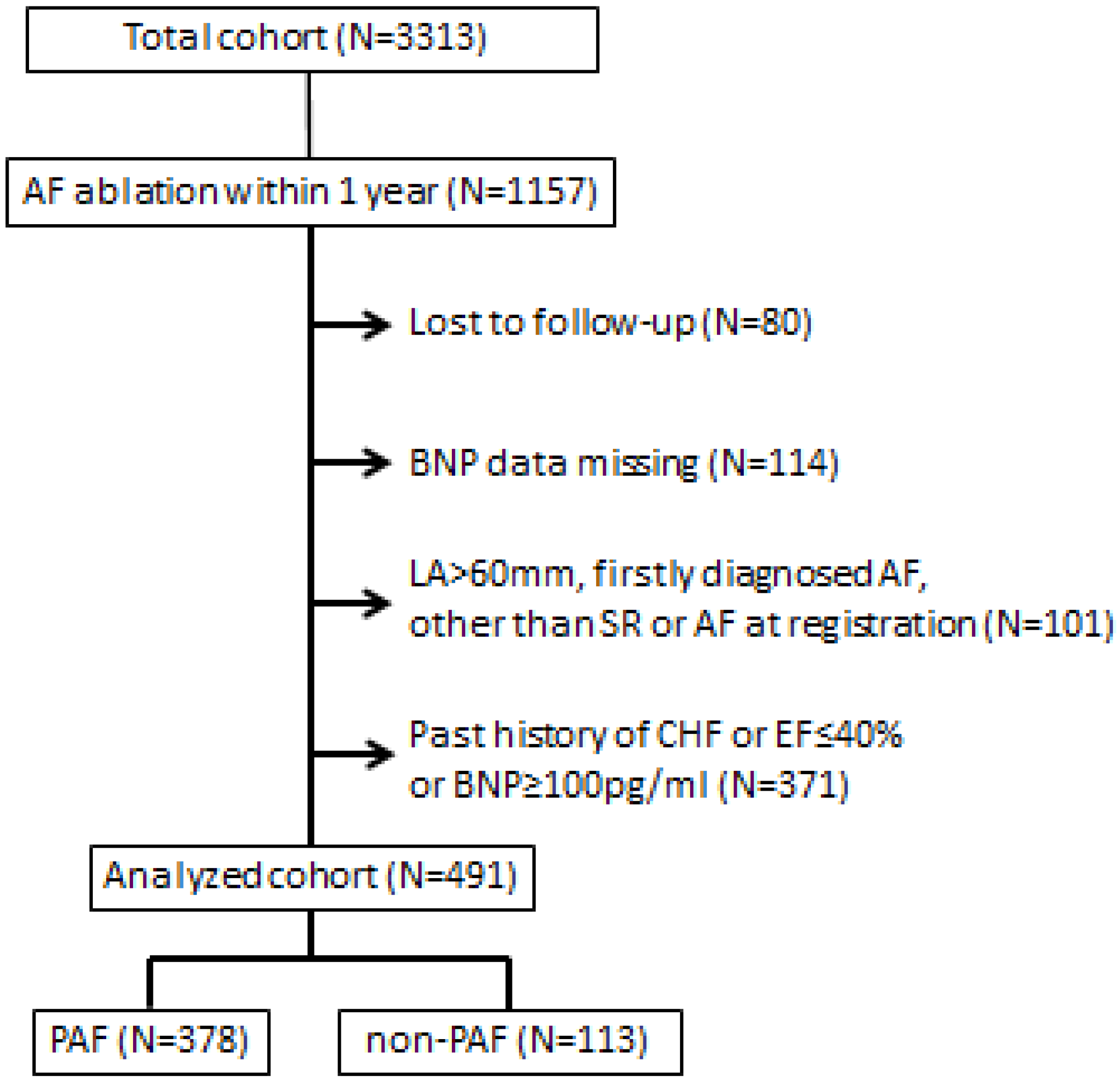
2.2. Studied Patients
2.3. Assessment of Patients’ Health Status
2.4. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Improvement in AFEQT Score
3.3. Comparative Analysis of PAF and Non-PAF Groups
4. Discussion
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wang, T.J.; Larson, M.G.; Levy, D.; Vasan, R.S.; Leip, E.P.; Wolf, P.A.; D’Agostino, R.B.; Murabito, J.M.; Kannel, W.B.; Benjamin, E.J. Temporal relations of atrial fibrillation and congestive heart failure and their joint influence on mortality: The framingham heart study. Circulation 2003, 107, 2920–2925. [Google Scholar] [CrossRef]
- Santhanakrishnan, R.; Wang, N.; Larson, M.G.; Magnani, J.W.; McManus, D.D.; Lubitz, S.A.; Ellinor, P.T.; Cheng, S.; Vasan, R.S.; Lee, D.S.; et al. Atrial fibrillation begets heart failure and vice versa: Temporal associations and differences in preserved versus reduced ejection fraction. Circulation 2016, 133, 484–492. [Google Scholar] [CrossRef]
- Mukoyama, M.; Nakao, K.; Saito, Y.; Ogawa, Y.; Hosoda, K.; Suga, S.; Shirakami, G.; Jougasaki, M.; Imura, H. Increased human brain natriuretic peptide in congestive heart failure. N. Engl. J. Med. 1990, 323, 757–758. [Google Scholar] [CrossRef]
- Ikemura, N.; Spertus, J.A.; Kimura, T.; Mahaffey, K.; Piccini, J.P.; Inohara, T.; Ueda, I.; Tanimoto, K.; Suzuki, M.; Nakamura, I.; et al. Cohort profile: Patient characteristics and quality-of-life measurements for newly-referred patients with atrial fibrillation-keio interhospital cardiovascular studies-atrial fibrillation (KICS-AF). BMJ Open 2019, 9, e032746. [Google Scholar] [CrossRef]
- Spertus, J.; Dorian, P.; Bubien, R.; Lewis, S.; Godejohn, D.; Reynolds, M.R.; Lakkireddy, D.R.; Wimmer, A.P.; Bhandari, A.; Burk, C. Development and validation of the atrial fibrillation effect on quality-of-life (AFEQT) questionnaire in patients with atrial fibrillation. Circ. Arrhythmia Electrophysiol. 2011, 4, 15–25. [Google Scholar] [CrossRef]
