Impact of Child Respiratory Syncytial Virus-Confirmed Infections on Caregivers in Japan: A Web-Based Survey

 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Research Participants
2.3. Measures
2.4. Data Handling and Statistical Analyses
2.5. Ethical Considerations
3. Results
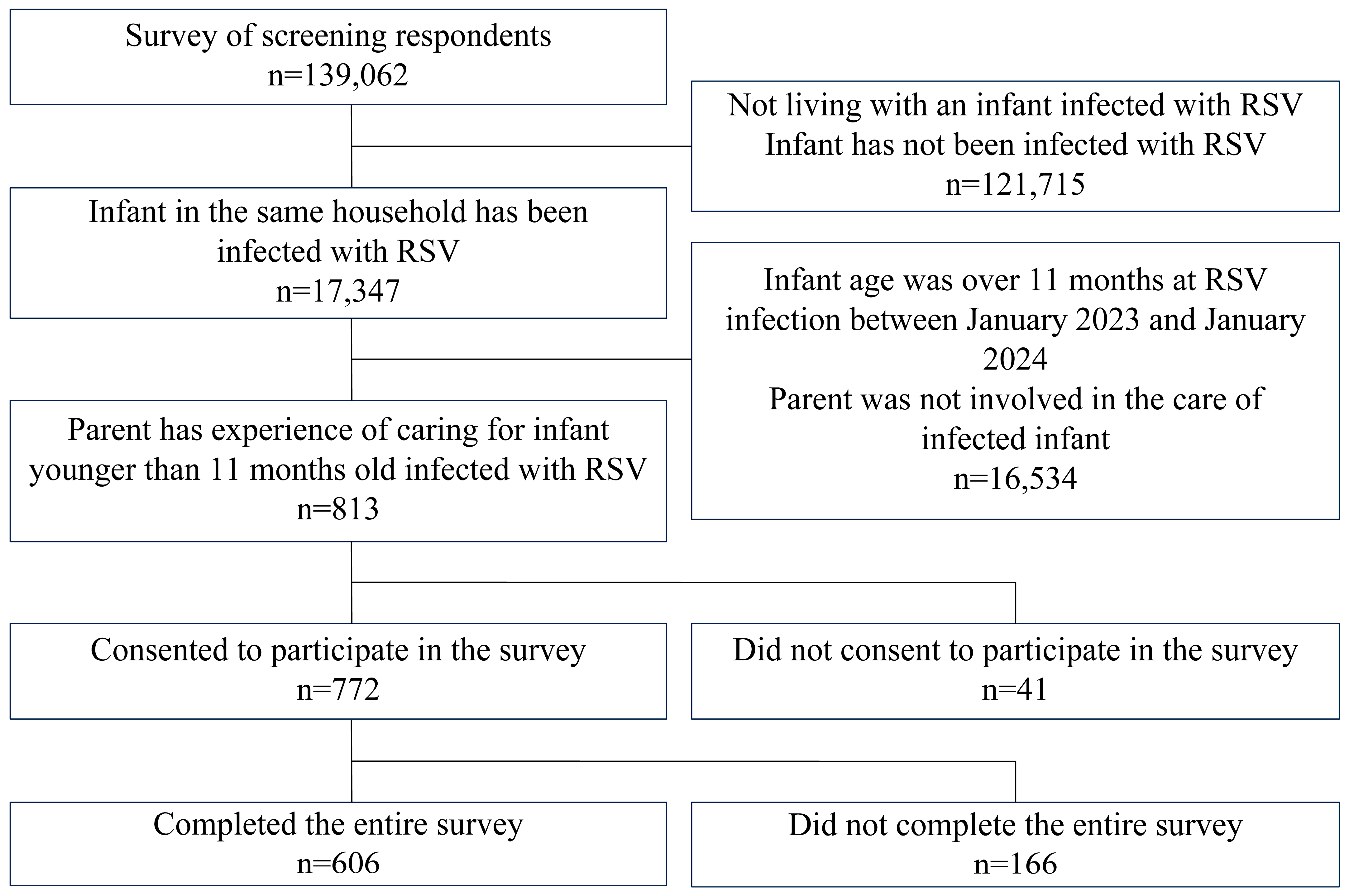
3.1. Selection of Participating Caregivers
3.2. Characteristics of Surveyed Infants with RSV and Their Caregivers
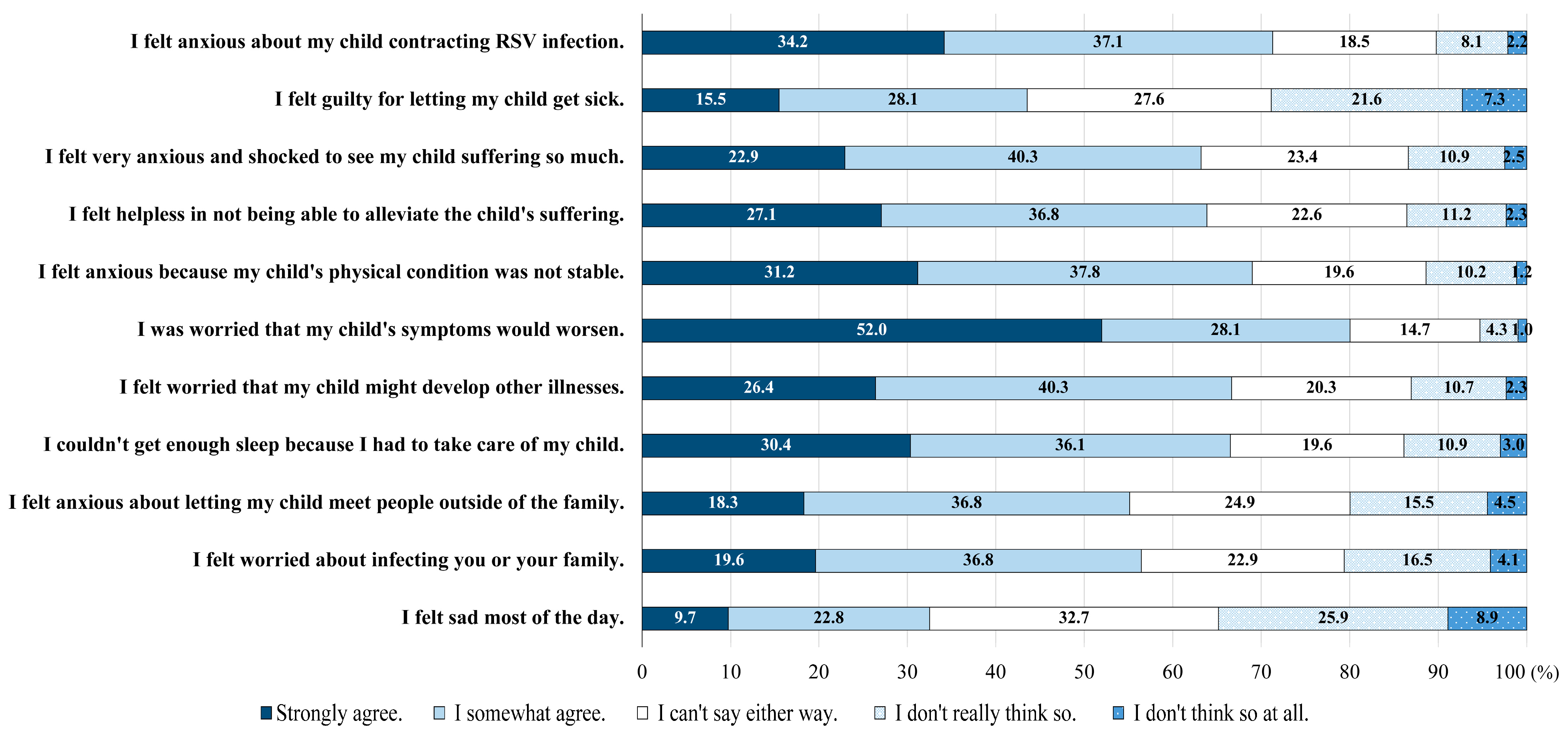
3.3. Psychological Burden of RSV Infection in Infants on the Caregivers
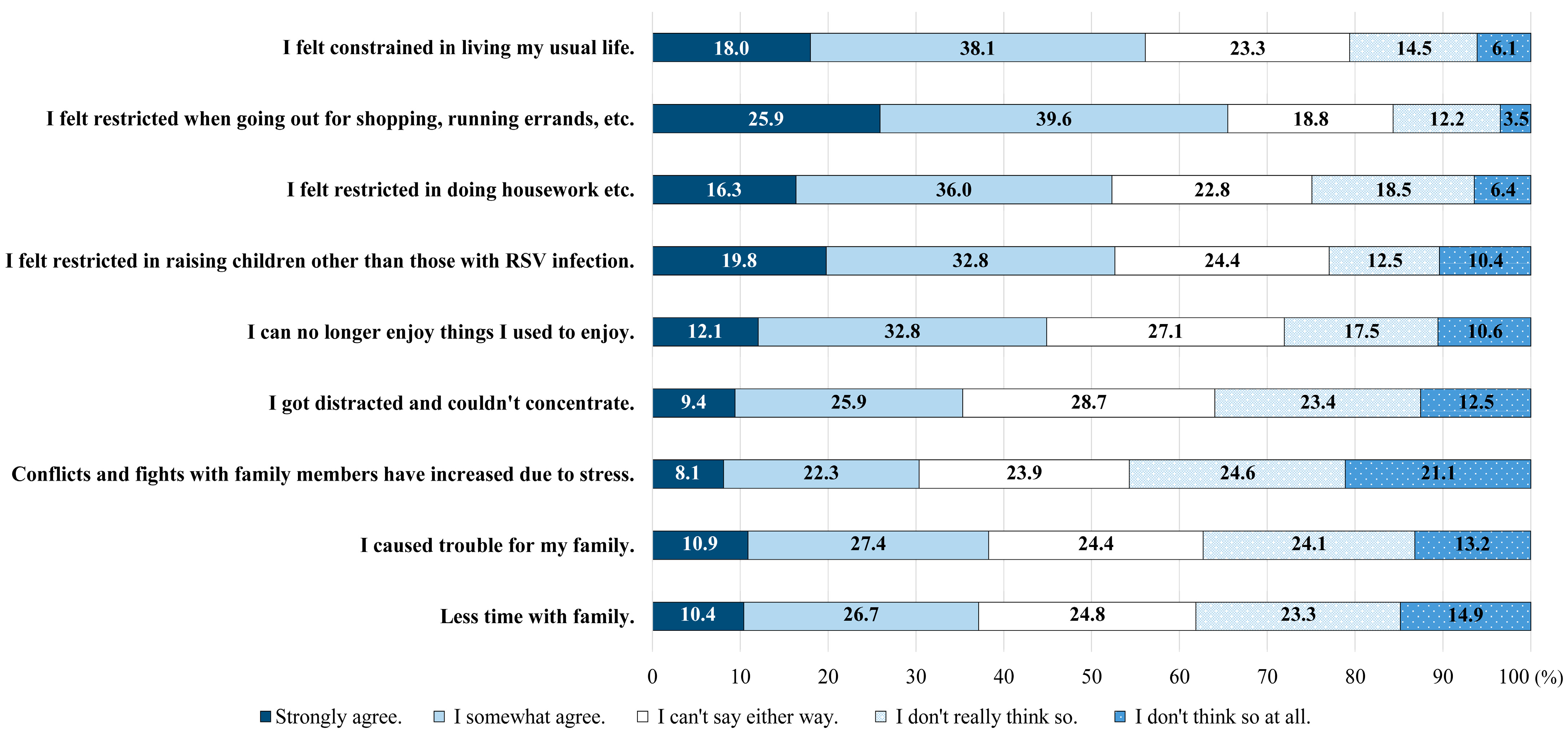
3.4. Impact of Infant with RSV Infection on Caregivers’ Daily Lives
