
Serum Soluble IL-2 Receptors Are Elevated in Febrile Illnesses and Useful for Differentiating Clinically Similar Malignant Lymphomas from Kikuchi Disease: A Cross-Sectional Study

 , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Patient Inclusion and Exclusion Criteria
2.2. Classification of Patients
2.3. Evaluation of Serum sIL-2R
2.4. Laboratory Examination
2.5. Statistical Analysis
2.6. Ethical Approval
3. Results
3.1. Patient Clinical Background
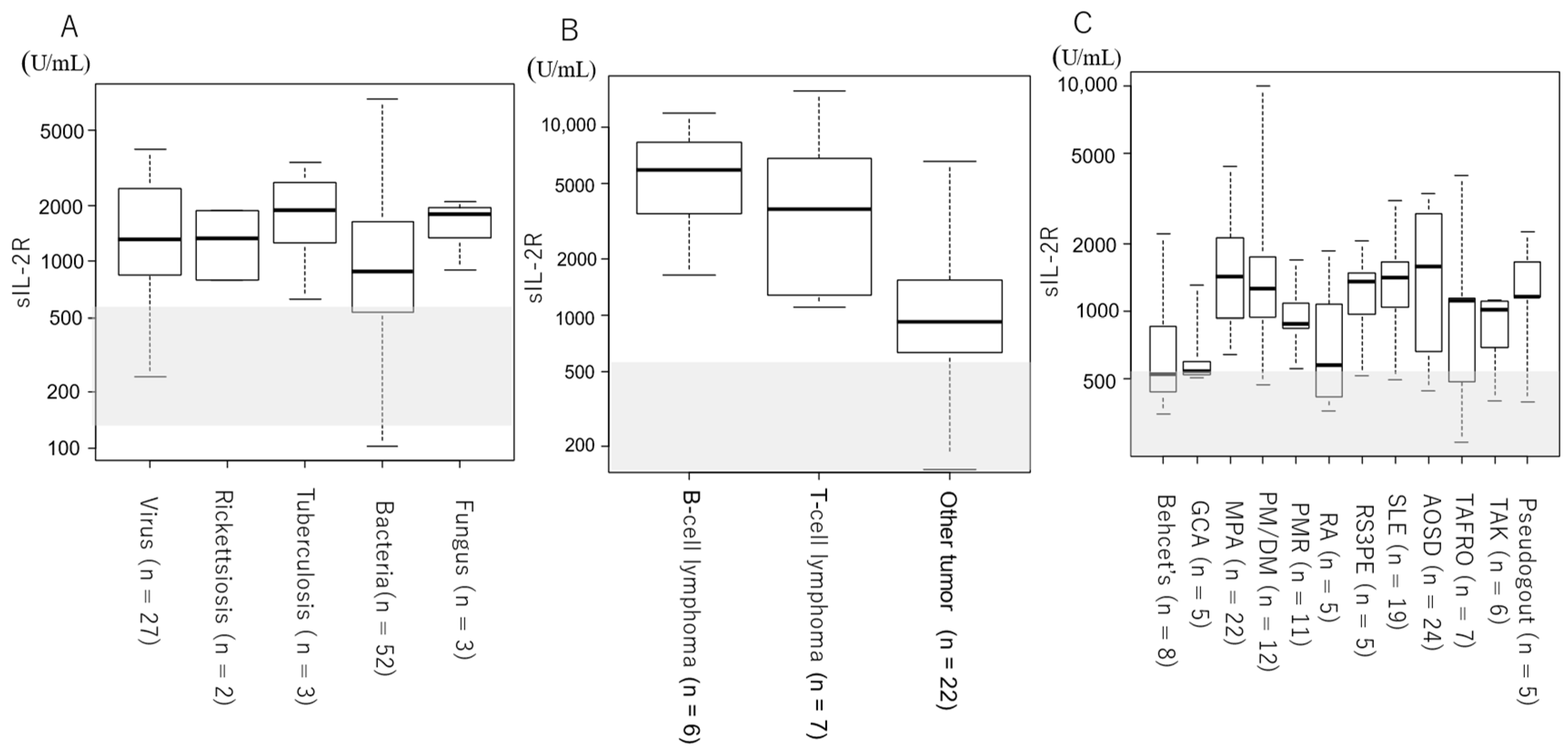
3.2. Serum sIL-2R Levels by Etiology and Disease
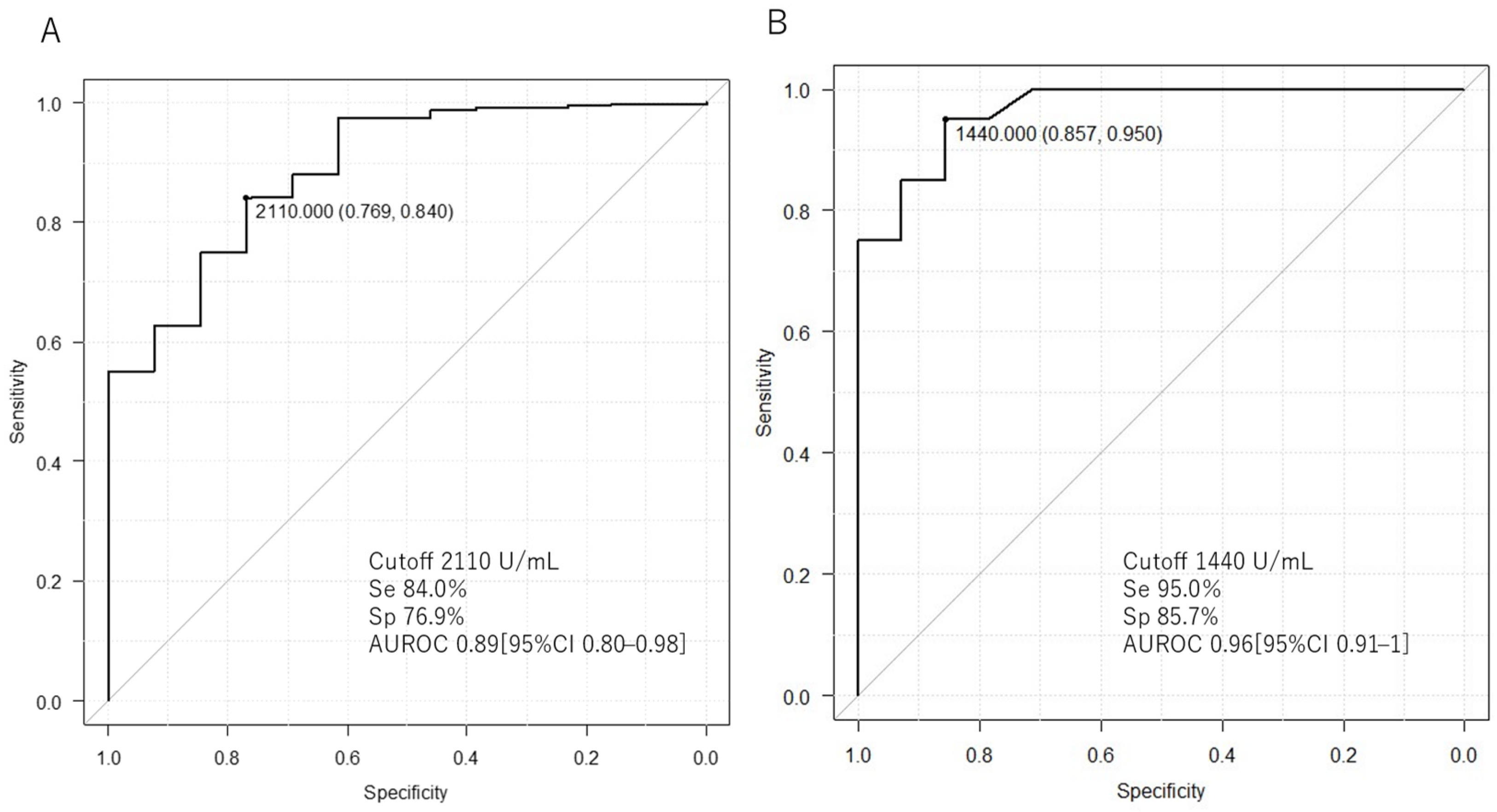
3.3. Comparison of Serum sIL-2R between ML and Non-ML
3.4. Comparison of Serum sIL-2R between ML and Kikuchi Disease
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Correction Statement
References
- Petersdorf, R.G.; Beeson, P.B. Fever of Unexplained Origin: Report on 100 Cases. Medicine 1961, 40, 1–30. [Google Scholar] [CrossRef]
- Durack, D.T.; Street, A.C. Fever of Unknown Origin—Reexamined and Redefined. Curr. Clin. Top Infect. Dis. 1991, 11, 35–51. [Google Scholar]
- Naito, T.; Mizooka, M.; Mitsumoto, F.; Kanazawa, K.; Torikai, K.; Ohno, S.; Morita, H.; Ukimura, A.; Mishima, N.; Otsuka, F.; et al. Diagnostic Workup for Fever of Unknown Origin: A Multicenter Collaborative Retrospective Study. BMJ Open 2013, 3, e003971. [Google Scholar] [CrossRef]
- Cunha, B.A.; Lortholary, O.; Cunha, C.B. Fever of Unknown Origin: A Clinical Approach. Am. J. Med. 2015, 128, 1138.e1–1138.e15. [Google Scholar] [CrossRef]
- Tal, S.; Guller, V.; Gurevich, A. Fever of Unknown Origin in Older Adults. Clin. Geriatr. Med. 2007, 23, 649–668. [Google Scholar] [CrossRef]
- Oka, K.; Tokumasu, K.; Hagiya, H.; Otsuka, F. Characteristics of Functional Hyperthermia Detected in an Outpatient Clinic for Fever of Unknown Origin. J. Clin. Med. 2024, 13, 889. [Google Scholar] [CrossRef]
- Olteanu, H.; Patnaik, M.; Koster, M.J.; Herrick, J.L.; Chen, D.; He, R.; Viswanatha, D.; Warrington, K.J.; Go, R.S.; Mangaonkar, A.A.; et al. Comprehensive Morphologic Characterization of Bone Marrow Biopsy Findings in a Large Cohort of Patients with VEXAS Syndrome: A Single-Institution Longitudinal Study of 111 Bone Marrow Samples from 52 Patients. Am. J. Clin. Pathol. 2024, aqad186. [Google Scholar] [CrossRef]
