
A Novel Suture-Based Vascular Closure Device to Achieve Hemostasis after Venous or Arterial Access While Leaving Nothing behind: A Review of the Technological Assessment and Early Clinical Outcomes


{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Vascular Closure Device Design Development
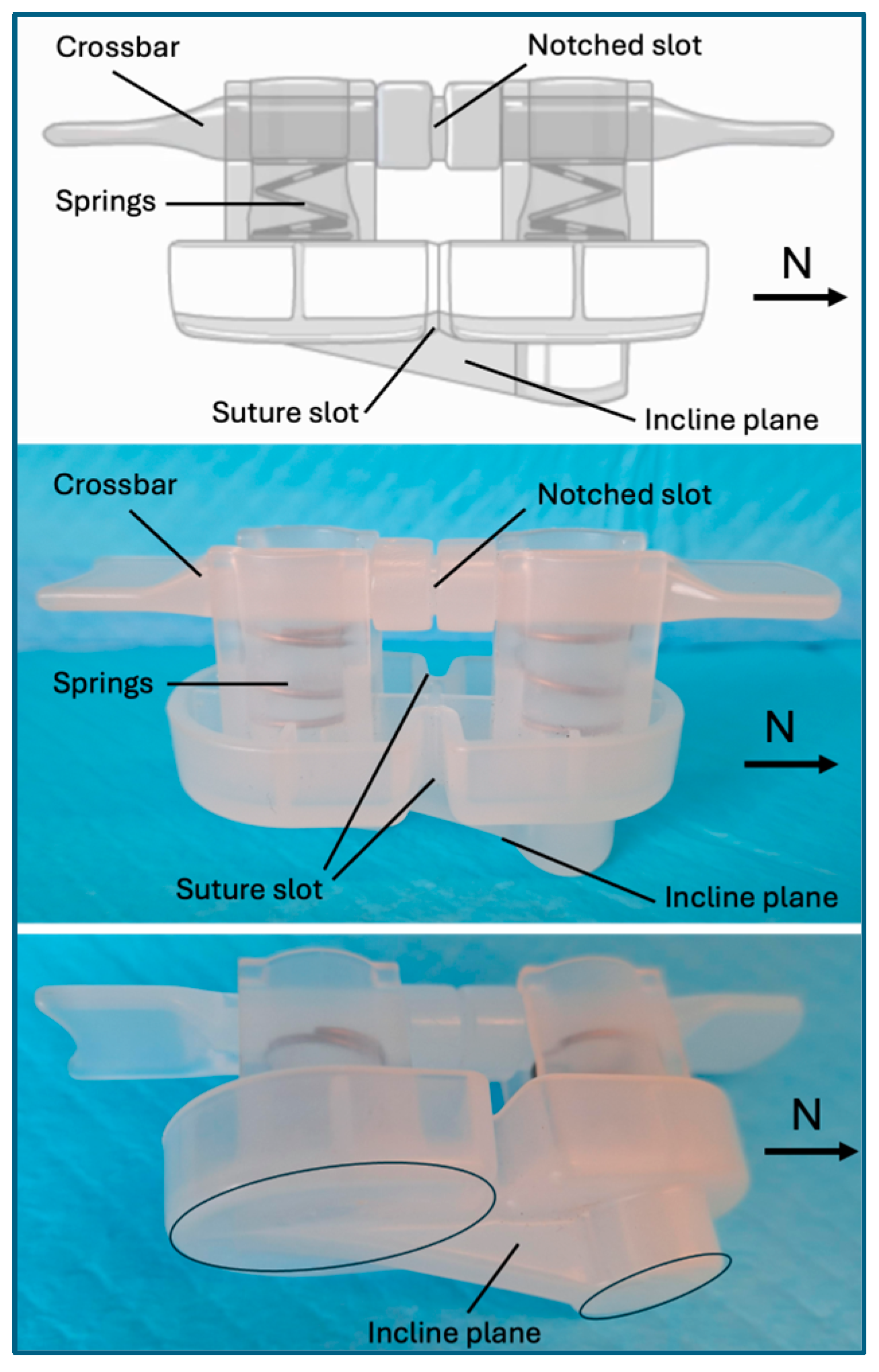
2.1. SiteSeal Vascular Closure Device
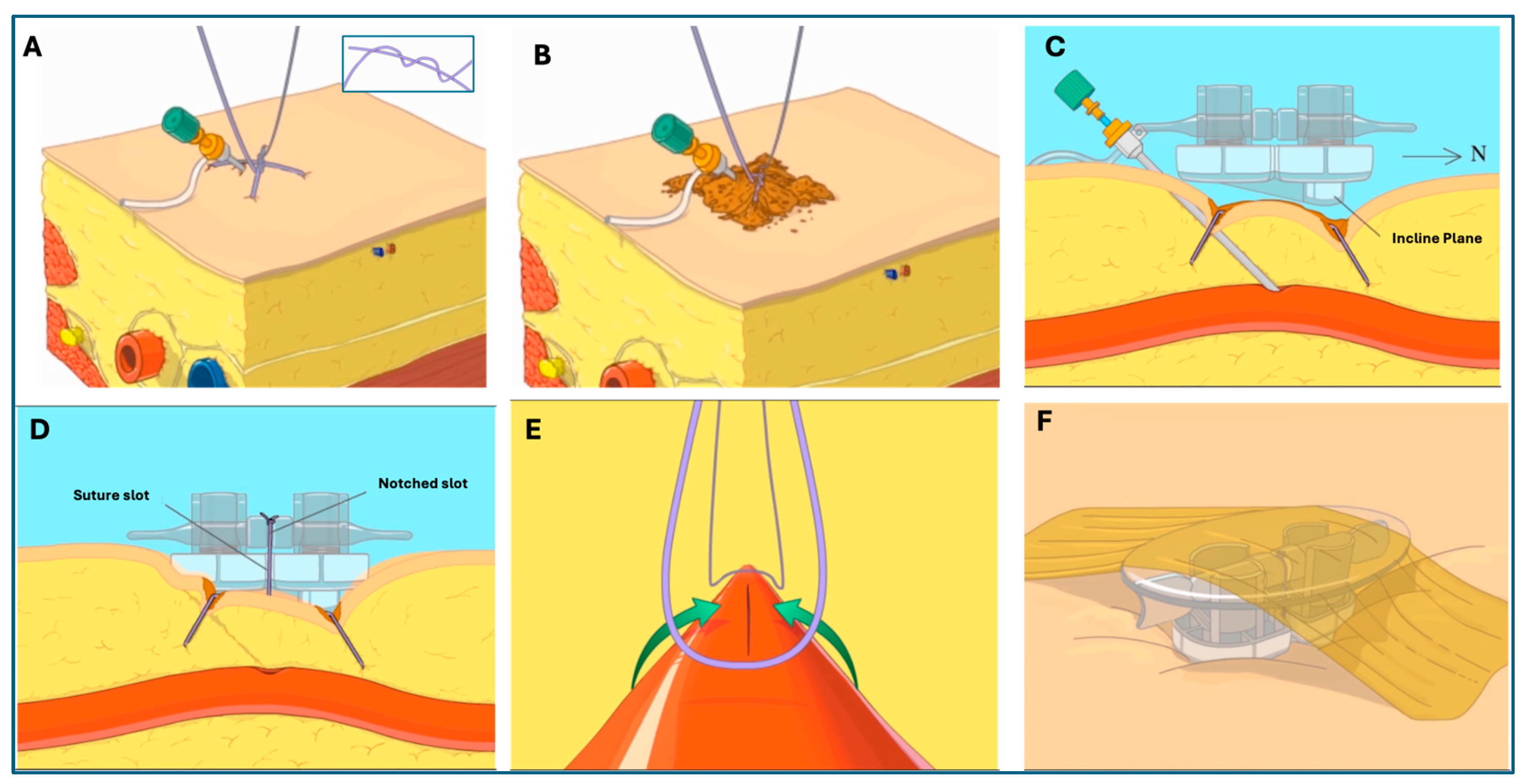
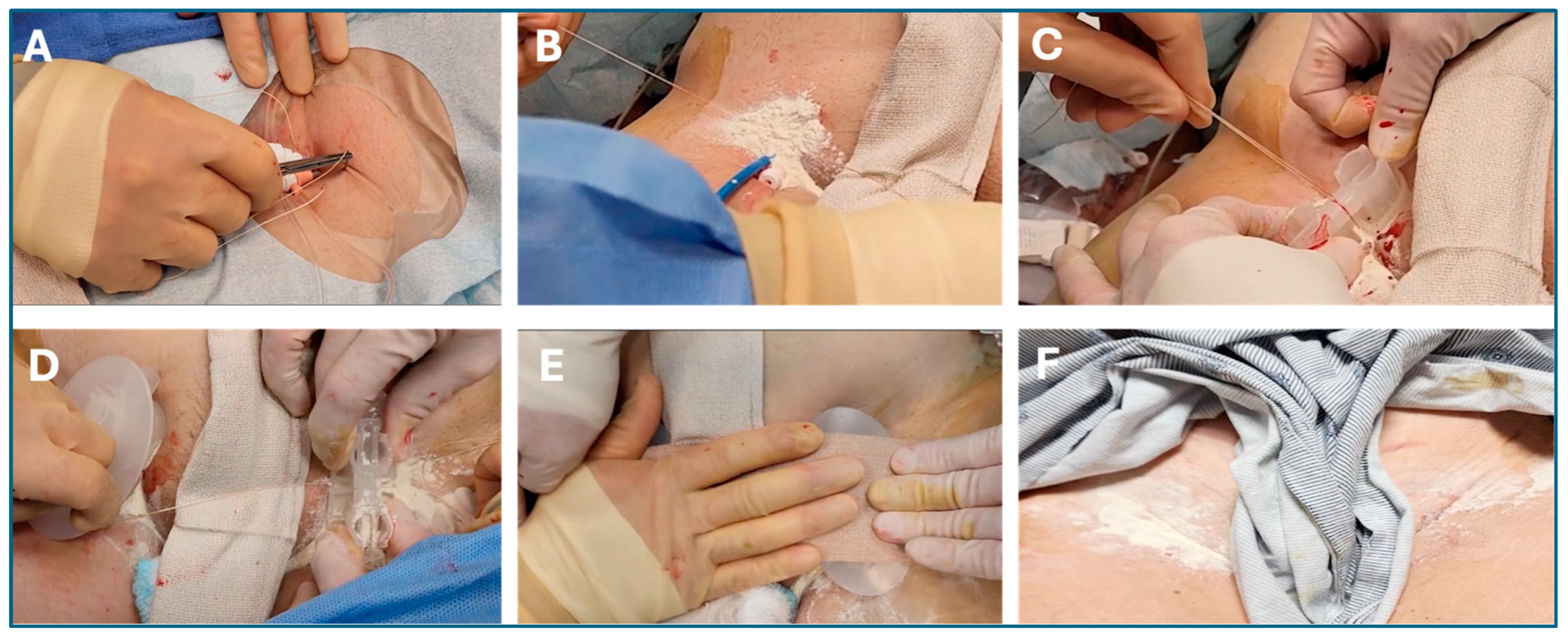
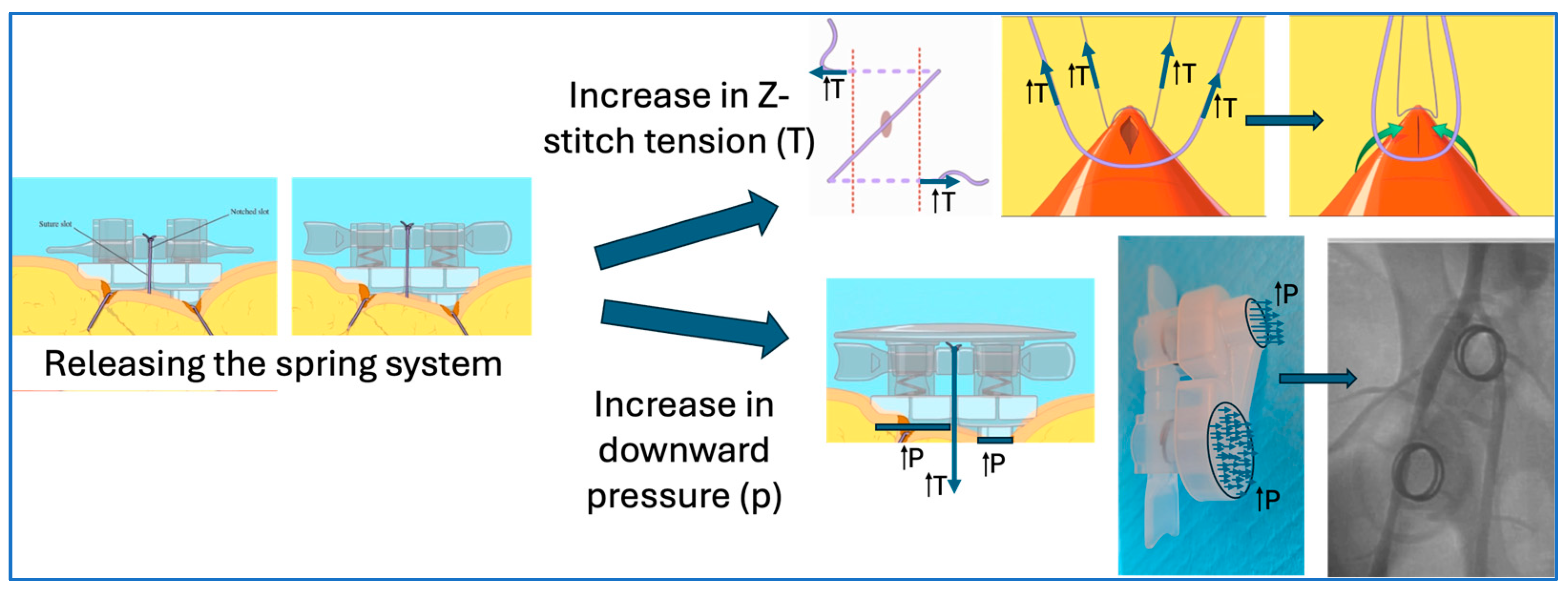
2.2. Deployment and Removal of the SiteSeal VCD
3. Clinical Experiences with the SiteSealTM VCD
4. Benefits of SiteSealTM VCD as Compared to Manual Compression and Figure-of-Eight Suture Techniques
5. Conclusions
Author Contributions
Funding
Informed Consent Statement
Conflicts of Interest
References
- Reynolds, D.; Duray, G.Z.; Omar, R.; Soejima, K.; Neuzil, P.; Zhang, S.; Narasimhan, C.; Steinwender, C.; Brugada, J.; Lloyd, M.; et al. A Leadless Intracardiac Transcatheter Pacing System. N. Engl. J. Med. 2016, 374, 533–541. [Google Scholar] [CrossRef] [PubMed]
- Calkins, H.; Hindricks, G.; Cappato, R.; Kim, Y.H.; Saad, E.B.; Aguinaga, L.; Akar, J.G.; Badhwar, V.; Brugada, J.; Camm, J.; et al. 2017 HRS/EHRA/ECAS/APHRS/SOLAECE expert consensus statement on catheter and surgical ablation of atrial fibrillation. Heart Rhythm. 2017, 14, e275–e444. [Google Scholar] [CrossRef]
- Hosseini, S.M.; Rozen, G.; Saleh, A.; Vaid, J.; Biton, Y.; Moazzami, K.; Heist, E.K.; Mansour, M.C.; Kaadan, M.I.; Vangel, M.; et al. Catheter Ablation for Cardiac Arrhythmias: Utilization and In-Hospital Complications, 2000 to 2013. JACC Clin. Electrophysiol. 2017, 3, 1240–1248. [Google Scholar] [CrossRef] [PubMed]