3.5. Impact of Infant with RSV Infection on Caregivers’ Economic and Working Environment
3.6. Caregivers’ Preferences for RSV Prophylaxis (Route of Administration)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Li, Y.; Wang, X.; Blau, D.M.; Caballero, M.T.; Feikin, D.R.; Gill, C.J.; Madhi, S.A.; Omer, S.B.; Simões, E.A.F.; Campbell, H.; et al. Global, Regional, and National Disease Burden Estimates of Acute Lower Respiratory Infections Due to Respiratory Syncytial Virus in Children Younger than 5 Years in 2019: A Systematic Analysis. Lancet 2022, 399, 2047–2064. [Google Scholar] [CrossRef] [PubMed]
- IASR. Special Feature: RSV Infections from January 2014 to September 2018. 2018, Volume 39. Available online: https://www.niid.go.jp/niid/ja/id/542-disease-based/alphabet/respiratory-syncytial/idsc/iasr-topic/8473-466t.html (accessed on 7 June 2024).
- Miyairi, Department of Pediatrics, Hamamatsu University School of Medicine. Mechanisms of Severe RSV Infection. Available online: https://www.niid.go.jp/niid/ja/typhi-m/iasr-reference/2564-related-articles/related-articles-506/11084-506r03.html (accessed on 7 June 2024).
- IASR. Special Feature: RSV Infections from 2018–2021. 2022, Volume 43. Available online: https://www.niid.go.jp/niid/ja/rs-virus-m/rs-virus-iasrtpc/11081-506t.html (accessed on 7 June 2024).
