

Can Concurrent Fibrate Use Reduce Cardiovascular Risks among Moderate Chronic Kidney Disease Patients Undergoing Statin Therapy? A Cohort Study
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source
2.2. Patient Selection and Study Design
2.3. Covariates
2.4. Outcomes Definition
2.5. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Five-Year Follow-Up Outcomes
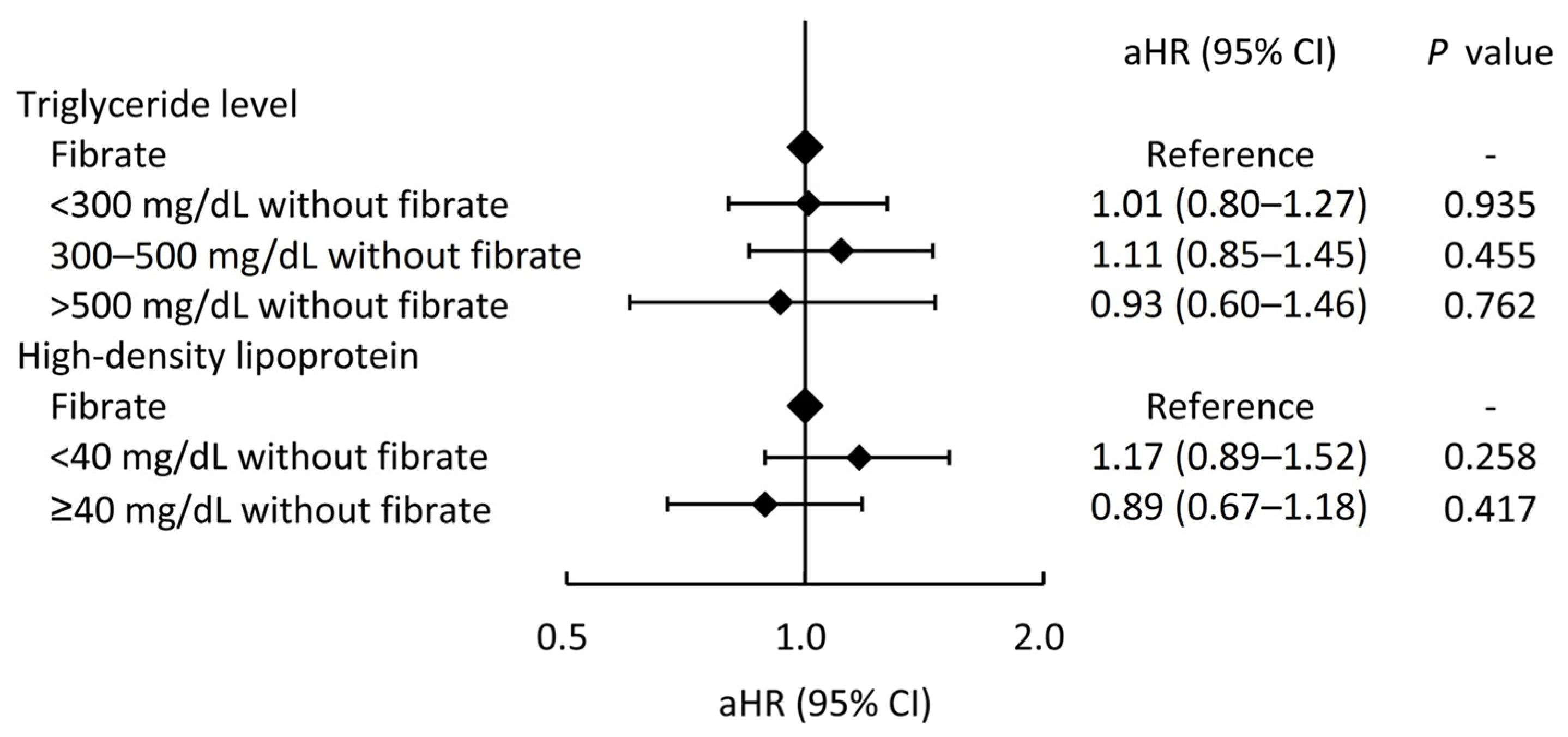
3.3. Subgroup Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Pirillo, A.; Casula, M.; Olmastroni, E.; Norata, G.D.; Catapano, A.L. Global epidemiology of dyslipidaemias. Nat. Rev. Cardiol. 2021, 18, 689–700. [Google Scholar] [CrossRef] [PubMed]
- Tenenbaum, A.; Klempfner, R.; Fisman, E.Z. Hypertriglyceridemia: A too long unfairly neglected major cardiovascular risk factor. Cardiovasc. Diabetol. 2014, 13, 159. [Google Scholar] [CrossRef] [PubMed]
- Kovesdy, C.P. Epidemiology of chronic kidney disease: An update 2022. Kidney Int. Suppl. 2022, 12, 7–11. [Google Scholar] [CrossRef] [PubMed]
- Thobani, A.; Jacobson, T.A. Dyslipidemia in Patients with Kidney Disease. Cardiol. Clin. 2021, 39, 353–363. [Google Scholar] [CrossRef] [PubMed]
- Zoccali, C.; Vanholder, R.; Massy, Z.A.; Ortiz, A.; Sarafidis, P.; Dekker, F.W.; Fliser, D.; Fouque, D.; Heine, G.H.; Jager, K.J.; et al. The systemic nature of CKD. Nat. Rev. Nephrol. 2017, 13, 344–358. [Google Scholar] [CrossRef] [PubMed]
- Jankowski, J.; Floege, J.; Fliser, D.; Bohm, M.; Marx, N. Cardiovascular Disease in Chronic Kidney Disease: Pathophysiological Insights and Therapeutic Options. Circulation 2021, 143, 1157–1172. [Google Scholar] [CrossRef] [PubMed]
- Sarnak, M.J.; Amann, K.; Bangalore, S.; Cavalcante, J.L.; Charytan, D.M.; Craig, J.C.; Gill, J.S.; Hlatky, M.A.; Jardine, A.G.; Landmesser, U.; et al. Chronic Kidney Disease and Coronary Artery Disease: JACC State-of-the-Art Review. J. Am. Coll. Cardiol. 2019, 74, 1823–1838. [Google Scholar] [CrossRef]
- Kaysen, G.A. Lipid and lipoprotein metabolism in chronic kidney disease. J. Ren. Nutr. 2009, 19, 73–77. [Google Scholar] [CrossRef]
- Bulbul, M.C.; Dagel, T.; Afsar, B.; Ulusu, N.N.; Kuwabara, M.; Covic, A.; Kanbay, M. Disorders of Lipid Metabolism in Chronic Kidney Disease. Blood Purif. 2018, 46, 144–152. [Google Scholar] [CrossRef]
