
Correlations between Resting Electrocardiogram Findings and Disease Profiles: Insights from the Qatar Biobank Cohort

 , , ,
, , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Cohort
2.2. Phenotypic Data: Serum Electrolytes, Sugars/Lipids, Blood and Inflammatory, and Clinical/Disease Traits
2.3. ECG Data
2.4. Statistical Analysis
3. Results
3.1. Association Analysis
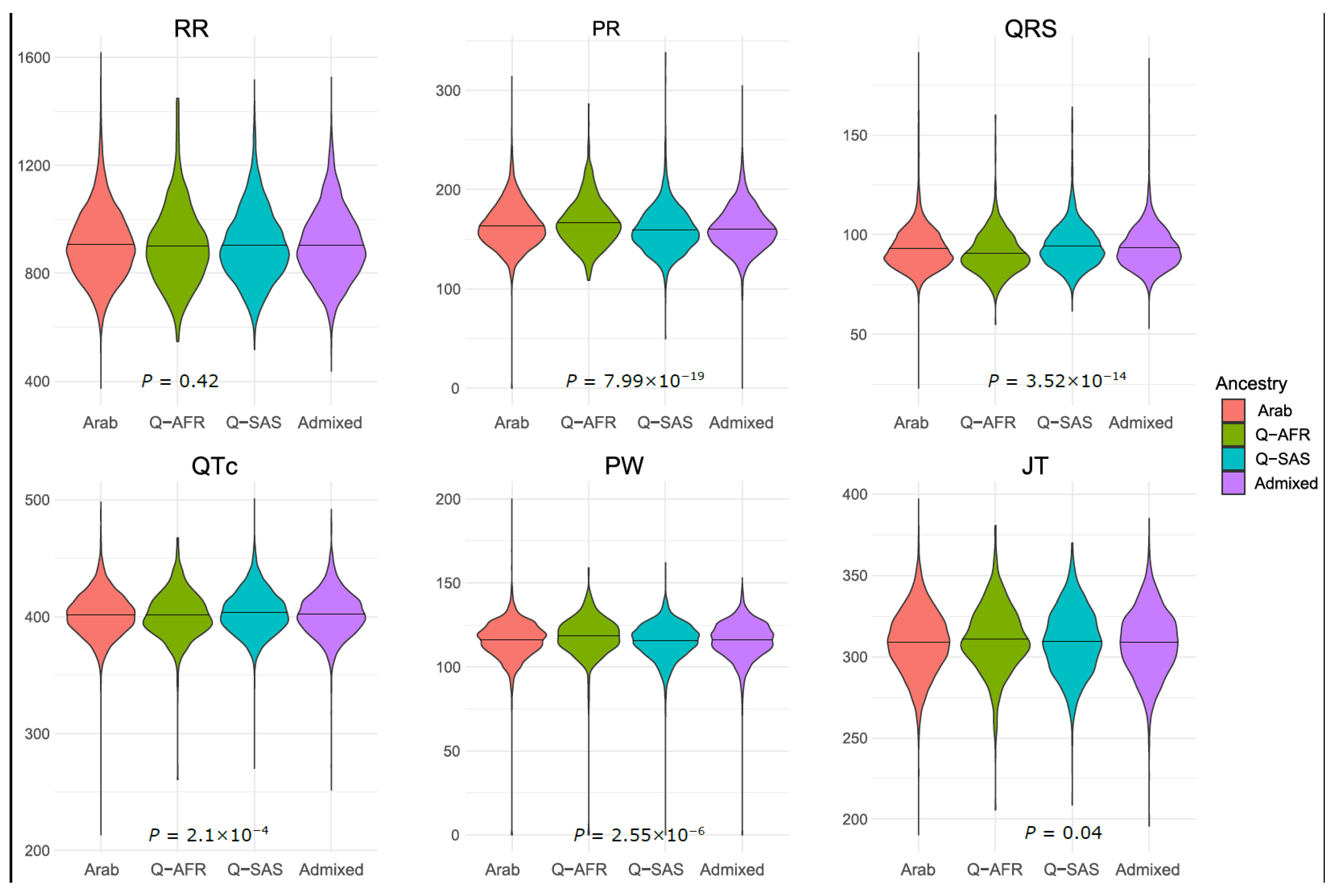
3.1.1. Demographics
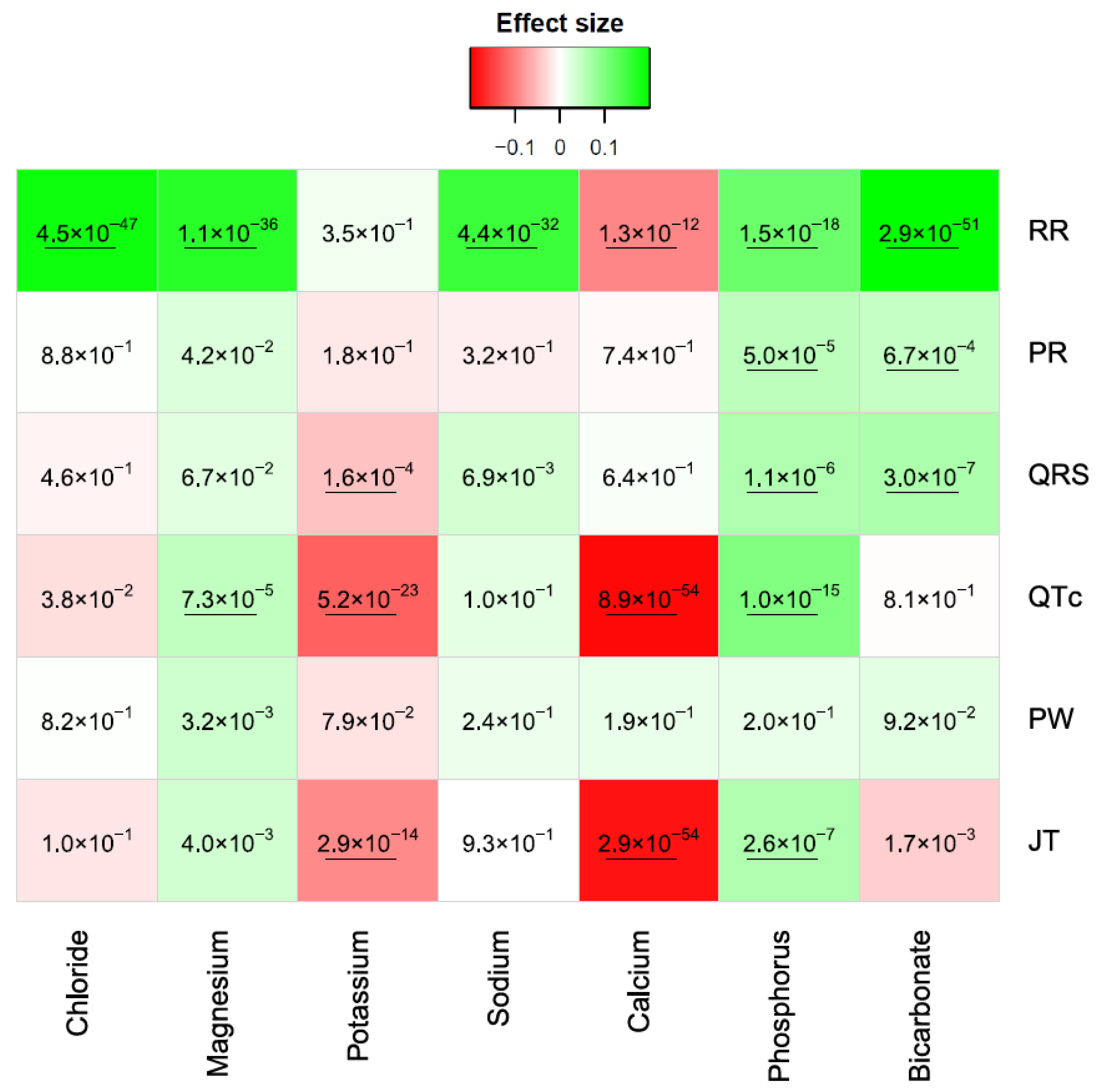
3.1.2. Serum Electrolytes
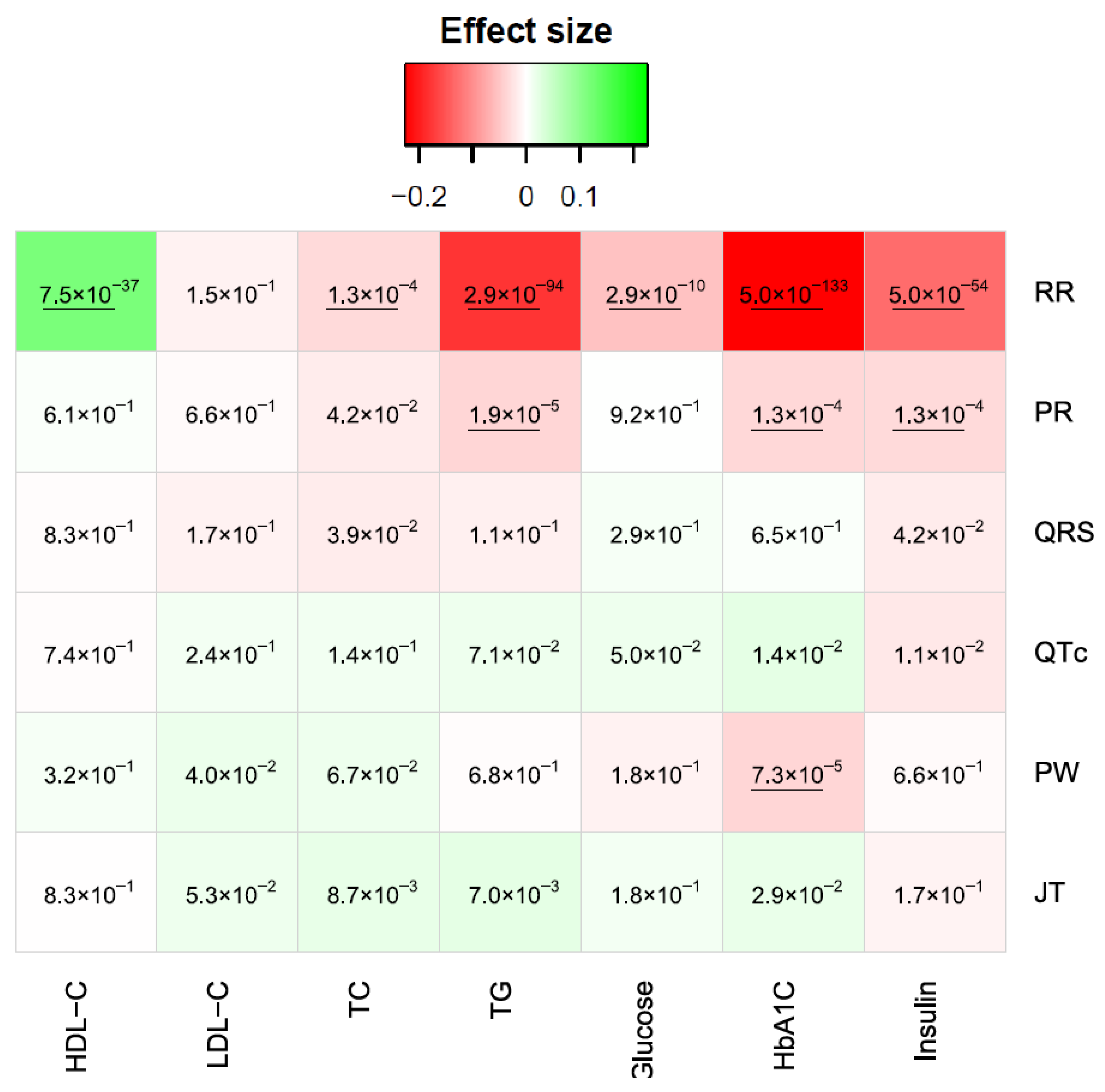
3.1.3. Sugars/Lipids
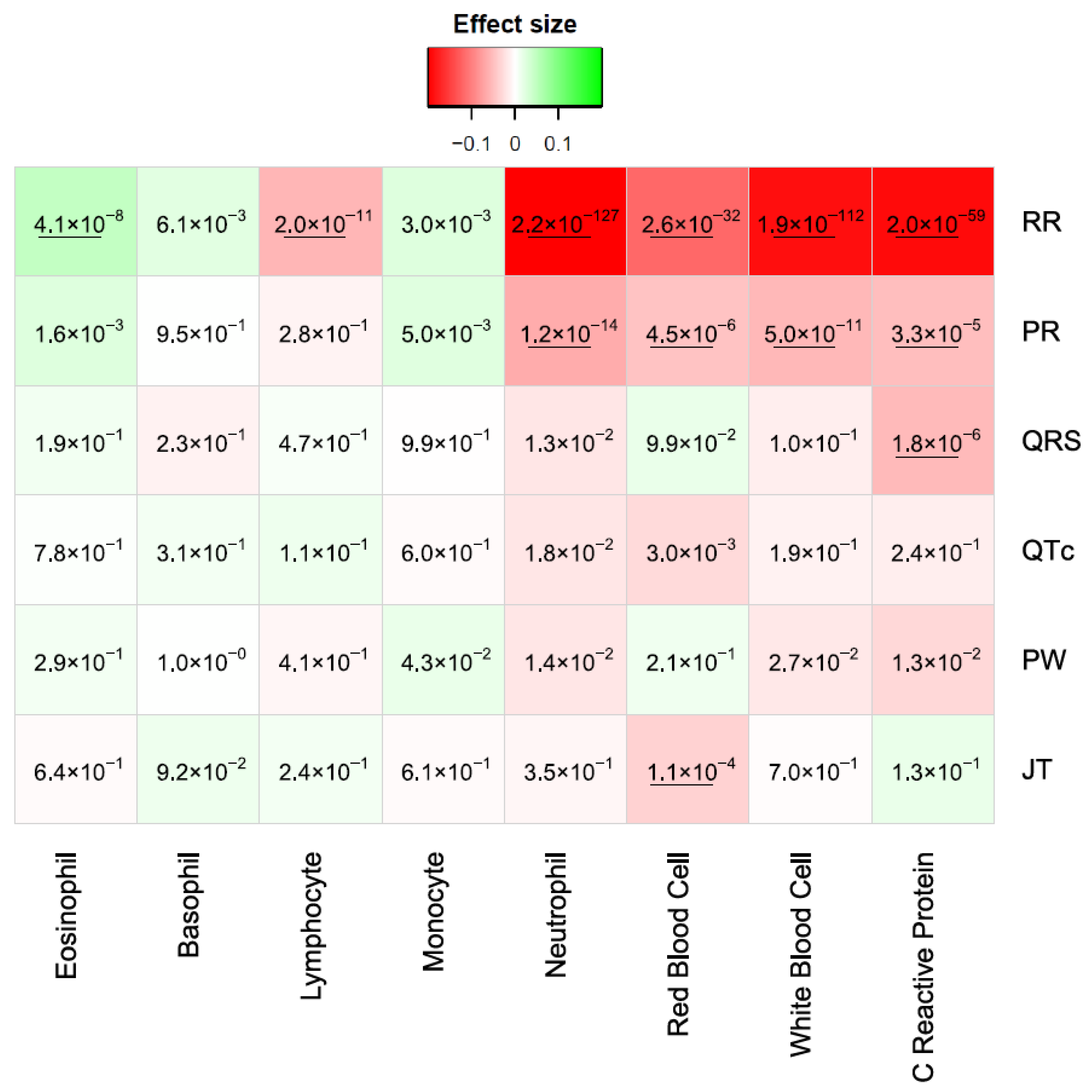
3.1.4. Blood and Inflammatory
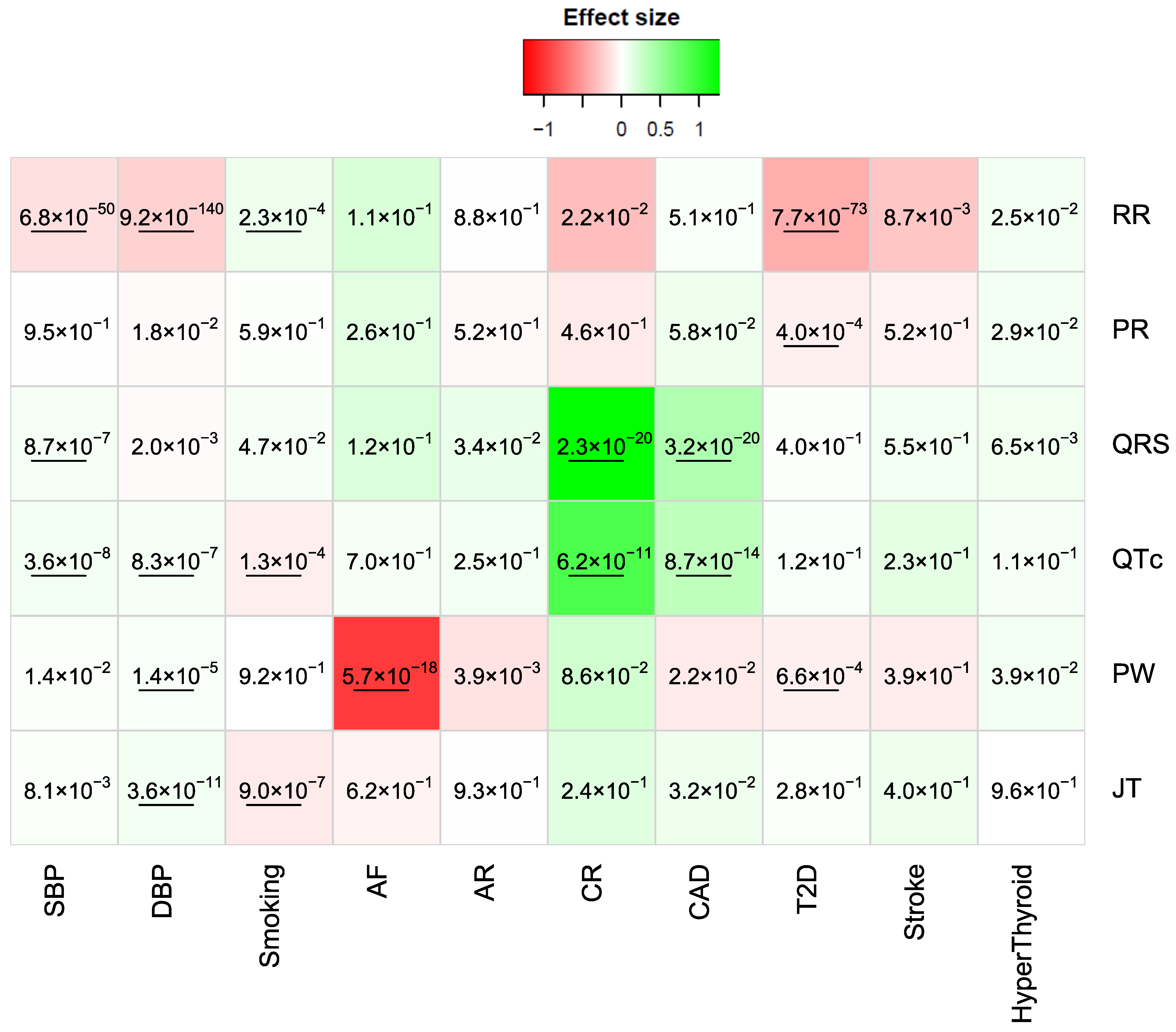
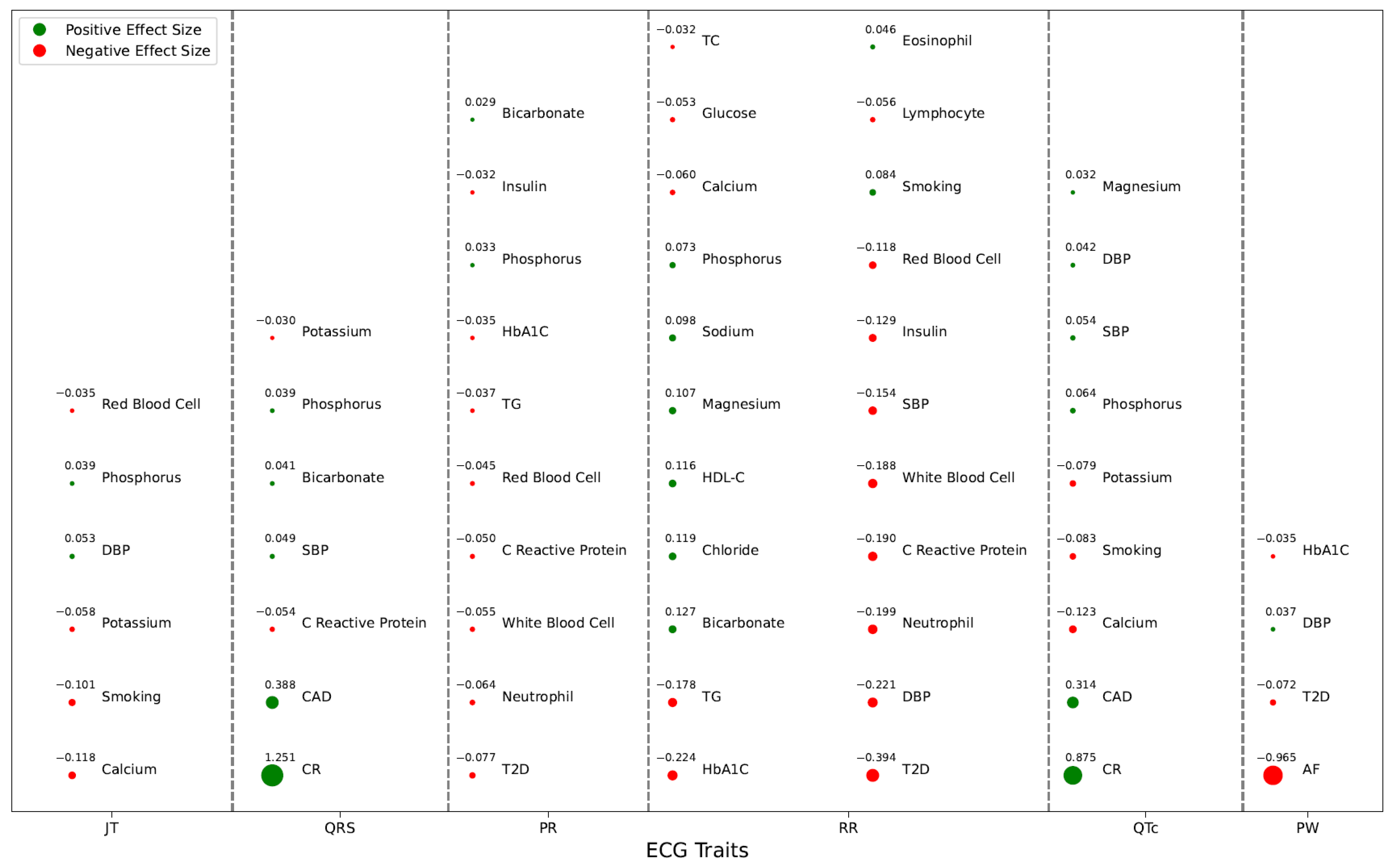
3.1.5. Clinical/Disease Traits
3.2. Risk Score Performance to Predict CAD
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hampton, J.R. The importance of minor abnormalities in the resting electrocardiogram. Eur. Heart J. 1984, 5 (Suppl. SA), 61–63. [Google Scholar] [CrossRef] [PubMed]
- Surber, R.; Schwarz, G.; Figulla, H.R.; Werner, G.S. Resting 12-lead electrocardiogram as a reliable predictor of functional recovery after recanalization of chronic total coronary occlusions. Clin. Cardiol. 2005, 28, 293–297. [Google Scholar] [CrossRef] [PubMed]
- Yue, W.; Wang, G.; Zhang, X.; Chen, B.; Wang, X.; Huangfu, F.; Jia, R. Electrocardiogram for predicting cardiac functional recovery. Cell Biochem. Biophys. 2014, 70, 87–91. [Google Scholar] [CrossRef] [PubMed]
- Perez, M.V.; Dewey, F.E.; Marcus, R.; Ashley, E.A.; Al-Ahmad, A.A.; Wang, P.J.; Froelicher, V.F. Electrocardiographic predictors of atrial fibrillation. Am. Heart J. 2009, 158, 622–628. [Google Scholar] [CrossRef] [PubMed]