- Humphries, K.H.; Kerr, C.R.; Connolly, S.J.; Klein, G.; Boone, J.A.; Green, M.; Sheldon, R.; Talajic, M.; Dorian, P.; Newman, D. New-onset atrial fibrillation: Sex differences in presentation, treatment, and outcome. Circulation 2001, 103, 2365–2370. [Google Scholar] [CrossRef]
- Bozkurt, B.; Coats, A.J.; Tsutsui, H.; Abdelhamid, M.; Adamopoulos, S.; Albert, N.; Anker, S.D.; Atherton, J.; Böhm, M.; Butler, J.; et al. Universal definition and classification of heart failure: A report of the heart failure society of america, heart failure association of the european society of cardiology, Japanese heart failure society and writing committee of the universal definition of heart failure. J. Card. Fail. 2021, 27, 87–413. [Google Scholar] [CrossRef]
- Tsutsui, H.; Isobe, M.; Ito, H.; Okumura, K.; Ono, M.; Kitakaze, M.; Kinugawa, K.; Kihara, Y.; Goto, Y.; Komuro, I.; et al. JCS 2017/JHFS 2017 guideline on diagnosis and treatment of acute and chronic heart failure—Digest version. Circ. J. 2019, 83, 2084–2184. [Google Scholar] [CrossRef]
- Marrouche, N.F.; Brachmann, J.; Andresen, D.; Siebels, J.; Boersma, L.; Jordaens, L.; Merkely, B.; Pokushalov, E.; Sanders, P.; Proff, J.; et al. Catheter ablation for atrial fibrillation with heart failure. N. Engl. J. Med. 2018, 378, 417–427. [Google Scholar] [CrossRef]
- Shaaya, G.; Al-Khazaali, A.; Arora, R. Heart rate as a biomarker in heart failure: Role of heart rate lowering agents. Am. J. Ther. 2017, 24, e532–e539. [Google Scholar] [CrossRef]
- Melenovsky, V.; Hay, I.; Fetics, B.J.; Borlaug, B.A.; Kramer, A.; Pastore, J.M.; Berger, R.; Kass, D.A. Functional impact of rate irregularity in patients with heart failure and atrial fibrillation receiving cardiac resynchronization therapy. Eur. Heart J. 2005, 26, 705–711. [Google Scholar] [CrossRef]
- Wozakowska-Kaplon, B.; Opolski, G. Atrial natriuretic peptide level after cardioversion of chronic atrial fibrillation. Int. J. Cardiol. 2002, 83, 159–165. [Google Scholar] [CrossRef]