- Wanner, C.; Amann, K.; Shoji, T. The heart and vascular system in dialysis. Lancet 2016, 388, 276–284. [Google Scholar] [CrossRef]
- Kshirsagar, A.V.; Bang, H.; Bomback, A.S.; Vupputuri, S.; Shoham, D.A.; Kern, L.M.; Klemmer, P.J.; Mazumdar, M.; August, P.A. A simple algorithm to predict incident kidney disease. Arch. Intern. Med. 2008, 168, 2466–2473. [Google Scholar] [CrossRef] [PubMed]
- Hermida, N.; Balligand, J.L. Low-density lipoprotein-cholesterol-induced endothelial dysfunction and oxidative stress: The role of statins. Antioxid. Redox Signal 2014, 20, 1216–1237. [Google Scholar] [CrossRef]
- Michos, E.D.; McEvoy, J.W.; Blumenthal, R.S. Lipid Management for the Prevention of Atherosclerotic Cardiovascular Disease. N. Engl. J. Med. 2019, 381, 1557–1567. [Google Scholar] [CrossRef]
- Reiner, Z. Hypertriglyceridaemia and risk of coronary artery disease. Nat. Rev. Cardiol. 2017, 14, 401–411. [Google Scholar] [CrossRef] [PubMed]
- Ginsberg, H.N.; Packard, C.J.; Chapman, M.J.; Boren, J.; Aguilar-Salinas, C.A.; Averna, M.; Ference, B.A.; Gaudet, D.; Hegele, R.A.; Kersten, S.; et al. Triglyceride-rich lipoproteins and their remnants: Metabolic insights, role in atherosclerotic cardiovascular disease, and emerging therapeutic strategies-a consensus statement from the European Atherosclerosis Society. Eur. Heart J. 2021, 42, 4791–4806. [Google Scholar] [CrossRef] [PubMed]
- Elam, M.B.; Ginsberg, H.N.; Lovato, L.C.; Corson, M.; Largay, J.; Leiter, L.A.; Lopez, C.; O’Connor, P.J.; Sweeney, M.E.; Weiss, D.; et al. Association of Fenofibrate Therapy With Long-term Cardiovascular Risk in Statin-Treated Patients With Type 2 Diabetes. JAMA Cardiol. 2017, 2, 370–380. [Google Scholar] [CrossRef] [PubMed]
- Keech, A.; Simes, R.J.; Barter, P.; Best, J.; Scott, R.; Taskinen, M.R.; Forder, P.; Pillai, A.; Davis, T.; Glasziou, P.; et al. Effects of long-term fenofibrate therapy on cardiovascular events in 9795 people with type 2 diabetes mellitus (the FIELD study): Randomised controlled trial. Lancet 2005, 366, 1849–1861. [Google Scholar] [CrossRef]
