

Robotic Lateral Pelvic Lymph Node Dissection in Rectal Cancer: A Feasibility Study from a European Centre


Abstract
:1. Introduction
2. Methods
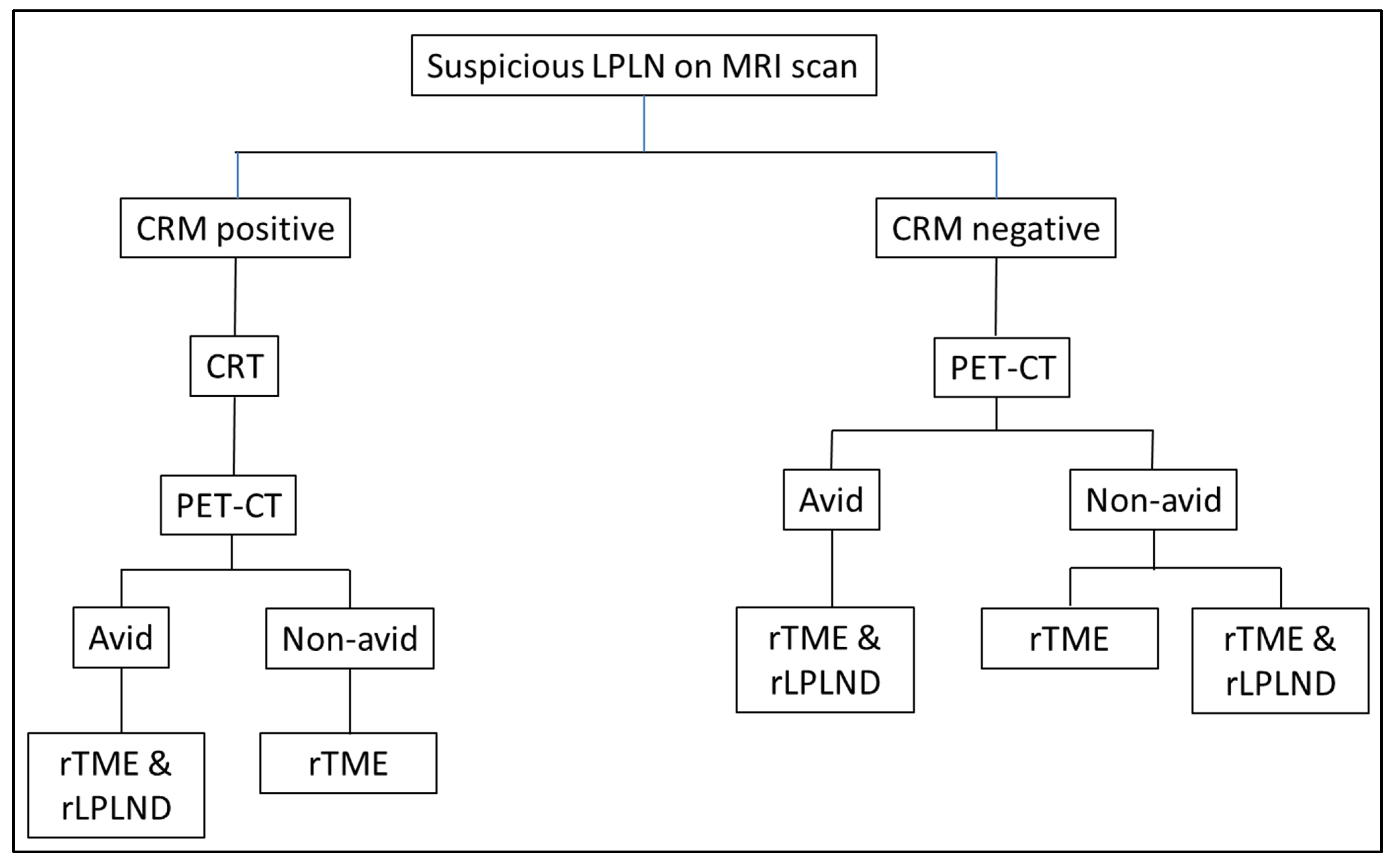
2.1. Patient Selection
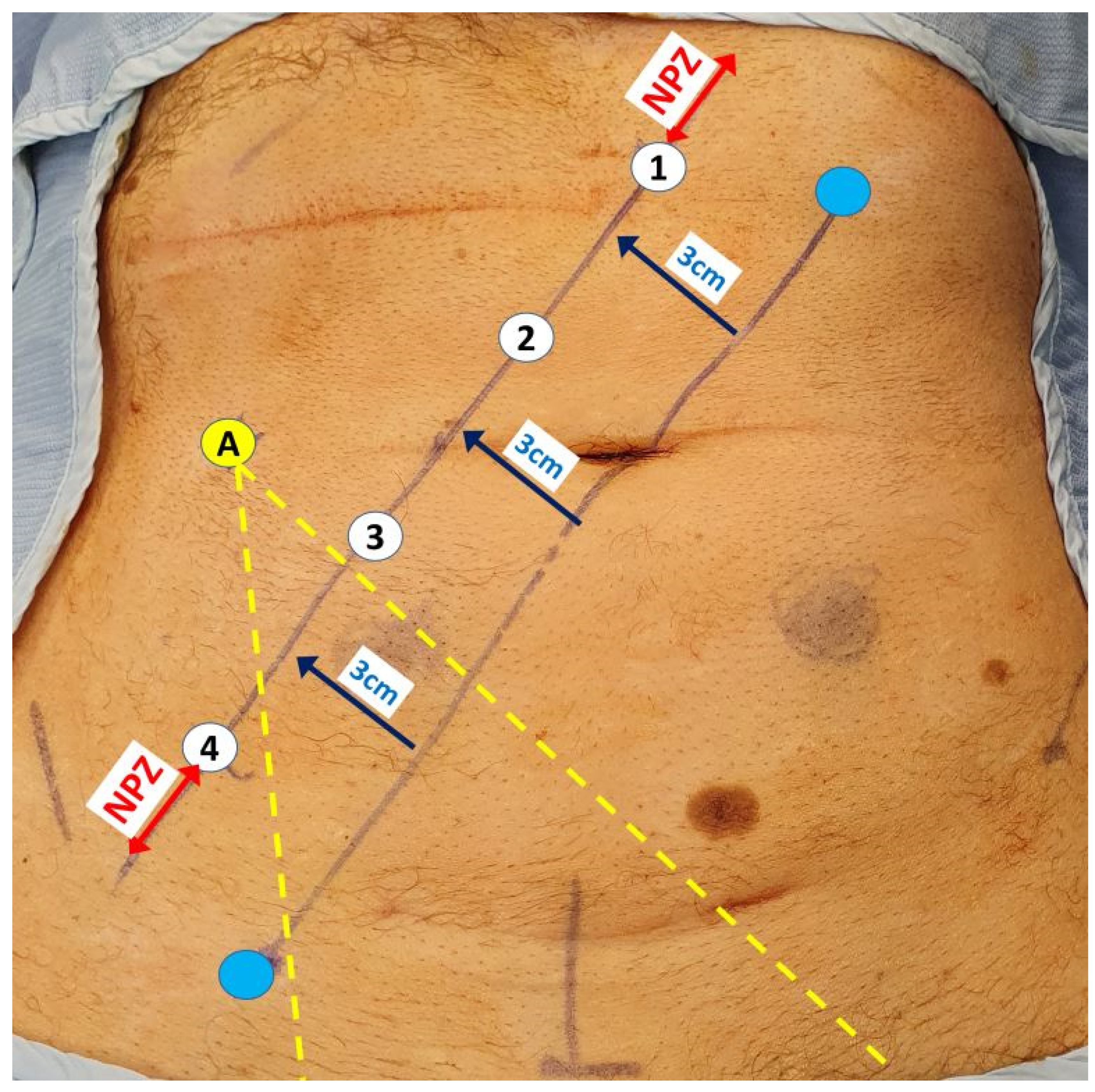
2.2. Robotic Setup
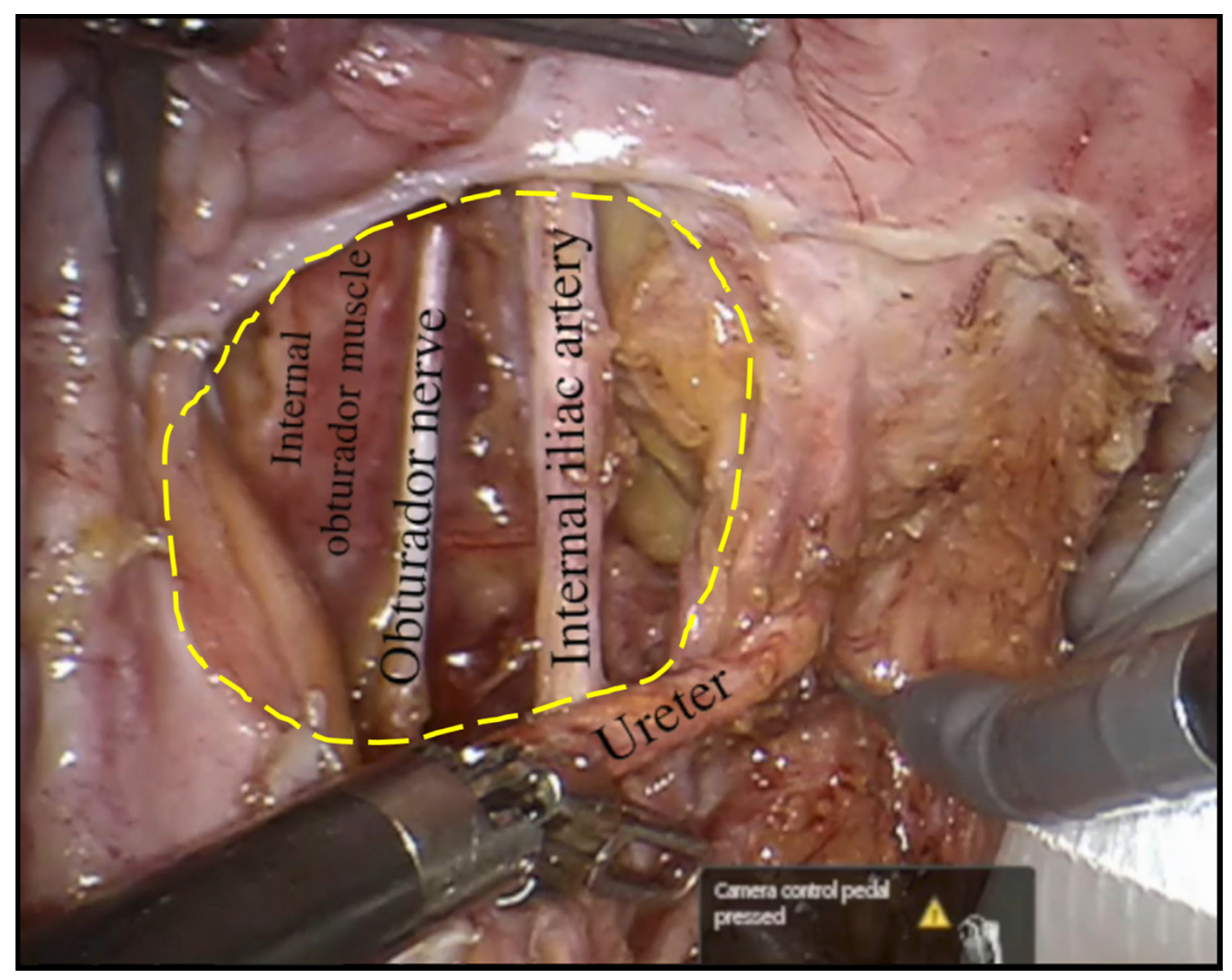
2.3. Anatomical Details and Surgical Technique
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Liu, Q.; Luo, D.; Cai, S.; Li, Q.; Li, X. Circumferential resection margin as a prognostic factor after rectal cancer surgery: A large population-based retrospective study. Cancer Med. 2018, 7, 3673–3681. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, T.; Muro, K.; Ajioka, Y.; Hashiguchi, Y.; Ito, Y.; Saito, Y.; Hamaguchi, T.; Ishida, H.; Ishiguro, M.; Ishihara, S.; et al. Japanese Society for Cancer of the Colon and Rectum (JSCCR) guidelines 2016 for the treatment of colorectal cancer. Int. J. Clin. Oncol. 2018, 23, 1–34. [Google Scholar] [CrossRef] [PubMed]
- Shimoyama, M.; Yamazaki, T.; Suda, T.; Hatakeyama, K. Prognostic significance of lateral lymph node micrometastases in lower rectal cancer: An immunohistochemical study with CAM5.2. Dis. Colon. Rectum. 2003, 46, 333–339. [Google Scholar] [CrossRef] [PubMed]
- Akiyoshi, T.; Watanabe, T.; Miyata, S.; Kotake, K.; Muto, T.; Sugihara, K. Results of a Japanese nationwide multi-institutional study on lateral pelvic lymph node metastasis in low rectal cancer: Is it regional or distant disease? Ann. Surg. 2012, 255, 1129–1134. [Google Scholar] [CrossRef] [PubMed]