- Shah, A.M.; Jefferies, J.L.; Rossano, J.W.; Decker, J.A.; Cannon, B.C.; Kim, J.J. Electrocardiographic abnormalities and arrhythmias are strongly associated with the development of cardiomyopathy in muscular dystrophy. Heart Rhythm. 2010, 7, 1484–1488. [Google Scholar] [CrossRef] [PubMed]
- Harms, P.P.; van der Heijden, A.A.; Rutters, F.; Tan, H.L.; Beulens, J.W.J.; Nijpels, G.; Elders, P.; Escape NET. Prevalence of ECG abnormalities in people with type 2 diabetes: The Hoorn Diabetes Care System cohort. J. Diabetes Complicat. 2021, 35, 107810. [Google Scholar] [CrossRef]
- Soliman, E.Z.; Backlund, J.C.; Bebu, I.; Orchard, T.J.; Zinman, B.; Lachin, J.M.; Group DER. Electrocardiographic Abnormalities and Cardiovascular Disease Risk in Type 1 Diabetes: The Epidemiology of Diabetes Interventions and Complications (EDIC) Study. Diabetes Care 2017, 40, 793–799. [Google Scholar] [CrossRef]
- Kaolawanich, Y.; Thongsongsang, R.; Songsangjinda, T.; Boonyasirinant, T. Clinical values of resting electrocardiography in patients with known or suspected chronic coronary artery disease: A stress perfusion cardiac MRI study. BMC Cardiovasc. Disord. 2021, 21, 621. [Google Scholar] [CrossRef]
- Lehtonen, A.O.; Puukka, P.; Varis, J.; Porthan, K.; Tikkanen, J.T.; Nieminen, M.S.; Huikuri, H.V.; Anttila, I.; Nikus, K.; Kahonen, M.; et al. Prevalence and prognosis of ECG abnormalities in normotensive and hypertensive individuals. J. Hypertens. 2016, 34, 959–966. [Google Scholar] [CrossRef]
- Ebong, I.A.; Bertoni, A.G.; Soliman, E.Z.; Guo, M.; Sibley, C.T.; Chen, Y.D.; Rotter, J.I.; Chen, Y.C.; Goff, D.C., Jr. Electrocardiographic abnormalities associated with the metabolic syndrome and its components: The multi-ethnic study of atherosclerosis. Metab. Syndr. Relat. Disord. 2012, 10, 92–97. [Google Scholar] [CrossRef]