- Das Pradhan, A.; Glynn, R.J.; Fruchart, J.C.; MacFadyen, J.G.; Zaharris, E.S.; Everett, B.M.; Campbell, S.E.; Oshima, R.; Amarenco, P.; Blom, D.J.; et al. Triglyceride Lowering with Pemafibrate to Reduce Cardiovascular Risk. N. Engl. J. Med. 2022, 387, 1923–1934. [Google Scholar] [CrossRef]
- Hager, M.R.; Narla, A.D.; Tannock, L.R. Dyslipidemia in patients with chronic kidney disease. Rev. Endocr. Metab. Disord. 2017, 18, 29–40. [Google Scholar] [CrossRef]
- Ting, R.D.; Keech, A.C.; Drury, P.L.; Donoghoe, M.W.; Hedley, J.; Jenkins, A.J.; Davis, T.M.; Lehto, S.; Celermajer, D.; Simes, R.J.; et al. Benefits and safety of long-term fenofibrate therapy in people with type 2 diabetes and renal impairment: The FIELD Study. Diabetes Care 2012, 35, 218–225. [Google Scholar] [CrossRef]
- Jun, M.; Zhu, B.; Tonelli, M.; Jardine, M.J.; Patel, A.; Neal, B.; Liyanage, T.; Keech, A.; Cass, A.; Perkovic, V. Effects of fibrates in kidney disease: A systematic review and meta-analysis. J. Am. Coll. Cardiol. 2012, 60, 2061–2071. [Google Scholar] [CrossRef] [PubMed]
- Shao, S.C.; Chan, Y.Y.; Kao Yang, Y.H.; Lin, S.J.; Hung, M.J.; Chien, R.N.; Lai, C.C.; Lai, E.C. The Chang Gung Research Database-A multi-institutional electronic medical records database for real-world epidemiological studies in Taiwan. Pharmacoepidemiol. Drug Saf. 2019, 28, 593–600. [Google Scholar] [CrossRef] [PubMed]
- McCaffrey, D.F.; Griffin, B.A.; Almirall, D.; Slaughter, M.E.; Ramchand, R.; Burgette, L.F. A tutorial on propensity score estimation for multiple treatments using generalized boosted models. Stat. Med. 2013, 32, 3388–3414. [Google Scholar] [CrossRef] [PubMed]
- Packard, C.J.; Boren, J.; Taskinen, M.R. Causes and Consequences of Hypertriglyceridemia. Front. Endocrinol. 2020, 11, 252. [Google Scholar] [CrossRef] [PubMed]
- Staels, B.; Dallongeville, J.; Auwerx, J.; Schoonjans, K.; Leitersdorf, E.; Fruchart, J.C. Mechanism of action of fibrates on lipid and lipoprotein metabolism. Circulation 1998, 98, 2088–2093. [Google Scholar] [CrossRef] [PubMed]
- Januszkiewicz, L.; The ACCORD Study Group. Effects of combination lipid therapy in type 2 diabetes mellitus. Kardiol. Pol. 2010, 68, 853–854; discussion 855. [Google Scholar]
- Moisi, M.I.; Bungau, S.G.; Vesa, C.M.; Diaconu, C.C.; Behl, T.; Stoicescu, M.; Toma, M.M.; Bustea, C.; Sava, C.; Popescu, M.I. Framing Cause-Effect Relationship of Acute Coronary Syndrome in Patients with Chronic Kidney Disease. Diagnostics 2021, 11, 1518. [Google Scholar] [CrossRef]