- Hsu, L.F.; Jaïs, P.; Sanders, P.; Garrigue, S.; Hocini, M.; Sacher, F.; Takahashi, Y.; Rotter, M.; Pasquié, J.L.; Scavée, C.; et al. Catheter ablation for atrial fibrillation in congestive heart failure. N. Engl. J. Med. 2004, 351, 2373–2383. [Google Scholar] [CrossRef]
- Hunter, R.J.; Berriman, T.J.; Diab, I.; Kamdar, R.; Richmond, L.; Baker, V.; Goromonzi, F.; Sawhney, V.; Duncan, E.; Page, S.P.; et al. A randomized controlled trial of catheter ablation versus medical treatment of atrial fibrillation in heart failure (the CAMTAF trial). Circ. Arrhythmia Electrophysiol. 2014, 7, 31–38. [Google Scholar] [CrossRef]
- Kim, Y.G.; Shim, J.; Choi, J.I.; Kim, Y.H. Radiofrequency catheter ablation improves the quality of life measured with a short form-36 questionnaire in atrial fibrillation patients: A systematic review and meta-analysis. PLoS ONE 2016, 11, e0163755. [Google Scholar] [CrossRef]
- Yagishita, A.; Yamauchi, Y.; Sato, H.; Yamashita, S.; Hirao, T.; Miyamoto, T.; Hirao, K. Efficacy of catheter ablation and concomitant antiarrhythmic drugs on the reduction of the arrhythmia burden in patients with long-standing persistent atrial fibrillation. J. Atr. Fibrillation 2017, 10, 1649. [Google Scholar] [CrossRef]
- Hamatani, Y.; Iguchi, M.; Ueno, K.; Aono, Y.; Esato, M.; Tsuji, H.; Wada, H.; Hasegawa, K.; Ogawa, H.; Abe, M.; et al. Prognostic significance of natriuretic peptide levels in atrial fibrillation without heart failure. Heart 2021, 107, 705–712. [Google Scholar] [CrossRef]
- Chang, K.W.; Hsu, J.C.; Toomu, A.; Fox, S.; Maisel, A.S. Clinical applications of biomarkers in atrial fibrillation. Am. J. Med. 2017, 130, 1351–1357. [Google Scholar] [CrossRef]
- York, M.K.; Gupta, D.K.; Reynolds, C.F.; Farber-Eger, E.; Wells, Q.S.; Bachmann, K.N.; Xu, M.; Harrell, F.E., Jr.; Wang, T.J. B-type natriuretic peptide levels and mortality in patients with and without heart failure. J. Am. Coll. Cardiol. 2018, 71, 2079–2088. [Google Scholar] [CrossRef]