- Judson, W.E.; Hollander, W. The effects of insulin-induced hypoglycemia in patients with angina pectoris; before and after intravenous hexamethonium. Am. Heart J. 1956, 52, 198–209. [Google Scholar] [CrossRef]
- Frier, B.M.; Schernthaner, G.; Heller, S.R. Hypoglycemia and cardiovascular risks. Diabetes Care 2011, 34 (Suppl. S2), S132–S137. [Google Scholar] [CrossRef] [PubMed]
- Diercks, D.B.; Shumaik, G.M.; Harrigan, R.A.; Brady, W.J.; Chan, T.C. Electrocardiographic manifestations: Electrolyte abnormalities. J. Emerg. Med. 2004, 27, 153–160. [Google Scholar] [CrossRef] [PubMed]
- Lu, T.P.; Chattopadhyay, A.; Lu, K.C.; Chuang, J.Y.; Yeh, S.S.; Chang, I.S.; Chen, C.J.; Wu, I.C.; Hsu, C.C.; Chen, T.Y.; et al. Develop and Apply Electrocardiography-Based Risk Score to Identify Community-Based Elderly Individuals at High-Risk of Mortality. Front. Cardiovasc. Med. 2021, 8, 738061. [Google Scholar] [CrossRef]
- Holkeri, A.; Eranti, A.; Haukilahti, M.A.E.; Kerola, T.; Kentta, T.V.; Tikkanen, J.T.; Anttonen, O.; Noponen, K.; Seppanen, T.; Rissanen, H.; et al. Predicting sudden cardiac death in a general population using an electrocardiographic risk score. Heart 2020, 106, 427–433. [Google Scholar] [CrossRef] [PubMed]
- Kang, M.; Chang, Y.; Kang, J.; Kim, Y.; Ryu, S. Electrocardiogram Risk Score and Prevalence of Subclinical Atherosclerosis: A Cross-Sectional Study. J. Pers. Med. 2022, 12, 463. [Google Scholar] [CrossRef] [PubMed]
- Macfarlane, P.W.; Norrie, J.; Committee, W.E. The value of the electrocardiogram in risk assessment in primary prevention: Experience from the West of Scotland Coronary Prevention Study. J. Electrocardiol. 2007, 40, 101–109. [Google Scholar] [CrossRef]