- Ali, M.; Shreenivas, S.S.; Pratt, D.N.; Lynch, D.R.; Kereiakes, D.J. Percutaneous Interventions for Secondary Mitral Regurgitation. Circ. Cardiovasc. Interv. 2020, 13, e008998. [Google Scholar] [CrossRef] [PubMed]
- Tzeis, S.; Gerstenfeld, E.P.; Kalman, J.; Saad, E.; Shamloo, A.S.; Andrade, J.G.; Barbhaiya, C.R.; Baykaner, T.; Boveda, S.; Calkins, H.; et al. 2024 European Heart Rhythm Association/Heart Rhythm Society/Asia Pacific Heart Rhythm Society/Latin American Heart Rhythm Society expert consensus statement on catheter and surgical ablation of atrial fibrillation. J. Interv. Card Electrophysiol. 2024, 26, euae043. [Google Scholar] [CrossRef]
- Mohammed, M.; Ramirez, R.; Steinhaus, D.A.; Yousuf, O.K.; Giocondo, M.J.; Ramza, B.M.; Wimmer, A.P.; Gupta, S.K. Comparative outcomes of vascular access closure methods following atrial fibrillation/flutter catheter ablation: Insights from VAscular Closure for Cardiac Ablation Registry. J. Interv. Card. Electrophysiol. 2022, 64, 301–310. [Google Scholar] [CrossRef]
- Pracon, R.; Bangalore, S.; Henzel, J.; Cendrowska-Demkow, I.; Pregowska-Chwala, B.; Tarnowska, A.; Dzielinska, Z.; Chmielak, Z.; Witkowski, A.; Demkow, M. A randomized comparison of modified subcutaneous "Z"-stitch versus manual compression to achieve hemostasis after large caliber femoral venous sheath removal. Catheter. Cardiovasc. Interv. 2018, 91, 105–112. [Google Scholar] [CrossRef] [PubMed]