- Hussein, A.A.; Saliba, W.I.; Martin, D.O.; Shadman, M.; Kanj, M.; Bhargava, M.; Dresing, T.; Chung, M.; Callahan, T.; Baranowski, B.; et al. Plasma B-type natriuretic peptide levels and recurrent arrhythmia after successful ablation of lone atrial fibrillation. Circulation 2011, 123, 2077–2082. [Google Scholar] [CrossRef]
- Verma, A.; Champagne, J.; Sapp, J.; Essebag, V.; Novak, P.; Skanes, A.; Morillo, C.A.; Khaykin, Y.; Birnie, D. Discerning the incidence of symptomatic and asymptomatic episodes of atrial fibrillation before and after catheter ablation (DISCERN AF): A prospective, multicenter study. JAMA Intern. Med. 2013, 173, 149–156. [Google Scholar] [CrossRef] [PubMed]
- Reynolds, M.R.; Lavelle, T.; Essebag, V.; Cohen, D.J.; Zimetbaum, P. Influence of age, sex, and atrial fibrillation recurrence on quality of life outcomes in a population of patients with new-onset atrial fibrillation: The fibrillation registry assessing costs, therapies, adverse events and lifestyle (FRACTAL) study. Am. Heart J. 2006, 152, 1097–1103. [Google Scholar] [CrossRef] [PubMed]
- Jenkins, L.S.; Brodsky, M.; Schron, E.; Chung, M.; Rocco, T., Jr.; Lader, E.; Constantine, M.; Sheppard, R.; Holmes, D.; Mateski, D.; et al. Quality of life in atrial fibrillation: The atrial fibrillation follow-up investigation of rhythm management (AFFIRM) study. Am. Heart J. 2005, 149, 112–120. [Google Scholar] [CrossRef] [PubMed]
- Yanagisawa, S.; Inden, Y.; Fujii, A.; Sakamoto, Y.; Tomomatsu, T.; Mamiya, K.; Okamoto, H.; Murohara, T.; Shibata, R. Early improvement of daily physical activity after catheter ablation for atrial fibrillation in an accelerometer assessment: A prospective pilot study. Ann. Noninvasive Electrocardiol. 2021, 26, e12807. [Google Scholar] [CrossRef]