- Cedres, B.L.; Liu, K.; Stamler, J.; Dyer, A.R.; Stamler, R.; Berkson, D.M.; Paul, O.; Lepper, M.; Lindberg, H.A.; Marquardt, J.; et al. Independent contribution of electrocardiographic abnormalities to risk of death from coronary heart disease, cardiovascular diseases and all causes. Findings of three Chicago epidemiologic studies. Circulation 1982, 65, 146–153. [Google Scholar] [CrossRef]
- Hippisley-Cox, J.; Coupland, C.; Brindle, P. Development and validation of QRISK3 risk prediction algorithms to estimate future risk of cardiovascular disease: Prospective cohort study. BMJ 2017, 357, j2099. [Google Scholar] [CrossRef]
- Pesaro, A.E.; Bittencourt, M.S.; Franken, M.; Carvalho, J.A.M.; Bernardes, D.; Tuomilehto, J.; Santos, R.D. The Finnish Diabetes Risk Score (FINDRISC), incident diabetes and low-grade inflammation. Diabetes Res. Clin. Pract. 2021, 171, 108558. [Google Scholar] [CrossRef]
- Al Thani, A.; Fthenou, E.; Paparrodopoulos, S.; Al Marri, A.; Shi, Z.; Qafoud, F.; Afifi, N. Qatar Biobank Cohort Study: Study Design and First Results. Am. J. Epidemiol. 2019, 188, 1420–1433. [Google Scholar] [CrossRef] [PubMed]
- Surawicz, B. Role of electrolytes in etiology and management of cardiac arrhythmias. Prog. Cardiovasc. Dis. 1966, 8, 364–386. [Google Scholar] [CrossRef] [PubMed]
- Johri, A.M.; Baranchuk, A.; Simpson, C.S.; Abdollah, H.; Redfearn, D.P. ECG manifestations of multiple electrolyte imbalance: Peaked T wave to P wave (“tee-pee sign”). Ann. Noninvasive. Electrocardiol. 2009, 14, 211–214. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Post, W.S.; Dalal, D.; Bansal, S.; Blasco-Colmenares, E.; Jan De Beur, S.; Alonso, A.; Soliman, E.Z.; Whitsel, E.A.; Brugada, R.; et al. Serum 25-hydroxyvitamin D, calcium, phosphorus, and electrocardiographic QT interval duration: Findings from NHANES III and ARIC. J. Clin. Endocrinol. Metab. 2011, 96, 1873–1882. [Google Scholar] [CrossRef] [PubMed]