- Makkar, R.; Behl, T.; Kumar, A.; Uddin, M.S.; Bungau, S. Untying the correlation between apolipoproteins and rheumatoid arthritis. Inflamm. Res. 2021, 70, 19–28. [Google Scholar] [CrossRef]
- Filler, G.; Taheri, S.; McIntyre, C.; Smith, C.; Subramanian, L.; Fusch, G.; Fusch, C. Chronic kidney disease stage affects small, dense low-density lipoprotein but not glycated low-density lipoprotein in younger chronic kidney disease patients: A cross-sectional study. Clin. Kidney J. 2018, 11, 383–388. [Google Scholar] [CrossRef]
- Chu, M.; Wang, A.Y.; Chan, I.H.; Chui, S.H.; Lam, C.W. Serum small-dense LDL abnormalities in chronic renal disease patients. Br. J. Biomed. Sci. 2012, 69, 99–102. [Google Scholar] [CrossRef]
- Tokuno, A.; Hirano, T.; Hayashi, T.; Mori, Y.; Yamamoto, T.; Nagashima, M.; Shiraishi, Y.; Ito, Y.; Adachi, M. The effects of statin and fibrate on lowering small dense LDL- cholesterol in hyperlipidemic patients with type 2 diabetes. J. Atheroscler. Thromb. 2007, 14, 128–132. [Google Scholar] [CrossRef]
- Lemieux, I.; Laperriere, L.; Dzavik, V.; Tremblay, G.; Bourgeois, J.; Despres, J.P. A 16-week fenofibrate treatment increases LDL particle size in type IIA dyslipidemic patients. Atherosclerosis 2002, 162, 363–371. [Google Scholar] [CrossRef] [PubMed]
- Boren, J.; Williams, K.J. The central role of arterial retention of cholesterol-rich apolipoprotein-B-containing lipoproteins in the pathogenesis of atherosclerosis: A triumph of simplicity. Curr. Opin. Lipidol. 2016, 27, 473–483. [Google Scholar] [CrossRef] [PubMed]
- Chan, D.T.; Dogra, G.K.; Irish, A.B.; Ooi, E.M.; Barrett, P.H.; Chan, D.C.; Watts, G.F. Chronic kidney disease delays VLDL-apoB-100 particle catabolism: Potential role of apolipoprotein C-III. J. Lipid Res. 2009, 50, 2524–2531. [Google Scholar] [CrossRef] [PubMed]
- Kastarinen, H.; Horkko, S.; Kauma, H.; Karjalainen, A.; Savolainen, M.J.; Kesaniemi, Y.A. Low-density lipoprotein clearance in patients with chronic renal failure. Nephrol. Dial. Transplant. 2009, 24, 2131–2135. [Google Scholar] [CrossRef] [PubMed]
