
Physical and Mental Components of Quality of Life after a Cardiac Rehabilitation Intervention: A Systematic Review and Meta-Analysis

 , , , ,
, , , ,  and
and
Abstract
1. Introduction
2. Methods
2.1. Research Question and Eligibility Criteria
2.2. Search Strategy and Selection of Studies
2.3. Data Extraction
2.4. Risk of Bias
2.5. Quality of Evidence Assessment
2.6. Data Synthesis and Analysis
3. Results
3.1. Characteristics of Studies and Participants
3.2. Systematic Review
3.3. Risk-of-Bias Assessment
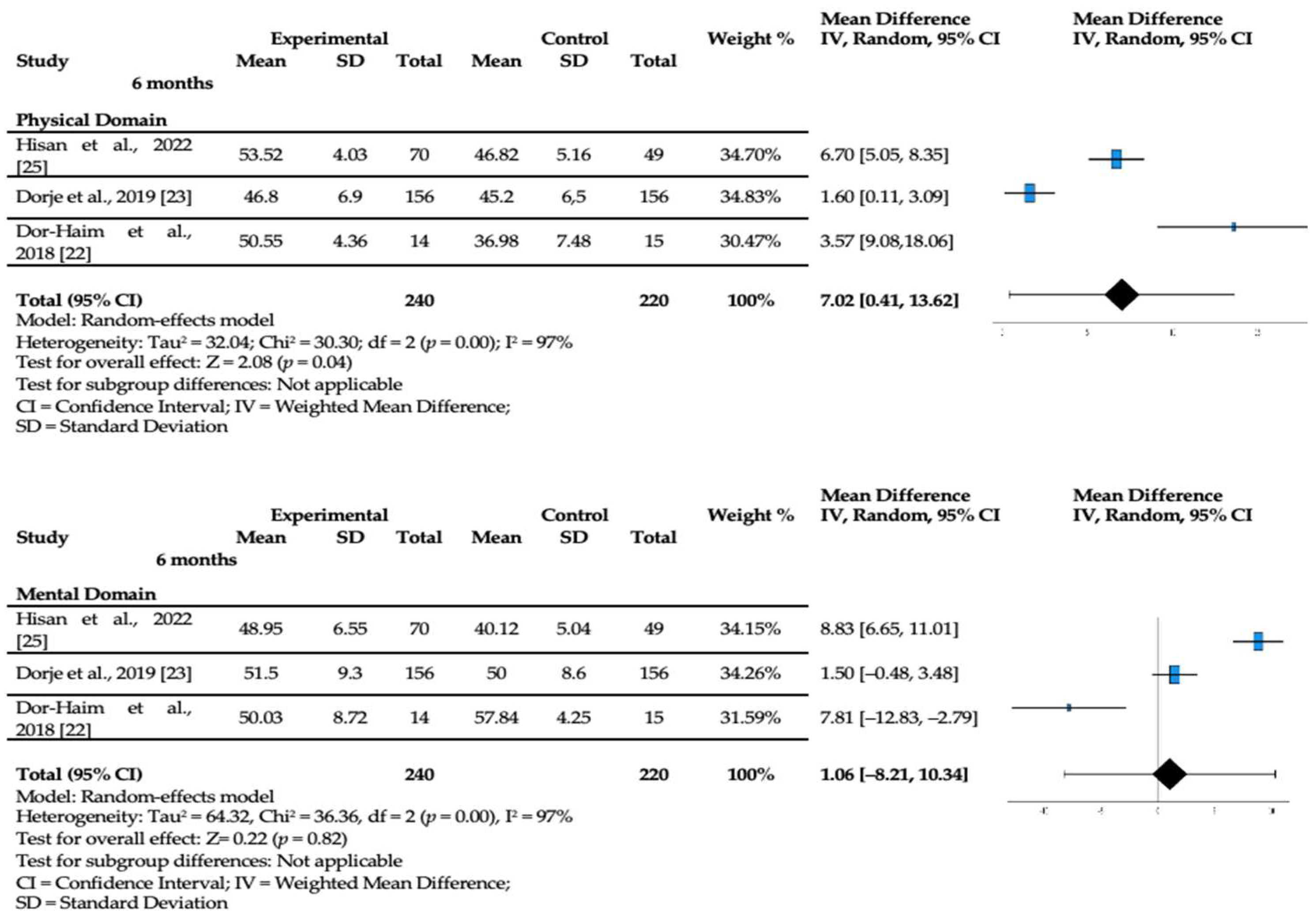
3.4. Meta-Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Top 10 Causes of Death. Available online: https://www.who.int/news-room/fact-sheets/detail/the-top-10-causes-of-death (accessed on 10 August 2024).