- Loewe, A.; Lutz, Y.; Nairn, D.; Fabbri, A.; Nagy, N.; Toth, N.; Ye, X.; Fuertinger, D.H.; Genovesi, S.; Kotanko, P.; et al. Hypocalcemia-Induced Slowing of Human Sinus Node Pacemaking. Biophys. J. 2019, 117, 2244–2254. [Google Scholar] [CrossRef] [PubMed]
- Nie, Y.; Zou, J.; Liang, Y.; Shen, B.; Liu, Z.; Cao, X.; Chen, X.; Ding, X. Electrocardiographic Abnormalities and QTc Interval in Patients Undergoing Hemodialysis. PLoS ONE 2016, 11, e0155445. [Google Scholar] [CrossRef]
- Kendir, C.; van den Akker, M.; Vos, R.; Metsemakers, J. Cardiovascular disease patients have increased risk for comorbidity: A cross-sectional study in the Netherlands. Eur. J. Gen. Pract. 2018, 24, 45–50. [Google Scholar] [CrossRef]
- Odutayo, A.; Wong, C.X.; Hsiao, A.J.; Hopewell, S.; Altman, D.G.; Emdin, C.A. Atrial fibrillation and risks of cardiovascular disease, renal disease, and death: Systematic review and meta-analysis. BMJ 2016, 354, i4482. [Google Scholar] [CrossRef]
- Li, Y.; Tang, C.; Wu, W.; Li, Z.; Li, X.; Huang, W.; Chen, W.; Mai, X.; Li, X.; Xu, C.; et al. Abnormal blood lipid and electrocardiogram characteristics in common mental disorders. BMC Psychiatry 2023, 23, 465. [Google Scholar] [CrossRef]
- Jayanthi, R.; Girijasivam, S.P.; Gaur, A. Association of blood pressure and BMI to corrected QT interval in young adults. Can. J. Physiol. Pharmacol. 2021, 99, 894–899. [Google Scholar] [CrossRef]
- Ng, K.W.; Allen, M.L.; Desai, A.; Macrae, D.; Pathan, N. Cardioprotective effects of insulin: How intensive insulin therapy may benefit cardiac surgery patients. Circulation 2012, 125, 721–728. [Google Scholar] [CrossRef] [PubMed]