- Kobayashi, Y.; Togo, K.; Agosti, Y.; McLaughlin, J.M. Epidemiology of Respiratory Syncytial Virus in Japan: A Nationwide Claims Database Analysis. Pediatr. Int. 2022, 64, e14957. [Google Scholar] [CrossRef] [PubMed]
- Mazur, N.I.; Terstappen, J.; Baral, R.; Bardají, A.; Beutels, P.; Buchholz, U.J.; Cohen, C.; Crowe, J.E., Jr.; Cutland, C.L.; Eckert, L.; et al. Respiratory Syncytial Virus Prevention within Reach: The Vaccine and Monoclonal Antibody Landscape. Lancet Infect. Dis. 2023, 23, e2–e21. [Google Scholar] [CrossRef] [PubMed]
- Scruggs-Wodkowski, E.A.; Malani, P.N.; Linder, K.A. Therapies to Decrease Severe Respiratory Syncytial Virus Illness. JAMA 2024, 331, 2127–2128. [Google Scholar] [CrossRef] [PubMed]
- Leidy, N.K.; Margolis, M.K.; Marcin, J.P.; Flynn, J.A.; Frankel, L.R.; Johnson, S.; Langkamp, D.; Simoes, E.A.F. The Impact of Severe Respiratory Syncytial Virus on the Child, Caregiver, and Family during Hospitalization and Recovery. Pediatrics 2005, 115, 1536–1546. [Google Scholar] [CrossRef]
- Pokrzywinski, R.M.; Swett, L.L.; Pannaraj, P.S.; Yi, J.; Pavilack, M.S.; Kumar, V.R.; McLaurin, K.K. Impact of Respiratory Syncytial Virus–Confirmed Hospitalizations on Caregivers of US Preterm Infants. Clin. Pediatr. 2019, 58, 837–850. [Google Scholar] [CrossRef] [PubMed]
- Glaser, E.L.; Hariharan, D.; Bowser, D.M.; Gervasio, R.M.; Rowlands, K.R.; Buckley, L.; Nelson, C.B.; Shepard, D.S. Impact of Respiratory Syncytial Virus on Child, Caregiver, and Family Quality of Life in the United States: Systematic Literature Review and Analysis. J. Infect. Dis. 2022, 226, S236–S245. [Google Scholar] [CrossRef]
- Okubo, Y.; Uda, K.; Ogimi, C.; Shimabukuro, R.; Ito, K. Clinical Practice Patterns and Risk Factors for Severe Conditions in Pediatric Hospitalizations with Respiratory Syncytial Virus in Japan: A Nationwide Analyses (2018–2022). Pediatr. Infect. Dis. J. 2024, 43, 187–193. [Google Scholar] [CrossRef] [PubMed]
- Wrotek, A.; Wrotek, O.; Jackowska, T. The Estimate of Parental Quality of Life Loss Due to Respiratory Syncytial Virus (RSV) Hospitalization. Diseases 2023, 11, 126. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, I.; Defoy, I.; Grubb, E. Burden of Respiratory Syncytial Virus Hospitalizations in Canada. Can. Respir. J. 2017, 2017, 4521302. [Google Scholar] [CrossRef] [PubMed]
- Hak, S.F.; Venekamp, R.P.; Billard, M.-N.; van Houten, M.A.; Pollard, A.J.; Heikkinen, T.; Cunningham, S.; Millar, M.; Mar-tinón-Torres, F.; Dacosta-Urbieta, A.; et al. Substantial Burden of Nonmedically Attended RSV Infection in Healthy-Term In-fants: An International Prospective Birth Cohort Study. J. Infect. Dis. 2024, 229, S40–S50. [Google Scholar] [CrossRef] [PubMed]
- Child and Family Agency. Survey on Medical Expense Assistance for Children, Fiscal Years 2022–2023. Available online: https://www.cfa.go.jp/policies/boshihoken/kodomoiryouhityousa-r4r5 (accessed on 7 June 2024).
- Takaku, R. Effects of Reduced Cost-Sharing on Children’s Health: Evidence from Japan. Soc. Sci. Med. 2016, 151, 46–55. [Google Scholar] [CrossRef] [PubMed]
- Mahadevia, P.J.; Masaquel, A.S.; Polak, M.J.; Weiner, L.B. Cost Utility of Palivizumab Prophylaxis among Pre-Term Infants in the United States: A National Policy Perspective. J. Med. Econ. 2012, 15, 987–996. [Google Scholar] [CrossRef] [PubMed]
- Neovius, K.; Buesch, K.; Sandström, K.; Neovius, M. Cost-Effectiveness Analysis of Palivizumab as Respiratory Syncytial Virus Prophylaxis in Preterm Infants in Sweden. Acta Paediatr. 2011, 100, 1306–1314. [Google Scholar] [CrossRef] [PubMed]
- Japan Pediatric Society. Position on Maternal Immunization Against RSV. Japan Pediatric Society. Available online: https://www.jpeds.or.jp/modules/activity/index.php?content_id=559 (accessed on 19 August 2024).
- Available online: https://www.jpeds.or.jp/uploads/files/20240522Beyfortus_GL.pdf (accessed on 19 August 2024).
