
Trends of Diagnosis, Disease Course, and Treatment of Atopic Dermatitis 2012–2021: Real-World Data from a Large Healthcare Provider




Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Data Source
2.2. Study Population
- At least one AD diagnosis (Dx; ICD-9 691.8) from a specialist (dermatology or immunology/allergy);
- At least one AD Dx from hospital or medical approval records or ‘active diagnosis’;
- At least two AD Dx from a primary care physician (PCP; pediatrician or general practitioner (GP));
- At least one AD Dx (any physician) and purchased topical calcineurin inhibitors.
2.3. Study Variables and Definitions
2.4. Statistical Analysis
3. Results
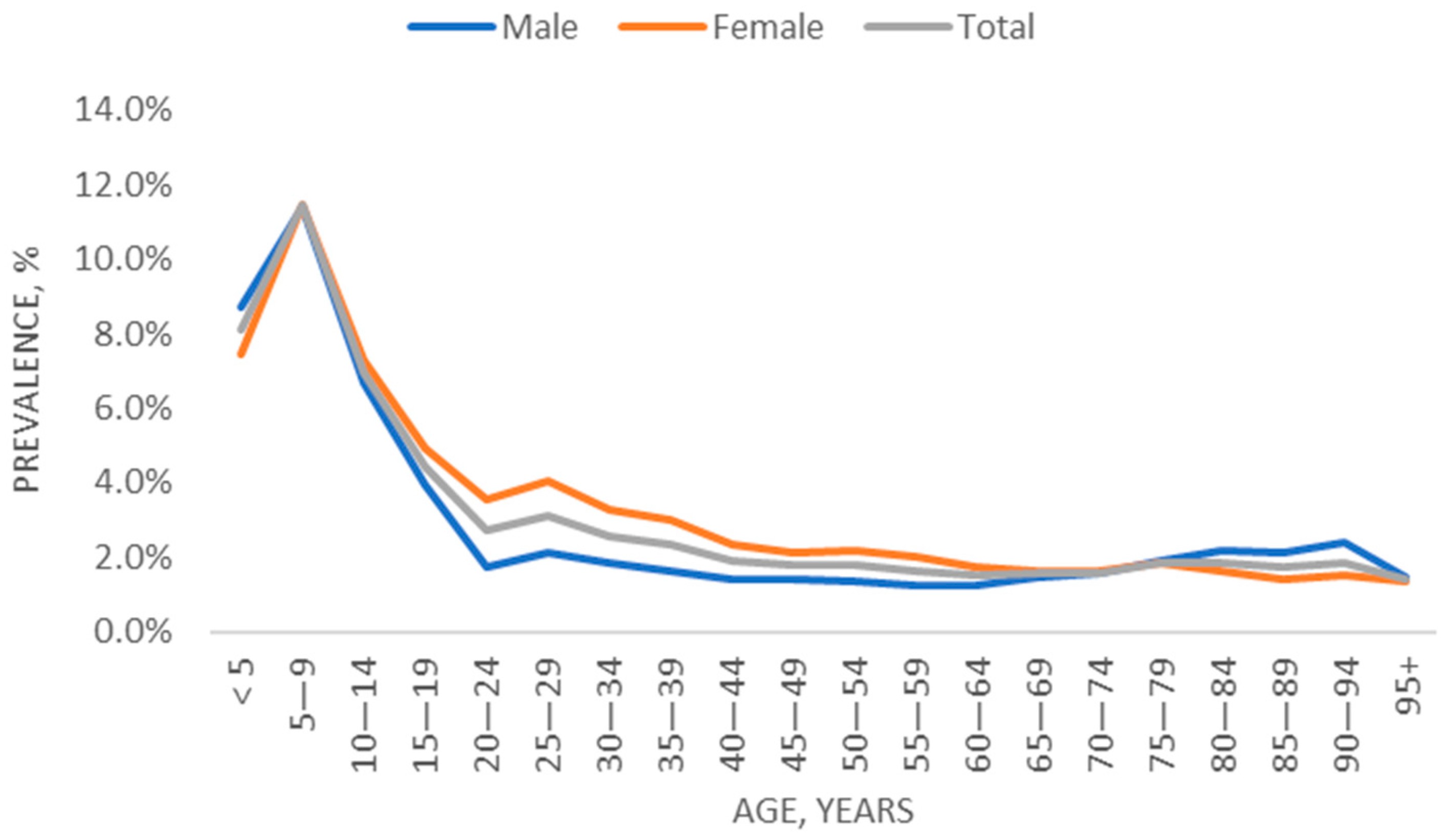
3.1. Trends over Time: Prevalence of AD
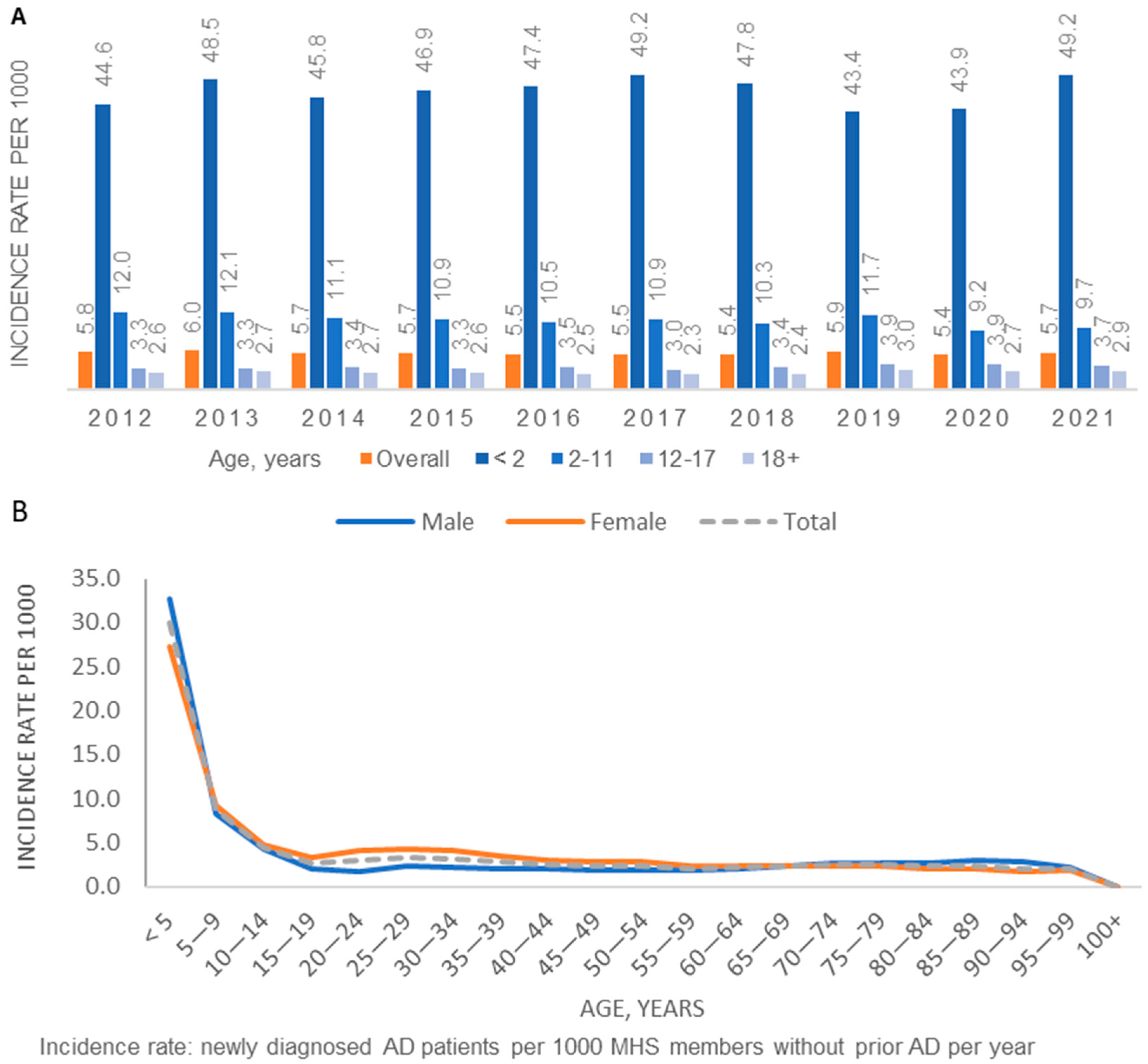
3.2. Trends over Time: Incidence of AD
3.3. Patient Characteristics at AD Diagnosis
3.4. AD Disease Severity and Characteristics of Prevalent Patients (2021)
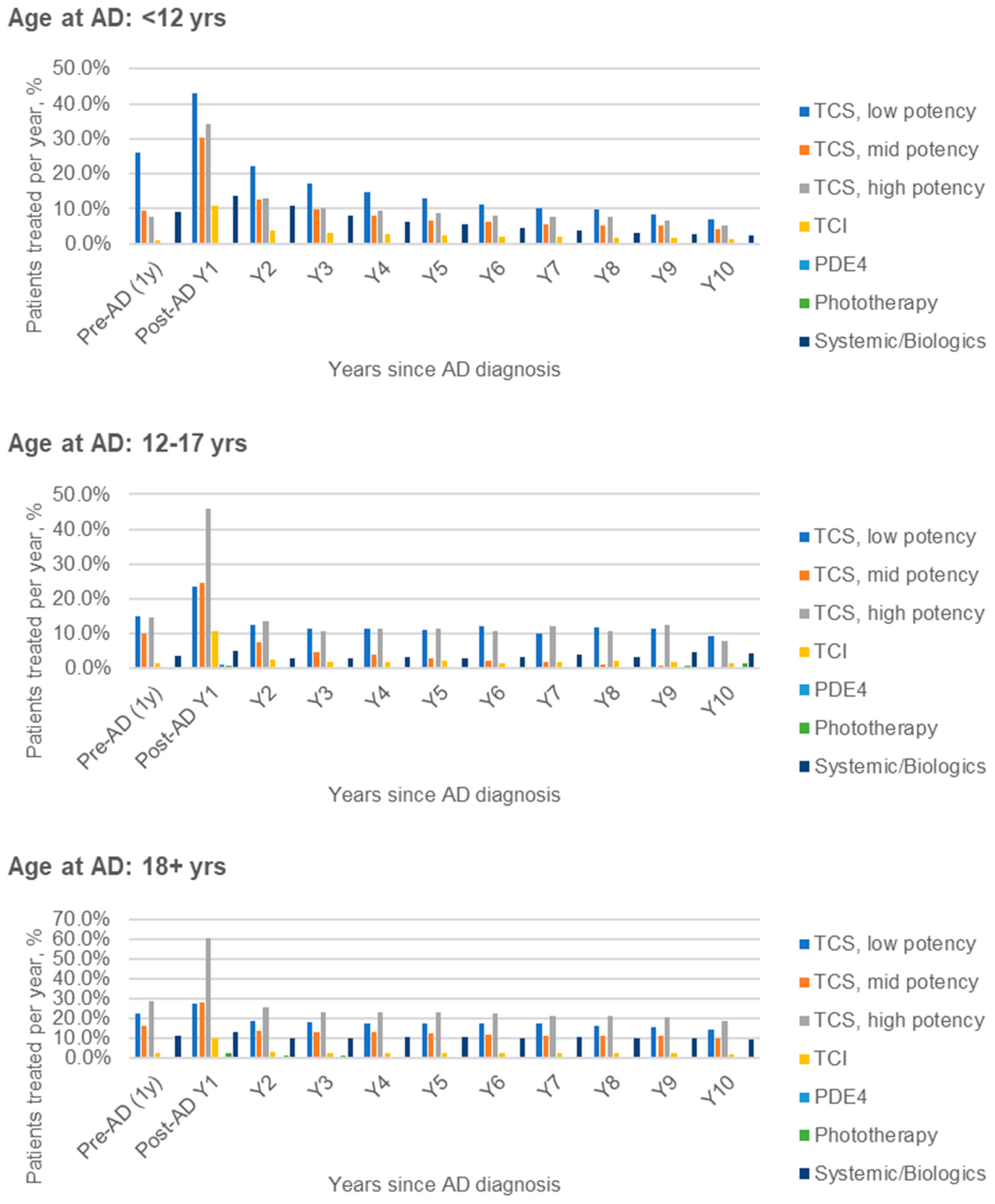
3.5. Longitudinal Treatment Patterns of Incident AD Patients (2012–2021)
3.6. Long-Term Patterns of AD Diagnosis and Treatment after 10 Years
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Laughter, M.; Maymone, M.B.; Mashayekhi, S.; Arents, B.W.; Karimkhani, C.; Langan, S.; Dellavalle, R.; Flohr, C. The global burden of atopic dermatitis: Lessons from the Global Burden of Disease Study 1990–2017. Br. J. Dermatol. 2021, 184, 304–309. [Google Scholar] [CrossRef] [PubMed]
- Israel Central Bureau of Statistics. Characterization and Classification of Geographic Units by the Socio-Economic Level of the Population 2015. Publication No. 1765. Available online: https://www.cbs.gov.il/he/publications/DocLib/2019/1765_socio_economic_2015/e_print.pdf (accessed on 1 October 2021).