- Sauer, R.; Becker, H.; Hohenberger, W.; Rödel, C.; Wittekind, C.; Fietkau, R.; Martus, P.; Tschmelitsch, J.; Hager, E.; Hess, C.F.; et al. Preoperative versus postoperative chemoradiotherapy for rectal cancer. N. Engl. J. Med. 2004, 351, 1731–1740. [Google Scholar] [CrossRef] [PubMed]
- Kapiteijn, E.; Marijnen, C.A.; Nagtegaal, I.D.; Putter, H.; Steup, W.H.; Wiggers, T.; Rutten, H.J.; Pahlman, L.; Glimelius, B.; Van Krieken, J.H.; et al. Preoperative radiotherapy combined with total mesorectal excision for resectable rectal cancer. N. Engl. J. Med. 2001, 345, 638–646. [Google Scholar] [CrossRef] [PubMed]
- Bosset, J.F.; Collette, L.; Calais, G.; Mineur, L.; Maingon, P.; Radosevic-Jelic, L.; Daban, A.; Bardet, E.; Beny, A.; Ollier, J.-C.; et al. Chemotherapy with preoperative radiotherapy in rectal cancer. N. Engl. J. Med. 2006, 355, 1114–1123. [Google Scholar] [CrossRef] [PubMed]
- Ogura, A.; Konishi, T.; Cunningham, C.; Garcia-Aguilar, J.; Iversen, H.; Toda, S.; Lee, I.K.; Lee, H.X.; Uehara, K.; Lee, P.; et al. Neoadjuvant (Chemo)radiotherapy With Total Mesorectal Excision Only Is Not Sufficient to Prevent Lateral Local Recurrence in Enlarged Nodes: Results of the Multicenter Lateral Node Study of Patients With Low cT3/4 Rectal Cancer. J. Clin. Oncol. 2019, 37, 33–43. [Google Scholar] [CrossRef] [PubMed]
- Nakanishi, R.; Yamaguchi, T.; Akiyoshi, T.; Nagasaki, T.; Nagayama, S.; Mukai, T.; Ueno, M.; Fukunaga, Y.; Konishi, T. Laparoscopic and robotic lateral lymph node dissection for rectal cancer. Surg. Today 2020, 50, 209–216. [Google Scholar] [CrossRef] [PubMed]