- Cheng, S.; Keyes, M.J.; Larson, M.G.; McCabe, E.L.; Newton-Cheh, C.; Levy, D.; Benjamin, E.J.; Vasan, R.S.; Wang, T.J. Long-term outcomes in individuals with prolonged PR interval or first-degree atrioventricular block. JAMA 2009, 301, 2571–2577. [Google Scholar] [CrossRef] [PubMed]
- Pretorius, L.; Du, X.J.; Woodcock, E.A.; Kiriazis, H.; Lin, R.C.; Marasco, S.; Medcalf, R.L.; Ming, Z.; Head, G.A.; Tan, J.W.; et al. Reduced phosphoinositide 3-kinase (p110alpha) activation increases the susceptibility to atrial fibrillation. Am. J. Pathol. 2009, 175, 998–1009. [Google Scholar] [CrossRef] [PubMed]
- De Bacquer, D.; De Backer, G.; Kornitzer, M. Prevalences of ECG findings in large population based samples of men and women. Heart 2000, 84, 625–633. [Google Scholar] [CrossRef] [PubMed]
- Stern, S.; Sclarowsky, S. The ECG in diabetes mellitus. Circulation 2009, 120, 1633–1636. [Google Scholar] [CrossRef]
- Rautaharju, P.M.; Kooperberg, C.; Larson, J.C.; LaCroix, A. Electrocardiographic abnormalities that predict coronary heart disease events and mortality in postmenopausal women: The Women’s Health Initiative. Circulation 2006, 113, 473–480. [Google Scholar] [CrossRef]
- Ramirez, J.; van Duijvenboden, S.; Young, W.J.; Orini, M.; Jones, A.R.; Lambiase, P.D.; Munroe, P.B.; Tinker, A. Analysing electrocardiographic traits and predicting cardiac risk in UK biobank. JRSM Cardiovasc. Dis. 2021, 10, 20480040211023664. [Google Scholar] [CrossRef]
- Hughes, J.W.; Tooley, J.; Torres Soto, J.; Ostropolets, A.; Poterucha, T.; Christensen, M.K.; Yuan, N.; Ehlert, B.; Kaur, D.; Kang, G.; et al. A deep learning-based electrocardiogram risk score for long term cardiovascular death and disease. NPJ Digit. Med. 2023, 6, 169. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Mean ± SD/N (%) | |