- Gupta, S.; Kolluri, R.; Simoes, T.; Pingle, S.C.; Nie, H.; Lloyd, M.S.; Steinhaus, D.; Westerman, S.B.; Shah, A.; Kline, J.; et al. Safety of multi-access site venous closure following catheter ablation of atrial fibrillation and flutter. J. Interv. Card. Electrophysiol. 2024. [Google Scholar] [CrossRef]
- Natale, A.; Mohanty, S.; Liu, P.Y.; Mittal, S.; Al-Ahmad, A.; De Lurgio, D.B.; Horton, R.; Spear, W.; Bailey, S.; Bunch, J.; et al. Venous Vascular Closure System Versus Manual Compression Following Multiple Access Electrophysiology Procedures: The AMBULATE Trial. JACC Clin. Electrophysiol. 2020, 6, 111–124. [Google Scholar] [CrossRef]
- Barbetta, I.; van den Berg, J.C. Access and hemostasis: Femoral and popliteal approaches and closure devices-why, what, when, and how? Semin. Interv. Radiol. 2014, 31, 353–360. [Google Scholar] [CrossRef]
- Sairaku, A.; Nakano, Y.; Oda, N.; Makita, Y.; Kajihara, K.; Tokuyama, T.; Kihara, Y. Rapid hemostasis at the femoral venous access site using a novel hemostatic pad containing kaolin after atrial fibrillation ablation. J. Interv. Card. Electrophysiol. 2011, 31, 157–164. [Google Scholar] [CrossRef] [PubMed]
- Mohanty, S.; Trivedi, C.; Beheiry, S.; Al-Ahmad, A.; Horton, R.; Della Rocca, D.G.; Gianni, C.; Gasperetti, A.; Abdul-Moheeth, M.; Turakhia, M.; et al. Venous access-site closure with vascular closure device vs. manual compression in patients undergoing catheter ablation or left atrial appendage occlusion under uninterrupted anticoagulation: A multicentre experience on efficacy and complications. Europace 2019, 21, 1048–1054. [Google Scholar] [CrossRef] [PubMed]