- Yamaguchi, T.; Kinugasa, Y.; Shiomi, A.; Tomioka, H.; Kagawa, H. Robotic-assisted laparoscopic versus open lateral lymph node dissection for advanced lower rectal cancer. Surg. Endosc. 2016, 30, 721–728. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.J.; Choi, G.S.; Park, J.S.; Park, S.Y.; Lee, H.J.; Woo, I.T.; Park, I.K. Selective lateral pelvic lymph node dissection: A comparative study of the robotic versus laparoscopic approach. Surg. Endosc. 2018, 32, 2466–2473. [Google Scholar] [CrossRef] [PubMed]
- Perez, R.O.; São Julião, G.P.; Vailati, B.B.; Fernandez, L.M.; Mattacheo, A.E.; Konishi, T. Lateral Node Dissection in Rectal Cancer in the Era of Minimally Invasive Surgery: A Step-by-Step Description for the Surgeon Unacquainted with This Complex Procedure with the Use of the Laparoscopic Approach. Dis. Colon. Rectum. 2018, 61, 1237–1240. [Google Scholar] [CrossRef] [PubMed]
- Khan, J.S.; Banerjee, A.K.; Kim, S.H.; Rockall, T.A.; Jayne, D.G. Robotic rectal surgery has advantages over laparoscopic surgery in selected patients and centres. Color. Dis. 2018, 20, 845–853. [Google Scholar] [CrossRef] [PubMed]
- Tejedor, P.; Sagias, F.; Nock, D.; Flashman, K.; Naqvi, S.; Kandala, N.L.; Khan, J.S. Advantages of using a robotic stapler in rectal cancer surgery. J. Robot. Surg. 2020, 14, 365–370. [Google Scholar] [CrossRef] [PubMed]
- Jayne, D.; Pigazzi, A.; Marshall, H.; Croft, J.; Corrigan, N.; Copeland, J.; Quirke, P.; West, N.; Rautio, T.; Thomassen, N.; et al. Effect of Robotic-Assisted vs Conventional Laparoscopic Surgery on Risk of Conversion to Open Laparotomy Among Patients Undergoing Resection for Rectal Cancer: The ROLARR Randomized Clinical Trial. JAMA 2017, 318, 1569–1580. [Google Scholar] [CrossRef] [PubMed]