- Approximately 120,000 to 140,000 Infants under the Age of 2 Are Diagnosed Annually with RSV Infections in Japan. Available online: https://www.jsog.or.jp/news/pdf/infection03.pdf (accessed on 19 August 2024).
- Fleming-Dutra, K.E.; Jones, J.M.; Roper, L.E.; Prill, M.M.; Ortega-Sanchez, I.R.; Moulia, D.L.; Wallace, M.; Godfrey, M.; Broder, K.R.; Tepper, N.K.; et al. Use of the Pfizer Respiratory Syncytial Virus Vaccine during Pregnancy for the Prevention of Respir-atory Syncytial Virus–Associated Lower Respiratory Tract Disease in Infants: Recommendations of the Advisory Committee on Immunization Practices—United States, 2023. MMWR Morb. Mortal. Wkly. Rep. 2023, 72, 1115–1122. [Google Scholar] [PubMed]
- Respiratory Syncytial Virus (RSV) Immunisation Programme: JCVI Advice, 7 June 2023. Available online: https://www.gov.uk/government/publications/rsv-immunisation-programme-jcvi-advice-7-june-2023/respiratory-syncytial-virus-rsv-immunisation-programme-jcvi-advice-7-june-2023 (accessed on 19 August 2024).
- Recommandation Vaccinale Contre les Infections à VRS Chez les Femmes Enceintes. Available online: https://www.has-sante.fr/jcms/p_3505344/fr/consultation-publique-sur-la-recommandation-vaccinale-contre-les-infections-a-vrs-chez-les-femmes-enceintes (accessed on 19 August 2024).
- Moline, H.L.; Tannis, A.; Toepfer, A.P.; Williams, J.V.; Boom, J.A.; Englund, J.A.; Halasa, N.B.; Staat, M.A.; Weinberg, G.A.; Selvarangan, R.; et al. Early Estimate of Nirsevimab Effectiveness for Prevention of Respiratory Syncytial Virus-Associated Hospitalization among Infants Entering Their First Respiratory Syncytial Virus Season—New Vaccine Surveillance Network, October 2023–February 2024. MMWR Morb. Mortal. Wkly. Rep. 2024, 73, 209–214. [Google Scholar] [CrossRef] [PubMed]
- Available online: https://www.cdc.gov/vaccines/acip/meetings/downloads/slides-2024-06-26-28/03-RSV-Mat-Peds-Moro-508.pdf (accessed on 19 August 2024).
- Maternal Respiratory Syncytial Virus Vaccination. Available online: https://www.acog.org/clinical/clinical-guidance/practice-advisory/articles/2023/09/maternal-respiratory-syncytial-virus-vaccination (accessed on 19 August 2024).

{kind=link}
{kind=link}
{kind=link}
| No. of Responders (%) | All | ||
|---|---|---|---|
| n = 606 | |||
| Infants with RSV | Sex | Male | 380 (62.7%) |
| Female | 226 (37.3%) | ||
| Infant age at infection (months) | ≥0 to <6 months | 303 (50.0%) | |
| ≥0 to <3 months | 200 (33.0%) | ||
| ≥3 to <6 months | 103 (17.0%) | ||
| ≥6 to <12 months | 303 (50.0%) | ||
| Birth weight | <2500 g | 64 (10.6%) | |
| ≥2500 g | 542 (89.4%) | ||
| Gestational age at infant’s birth | <37 weeks | 107 (17.7%) | |
| ≥37 weeks | 499 (82.3%) | ||
| Use of childcare facilities for RSV-infected infant | Yes | 257 (42.4%) | |
| No | 349 (57.6%) | ||
| Caregiver | Age | Mean (SD) | 34.2 (5.6) |
| Median (Q1, Q3) | 34.0 (30.0, 37.0) | ||
| Min, max | 20,57 | ||
| 20–24 years | 12 (2.0%) | ||
| 25–29 years | 111 (18.3%) | ||
| 30–34 years | 208 (34.3%) | ||
| 35–39 years | 174 (28.7%) | ||
| 40–44 years | 69 (11.4%) | ||
| 45–49 years | 24 (4.0%) | ||
| 50–54 years | 6 (1.0%) | ||
| 55–59 years | 2 (0.3%) | ||
| ≥60 years | 0 (0%) | ||
| Sex | Male | 128 (21.1%) | |
| Female | 478 (78.9%) | ||
| Annual household income (JPY) | <2,000,000 | 9 (1.5%) | |
| 2,000,000–4,000,000 | 77 (12.7%) | ||
| 4,000,000–6,000,000 | 105 (17.3%) | ||
| 6,000,000–8,000,000 | 92 (15.2%) | ||
| 8,000,000–10,000,000 | 47 (7.8%) | ||