- Roth, A.R.; Basello, G.M. Approach to the Adult Patient with Fever of Unknown Origin. Am. Fam. Physician 2003, 68, 2223–2229. [Google Scholar]
- Naito, T.; Torikai, K.; Mizooka, M.; Mitsumoto, F.; Kanazawa, K.; Ohno, S.; Morita, H.; Ukimura, A.; Mishima, N.; Otsuka, F.; et al. Relationships between Causes of Fever of Unknown Origin and Inflammatory Markers: A Multicenter Collaborative Retrospective Study. Intern. Med. 2015, 54, 1989–1994. [Google Scholar] [CrossRef]
- Kanda, N.; Yamaguchi, R.; Yamamoto, Y.; Matsumura, M.; Hatakeyama, S. Performance of Serum Soluble Interleukin-2 Receptor as a Diagnostic Marker for Lymphoma in Patients with Fever. Sci. Rep. 2023, 13, 18784. [Google Scholar] [CrossRef]
- Rubin, L.A.; Nelson, D.L. The Soluble Interleukin-2 Receptor: Biology, Function, and Clinical Application. Ann. Intern. Med. 1990, 113, 619–627. [Google Scholar] [CrossRef]
- Lin, M.; Park, S.; Hayden, A.; Giustini, D.; Trinkaus, M.; Pudek, M.; Mattman, A.; Schneider, M.; Chen, L.Y.C. Clinical Utility of Soluble Interleukin-2 Receptor in Hemophagocytic Syndromes: A Systematic Scoping Review. Ann. Hematol. 2017, 96, 1241–1251. [Google Scholar] [CrossRef] [PubMed]
- Katsuya, H.; Shimokawa, M.; Ishitsuka, K.; Kawai, K.; Amano, M.; Utsunomiya, A.; Hino, R.; Hanada, S.; Jo, T.; Tsukasaki, K.; et al. Prognostic Index for Chronic- and Smoldering-Type Adult T-Cell Leukemia-Lymphoma. Blood 2017, 130, 39–47. [Google Scholar] [CrossRef] [PubMed]
- Sakthivel, P.; Bruder, D. Mechanism of Granuloma Formation in Sarcoidosis. Curr. Opin. Hematol. 2017, 24, 59–65. [Google Scholar] [CrossRef] [PubMed]
- Damoiseaux, J. The IL-2—IL-2 Receptor Pathway in Health and Disease: The Role of the Soluble IL-2 Receptor. Clin. Immunol. 2020, 218, 108515. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Li, Y.; Ding, X.; Zou, J.; Shen, B.; Liu, Z.; Lv, W.; Cao, X.; Xiang, F. The Significance of Serum Levels of Soluble Interleukin-2 Receptor in Patients Undergoing Maintenance Hemodialysis. Ren. Fail. 2020, 42, 419–427. [Google Scholar] [CrossRef] [PubMed]