- Piepoli, M.F.; Hoes, A.W.; Agewall, S.; Albus, C.; Brotons, C.; Catapano, A.L.; Cooney, M.T.; Corrà, U.; Cosyns, B.; Deaton, C.; et al. 2016 European Guidelines on cardiovascular disease prevention in clinical practice: The Sixth Joint Task Force of the European Society of Cardiology and Other Societies on Cardiovascular Disease Prevention in Clinical Practice (constituted by representatives of 10 societies and by invited experts) Developed with the special contribution of the European Association for Cardiovascular Prevention & Rehabilitation (EACPR). Eur. Heart J. 2016, 37, 2315–2381. [Google Scholar] [CrossRef] [PubMed]
- Arnett, D.K.; Blumenthal, R.S.; Albert, M.A.; Buroker, A.B.; Goldberger, Z.D.; Hahn, E.J.; Himmelfarb, C.D.; Khera, A.; Lloyd-Jones, D.; McEvoy, J.W.; et al. 2019 ACC/AHA Guideline on the Primary Prevention of Cardiovascular Disease: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation 2019, 140, 596–646. [Google Scholar] [CrossRef]
- Winnige, P.; Vysoky, R.; Dosbaba, F.; Batalik, L. Cardiac rehabilitation and its essential role in the secondary prevention of cardiovascular diseases. World J. Clin. Cases 2021, 9, 1761–1784. [Google Scholar] [CrossRef] [PubMed]
- Moreira, J.M.A.; Grilo, E.N. Quality of life after coronary artery bypass graft surgery—Results of cardiac rehabilitation programme. J. Exerc. Rehabil. 2019, 15, 715–722. [Google Scholar] [CrossRef]
- Blumer, V.; Greene, S.J.; Wu, A.; Butler, J.; Ezekowitz, J.A.; Lindenfeld, J.; Alhanti, B.; Hernandez, A.F.; O’Connor, C.M.; Mentz, R.J. Sex Differences in Clinical Course and Patient-Reported Outcomes among Patients Hospitalized for Heart Failure. Heart Fail. 2021, 9, 336–345. [Google Scholar] [CrossRef]
- Dawson, J.; Doll, H.; Fitzpatrick, R.; Jenkinson, C.; Carr, A.J. The routine use of patient reported outcome measures in healthcare settings. BMJ 2010, 340, 186. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, S.; Ware, P.; Gardner, W.; Witter, J.; Bingham, C.O.; Kairy, D.; Bartlett, S.J. Montreal Accord on Patient-Reported Outcomes (PROs) use series—Paper 8: Patient-reported outcomes in electronic health records can inform clinical and policy decisions. J. Clin. Epidemiol. 2017, 89, 160–167. [Google Scholar] [CrossRef]
- McKenna, S.P. Measuring patient-reported outcomes: Moving beyond misplaced common sense to hard science. BMC Med. 2011, 14, 86. [Google Scholar] [CrossRef]
- McMurray, J.; McNeil, H.; Gordon, A.; Elliott, J.; Stolee, P. Psychometric Testing of a Rehabilitative Care Patient Experience Instrument. Arch. Phys. Med. Rehabil. 2018, 99, 1840–1847. [Google Scholar] [CrossRef]
- Salzwedel, A.; Koran, I.; Langheim, E.; Schlitt, A.; Nothroff, J.; Bongarth, C.; Wrenger, M.; Sehner, S.; Reibis, R.; Wegscheider, K.; et al. Patient-reported outcomes predict return to work and health-related quality of life six months after cardiac rehabilitation: Results from a German multi-centre registry (OutCaRe). PLoS ONE 2020, 15, e0232752. [Google Scholar] [CrossRef]
- Mansilla-Chacón, M.; Gómez-Urquiza, J.L.; Martos-Cabrera, M.B.; Albendín-García, L.; Romero-Béjar, J.L.; Cañadas-De La Fuente, G.A.; Suleiman-Martos, N. Effects of Supervised Cardiac Rehabilitation Programmes on Quality of Life among Myocardial Infarction Patients: A Systematic Review and Meta-Analysis. J. Cardiovasc. Dev. Dis. 2021, 8, 166. [Google Scholar] [CrossRef] [PubMed]
- Candelaria, D.; Randall, S.; Ladak, L.; Gallagher, R. Health-related quality of life and exercise-based cardiac rehabilitation in contemporary acute coronary syndrome patients: A systematic review and meta-analysis. Qual. Life Res. 2020, 29, 579–592. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. Cochrane Handbook for Systematic Reviews of Interventions, 2nd ed.; John Wiley & Sons: Chichester, UK, 2019. [Google Scholar]
