
Performance of the FebriDx Rapid Point-of-Care Test for Differentiating Bacterial and Viral Respiratory Tract Infections in Patients with a Suspected Respiratory Tract Infection in the Emergency Department
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Inclusion and Exclusion Criteria
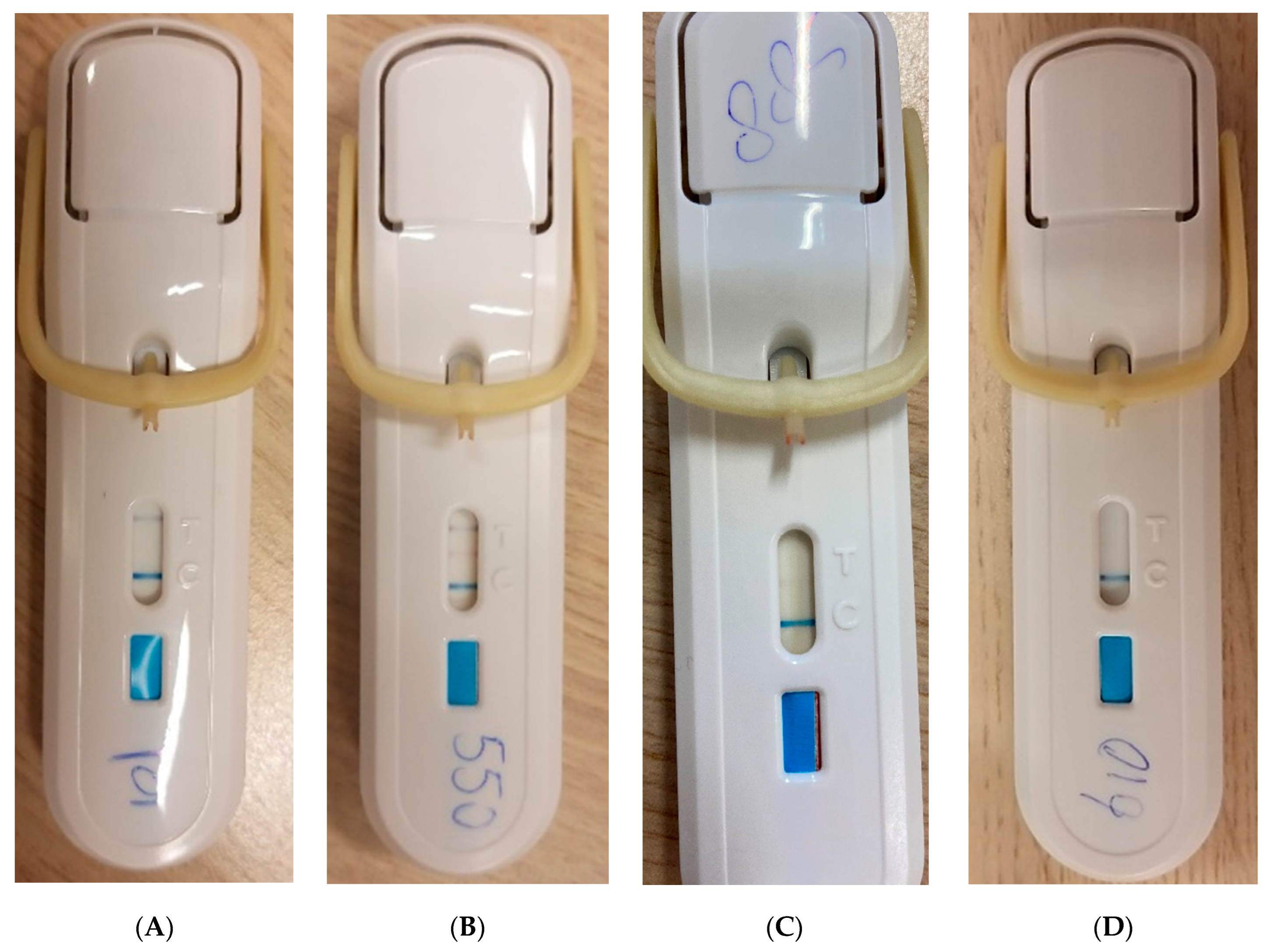
2.3. FebriDx Testing
2.4. Data Collection
2.5. Outcome
2.6. Statistical Analysis
3. Results
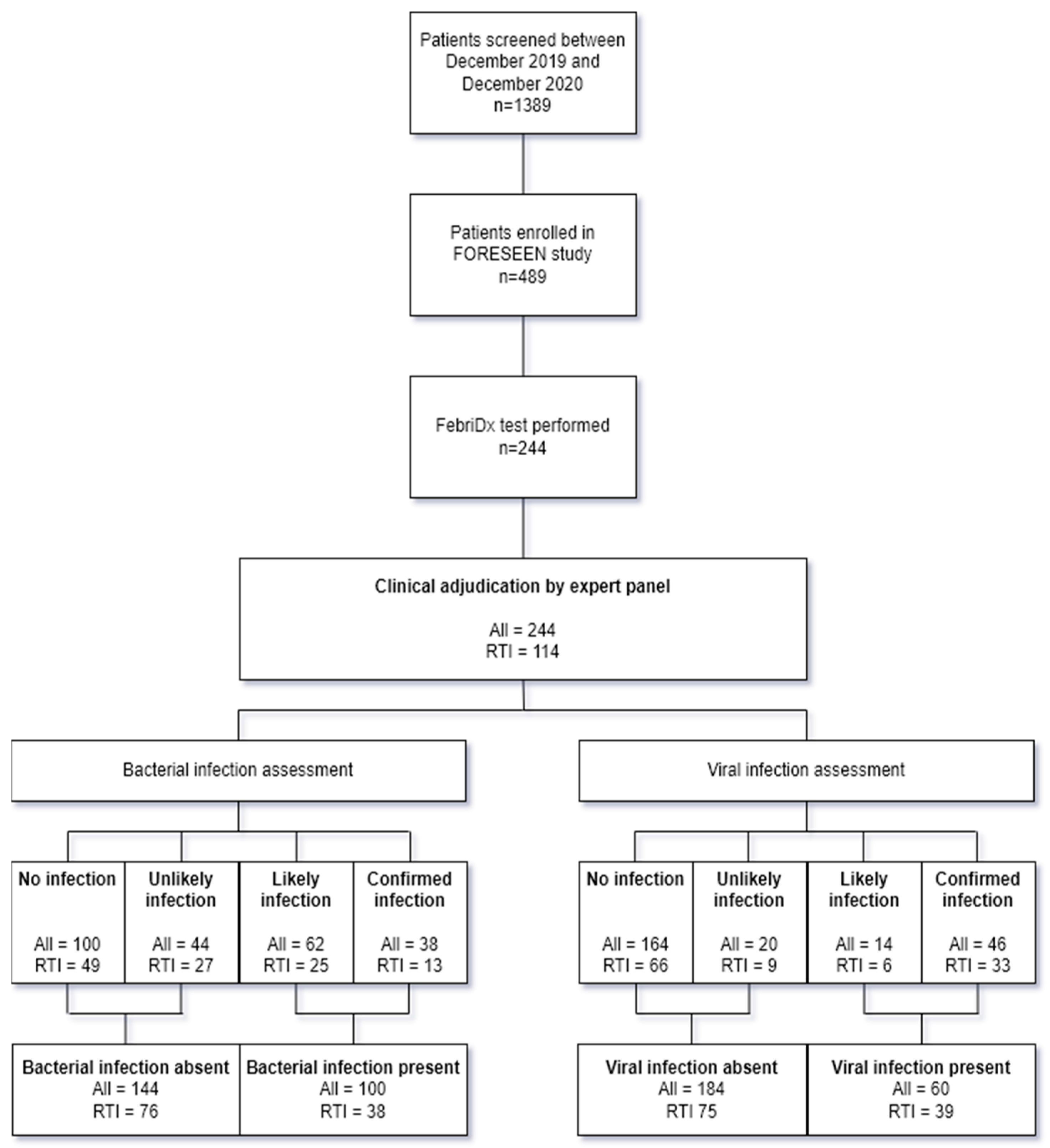
3.1. Clinical Adjudication
3.2. Diagnostic Accuracy FebriDx in Immunocompetent Patients with Symptoms of Acute RTI
3.3. Diagnostic Accuracy of FebriDx in the Total Cohort
3.4. Diagnostic Accuracy of FebriDx in Other Subgroups
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ferrer, R.; Martin-Loeches, I.; Phillips, G.; Osborn, T.M.; Townsend, S.; Dellinger, R.P.; Artigas, A.; Schorr, C.; Levy, M.M. Empiric antibiotic treatment reduces mortality in severe sepsis and septic shock from the first hour: Results from a guideline-based performance improvement program. Crit. Care Med. 2014, 42, 1749–1755. [Google Scholar] [CrossRef] [PubMed]
- Gabay, C.; Kushner, I. Acute-phase proteins and other systemic responses to inflammation. N. Engl. J. Med. 1999, 340, 448–454. [Google Scholar] [CrossRef] [PubMed]
- Wacker, C.; Prkno, A.; Brunkhorst, F.M.; Schlattmann, P. Procalcitonin as a diagnostic marker for sepsis: A systematic review and meta-analysis. Lancet Infect. Dis. 2013, 13, 426–435. [Google Scholar] [CrossRef]