- Cilingiroglu, M.; Salinger, M.; Zhao, D.; Feldman, T. Technique of temporary subcutaneous "Figure-of-Eight" sutures to achieve hemostasis after removal of large-caliber femoral venous sheaths. Catheter. Cardiovasc. Interv. 2011, 78, 155–160. [Google Scholar] [CrossRef] [PubMed]
- Traullé, S.; Kubala, M.; Doucy, A.; Quenum, S.; Hermida, J.S. Feasibility and safety of temporary subcutaneous venous figure-of-eight suture to achieve haemostasis after ablation of atrial fibrillation. Europace 2016, 18, 815–819. [Google Scholar] [CrossRef] [PubMed]
- Kumar, V.; Wish, M.; Venkataraman, G.; Bliden, K.; Jindal, M.; Strickberger, A. A randomized comparison of manual pressure versus figure-of-eight suture for hemostasis after cryoballoon ablation for atrial fibrillation. J. Cardiovasc. Electrophysiol. 2019, 30, 2806–2810. [Google Scholar] [CrossRef] [PubMed]
- Jensen, C.J.; Schnur, M.; Lask, S.; Attanasio, P.; Gotzmann, M.; Kara, K.; Hanefeld, C.; Mügge, A.; Wutzler, A. Feasibility of the Figure-of-8-Suture as Venous Closure in Interventional Electrophysiology: One Strategy for All? Int. J. Med. Sci. 2020, 17, 965–969. [Google Scholar] [CrossRef] [PubMed]
- Atti, V.; Turagam, M.K.; Garg, J.; Alratroot, A.; Abela, G.S.; Rayamajhi, S.; Lakkireddy, D. Efficacy and safety of figure-of-eight suture versus manual pressure for venous access closure: A systematic review and meta-analysis. J. Interv. Card. Electrophysiol. 2020, 57, 379–385. [Google Scholar] [CrossRef] [PubMed]
- Bin Waleed, K.; Leung, L.W.; Akhtar, Z.; Sohal, M.; Zuberi, Z.; Gallagher, M.M. New approaches to achieving hemostasis after venous access in cardiovascular patients. Kardiol. Pol. 2022, 80, 750–759. [Google Scholar] [CrossRef] [PubMed]