- Kanda, Y. Investigation of the Freely Available Easy-to-Use Software “EZR” for Medical Statistics. Bone Marrow Transpl. 2013, 48, 452–458. [Google Scholar] [CrossRef] [PubMed]
- Maier, L.M.; Anderson, D.E.; Severson, C.A.; Baecher-Allan, C.; Healy, B.; Liu, D.V.; Wittrup, K.D.; De Jager, P.L.; Hafler, D.A. Soluble IL-2RA Levels in Multiple Sclerosis Subjects and the Effect of Soluble IL-2RA on Immune Responses. J. Immunol. 2009, 182, 1541–1547. [Google Scholar] [CrossRef] [PubMed]
- Giordano, C.; Galluzzo, A.; Marco, A.; Panto, F.; Amato, M.P.; Caruso, C.; Bompiani, G.D. Increased Soluble Interleukin-2 Receptor Levels in the Sera of Type 1 Diabetic Patients. Diabetes Res. 1988, 8, 135–138. [Google Scholar] [PubMed]
- Greenberg, S.J.; Marcon, L.; Hurwitz, B.J.; Waldmann, T.A.; Nelson, D.L.; Trotter, J.L.; Van Der Veen, R.C.; Clifford, D.B. Elevated Levels of Soluble Interleukin-2 Receptors in Multiple Sclerosis. N. Engl. J. Med. 1988, 319, 1019–1020. [Google Scholar] [CrossRef]
- Semenzato, G.; Bambara, L.M.; Biasi, D.; Frigo, A.; Vinante, F.; Zuppini, B.; Trentin, L.; Feruglio, C.; Chilosi, M.; Pizzolo, G. Increased Serum Levels of Soluble Interleukin-2 Receptor in Patients with Systemic Lupus Erythematosus and Rheumatoid Arthritis. J. Clin. Immunol. 1988, 8, 447–452. [Google Scholar] [CrossRef]
- Witkowska, A.M. On the Role of SIL-2R Measurements in Rheumatoid Arthritis and Cancers. Mediat. Inflamm. 2005, 2005, 121–130. [Google Scholar] [CrossRef] [PubMed]
- Ohno, H.; Ishikawa, T.; Kitajima, H.; Nomura, S.; Suzuki, T.; Konishi, H.; Ohno, Y.; Onishi, R.; Konaka, Y.; Arima, N.; et al. Significance of Soluble Interleukin-2 Receptor Alpha Chain in the Management of Patients with Malignant Lymphoma: A Multi-Center Study. [Rinsho Ketsueki] Jpn. J. Clin. Hematol. 2002, 43, 170–175. [Google Scholar]