- Hogue, J.C.; Lamarche, B.; Deshaies, Y.; Tremblay, A.J.; Bergeron, J.; Gagne, C.; Couture, P. Differential effect of fenofibrate and atorvastatin on in vivo kinetics of apolipoproteins B-100 and B-48 in subjects with type 2 diabetes mellitus with marked hypertriglyceridemia. Metabolism 2008, 57, 246–254. [Google Scholar] [CrossRef] [PubMed]
- Graham, D.J.; Staffa, J.A.; Shatin, D.; Andrade, S.E.; Schech, S.D.; La Grenade, L.; Gurwitz, J.H.; Chan, K.A.; Goodman, M.J.; Platt, R. Incidence of hospitalized rhabdomyolysis in patients treated with lipid-lowering drugs. JAMA 2004, 292, 2585–2590. [Google Scholar] [CrossRef] [PubMed]
- Jacobson, T.A.; Zimmerman, F.H. Fibrates in combination with statins in the management of dyslipidemia. J. Clin. Hypertens. 2006, 8, 35–41; quiz 42–43. [Google Scholar] [CrossRef]
- Harper, C.R.; Jacobson, T.A. Managing dyslipidemia in chronic kidney disease. J. Am. Coll. Cardiol. 2008, 51, 2375–2384. [Google Scholar] [CrossRef]
- Gheorghe, G.; Toth, P.P.; Bungau, S.; Behl, T.; Ilie, M.; Pantea Stoian, A.; Bratu, O.G.; Bacalbasa, N.; Rus, M.; Diaconu, C.C. Cardiovascular Risk and Statin Therapy Considerations in Women. Diagnostics 2020, 10, 483. [Google Scholar] [CrossRef]
- Vesa, C.M.; Bungau, S.G. Novel Molecules in Diabetes Mellitus, Dyslipidemia and Cardiovascular Disease. Int. J. Mol. Sci. 2023, 24, 4029. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Before GBM IPTW | After GBM IPTW | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Variables | Available Number | Total (n = 3312) | Fibrate (n = 954) | Non-Fibrate (n = 2358) | MASD | Fibrate | Non-Fibrate | MASD | |
| Age, years | 3312 | 61.6 ± 11.9 | 61.4 ± 10.9 | 61.7 ± 12.3 | −0.03 | 61.6 ± 11.3 | 61.6 ± 12.2 | <0.01 | |
| Age ≥65 years | 3312 | 1366 (41.2) | 357 (37.4) | 1009 (42.8) | −0.11 | 39.6% | 42.1% | −0.05 | |
| Male | 3312 | 1929 (58.2) | 620 (65.0) | 1309 (55.5) | 0.19 | 61.0% | 56.4% | 0.09 | |
| Body mass index, kg/m2 | 2656 | 27.1 ± 4.8 | 27.3 ± 5.1 | 27.0 ± 4.7 | 0.07 | 27.1 ± 4.3 | 27.0 ± 4.3 | 0.03 | |
| Primary renal disease | 3312 | ||||||||
| Hypertension nephropathy | 740 (22.3) | 190 (19.9) | 550 (23.3) | −0.08 | 22.2% | 22.7% | −0.01 | ||
| Diabetes nephropathy | 1933 (58.4) | 612 (64.2) | 1321 (56.0) | 0.17 | 61.2% | 57.3% | 0.08 | ||