- Guyatt, G.H.; Oxman, A.D.; Kunz, R.; Vist, G.E.; Falck-Ytter, Y.; Schünemann, H.J. What is “quality of evidence” and why is it important to clinicians? BMJ 2008, 336, 995–998. [Google Scholar] [CrossRef] [PubMed]
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials. Control. Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef] [PubMed]
- Egger, M.; Davey Smith, G.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef]
- Campo, G.; Tonet, E.; Chiaranda, G.; Sella, G.; Maietti, E.; Bugani, G.; Vitali, F.; Serenelli, M.; Mazzoni, G.; Ruggiero, R.; et al. Exercise intervention improves quality of life in older adults after myocardial infarction: Randomised clinical trial. Heart 2020, 106, 1658–1664. [Google Scholar] [CrossRef] [PubMed]
- Casper, E.A.; El Wakeel, L.M.; Saleh, M.A.; El-Hamamsy, M.H. Management of pharmacotherapy-related problems in acute coronary syndrome: Role of clinical pharmacist in cardiac rehabilitation unit. Basic Clin. Pharmacol. Toxicol. 2019, 125, 44–53. [Google Scholar] [CrossRef]
- Deng, B.; Shou, X.; Ren, A.; Liu, X.; Wang, Q.; Wang, B.; Wang, Y.; Yan, T.; Zhao, X.; Zhu, L. Effect of aerobic training on exercise capacity and quality of life in patients older than 75 years with acute coronary syndrome undergoing percutaneous coronary intervention. Physiother. Theory Pract. 2022, 38, 1135–1144. [Google Scholar] [CrossRef]
- Dor-Haim, H.; Barak, S.; Horowitz, M.; Yaakobi, E.; Katzburg, S.; Swissa, M.; Lotan, C. Improvement in cardiac dysfunction with a novel circuit training method combining simultaneous aerobic-resistance exercises. A randomized trial. PLoS ONE 2018, 13, e0188551. [Google Scholar] [CrossRef]
- Dorje, T.; Zhao, G.; Tso, K.; Wang, J.; Chen, Y.; Tsokey, L.; Tan, B.K.; Scheer, A.; Jacques, A.; Li, Z.; et al. Smartphone and social media-based cardiac rehabilitation and secondary prevention in China (SMART-CR/SP): A parallel-group, single-blind, randomised controlled trial. Lancet Digit. Health 2019, 1, 363–374. [Google Scholar] [CrossRef] [PubMed]
- Herring, L.Y.; Dallosso, H.; Schreder, S.; Smith, E.J.; Waheed, G.; Gray, L.J.; Khunti, K.; Yates, T.; Highton, P.J.; Rowlands, A.V.; et al. Physical Activity after Cardiac EventS (PACES): A group education programme with subsequent text message support designed to increase physical activity in individuals with diagnosed coronary heart disease: A randomised controlled trial. Open Heart 2021, 8, e001351. [Google Scholar] [CrossRef] [PubMed]
- Hisam, A.; Haq, Z.U.; Aziz, S.; Doherty, P.; Pell, J. Effectiveness of Mobile Health Augmented Cardiac Rehabilitation (MCard) on health-related quality of life among post-acute coronary syndrome patients: A randomized controlled trial. Pak. J. Med. Sci. 2022, 38, 716–723. [Google Scholar] [CrossRef] [PubMed]
- Ma, L.; Deng, L.; Yu, H. The effects of a comprehensive rehabilitation and intensive education program on anxiety, depression, quality of life, and major adverse cardiac and cerebrovascular events in unprotected left main coronary artery disease patients who underwent coronary artery bypass grafting. Ir. J. Med. Sci. 2020, 189, 477–488. [Google Scholar] [CrossRef]
- Muthukrishnan, R.; Malik, G.S.; Gopal, K.; Shehata, M.A. Power walking based outpatient cardiac rehabilitation in patients with post-coronary angioplasty: Randomized control trial. Physiother. Res. Int. 2021, 26, e1919. [Google Scholar] [CrossRef]
- Pedersen, C.G.; Nielsen, C.V.; Lynggaard, V.; Zwisler, A.D.; Maribo, T. Cardiac rehabilitation: Pedagogical education strategies have positive effect on long-term patient-reported outcomes. Health Educ. Res. 2023, 38, 597–609. [Google Scholar] [CrossRef]