- Heah, N.H.; Wong, K.Y. Feasibility of robotic assisted bladder sparing pelvic exenteration for locally advanced rectal cancer: A single institution case series. World J. Gastrointest. Surg. 2020, 12, 190–196. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age (year) | 63 (27–79) |
Sex
| 12 (71) 5 (29) |
| Body mass index (kg/m2) | 26 (20–40) |
| Neoadjuvant treatment | 6 (35) |
| 3 (18) 2 (12) 1 (6) |
| ASA grade | 2 (2–3) |
| Tumour distance from the anal verge (cm) | 6 (4–10) |
Laterality
| 15 (88) 2 (12) |
Operative procedure
| 10 (59) 1 (6) 6 (35) |
| Length of extraction site (cm) | 5 (4–6) |
| Intraoperative blood loss (ml) | 20 (0–100) |
| Operative time (minutes) | 280 (80–380) |
Pelvic drain
| 11 (65) 6 (35) |
| Peri-operative blood transfusion | 0 (0) |
| Length of HDU stay (days) | 1 (1–9) |
| Length of inpatient stay (days) | 7 (3–20) |
| Length of HDU stay (days) | 2 (1–9) |
| Post-operative complication | 3 (17) |
| 1 (6) 1 (6) 1 (6) |
Conversion
| 0 (0) 0 (0) |
| 30-day return to theatre | 0 (0) |
| Unplanned 30-day re-admission | 2 (12) |
| 1 (6) 1 (6) |
| Time to ileostomy reversal (months) | 7 (6–24) |
| Adjuvant chemotherapy | 9 (17) |
| Follow-up (months) | 18 (1–73) |
| Six-month local recurrence | 1 (6) |
| 4 |
| Number of LPLND-positive cases | 7 (41) |
| Number of lymph nodes harvested | 8 (1–18) |
| Number of positive lymph nodes | 1 (1–5) |
| LPLND specimen volume (mm3) | 48,000 (7200–115,000) |