|---|---|
| Sex (male) | 6340 (44.46) |
| Age | 40.12 ± 13.11 |
| BMI | 29.6 ± 6.16 |
| AF | 67 (0.005) |
| AR | 156 (0.011) |
| CR | 48 (0.003) |
| CAD | 527 (0.038) |
| T2D | 3308 (0.236) |
| Hyperthyroidism | 1369 (0.098) |
| Smoking | 3615 (0.258) |
| Stroke | 92 (0.007) |
| RR | 905.29 ± 131.23 |
| PR | 162 ± 22.55 |
| QRS | 93.28 ± 10.63 |
| QTc | 402.29 ± 18.56 |
| PW | 116.15 ± 11.13 |
| JT | 309.01 ± 19.78 |
| Sex | Age | BMI | Ancestry | ||||
|---|---|---|---|---|---|---|---|
| b | p | b | p | b | p | p | |
| RR | −0.44 | 6.04 × 10−150 | −0.06 | 3.81 × 10−13 | −0.15 | 6.27 × 10−66 | 0.42 |
| PR | −0.24 | 3.12 × 10−43 | 0.23 | 8.67 × 10−163 | 0.18 | 1.86 × 10−96 | 7.99 × 10−19 |
| QRS | −0.71 | 0 | 0.12 | 1.20 × 10−42 | 0.10 | 1.07 × 10−31 | 3.52 × 10−14 |
| QTc | 0.56 | 1.29 × 10−247 | 0.26 | 3.43 × 10−218 | 0.20 | 7.58 × 10−122 | 2.12 × 10−4 |
| PW | −0.29 | 2.05 × 10−66 | 0.23 | 2.01 × 10−168 | 0.27 | 9.14 × 10−222 | 2.55 × 10−6 |
| JT | 0.91 | 0 | 0.18 | 1.84 × 10−106 | 0.13 | 8.13 × 10−55 | 0.04 |
| Risk Score | ||||||
|---|---|---|---|---|---|---|
| OR | OR 95% CI | p | OR Decile | AUC | AUC 95% CI | |
| Multivariate regression | ||||||
| BMI + Ancestry | 1.24 | [1.06, 1.46] | 6.34 × 10−3 | 1.36 | 0.56 | [0.52, 0.61] |
| Sex + Age | 3.84 | [3.21, 4.59] | 3.55 × 10−49 | 11.73 | 0.84 | [0.81, 0.87] |
| PR + QRS + QTc | 1.65 | [1.45, 1.88] | 4.00 × 10−14 | 3.76 | 0.66 | [0.61, 0.7] |
| HDL + HbA1C | 2.04 | [1.8, 2.32] | 9.88 × 10−29 | 7.57 | 0.75 | [0.7, 0.79] |
| Chloride + Magnesium + Potassium + Calcium | 1.76 | [1.52, 2.04] | 1.94 × 10−14 | 4.32 | 0.64 | [0.59, 0.69] |
| SBP + DBP + Smoking + T2D + Stroke | 2.85 | [2.46, 3.31] | 8.76 × 10−44 | 9.29 | 0.8 | [0.77, 0.84] |