- Ul-Haq, Z.; Khan, D.; Hisam, A.; Yousafzai, Y.M.; Hafeez, S.; Zulfiqar, F.; Gul, A.M.; Hafizullah, M.; Pell, J. Effectiveness of Cardiac Rehabilitation on Health-related Quality of Life in Patients with Myocardial Infarction in Pakistan. J. Coll. Physicians Surg. Pak. 2019, 29, 803–809. [Google Scholar] [CrossRef]
- Wienbergen, H.; Fach, A.; Meyer, S.; Meyer, J.; Stehmeier, J.; Backhaus, T.; Michel, S.; Krämer, K.; Osteresch, R.; Schmucker, J.; et al. Effects of an intensive long-term prevention programme after myocardial infarction—A randomized trial. Eur. J. Prev. Cardiol. 2019, 26, 522–530. [Google Scholar] [CrossRef]
- Dibben, G.O.; Faulkner, J.; Oldridge, N.; Rees, K.; Thompson, D.R.; Zwisler, A.D.; Taylor, R.S. Exercise-based cardiac rehabilitation for coronary heart disease: A meta-analysis. Eur. Heart J. 2023, 44, 452–469. [Google Scholar] [CrossRef]
- Foster, A.; Croot, L.; Brazier, J.; Harris, J.; O’Cathain, A. The facilitators and barriers to implementing patient reported outcome measures in organisations delivering health related services: A systematic review of reviews. J. Patient Rep. Outcomes 2018, 2, 46. [Google Scholar] [CrossRef]
- Johnston, B.C.; Patrick, D.L.; Busse, J.W.; Schünemann, H.J.; Agarwal, A.; Guyatt, G.H. Patient-reported outcomes in meta-analyses—Part 1: Assessing risk of bias and combining outcomes. Health Qual. Life Outcomes 2013, 11, 109. [Google Scholar] [CrossRef] [PubMed]
- Cornélio, M.E.; Alexandre, N.M.; São-João, T.M. Measuring instruments in cardiology adapted into Portuguese language of Brazil: A systematic review. Rev. Esc. Enferm. USP 2014, 48, 368–376. [Google Scholar] [CrossRef]
- Moreira, J.; Miguel, S.; Delgado, B.; Boto, P. Patient-reported outcome measures in rehabilitation after knee surgery: A rapid systematic review. J. Public Health. 2024, 1–15. [Google Scholar] [CrossRef]
- Moreira, J.; Mesquita, M.; Flamínio, J.; Almeida, M.; Delgado, B.; Boto, P. Patient-reported outcome measures in knee injuries rehabilitation: A protocol for intervention. MethodsX 2024, 12, 102647. [Google Scholar] [CrossRef]
- Maruszczyk, K.; McMullan, C.; Aiyegbusi, O.L.; Keeley, T.; Wilson, R.; Collis, P.; Bottomley, C.; Calvert, M.J. Paving the way for patient centricity in real-world evidence (RWE): Qualitative interviews to identify considerations for wider implementation of patient-reported outcomes in RWE generation. Heliyon 2023, 9, e20157. [Google Scholar] [CrossRef] [PubMed]
- Rahimi, K.; Malhotra, A.; Banning, A.P.; Jenkinson, C. Outcome selection and role of patient reported outcomes in contemporary cardiovascular trials: Systematic review. BMJ 2010, 341, c5707. [Google Scholar] [CrossRef]
- Snoek, J.A.; Prescott, E.I.; van der Velde, A.E.; Eijsvogels, T.M.; Mikkelsen, N.; Prins, L.F.; Bruins, W.; Meindersma, E.; González-Juanatey, J.R.; Peña-Gil, C.; et al. Effectiveness of Home-Based Mobile Guided Cardiac Rehabilitation as Alternative Strategy for Nonparticipation in Clinic-Based Cardiac Rehabilitation among Elderly Patients in Europe: A Randomized Clinical Trial. JAMA Cardiol. 2021, 6, 463–468. [Google Scholar] [CrossRef] [PubMed]
- Francis, T.; Kabboul, N.; Rac, V.; Mitsakakis, N.; Pechlivanoglou, P.; Bielecki, J.; Alter, D.; Krahn, M. The Effect of Cardiac Rehabilitation on Health-Related Quality of Life in Patients with Coronary Artery Disease: A Meta-analysis. Can. J. Cardiol. 2019, 35, 352–364. [Google Scholar] [CrossRef]
- Warburton, D.E.; Bredin, S.S. Health benefits of physical activity: A systematic review of current systematic reviews. Health Qual. Life Outcomes 2007, 32, 541–556. [Google Scholar] [CrossRef]