| Tumour size (mm) | 40 (30–60) |
Histology
| 15 (88) 1 (6) 1 (6) |
Tumour grade
| 16 (100) 0 (0) |
| Rectal tumour resection margin R0 R1/2 | 11 (100) 0 (0) |
| LPLN Positive (n = 7) | LPLN Negative (n = 10) | |
|---|---|---|
| LN size, mm | 14 (12–15) * | 8 (4–15) * |
| Tumour height | 5 (5–6) ¥ | 7 (4–10) ƛ |
| Neoadjuvant treatment (yes/no) | 0/2 ¥ | 5/4 ƛ |
| Tumour size | 30 (30–35) ¥ | 48 (30–75) ƛ |
| EMVI/TD laterality positive (yes/no) | 1/1 ¥ | 6/3 ƛ |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chang, T.P.; Ali, O.; Tsimogiannis, K.; Sica, G.S.; Khan, J.S. Robotic Lateral Pelvic Lymph Node Dissection in Rectal Cancer: A Feasibility Study from a European Centre. J. Clin. Med. 2024, 13, 90. https://doi.org/10.3390/jcm13010090
Chang TP, Ali O, Tsimogiannis K, Sica GS, Khan JS. Robotic Lateral Pelvic Lymph Node Dissection in Rectal Cancer: A Feasibility Study from a European Centre. Journal of Clinical Medicine. 2024; 13(1):90. https://doi.org/10.3390/jcm13010090
Chicago/Turabian StyleChang, Tou Pin, Oroog Ali, Kostas Tsimogiannis, Giuseppe S. Sica, and Jim S. Khan. 2024. "Robotic Lateral Pelvic Lymph Node Dissection in Rectal Cancer: A Feasibility Study from a European Centre" Journal of Clinical Medicine 13, no. 1: 90. https://doi.org/10.3390/jcm13010090
APA StyleChang, T. P., Ali, O., Tsimogiannis, K., Sica, G. S., & Khan, J. S. (2024). Robotic Lateral Pelvic Lymph Node Dissection in Rectal Cancer: A Feasibility Study from a European Centre. Journal of Clinical Medicine, 13(1), 90. https://doi.org/10.3390/jcm13010090