- Mujer, M.T.; Al-Abcha, A.; Flores, J.; Saleh, Y.; Robinson, P. A comparison of figure-of-8-suture versus manual compression for venous access closure after cardiac procedures: An updated meta-analysis. Pacing Clin. Electrophysiol. 2020, 43, 856–865. [Google Scholar] [CrossRef]
- Gianni, C.; Chafizadeh, T.; Della Rocca, D.G.; Mohanty, S.; Al-Ahmad, A.; Burkhardt, J.D.; Gallinghouse, G.J.; Horton, R.P.; Hranitzky, P.M.; Sanchez, J.E.; et al. Comparison of Three Vascular Closure Devices for Vascular Access Closure After Cardiac Electrophysiology Procedures. Circulation 2022, 146, A14277. [Google Scholar] [CrossRef]
- Dangas, G.; Mehran, R.; Kokolis, S.; Feldman, D.; Satler, L.F.; Pichard, A.D.; Kent, K.M.; Lansky, A.J.; Stone, G.W.; Leon, M.B. Vascular complications after percutaneous coronary interventions following hemostasis with manual compression versus arteriotomy closure devices. J. Am. Coll. Cardiol. 2001, 38, 638–641. [Google Scholar] [CrossRef] [PubMed]
- Okada, M.; Inoue, K.; Tanaka, K.; Ninomiya, Y.; Hirao, Y.; Oka, T.; Tanaka, N.; Inoue, H.; Nakamaru, R.; Koyama, Y.; et al. Efficacy and Safety of Figure-of-Eight Suture for Hemostasis After Radiofrequency Catheter Ablation for Atrial Fibrillation. Circ. J. Off. J. Jpn. Circ. Soc. 2018, 82, 956–964. [Google Scholar] [CrossRef] [PubMed]
- Anderson, F.A., Jr.; Spencer, F.A. Risk factors for venous thromboembolism. Circulation 2003, 107 (Suppl. 1), I9–I16. [Google Scholar] [CrossRef] [PubMed]