- Shibata, A.; Oka, K.; Nakamura, Y.; Muraoka, I. Recommended level of physical activity and health-related quality of life among Japanese adults. Health Qual. Life Outcomes 2007, 5, 64. [Google Scholar] [CrossRef]
- Rumsfeld, J.S.; Alexander, K.P.; Goff, D.C., Jr.; Graham, M.M.; Ho, P.M.; Masoudi, F.A.; Moser, D.K.; Roger, V.L.; Slaughter, M.S.; Smolderen, K.G.; et al. Cardiovascular health: The importance of measuring patient-reported health status: A scientific statement from the American Heart Association. Circulation 2013, 127, 2233–2249. [Google Scholar] [CrossRef]
- Houle, J.; Doyon, O.; Vadeboncoeur, N.; Turbide, G.; Diaz, A.; Poirier, P. Effectiveness of a pedometer-based program using a socio-cognitive intervention on physical activity and quality of life in a setting of cardiac rehabilitation. Can. J. Cardiol. 2012, 28, 27–32. [Google Scholar] [CrossRef]
- Ladak, L.A.; Hasan, B.S.; Gullick, J.; Gallagher, R. Health-related quality of life in congenital heart disease surgery in children and young adults: A systematic review and meta-analysis. Arch. Dis. Child. 2019, 104, 340–347. [Google Scholar] [CrossRef]
- Salzwedel, A.; Völler, H. Cardiac rehabilitation: Patient-reported outcomes are decisive for success. Dtsch. Ärzteblatt Int. 2021, 118, 505–506. [Google Scholar] [CrossRef]
- Shepard, D.S.; Zakir, S.; Gaalema, D.E.; Ades, P.A. Cost-Effectiveness of Cardiac Rehabilitation in Older Adults with Coronary Heart Disease. J. Cardiopulm. Rehabil. Prev. 2024, 44, 107–114. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Author, Year | Country | Study Design (Sample Size) | Age (Years) | Type of Intervention | PROM(s): Measuring Quality of Life | Timing of PROM(s) |
|---|---|---|---|---|---|---|
| Campo et al., 2020 [19] | Italy | RCT (n = 235) | 76 ◊ | —IG 6 received 4 supervised sessions of exercise after discharge combined with home-based exercise. —CG 1 attended a health education intervention only. | EQ-5D-3L 3 | Baseline, at month 6, 12 |
| Casper et al., 2019 [20] | Egypt | RCT (n = 40) | 52.3 ◊ | —IG 6 received standard treatment, educational intervention 30–40 min/session every 2 weeks for 3 months, and regular telephone follow-up reminders every week for 3 months. —CG 1 attended counselling about diet and smoking cessation, adjusting cardiovascular medication when needed, and exercise intervention. | SF-36 8 | Baseline, at month 3 |
| Deng et al., 2020 [21] | China | RCT (n = 70) | 81.6 ◊ | —IG 6 received a supervised session combined with home-based exercise; the duration was 12 weeks, 5 sessions/week with 40 min/session. —CG 1 received standard treatment including education, social support, and advice on diet and exercise. | SF-12 9 | Baseline, at month 3 |
| Dor-Haim et al., 2018 [22] | Israel | RCT (n = 29) | 47–69 | —IG 6 received for 12 weeks a super-circuit training, performed moderate- to high-intensity exercise, alternating between resistance and aerobic training, at 75–85% of their heart reserve. —CG 1 participants performed exercise intervention at 60–70% of their cardiac reserve, where each session lasted 45 min. | SF-12 9 | Baseline, at month 3 |
| Dorje et al., 2019 [23] | China | RCT (n = 312) | 59.1 ◊ | —IG 6 received a 2-month intensive program, followed by a 4-month step-down stage. During the intensive intervention phase, participants received 4 educational modules/week via chat. In the step-down phase, participants received only two cartoon pictures with key motivational messages per week. —CG 1 received standard care, as provided by their community doctors and cardiologists after hospital discharge. | SF-12 9 | Baseline, at month 2, 6, 12 |