| 10,000,000–12,000,000 | 30 (5.0%) | ||
| 12,000,000–15,000,000 | 75 (12.4%) | ||
| 15,000,000–20,000,000 | 7 (1.2%) | ||
| ≥20,000,000 | 8 (1.3%) | ||
| Unknown | 48 (7.9%) | ||
| Not stated | 108 (17.8%) | ||
| Marital status at the time of RSV infection | Married | 578 (95.4%) | |
| Separated or bereaved | 19 (3.1%) | ||
| Unmarried | 9 (1.5%) | ||
| Involvement of caregiver in the care of infant | Primary caregiver (mainly cared for the infant) | 545 (89.9%) | |
| Someone else did the primary nursing care. | 61 (10.1%) | ||
| Not involved in nursing at all. | 0 (0%) | ||
| Employment status of caregiver | Full-time work (work in the office at least 3 days a week) | 230 (38.0%) | |
| Full-time work (work from home at least 3 days a week) | 21 (3.5%) | ||
| Short time/part time | 68 (11.2%) | ||
| During maternity or childcare leave | 174 (28.7%) | ||
| Other | 2 (0.3%) | ||
| Unemployed | 111 (18.3%) | ||
| Characteristics of RSV-infected infant | Use of palivizumab prophylaxis against RSV infection | Never administered | 427 (70.5%) |
| Palivizumab previously administered, discon-tinued prior to the RSV infection onset | 56 (9.2%) | ||
| Receiving palivizumab prophylaxis at the on-set of RSV infection | 34 (5.6%) | ||
| Don’t know/don’t remember | 89 (14.7%) | ||
| Risk factor for severe disease *** | Diagnosed with infant congenital heart disease | 12 (2.0%) | |
| Diagnosed with Down syndrome | 2 (0.3%) | ||
| Diagnosed with immunodeficiency (severe combined immunodeficiency, leukemia, hematopoietic cell/lung transplantation, etc.) | 7 (1.2%) | ||
| Diagnosed with bronchial asthma | 38 (6.3%) | ||
| Diagnosed with a lung disease such as chronic lung disease (bronchopulmonary dysplasia) or cystic fibrosis | 7 (1.2%) | ||
| Infant may be exposed to second-hand smoke (Infant may be in an area where someone is smoking in your home or car) | 57 (9.4%) | ||
| Exposed to human immunodeficiency virus (someone close to you, such as your mother, has been infected) | 11 (1.8%) | ||
| Childcare consisted mainly of artificial milk (powdered milk, etc.) | 147 (24.3%) | ||
| None of the above apply | 394 (65.0%) | ||
| Symptom *** | Sneezing | 209 (34.5%) | |
| Runny nose | 495 (81.7%) | ||
| Fever | 487 (80.4%) | ||
| Wheezing (breathing sounds such as whistling and wheezing) | 265 (43.7%) | ||
| Cough | 473 (78.1%) | ||
| Apnea (including feeling like you are about to stop breathing) | 19 (3.1%) | ||
| Dyspnea (breathing seems difficult, shortness of breath, etc.) | 83 (13.7%) | ||
| Sleeplessness | 132 (21.8%) | ||
| Decrease in suckling amount, decrease in food intake | 165 (27.2%) | ||
| Decreased urination volume | 42 (6.9%) | ||
| Irritability | 141 (23.3%) | ||
| Cramps | 11 (1.8%) | ||
| Paleness | 37 (6.1%) | ||
| Others | 17 (2.8%) | ||
| Don’t know/don’t remember | 5 (0.8%) | ||
| Hospitalization | Hospitalized | 219 (36.1%) | |
| Not hospitalized | 387 (63.9%) | ||
| Duration of hospitalization *** | Within 3 days | 20 (9.1%) | |
| 4–6 days | 60 (27.4%) | ||
| 7–9 days | 72 (32.9%) | ||
| 10–14 days | 45 (20.5%) | ||
| 15–30 days | 4 (1.8%) | ||
| >31 days | 2 (0.9%) | ||
| Still under treatment and not fully recovered | 16 (7.3%) | ||
| Type of treatment during hospitalization *,*** | Inspiration | 153 (69.9%) | |
| Internal medication (e.g., expectorants) | 149 (68.0%) | ||
| Oxygen therapy (oxygen mask, oxygen hood, etc., or oxygen administration for less severe cases than ventilation) | 132 (60.3%) | ||