- Ezzat, V.A.; Chew, A.; McCready, J.W.; Lambiase, P.D.; Chow, A.W.; Lowe, M.D.; Rowland, E.; Segal, O.R. Catheter ablation of atrial fibrillation-patient satisfaction from a single-center UK experience. J. Interv. Card. Electrophysiol. 2013, 37, 291–303. [Google Scholar] [CrossRef]
- Charitakis, E.; Barmano, N.; Walfridsson, U.; Walfridsson, H. Factors predicting arrhythmia-related symptoms and health-related quality of life in patients referred for radiofrequency ablation of atrial fibrillation: An observational study (the SMURF study). JACC Clin. Electrophysiol. 2017, 3, 494–502. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics, Count (%) | Quartile 1 (Lowest, 1.32–18.5) n = 123 | Quartile 2 (18.7–37.7) n = 123 | Quartile 3 (37.9–63.5) n = 122 | Quartile 4 (Highest, 63.8–99.8) n = 123 | p Value |
|---|---|---|---|---|---|
| Age, years, mean ± SD | 57 ± 10 | 61 ± 10 | 62 ± 11 | 64 ± 10 | <0.001 |
| Female | 19 (15) | 26 (21) | 31 (25) | 30 (24) | 0.224 |
| BMI, kg/m2 | 24 ± 3 | 24 ± 3 | 24 ± 3 | 24 ± 4 | 0.706 |
| Hear rate, bpm | 74 ± 14 | 73 ± 16 | 73 ± 16 | 78 ± 17 | 0.05 |
| Comorbidities | |||||
| Hypertension | 55 (48) | 53 (43) | 58 (48) | 61 (50) | 0.743 |
| Diabetes Mellitus | 10 (8) | 16 (13) | 13 (11) | 14 (11) | 0.665 |
| Dyslipidemia | 46 (37) | 40 (33) | 40 (33) | 45 (37) | 0.793 |
| Stroke or TIA | 7 (6) | 7 (6) | 4 (3) | 7 (6) | 0.777 |
| Obstructive sleep apnea | 7 (6) | 6 (5) | 6 (5) | 2 (2) | 0.401 |
| Coronary artery disease | 2 (2) | 3 (2) | 8 (7) | 2 (2) | 0.075 |
| Sick sinus syndrome | 4 (3) | 3 (2) | 7 (6) | 4 (3) | 0.547 |
| eGFR, mL/min/1.73 m2 | 71 ± 13 | 68 ± 14 | 67 ± 13 | 65 ± 12 | <0.01 |
| CHADS2 score | 0.7 ± 0.8 | 0.7 ± 0.9 | 0.7 ± 0.8 | 0.9 ± 0.9 | 0.408 |
| CHA2DS2-Vasc score | 1.1 ± 1.1 | 1.3 ± 1.2 | 1.5 ± 1.3 | 1.7 ± 1.3 | <0.005 |
| Paroxysmal AF | 118 (96) | 102 (83) | 89 (73) | 69 (57) | <0.001 |
| Medications | |||||
| Beta blocker | 40 (33) | 61 (50) | 50 (41) | 65 (53) | <0.01 |
| Antiarrhythmics | 53 (43) | 54 (44) | 37 (30) | 43 (35) | 0.083 |