| SBP + DBP + Smoking + T2D + Stroke + RR + PR + QRS + QTc + HbA1C + Magnesium + Potassium + Ancestry | 2.85 | [2.46, 3.3] | 2.20 × 10−44 | 9.57 | 0.81 | [0.77, 0.85] |
| xgboost | ||||||
| T2D + HbA1C + TC + QRS + SBP + QTc + Smoking + Glucose + RR + Potassium + LDL-C + PW + TG + BMI + DBP + Insulin + Stroke + HDL-C + PR | 2.06 | [1.87, 2.28] | 2.10 × 10−46 | 13.99 | 0.84 | [0.81, 0.88] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Qafoud, F.; Kunji, K.; Elshrif, M.; Althani, A.; Salam, A.; Al Suwaidi, J.; Darbar, D.; Asaad, N.; Saad, M. Correlations between Resting Electrocardiogram Findings and Disease Profiles: Insights from the Qatar Biobank Cohort. J. Clin. Med. 2024, 13, 276. https://doi.org/10.3390/jcm13010276
Qafoud F, Kunji K, Elshrif M, Althani A, Salam A, Al Suwaidi J, Darbar D, Asaad N, Saad M. Correlations between Resting Electrocardiogram Findings and Disease Profiles: Insights from the Qatar Biobank Cohort. Journal of Clinical Medicine. 2024; 13(1):276. https://doi.org/10.3390/jcm13010276
Chicago/Turabian StyleQafoud, Fatima, Khalid Kunji, Mohamed Elshrif, Asma Althani, Amar Salam, Jassim Al Suwaidi, Dawood Darbar, Nidal Asaad, and Mohamad Saad. 2024. "Correlations between Resting Electrocardiogram Findings and Disease Profiles: Insights from the Qatar Biobank Cohort" Journal of Clinical Medicine 13, no. 1: 276. https://doi.org/10.3390/jcm13010276
APA StyleQafoud, F., Kunji, K., Elshrif, M., Althani, A., Salam, A., Al Suwaidi, J., Darbar, D., Asaad, N., & Saad, M. (2024). Correlations between Resting Electrocardiogram Findings and Disease Profiles: Insights from the Qatar Biobank Cohort. Journal of Clinical Medicine, 13(1), 276. https://doi.org/10.3390/jcm13010276