| Chronic glomerulonephritis | 429 (13.0) | 106 (11.1) | 323 (13.7) | −0.08 | 12.0% | 13.3% | −0.04 | ||
| Others * | 210 (6.3) | 46 (4.8) | 164 (7.0) | −0.09 | 4.6% | 6.8% | −0.09 | ||
| Comorbidities | |||||||||
| Hypertension | 3312 | 2573 (77.7) | 761 (79.8) | 1812 (76.8) | 0.07 | 80.1% | 76.8% | 0.08 | |
| Diabetes mellitus | 3312 | 2163 (65.3) | 686 (71.9) | 1477 (62.6) | 0.20 | 70.1% | 63.8% | 0.13 | |
| Atrial fibrillation | 3312 | 104 (3.1) | 35 (3.7) | 69 (2.9) | 0.04 | 3.2% | 2.8% | 0.02 | |
| Peripheral artery disease | 3312 | 124 (3.7) | 30 (3.1) | 94 (4.0) | −0.05 | 2.9% | 3.9% | −0.06 | |
| Dementia | 3312 | 88 (2.7) | 26 (2.7) | 62 (2.6) | 0.01 | 2.5% | 2.6% | −0.01 | |
| Heart failure | 3312 | 141 (4.3) | 41 (4.3) | 100 (4.2) | <0.01 | 3.7% | 3.9% | −0.01 | |
| Myocardial infarction | 3312 | 219 (6.6) | 68 (7.1) | 151 (6.4) | 0.03 | 5.8% | 6.1% | −0.01 | |
| Stroke | 3312 | 368 (11.1) | 97 (10.2) | 271 (11.5) | −0.04 | 11.9% | 11.7% | 0.01 | |
| Admissions in the previous year | 3312 | ||||||||
| 0 | 2422 (73.1) | 768 (80.5) | 1654 (70.1) | 0.24 | 78.3% | 71.5% | 0.16 | ||
| 1–2 | 841 (25.4) | 173 (18.1) | 668 (28.3) | −0.24 | 20.5% | 27.0% | −0.15 | ||
| ≥3 | 49 (1.5) | 13 (1.4) | 36 (1.5) | −0.01 | 1.2% | 1.5% | −0.02 | ||
| Medication at baseline | |||||||||
| High potency statin | 3312 | 158 (4.8) | 50 (5.2) | 108 (4.6) | 0.03 | 5.9% | 4.7% | 0.06 | |
| ACEi/ARB | 3312 | 1839 (55.5) | 444 (46.5) | 1395 (59.2) | −0.25 | 54.7% | 57.9% | −0.06 | |
| Beta-blockers | 3312 | 854 (25.8) | 213 (22.3) | 641 (27.2) | −0.11 | 25.4% | 27.0% | −0.04 | |
| Calcium-channel blocker | 3312 | 1170 (35.3) | 281 (29.5) | 889 (37.7) | −0.18 | 35.3% | 37.2% | −0.04 | |
| Spironolacton | 3312 | 151 (4.6) | 21 (2.2) | 130 (5.5) | −0.17 | 3.0% | 5.2% | −0.11 | |
| Nitrates | 3312 | 480 (14.5) | 90 (9.4) | 390 (16.5) | −0.21 | 10.7% | 15.5% | −0.14 | |
| Vasodilator | 3312 | 46 (1.4) | 11 (1.2) | 35 (1.5) | −0.03 | 1.4% | 1.4% | <0.01 | |
| Thiazide | 3312 | 362 (10.9) | 96 (10.1) | 266 (11.3) | −0.04 | 12.6% | 11.1% | 0.05 | |
| Antiplatelet agents | 3312 | 1419 (42.8) | 434 (45.5) | 985 (41.8) | 0.08 | 45.4% | 41.8% | 0.07 | |
| NSAIDs | 3312 | 107 (3.2) | 30 (3.1) | 77 (3.3) | −0.01 | 3.9% | 3.3% | 0.04 | |