- Rossman, H.; Shilo, S.; Meir, T.; Gorfine, M.; Shalit, U.; Segal, E. COVID-19 dynamics after a national immunization program in Israel. Nat. Med. 2021, 27, 1055–1061. [Google Scholar] [CrossRef] [PubMed]
- Chodick, G.; Heymann, A.D.; Shalev, V.; Kookia, E. The epidemiology of diabetes in a large Israeli HMO. Eur. J. Epidemiol. 2003, 18, 1143–1146. [Google Scholar] [CrossRef]
- Shalev, V.; Chodick, G.; Goren, I.; Silber, H.; Kokia, E.; Heymann, A.D. The use of an automated patient registry to manage and monitor cardiovascular conditions and related outcomes in a large health organization. Int. J. Cardiol. 2011, 152, 345–349. [Google Scholar] [CrossRef] [PubMed]
- Coresh, J.; Turin, T.C.; Matsushita, K.; Sang, Y.; Ballew, S.H.; Appel, L.J.; Arima, H.; Chadban, S.J.; Cirillo, M.; Djurdjev, O. Decline in estimated glomerular filtration rate and subsequent risk of end-stage renal disease and mortality. JAMA 2014, 311, 2518–2531. [Google Scholar] [CrossRef] [PubMed]
- Weitzman, D.; Chodick, G.; Shalev, V.; Grossman, C.; Grossman, E. Prevalence and factors associated with resistant hypertension in a large health maintenance organization in Israel. Hypertension 2014, 64, 501–507. [Google Scholar] [CrossRef] [PubMed]
- Weil, C.; Sugerman, P.B.; Chodick, G.; Liang, H.; Wang, H.; Calimlim, B.M.; Dorfman, A.; Shalev, V.; Ben Amitai, D.; Leshem, Y.A. Epidemiology and Economic Burden of Atopic Dermatitis: Real-World Retrospective Data from a Large Nationwide Israeli Healthcare Provider Database. Adv. Ther. 2022, 39, 2502–2514. [Google Scholar] [CrossRef]
- Shalom, G.; Babaev, M.; Kridin, K.; Schonmann, Y.; Horev, A.; Dreiher, J.; Shani, M.; Tiosano, S.; Fisher, S.; Comaneshter, D. Healthcare service utilization by 116,816 patients with atopic dermatitis in Israel. Acta Derm.-Venereol. 2019, 99, 370–374. [Google Scholar] [CrossRef]
- Dizon, M.; Yu, A.; Singh, R.; Wan, J.; Chren, M.M.; Flohr, C.; Silverberg, J.; Margolis, D.; Langan, S.; Abuabara, K. Systematic review of atopic dermatitis disease definition in studies using routinely collected health data. Br. J. Dermatol. 2018, 178, 1280–1287. [Google Scholar] [CrossRef] [PubMed]
- Henriksen, L.; Simonsen, J.; Haerskjold, A.; Linder, M.; Kieler, H.; Thomsen, S.F.; Stensballe, L.G. Incidence rates of atopic dermatitis, asthma, and allergic rhinoconjunctivitis in Danish and Swedish children. J. Allergy Clin. Immunol. 2015, 136, 360–366.e2. [Google Scholar] [CrossRef]
- Mohn, C.H.; Blix, H.S.; Halvorsen, J.A.; Nafstad, P.; Valberg, M.; Lagerløv, P. Incidence Trends of Atopic Dermatitis in Infancy and Early Childhood in a Nationwide Prescription Registry Study in Norway. JAMA Netw. Open 2018, 1, e184145. [Google Scholar] [CrossRef] [PubMed]
- Tian, J.; Zhang, D.; Yang, Y.; Huang, Y.; Wang, L.; Yao, X.; Lu, Q. Global epidemiology of atopic dermatitis: A comprehensive systematic analysis and modelling study. Br. J. Dermatol. 2023, 190, 55–61. [Google Scholar] [CrossRef] [PubMed]
- Hill, D.A.; Grundmeier, R.W.; Ram, G.; Spergel, J.M. The epidemiologic characteristics of healthcare provider-diagnosed eczema, asthma, allergic rhinitis, and food allergy in children: A retrospective cohort study. BMC Pediatr. 2016, 16, 133. [Google Scholar] [CrossRef] [PubMed]