| Echocardiography | |||||
| LVEF, % | 60 ± 5 | 59 ± 3 | 59 ± 4 | 59 ± 5 | <0.05 |
| Left atrium diameter, cm | 3.7 ± 0.6 | 3.8 ± 0.6 | 4.0 ± 0.7 | 4.0 ± 0.7 | <0.001 |
| E/e’ | 7.5 ± 2.4 | 9.5 ± 5.7 | 8.5 ± 3.5 | 8.7 ± 3.3 | <0.005 |
| LAAFV, cm/sec | 67 ± 21 | 61 ± 19 | 57 ± 21 | 52 ± 21 | <0.001 |
| AFEQT scores | |||||
| Overall | 71.1 ± 18.4 | 74.7 ± 17.0 | 77.7 ± 17.6 | 75.4 ± 18.6 | <0.05 |
| Symptom | 69.7 ± 21.6 | 71.8 ± 21.1 | 76.7 ± 20.3 | 76.7 ± 19.1 | <0.05 |
| Daily Activities | 75.0 ± 22.8 | 77.4 ± 21.5 | 79.7 ± 21.1 | 76.2 ± 24.3 | 0.403 |
| Treatment concern | 66.4 ± 19.3 | 72.7 ± 17.4 | 75.5 ± 18.3 | 73.2 ± 17.7 | <0.001 |
| Satisfaction | 59.8 ± 20.8 | 63.2 ± 19.9 | 62.7 ± 18.3 | 60.3 ± 22.0 | 0.559 |
| Quartile 1 | Quartile 2 | Quartile 3 | Quartile 4 | p Value | |
|---|---|---|---|---|---|
| AFEQT scores at 1 year follow-up | |||||
| Overall | 90.8 ± 10.3 | 90.8 ± 10.4 | 89.6 ± 12.4 | 90.2 ± 11.3 | 0.79 |
| Symptom | 90.6 ± 12.8 | 92.5 ± 9.7 | 89.0 ± 16.7 | 92.1 ± 11.9 | 0.14 |
| Daily Activities | 92.7 ± 11.7 | 91.2 ± 12.8 | 90.1 ± 14.7 | 90.3 ± 14.8 | 0.441 |
| Treatment concern | 88.5 ± 12.4 | 88.7 ± 12.0 | 89.2 ± 11.7 | 88.5 ± 11.9 | 0.972 |
| Satisfaction | 84.9 ± 19.4 | 85.2 ± 18.9 | 84.4 ± 19.3 | 87.1 ± 16.0 | 0.684 |
| Absolute changes in AFEQT score during 1 year | |||||
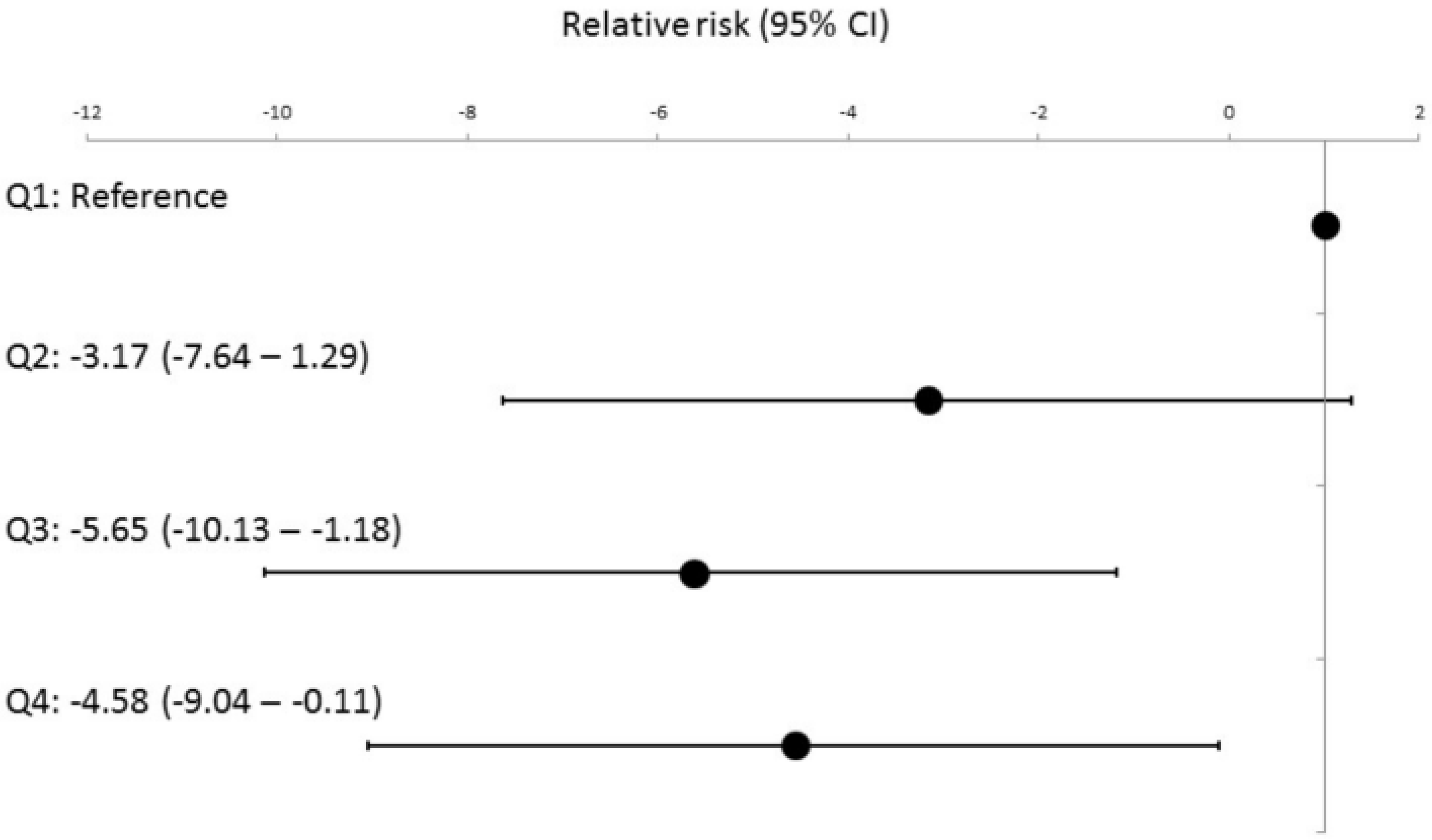
| Overall | 19.7 ± 18.2 | 16.2 ± 17.3 | 11.9 ± 15.8 | 14.9 ± 17.4 | <0.005 |
| Symptom | 20.3 ± 22.7 | 20.6 ± 21.0 | 12.4 ± 22.4 | 15.5 ± 20.5 | <0.01 |
| Daily Activities | 17.7 ± 23.4 | 13.9 ± 23.0 | 10.5 ± 17.8 | 14.1 ± 21.7 | 0.08 |
| Treatment concern | 22.1 ± 18.6 | 16.3 ± 17.1 | 13.7 ± 16.1 | 15.4 ± 18.3 | <0.005 |
| Satisfaction | 24.4 ± 25.9 | 20.2 ± 26.7 | 21.9 ± 24.5 | 27.0 ± 22.4 | 0.249 |
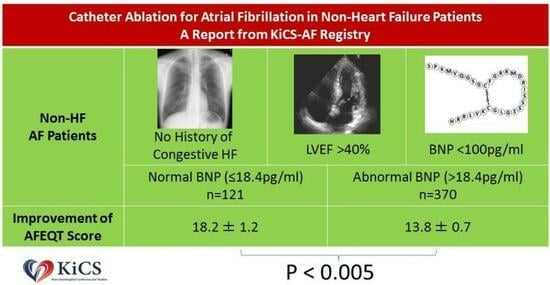
| Normal BNP n = 121 | Abnormal BNP n = 370 | p Value | |
|---|---|---|---|
| Overall | 18.2 ± 1.2 15.9–20.6 | 13.8 ± 0.7 12.5–15.1 | <0.005 |