- Yorgun, H.; Canpolat, U.; Ates, A.H.; Oksul, M.; Sener, Y.Z.; Akkaya, F.; Aytemir, K. Comparison of standard vs modified "figure-of-eight" suture to achieve femoral venous hemostasis after cryoballoon based atrial fibrillation ablation. Pacing Clin. Electrophysiol. 2019, 42, 1175–1182. [Google Scholar] [CrossRef] [PubMed]
- Rasmussen, C.W.; Korsholm, K.; Kramer, A.D.; Nielsen-Kudsk, J.E.; Andersen, A. Figure-of-eight suture combined with a three-way stopcock for venous closure following left atrial appendage occlusion or patent foramen ovale closure. Interv. Cardiol. 2021, 13, 392–399. [Google Scholar]
- Corbin, C.L.; Kelley, S.W.; Schwartz, R.W. Concepts in service marketing for healthcare professionals. Am. J. Surg. 2001, 181, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, S.; Gallo, J.J.; Parashar, A.; Agarwal, K.K.; Ellis, S.G.; Khot, U.N.; Spooner, R.; Murat Tuzcu, E.; Kapadia, S.R. Impact of lean six sigma process improvement methodology on cardiac catheterization laboratory efficiency. Cardiovasc. Revascularization Med. Incl. Mol. Interv. 2016, 17, 95–101. [Google Scholar] [CrossRef]
- Payne, J.; Bickel, T.; Gautam, S. Figure-of-eight sutures for hemostasis result in shorter lab recovery time after ablation for atrial fibrillation. Pacing Clin. Electrophysiol. 2018, 41, 1017–1021. [Google Scholar] [CrossRef] [PubMed]
- Karahalios, B.; Rojas, S.F.; Singh, R.; Cavazos, M.C.; Chinnadurai, P.; Huie Lin, C. Torque device suture technique to achieve hemostasis in large-bore venous access. Catheter. Cardiovasc. Interv. 2020, 95, 722–725. [Google Scholar] [CrossRef]