- Lucas, G.; Bartolf, A.; Kroll, N.; De Thabrew, A.U.; Murtaza, Z.; Kumar, S.; Gani, A.; Annoni, A.; Parsons, M.; Pardoe, H. Procalcitonin (PCT) Level in the Emergency Department Identifies a High-Risk Cohort for All Patients Treated for Possible Sepsis. EJIFCC 2021, 32, 20–26. [Google Scholar] [PubMed]
- Magrini, L.; Gagliano, G.; Travaglino, F.; Vetrone, F.; Marino, R.; Cardelli, P.; Salerno, G.; Di Somma, S. Comparison between white blood cell count, procalcitonin and C reactive protein as diagnostic and prognostic biomarkers of infection or sepsis in patients presenting to emergency department. Clin. Chem. Lab. Med. 2014, 52, 1465–1472. [Google Scholar] [CrossRef] [PubMed]
- Hu, L.; Shi, Q.; Shi, M.; Liu, R.; Wang, C. Diagnostic Value of PCT and CRP for Detecting Serious Bacterial Infections in Patients with Fever of Unknown Origin: A Systematic Review and Meta-analysis. Appl. Immunohistochem. Mol. Morphol. 2017, 25, e61–e69. [Google Scholar] [CrossRef] [PubMed]
- Ronni, T.; Melén, K.; Malygin, A.; Julkunen, I. Control of IFN-inducible MxA gene expression in human cells. J. Immunol. 1993, 150, 1715–1726. [Google Scholar] [CrossRef]
- Haller, O.; Kochs, G. Human MxA protein: An interferon-induced dynamin-like GTPase with broad antiviral activity. J. Interferon Cytokine Res. 2011, 31, 79–87. [Google Scholar] [CrossRef]