| Symptom | 20.2 ± 1.6 17.1–23.3 | 15.2 ± 0.8 13.5–16.8 | <0.005 |
| Daily Activities | 15.8 ± 1.6 12.7–18.8 | 12.4 ± 0.9 10.7–14.1 | 0.055 |
| Treatment concern | 20.8 ± 1.3 18.3–23.3 | 14.8 ± 0.7 13.5–16.1 | <0.001 |
| Satisfaction | 24.3 ± 1.8 20.8–27.8 | 22.5 ± 1.0 20.6–24.5 | 0.385 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kashimura, S.; Ikemura, N.; Kohsaka, S.; Katsumata, Y.; Kimura, T.; Shinmura, D.; Fukumoto, K.; Negishi, K.; Ueda, I.; Takatsuki, S.; et al. Clinical Utility of Baseline Brain Natriuretic Peptide Levels on Health Status Outcomes after Catheter Ablation for Atrial Fibrillation in Individuals without Heart Failure. J. Clin. Med. 2024, 13, 407. https://doi.org/10.3390/jcm13020407
Kashimura S, Ikemura N, Kohsaka S, Katsumata Y, Kimura T, Shinmura D, Fukumoto K, Negishi K, Ueda I, Takatsuki S, et al. Clinical Utility of Baseline Brain Natriuretic Peptide Levels on Health Status Outcomes after Catheter Ablation for Atrial Fibrillation in Individuals without Heart Failure. Journal of Clinical Medicine. 2024; 13(2):407. https://doi.org/10.3390/jcm13020407
Chicago/Turabian StyleKashimura, Shin, Nobuhiro Ikemura, Shun Kohsaka, Yoshinori Katsumata, Takehiro Kimura, Daisuke Shinmura, Kotaro Fukumoto, Koji Negishi, Ikuko Ueda, Seiji Takatsuki, and et al. 2024. "Clinical Utility of Baseline Brain Natriuretic Peptide Levels on Health Status Outcomes after Catheter Ablation for Atrial Fibrillation in Individuals without Heart Failure" Journal of Clinical Medicine 13, no. 2: 407. https://doi.org/10.3390/jcm13020407
APA StyleKashimura, S., Ikemura, N., Kohsaka, S., Katsumata, Y., Kimura, T., Shinmura, D., Fukumoto, K., Negishi, K., Ueda, I., Takatsuki, S., & Ieda, M. (2024). Clinical Utility of Baseline Brain Natriuretic Peptide Levels on Health Status Outcomes after Catheter Ablation for Atrial Fibrillation in Individuals without Heart Failure. Journal of Clinical Medicine, 13(2), 407. https://doi.org/10.3390/jcm13020407