| Steroid | 3312 | 59 (1.8) | 11 (1.2) | 48 (2.0) | −0.07 | 1.7% | 1.9% | −0.02 | |
| Proton pump inhibitor | 3312 | 183 (5.5) | 35 (3.7) | 148 (6.3) | −0.12 | 3.4% | 5.9% | −0.12 | |
| Insulin | 3312 | 264 (8.0) | 50 (5.2) | 214 (9.1) | −0.15 | 6.2% | 8.8% | −0.10 | |
| OHAs | 3312 | 1555 (47.0) | 445 (46.6) | 1110 (47.1) | −0.01 | 49.3% | 47.9% | 0.03 | |
| Pentoxyfillin | 3312 | 91 (2.7) | 40 (4.2) | 51 (2.2) | 0.12 | 3.4% | 2.2% | 0.08 | |
| Sodium bicarbonate | 3312 | 9 (0.3) | 1 (0.1) | 8 (0.3) | −0.05 | 0.04% | 0.36% | −0.07 | |
| Laboratory data at baseline | |||||||||
| Creatinine, mg/dL | 3312 | 1.40 ± 0.29 | 1.39 ± 0.28 | 1.41 ± 0.29 | −0.06 | 1.40 ± 0.29 | 1.41 ± 0.29 | −0.01 | |
| eGFR, ml/min/1.73 m2 | 3312 | 47.3 ± 8.4 | 48.6 ± 8.2 | 46.8 ± 8.5 | 0.22 | 47.8 ± 8.5 | 47.0 ± 8.5 | 0.08 | |
| Blood urine nitrogen, mg/dL | 1773 | 24.2 ± 10.2 | 23.5 ± 9.3 | 24.4 ± 10.5 | −0.09 | 23.5 ± 7.5 | 23.8 ± 8.1 | −0.04 | |
| Proteinuria group, mg/dL | 1794 | ||||||||
| Negative or Trace (0–29) | 834 (46.5) | 262 (56.7) | 572 (42.9) | 0.28 | 52.1% | 43.8% | 0.17 | ||
| 1+ or 2+ (30–299) | 486 (27.1) | 110 (23.8) | 376 (28.2) | −0.10 | 24.7% | 28.0% | −0.08 | ||
| 3+ or 4+ (≥300) | 474 (26.4) | 90 (19.5) | 384 (28.8) | −0.22 | 23.2% | 28.2% | −0.11 | ||
| Potassium, mg/dL | 1973 | 4.1 ± 0.6 | 4.2 ± 0.6 | 4.1 ± 0.6 | 0.15 | 4.2 ± 0.4 | 4.2 ± 0.5 | 0.08 | |
| Sodium, mg/dL | 1609 | 138.9 ± 4.0 | 139.2 ± 4.0 | 138.8 ± 4.0 | 0.09 | 138.9 ± 2.9 | 139.0 ± 3.0 | −0.02 | |
| HbA1C, % | 2409 | 8.4 ± 2.2 | 8.1 ± 1.9 | 8.5 ± 2.3 | −0.19 | 8.0 ± 1.8 | 8.2 ± 2.1 | −0.08 | |
| Albumin, g/dL | 1026 | 3.6 ± 0.9 | 3.9 ± 0.7 | 3.5 ± 0.9 | 0.56 | 3.8 ± 0.5 | 3.7 ± 0.6 | 0.13 | |
| Hemoglobin, g/dL | 1884 | 12.7 ± 2.1 | 12.7 ± 2.1 | 12.7 ± 2.1 | 0.02 | 12.9 ± 1.6 | 12.9 ± 1.8 | <0.01 | |
| Uric acid, mg/dL | 2024 | 7.5 ± 2.0 | 6.9 ± 1.9 | 7.7 ± 2.0 | −0.44 | 7.2 ± 1.5 | 7.5 ± 1.6 | −0.19 | |
| Lipids profile at inclusion | |||||||||
| LDL, mg/dL | 2956 | 130.2 ± 70.0 | 122.9 ± 66.7 | 133.3 ± 71.2 | −0.15 | 123.2 ± 65.0 | 134.4 ± 69.2 | −0.17 | |
| HDL, mg/dL | 2362 | 40.3 ± 10.5 | 40.4 ± 10.7 | 40.2 ± 10.4 | 0.01 | 40.1 ± 9.0 | 40.0 ± 8.9 | 0.01 | |
| Total cholesterol, mg/dL | 2689 | 219.6 ± 64.8 | 208.2 ± 58.4 | 224.7 ± 66.8 | −0.26 | 216.4 ± 58.6 | 223.1 ± 62.7 | −0.11 | |