| Herring et al., 2021 [24] | UK | RCT (n = 291) | 66.48 ◊ | —IG 6 received one session with information leaflet and an education intervention that comprised 2 and 5 h sessions delivered 2 weeks apart by two trained facilitators. —CG 1 received one session with an information leaflet and returned to their general practitioner standard care. | EQ-5D-5L 2 MacNew 7 | Baseline, at month 12 |
| Hisam et al., 2022 [25] | Pakistan | RCT (n = 160) | 53.6 ◊ | —IG 6 received the intervention, supervised, in addition to standard post-ACS care. The first phase included individualized psychotherapy during the hospital stay and the second phase included diurnal mobile texting of standardized messages about healthy lifestyle changes through a specially developed app. —CG 1 received standard post-ACS care. | SF-12 9 MacNew 7 | Baseline, at month 3, 6 |
| Ma et al., 2020 [26] | China | RCT (n = 300) | 63.1 ◊ | —IG 6 received the program, consisting of a four-part intervention: related health education, supervised exercise and surveillance, risk factor control, and psychological nursing. —CG 1 was given usual care. | SF-12 9 | Baseline, at month 3, 6, 12 |
| Muthukrishnan et al., 2021 [27] | UAE | RCT (n = 24) | 49 ◊ | —IG 6 received an aerobic intervention with progressively intensive power walking based on a prescribed target heart rate on treadmill. —CG 1 received for 4 weeks a program,3 times a week, in 12 sessions under supervision. | HeartQoL 5 | Baseline, at month 1 |
| Pedersen et al., 2023 [28] | Denmark | RCT (n = 312) | 49 ◊ | —IG 6 received a multidisciplinary program and pedagogical strategy empowerment, motivation, and medical adherence. —CG 1 received a multidisciplinary program. | HeartQoL 5 | Baseline, at month 6, 12 |
| Ul-Haq et al., 2019 [29] | Pakistan | RCT (n = 206) | 53 ◊ | —IG 6 received a structured counselling intervention, counselling and health education, medicine prescription, and follow-up advice. —CG 1 obtained only the standard communication from the cardiologist and routine follow-up care. | GHQ 4 MacNew 7 | Baseline, at month 8 |
| Wienbergen et al., 2019 [30] | Germany | RCT (n = 281) | 56.5 ◊ | —IG 6 participants were educated and controlled to change their lifestyle in a way to reduce cardiovascular risk factors and maintain or optimize medical secondary prevention therapy (every 3 weeks the prevention assistant had personal telephone contact). —CG 1 received medical and interventional therapy following the current standard of care. | EQ-5D-5L 2 | Baseline, at month 6, 12 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moreira, J.; Bravo, J.; Aguiar, P.; Delgado, B.; Raimundo, A.; Boto, P. Physical and Mental Components of Quality of Life after a Cardiac Rehabilitation Intervention: A Systematic Review and Meta-Analysis. J. Clin. Med. 2024, 13, 5576. https://doi.org/10.3390/jcm13185576
Moreira J, Bravo J, Aguiar P, Delgado B, Raimundo A, Boto P. Physical and Mental Components of Quality of Life after a Cardiac Rehabilitation Intervention: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine. 2024; 13(18):5576. https://doi.org/10.3390/jcm13185576
Chicago/Turabian StyleMoreira, José, Jorge Bravo, Pedro Aguiar, Bruno Delgado, Armando Raimundo, and Paulo Boto. 2024. "Physical and Mental Components of Quality of Life after a Cardiac Rehabilitation Intervention: A Systematic Review and Meta-Analysis" Journal of Clinical Medicine 13, no. 18: 5576. https://doi.org/10.3390/jcm13185576
APA StyleMoreira, J., Bravo, J., Aguiar, P., Delgado, B., Raimundo, A., & Boto, P. (2024). Physical and Mental Components of Quality of Life after a Cardiac Rehabilitation Intervention: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine, 13(18), 5576. https://doi.org/10.3390/jcm13185576