- Mahajan, V.K.; Sharma, V.; Sharma, N.; Rani, R. Kikuchi-Fujimoto Disease: A Comprehensive Review. World J. Clin. Cases 2023, 11, 3664–3679. [Google Scholar] [CrossRef] [PubMed]
- Deaver, D.; Horna, P.; Cualing, H.; Sokol, L. Pathogenesis, Diagnosis, and Management of Kikuchi-Fujimoto Disease. Cancer Control 2014, 21, 313–321. [Google Scholar] [CrossRef]
- Brown, R.E.; Harave, S. Diagnostic Imaging of Benign and Malignant Neck Masses in Children-A Pictorial Review. Quant. Imaging Med. Surg. 2016, 6, 591. [Google Scholar] [CrossRef] [PubMed]
- Kernan, K.F.; Carcillo, J.A. Hyperferritinemia and Inflammation. Int. Immunol. 2017, 29, 401–409. [Google Scholar] [CrossRef]
- Ohshima, K.; Karube, K.; Hamasaki, M.; Makimoto, Y.; Fujii, A.; Kawano, R.; Tutiya, T.; Yamaguchi, T.; Suzumiya, J.; Kikuchi, M. Apoptosis- and Cell Cycle-Associated Gene Expression Profiling of Histiocytic Necrotising Lymphadenitis. Eur. J. Haematol. 2004, 72, 322–329. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Include HPS | Exclude HPS | Age, Years | Women (%) | sIL-2R (U/mL) | |
|---|---|---|---|---|---|
| Total | 351 | 344 | 63.5 (39–75) | 166 (48) | 1058 (646–1700) |
| Infection | 88 | 87 | 64 (41–73.50) | 31 (36) | 1010 (607–1865) |
| Autoimmune | 173 | 168 | 62 (38–75) | 93 (55) | 1105 (687–1643) |
| Tumor | 35 | 35 | 73 (62.75–80.00) | 16 (46) | 1408 (799–5420) |
| Drug fever | 11 | 11 | 57 (51.50–75.00) | 5 (45) | 764 (641–1200) |
| Kikuchi | 20 | 20 | 23 (18.75–33.25) | 11 (55) | 705 (538–1091) |
| Unknown | 24 | 23 | 69 (52.00–78.00) | 9 (36) | 824 (220–35,200) |
| n | sIL-2R (U/mL) | |
|---|---|---|
| Infection | 87 | 1010 (607–1865) |
| bacteria | 52 | 874 (537–1595) |
| virus | 27 | 1303 (841–2443) |
| Tuberculosis | 3 | 1870 (1249–2627) |
| Fungus | 3 | 1780 (1337–1936) |
| Rickettsiosis | 2 | 1328 (1062–1594) |
| Tumor | 35 | 1408 (799–5420) |
| ML | 13 | 4760 (2120–6730) |
| T-cell ML | 6 | 3630 (1590–6230) |
| ATLL | 1 | 6730 |
| T-LBL | 1 | 1106 |
| PTCL | 3 | 4730 (3630–10,115) |
| EATL | 1 | 1277 |
| B-cell ML | 7 | 5800 (3440–8275) |
| DLBCL | 4 | 7890 (4880–10,460) |
| IVL | 3 | 4760 (3190–5665) |
| Other tumor | 22 | 912 (652–1460) |