| Drip management (intravenous infusion, etc.) | 162 (74.0%) | ||
| Antibacterial (antibiotics) | 82 (37.4%) | ||
| Steroid | 27 (12.3%) | ||
| Ventilatory management (use of ventilators in hospitalization, etc.) | 10 (4.6%) | ||
| Intensive care unit management (ICU) | 11 (5.0%) | ||
| Other (FA) | 3 (1.4%) | ||
| Don’t know/don’t remember | 2 (0.9%) | ||
| Ventilatory management or ICU ** | 15 (6.9%) | ||
| Complication *** | Upper respiratory tract infection (cold symptoms) | 104 (17.2%) | |
| Bronchitis (bronchiolitis) | 219 (36.1%) | ||
| Pneumonia | 42 (6.9%) | ||
| Otitis media | 46 (7.6%) | ||
| Febrile seizure | 22 (3.6%) | ||
| Encephalopathy/encephalitis | 4 (0.7%) | ||
| Other | 5 (0.8%) | ||
| No other diagnosis besides RSV infection | 282 (46.5%) | ||
| Answer | All | Sex of Caregiver | Hospitalization | Duration of Hospitalization or Disease | Infant Age at Infection | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| Male | Female | Hospitalized | Not Hospitalized | ≤6 days | ≥7 days | ≥0 to <6 months | ≥6 to <12 months | |||
| n = 606 | n = 128 | n = 478 | n = 219 | n = 387 | n = 80 | n = 123 | n = 303 | n = 303 | ||
| Didn’t interfere with your life | 255 (42.1%) | 73 (57.0%) | 182 (38.1%) | 69 (31.5%) | 186 (48.1%) | 32 (40.0%) | 24 (19.5%) | 133 (43.9%) | 122 (40.3%) | |
| You didn’t worry too much about your child and it didn’t interfere with your life. | 39 (6.4%) | 22 (17.2%) | 17 (3.6%) | 15 (6.8%) | 24 (6.2%) | 5 (6.3%) | 4 (3.3%) | 22 (7.3%) | 17 (5.6%) | |
| You were worried about your child, but it didn’t interfere with your life. | 216 (35.6%) | 51 (39.8%) | 165 (34.5%) | 54 (24.7%) | 162 (41.9%) | 27 (33.8%) | 20 (16.3%) | 111 (36.6%) | 105 (34.7%) | |
| Interfered with your life | 338 (55.8%) | 47 (36.7%) | 291 (60.9%) | 147 (67.1%) | 191 (49.4%) | 46 (57.5%) | 98 (79.7%) | 164 (54.1%) | 174 (57.4%) | |
| Worrying about your child has interfered with your life. | 235 (38.8%) | 28 (21.9%) | 207 (43.3%) | 96 (43.8%) | 139 (35.9%) | 21 (26.3%) | 74 (60.2%) | 106 (35.0%) | 129 (42.6%) | |
| You were extremely worried about your child and it interfered with your daily life. | 103 (17.0%) | 19 (14.8%) | 84 (17.6%) | 51 (23.3%) | 52 (13.4%) | 25 (31.3%) | 24 (19.5%) | 58 (19.1%) | 45 (14.9%) | |
| I don’t know/I don’t remember. | 13 (2.1%) | 8 (6.3%) | 5 (1.0%) | 3 (1.4%) | 10 (2.6%) | 2 (2.5%) | 1 (0.8%) | 6 (2.0%) | 7 (2.3%) | |
| Infant Age at RSV Infected | Odds Ratio | 95% CI | p-Value |
|---|---|---|---|
| ≥6 to <12 months | (reference) | ||
| <6 months | 1.43 | 0.95–2.16 | 0.083 |
| ||
| All | ||
| n = 606 | ||
| They had a financial burden. | 391 (64.5%) | |
| Medical expenses | 207 (34.2%) | |
| Transportation expenses for treatment | 117 (19.3%) | |
| Sick childcare (service to care for and care for sick children) | 42 (6.9%) | |
| Sitter fee (excluding children with RSV infection) | 26 (4.3%) | |
| Items that cost more than the usual food expenses for the entire household | 171 (28.2%) | |
| Hotel expenses for the caregiver or person being cared for | 21 (3.5%) | |
| Hospitalization costs (different bed charges, etc.) | 108 (17.8%) | |
| Others | 17 (2.8%) | |
| There was no financial burden. | 215 (35.5%) | |
| ||
| There was financial burden | ||
| n = 391 | ||
| JPY < 10,000 | 144 (36.8%) | |
| JPY 10,000–30,000 | 75 (19.2%) | |
| JPY 30,000–50,000 | 33 (8.4%) | |
| JPY 50,000–100,000 | 23 (5.9%) | |
| JPY 100,000–200,000 | 57 (14.6%) | |