- Liebhart, J.; Dobek, R.; Malolepszy, J.; Wojtyniak, B.; Pisiewicz, K.; Plusa, T.; Gladysz, U. The Prevalence of Allergic Diseases in Poland—The Results of the PMSEAD Study in Relation to Gender Differences. Adv. Clin. Exp. Med. 2014, 23, 757–762. [Google Scholar] [CrossRef] [PubMed]
- de Lusignan, S.; Alexander, H.; Broderick, C.; Dennis, J.; McGovern, A.; Feeney, C.; Flohr, C. The epidemiology of eczema in children and adults in England: A population-based study using primary care data. Clin. Exp. Allergy 2021, 51, 471–482. [Google Scholar] [CrossRef] [PubMed]
- Sandhu, J.K.; Salame, N.; Ehsani-Chimeh, N.; Armstrong, A.W. Economic burden of cutaneous infections in children and adults with atopic dermatitis. Pediatr. Dermatol. 2019, 36, 303–310. [Google Scholar] [CrossRef] [PubMed]
- Sicras-Mainar, A.; Navarro-Artieda, R.; Carrillo, J.C. Economic impact of atopic dermatitis in adults: A population-based study (IDEA study). Actas Dermo-Sifiliogr. Engl. Ed. 2018, 109, 35–46. [Google Scholar] [CrossRef]
- Shrestha, S.; Miao, R.; Wang, L.; Chao, J.; Yuce, H.; Wei, W. Burden of atopic dermatitis in the United States: Analysis of healthcare claims data in the commercial, Medicare, and Medi-Cal databases. Adv. Ther. 2017, 34, 1989–2006. [Google Scholar] [CrossRef]
- Chung, J.; Simpson, E.L. The socioeconomics of atopic dermatitis. Ann. Allergy Asthma Immunol. 2019, 122, 360–366. [Google Scholar] [CrossRef]
- Hill, D.A.; Spergel, J.M. The atopic march: Critical evidence and clinical relevance. Ann. Allergy Asthma Immunol. 2018, 120, 131–137. [Google Scholar] [CrossRef]
- Drucker, A.M.; Eyerich, K.; de Bruin-Weller, M.S.; Thyssen, J.P.; Spuls, P.I.; Irvine, A.D.; Girolomoni, G.; Dhar, S.; Flohr, C.; Murrell, D.F.; et al. Use of systemic corticosteroids for atopic dermatitis: International Eczema Council consensus statement. Br. J. Dermatol. 2018, 178, 768–775. [Google Scholar] [CrossRef] [PubMed]
- Stensballe, L.G.; Klansø, L.; Jensen, A.; Hærskjold, A.; Thomsen, S.F.; Simonsen, J. The validity of register data to identify children with atopic dermatitis, asthma or allergic rhinoconjunctivitis. Pediatr. Allergy Immunol. 2017, 28, 535–542. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Characteristics at AD Diagnosis | Age at AD Diagnosis, Years | ||||
|---|---|---|---|---|---|
| <12 | 12–17 | 18+ | Total | ||
| Total | 82,013 (100.0) | 5672 (100.0) | 36,865 (100.0) | 124,550 (100.0) | |
| Age, years | Median (IQR) | 1.7 (0.6–4.2) | 14.5 (13.2–16.2) | 41.7 (30.0–55.6) | 4.4 (1.1–26.0) |
| Sex | Male | 43,663 (53.2) | 2433 (42.9) | 14,327 (38.9) | 60,423 (48.5) |
| Female | 38,350 (46.8) | 3239 (57.1) | 22,538 (61.1) | 64,127 (51.5) | |
| Residence area | North | 11,610 (14.2) | 960 (16.9) | 7402 (20.1) | 19,972 (16.0) |
| Sharon | 18,838 (23.0) | 1293 (22.8) | 7213 (19.6) | 27,344 (22.0) | |
| South | 13,956 (17.0) | 861 (15.2) | 5279 (14.3) | 20,096 (16.1) | |
| Center | 18,376 (22.4) | 1119 (19.7) | 8347 (22.6) | 27,842 (22.4) | |
| J-lem and Shfela | 19,233 (23.5) | 1439 (25.4) | 8624 (23.4) | 29,296 (23.5) | |