| Triglyceride, mg/dL | 3296 | 313.7 ± 195.6 | 310.6 ± 274.1 | 314.9 ± 153.7 | −0.02 | 315.7 ± 208.3 | 323.3 ± 169.9 | −0.04 | |
| Follow-up duration, year | 3312 | 7.0 ± 4.1 | 7.1 ± 3.9 | 6.9 ± 4.2 | 0.05 | 7.5 ± 3.9 | 7.0 ± 4.2 | 0.12 | |
| Before IPTW * | After GBM IPTW # | |||||
|---|---|---|---|---|---|---|
| Outcome | Fibrate (n = 705) | Non-Fibrate (n = 2020) | Fibrate | Non-Fibrate | HR/SHR (95% CI) of Fibrate | p Value |
| All-cause death | 54 (5.7) | 151 (6.4) | 5.7% | 6.1% | 0.91 (0.63–1.30) | 0.591 |
| MACCEs | ||||||
| Cardiovascular death | 29 (3.0) | 95 (4.0) | 3.2% | 3.8% | 0.81 (0.50–1.29) | 0.365 |
| Acute myocardial infarction | 45 (4.7) | 130 (5.5) | 4.4% | 5.4% | 0.77 (0.61–0.98) | 0.035 |
| Ischemic stroke | 84 (8.8) | 214 (9.1) | 9.2% | 8.9% | 1.02 (0.85–1.22) | 0.831 |
| Composite outcome $ | 138 (14.5) | 376 (15.9) | 14.7% | 15.6% | 0.91 (0.72–1.15) | 0.428 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ma, L.-Y.; Fan, P.-C.; Chen, C.-Y.; Tu, Y.-R.; Hsiao, C.-C.; Yen, C.-L.; Chang, C.-H. Can Concurrent Fibrate Use Reduce Cardiovascular Risks among Moderate Chronic Kidney Disease Patients Undergoing Statin Therapy? A Cohort Study. J. Clin. Med. 2024, 13, 168. https://doi.org/10.3390/jcm13010168
Ma L-Y, Fan P-C, Chen C-Y, Tu Y-R, Hsiao C-C, Yen C-L, Chang C-H. Can Concurrent Fibrate Use Reduce Cardiovascular Risks among Moderate Chronic Kidney Disease Patients Undergoing Statin Therapy? A Cohort Study. Journal of Clinical Medicine. 2024; 13(1):168. https://doi.org/10.3390/jcm13010168
Chicago/Turabian StyleMa, Li-Yi, Pei-Chun Fan, Chao-Yu Chen, Yi-Ran Tu, Ching-Chung Hsiao, Chieh-Li Yen, and Chih-Hsiang Chang. 2024. "Can Concurrent Fibrate Use Reduce Cardiovascular Risks among Moderate Chronic Kidney Disease Patients Undergoing Statin Therapy? A Cohort Study" Journal of Clinical Medicine 13, no. 1: 168. https://doi.org/10.3390/jcm13010168
APA StyleMa, L.-Y., Fan, P.-C., Chen, C.-Y., Tu, Y.-R., Hsiao, C.-C., Yen, C.-L., & Chang, C.-H. (2024). Can Concurrent Fibrate Use Reduce Cardiovascular Risks among Moderate Chronic Kidney Disease Patients Undergoing Statin Therapy? A Cohort Study. Journal of Clinical Medicine, 13(1), 168. https://doi.org/10.3390/jcm13010168