| JPY 200,000–300,000 | 30 (7.7%) | |
| JPY 300,000–400,000 | 4 (1.0%) | |
| JPY 400,000–500,000 | 3 (0.8%) | |
| JPY 500,000–1 million | 3 (0.8%) | |
| JPY 1 million–2 million | 2 (0.5%) | |
| JPY ≥ 2 million | 0 (0%) | |
| I don’t know/I don’t remember | 17 (4.4%) | |
| ||
| Caregivers | Spouse/partner | |
| n = 321 | n = 469 | |
| I took paid leave. | 121 (37.7%) | 81 (17.3%) |
| I took unpaid leave. | 24 (7.5%) | 6 (1.3%) |
| Reduced working hours by leaving work early etc. | 142 (44.2%) | 126 (26.9%) |
| I had someone else follow up on my work. | 64 (19.5%) | 50 (10.7%) |
| I quit my job | 2 (0.6%) | 3 (0.6%) |
| Others | 3 (0.9%) | 5 (1.1%) |
| There was no particular impact. | 47 (14.6%) | 250 (53.3%) |
| Answer | All | Infant Age at Infection | Symptoms of Infant * | Type of Treatment during Hospitalization | Knowledge about RSV Infection | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| 0–6 Months | 6–12 Months | (A) | I Don’t Know/I Don’t Remember (B) | Other than(A)(B) | Ventilatory Management or ICU | No Ventilatory Management or ICU | I Had Never Heard of It ** | I Had Heard of It, but I Didn’t Know What Kind of Disease It Was. | I Had Heard of it and Had Some Idea of What Kind of Disease It Was. | ||
| n = 606 | n = 303 | n = 303 | n = 276 | n = 5 | n = 325 | n = 15 | n = 591 | n = 116 | n = 247 | n = 243 | |
| I would like to vaccinate | 466 (76.9%) | 226 (74.6%) | 240 (79.2%) | 220 (79.7%) | 3 (60.0%) | 243 (74.8%) | 14 (93.3%) | 452 (76.5%) | 82 (70.7%) | 201 (81.4%) | 183 (75.3%) |
| I would like to vaccinate my child after giving birth. | 230 (38.0%) | 94 (31.0%) | 136 (44.9%) | 88 (31.9%) | 1 (20.0%) | 141 (43.4%) | 4 (26.7%) | 226 (38.2%) | 47 (40.5%) | 121 (49.0%) | 62 (25.5%) |
| I would like to have the mother vaccinated during pregnancy *** | 236 (38.9%) | 132 (43.6%) | 104 (34.3%) | 132 (47.8%) | 2 (40.0%) | 102 (31.4%) | 10 (66.7%) | 226 (38.2%) | 35 (30.2%) | 80 (32.4%) | 121 (49.8%) |
| I don’t want either | 61 (10.1%) | 38 (12.5%) | 23 (7.6%) | 25 (9.1%) | 1 (20.0%) | 35 (10.8%) | 0 (0%) | 61 (10.3%) | 16 (13.8%) | 17 (6.9%) | 28 (11.5%) |
| I don’t know | 79 (13.0%) | 39 (12.9%) | 40 (13.2%) | 31 (11.2%) | 1 (20.0%) | 47 (14.5%) | 1 (6.7%) | 78 (13.2%) | 18 (15.5%) | 29 (11.7%) | 32 (13.2%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tanaka, M.; Morioka, I.; Funakoshi, Y.; Xu, L.; Kobayashi, Y.; Muramatu, A.; Ito, S. Impact of Child Respiratory Syncytial Virus-Confirmed Infections on Caregivers in Japan: A Web-Based Survey. J. Clin. Med. 2024, 13, 5355. https://doi.org/10.3390/jcm13185355
Tanaka M, Morioka I, Funakoshi Y, Xu L, Kobayashi Y, Muramatu A, Ito S. Impact of Child Respiratory Syncytial Virus-Confirmed Infections on Caregivers in Japan: A Web-Based Survey. Journal of Clinical Medicine. 2024; 13(18):5355. https://doi.org/10.3390/jcm13185355
Chicago/Turabian StyleTanaka, Mamoru, Ichiro Morioka, Yu Funakoshi, Linghua Xu, Yasuhiro Kobayashi, Akari Muramatu, and Shuhei Ito. 2024. "Impact of Child Respiratory Syncytial Virus-Confirmed Infections on Caregivers in Japan: A Web-Based Survey" Journal of Clinical Medicine 13, no. 18: 5355. https://doi.org/10.3390/jcm13185355
APA StyleTanaka, M., Morioka, I., Funakoshi, Y., Xu, L., Kobayashi, Y., Muramatu, A., & Ito, S. (2024). Impact of Child Respiratory Syncytial Virus-Confirmed Infections on Caregivers in Japan: A Web-Based Survey. Journal of Clinical Medicine, 13(18), 5355. https://doi.org/10.3390/jcm13185355