| Autoimmune | 168 | 1105 (687–1643) |
| Behcet’s | 8 | 523 (438–792) |
| GCA | 5 | 541 (523–595) |
| MPA | 22 | 1410 (991–2012) |
| PM/DM | 12 | 1250 (944–1667) |
| PMR | 11 | 871 (833–1085) |
| RA | 5 | 573 (416–1070) |
| RS3PE | 5 | 1340 (973–1480) |
| SLE | 19 | 1400 (1045–1645) |
| AOSD | 24 | 1575 (670–2665) |
| TAFRO | 7 | 1100 (485–1140) |
| TAK | 6 | 1013 (764–1094) |
| CPPD | 5 | 1160 (1160–1650) |
| n | sIL-2R (U/mL) | p-Value | |
| ML | 13 | 4760 (2120–6730) | <0.001 |
| non-ML | 331 | 998 (640–1625) | |
| n | Median [25–75%] | p-Value | |
| ML | 13 | 4760 (2120–6730) | <0.001 |
| Kikuchi | 20 | 705 (538–1091) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fuwa, M.; Tamai, Y.; Kato, A.; Asano, M.; Mori, I.; Watanabe, D.; Morita, H. Serum Soluble IL-2 Receptors Are Elevated in Febrile Illnesses and Useful for Differentiating Clinically Similar Malignant Lymphomas from Kikuchi Disease: A Cross-Sectional Study. J. Clin. Med. 2024, 13, 3248. https://doi.org/10.3390/jcm13113248
Fuwa M, Tamai Y, Kato A, Asano M, Mori I, Watanabe D, Morita H. Serum Soluble IL-2 Receptors Are Elevated in Febrile Illnesses and Useful for Differentiating Clinically Similar Malignant Lymphomas from Kikuchi Disease: A Cross-Sectional Study. Journal of Clinical Medicine. 2024; 13(11):3248. https://doi.org/10.3390/jcm13113248
Chicago/Turabian StyleFuwa, Masayuki, Yuya Tamai, Ayaka Kato, Motochika Asano, Ichiro Mori, Daichi Watanabe, and Hiroyuki Morita. 2024. "Serum Soluble IL-2 Receptors Are Elevated in Febrile Illnesses and Useful for Differentiating Clinically Similar Malignant Lymphomas from Kikuchi Disease: A Cross-Sectional Study" Journal of Clinical Medicine 13, no. 11: 3248. https://doi.org/10.3390/jcm13113248
APA StyleFuwa, M., Tamai, Y., Kato, A., Asano, M., Mori, I., Watanabe, D., & Morita, H. (2024). Serum Soluble IL-2 Receptors Are Elevated in Febrile Illnesses and Useful for Differentiating Clinically Similar Malignant Lymphomas from Kikuchi Disease: A Cross-Sectional Study. Journal of Clinical Medicine, 13(11), 3248. https://doi.org/10.3390/jcm13113248