| SES | Low | 15,912 (19.4) | 1019 (18.0) | 5746 (15.6) | 22,677 (18.2) |
| Medium | 22,470 (27.4) | 1562 (27.5) | 11,200 (30.4) | 35,232 (28.3) | |
| High | 43,557 (53.1) | 3088 (54.4) | 19,879 (53.9) | 66,524 (53.4) | |
| Missing | 73 (0.1) | 3 (0.1) | 40 (0.1) | 116 (0.1) | |
| BMI, kg/m2 a | <18.5 | 37,863 (46.2) | 1824 (32.2) | 1154 (3.1) | 40,841 (32.8) |
| 18.5–24.9 | 4799 (5.9) | 2386 (42.1) | 14,384 (39.0) | 21,569 (17.3) | |
| 25.0–29.9 | 190 (0.2) | 486 (8.6) | 10,146 (27.5) | 10,822 (8.7) | |
| ≥30 | 85 (0.1) | 172 (3.0) | 6329 (17.2) | 6586 (5.3) | |
| Missing | 39,076 (47.6) | 804 (14.2) | 4852 (13.2) | 44,732 (35.9) | |
| Asthma | Ever | 9540 (11.6) | 1614 (28.5) | 6909 (18.7) | 18,063 (14.5) |
| Prior 5 years | 8162 (10.0) | 508 (9.0) | 3329 (9.0) | 11,999 (9.6) | |
| Allergic rhinitis | Ever | 3235 (3.9) | 1319 (23.3) | 12,385 (33.6) | 16,939 (13.6) |
| Prior 5 years | 3087 (3.8) | 927 (16.3) | 6536 (17.7) | 10,550 (8.5) | |
| Nasal polyposis | Ever | 79 (0.1) | 26 (0.5) | 667 (1.8) | 772 (0.6) |
| Ophthalmic conditions | Ever | 11 (0.0) | 9 (0.2) | 8 (0.0) | 28 (0.0) |
| Anemia—iron deficiency b | Fe, tested | 2763 | 828 | 10,506 | 14,097 |
| Low Fe (% in tested) | 457 (16.5) | 78 (9.4) | 2602 (24.8) | 3137 (22.3) | |
| Low Fe (% in total) | 457 (0.6) | 78 (1.4) | 2602 (7.1) | 3137 (2.5) | |
| Anemia—low Hb b | Hb, tested | 33,209 | 2187 | 25,497 | 60,893 |
| Low Hb (% in tested) | 4491 (13.5) | 263 (12.0) | 5607 (22.0) | 10,361 (17.0) | |
| Low Hb (% in total) | 4491 (5.5) | 263 (4.6) | 5607 (15.2) | 10,361 (8.3) | |
| Anemia b | Low Hb/Fe (% in total) | 4851 (5.9) | 317 (5.6) | 6957 (18.9) | 12,125 (9.7) |
| Other comorbidities (ever) | Diabetes | 15 (0.0) | 15 (0.3) | 2805 (7.6) | 2835 (2.3) |
| Hypertension | 8 (0.0) | 9 (0.2) | 6665 (18.1) | 6682 (5.4) | |
| CVD | 881 (1.1) | 63 (1.1) | 2791 (7.6) | 3735 (3.0) | |
| ADHD c | 956 (1.2) | 1061 (18.7) | 2467 (6.7) | 4484 (3.6) | |
| Depression d | 38 (0.0) | 148 (2.6) | 7156 (19.4) | 7342 (5.9) | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Weil, C.; Adiri, R.; Chodick, G.; Gersten, M.; Cohen Barak, E. Trends of Diagnosis, Disease Course, and Treatment of Atopic Dermatitis 2012–2021: Real-World Data from a Large Healthcare Provider. J. Clin. Med. 2024, 13, 281. https://doi.org/10.3390/jcm13010281
Weil C, Adiri R, Chodick G, Gersten M, Cohen Barak E. Trends of Diagnosis, Disease Course, and Treatment of Atopic Dermatitis 2012–2021: Real-World Data from a Large Healthcare Provider. Journal of Clinical Medicine. 2024; 13(1):281. https://doi.org/10.3390/jcm13010281
Chicago/Turabian StyleWeil, Clara, Roni Adiri, Gabriel Chodick, Merril Gersten, and Eran Cohen Barak. 2024. "Trends of Diagnosis, Disease Course, and Treatment of Atopic Dermatitis 2012–2021: Real-World Data from a Large Healthcare Provider" Journal of Clinical Medicine 13, no. 1: 281. https://doi.org/10.3390/jcm13010281
APA StyleWeil, C., Adiri, R., Chodick, G., Gersten, M., & Cohen Barak, E. (2024). Trends of Diagnosis, Disease Course, and Treatment of Atopic Dermatitis 2012–2021: Real-World Data from a Large Healthcare Provider. Journal of Clinical Medicine, 13(1), 281. https://doi.org/10.3390/jcm13010281