- Pang, N.; Gao, J.; Zhang, B.; Guo, M.; Zhang, N.; Sun, M.; Wang, R. Vascular Closure Devices versus Manual Compression in Cardiac Interventional Procedures: Systematic Review and Meta-Analysis. Cardiovasc. Ther. 2022, 2022, 8569188. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yazdani, S.K.; Shedd, O.; Christy, G.; Teeslink, R. A Novel Suture-Based Vascular Closure Device to Achieve Hemostasis after Venous or Arterial Access While Leaving Nothing behind: A Review of the Technological Assessment and Early Clinical Outcomes. J. Clin. Med. 2024, 13, 4606. https://doi.org/10.3390/jcm13164606
Yazdani SK, Shedd O, Christy G, Teeslink R. A Novel Suture-Based Vascular Closure Device to Achieve Hemostasis after Venous or Arterial Access While Leaving Nothing behind: A Review of the Technological Assessment and Early Clinical Outcomes. Journal of Clinical Medicine. 2024; 13(16):4606. https://doi.org/10.3390/jcm13164606
Chicago/Turabian StyleYazdani, Saami K., Omer Shedd, George Christy, and Rex Teeslink. 2024. "A Novel Suture-Based Vascular Closure Device to Achieve Hemostasis after Venous or Arterial Access While Leaving Nothing behind: A Review of the Technological Assessment and Early Clinical Outcomes" Journal of Clinical Medicine 13, no. 16: 4606. https://doi.org/10.3390/jcm13164606
APA StyleYazdani, S. K., Shedd, O., Christy, G., & Teeslink, R. (2024). A Novel Suture-Based Vascular Closure Device to Achieve Hemostasis after Venous or Arterial Access While Leaving Nothing behind: A Review of the Technological Assessment and Early Clinical Outcomes. Journal of Clinical Medicine, 13(16), 4606. https://doi.org/10.3390/jcm13164606