- Nakabayashi, M.; Adachi, Y.; Itazawa, T.; Okabe, Y.; Kanegane, H.; Kawamura, M.; Tomita, A.; Miyawaki, T. MxA-based recognition of viral illness in febrile children by a whole blood assay. Pediatr. Res. 2006, 60, 770–774. [Google Scholar] [CrossRef]
- Engelmann, I.; Dubos, F.; Lobert, P.E.; Houssin, C.; Degas, V.; Sardet, A.; Decoster, A.; Dewilde, A.; Martinot, A.; Hober, D. Diagnosis of viral infections using myxovirus resistance protein A (MxA). Pediatrics 2015, 135, e985–e993. [Google Scholar] [CrossRef]
- Tong-Minh, K.; van Hooijdonk, S.; Versnel, M.A.; van Helden-Meeuwsen, C.G.; van Hagen, P.M.; van Gorp, E.C.M.; Endeman, H.; van der Does, Y.; Dalm, V.; Dik, W.A. Blood myxovirus resistance protein-1 measurement in the diagnostic work-up of suspected COVID-19 infection in the emergency department. Immun. Inflamm. Dis. 2022, 10, e609. [Google Scholar] [CrossRef] [PubMed]
- Brendish, N.J.; Malachira, A.K.; Armstrong, L.; Houghton, R.; Aitken, S.; Nyimbili, E.; Ewings, S.; Lillie, P.J.; Clark, T.W. Routine molecular point-of-care testing for respiratory viruses in adults presenting to hospital with acute respiratory illness (ResPOC): A pragmatic, open-label, randomised controlled trial. Lancet Respir. Med. 2017, 5, 401–411. [Google Scholar] [CrossRef] [PubMed]
- Fjelltveit, E.B.; Cox, R.J.; Ostensjo, J.; Blomberg, B.; Ebbesen, M.H.; Langeland, N.; Mohn, K.G. Point-of-care influenza testing impacts clinical decision, patient flow and length of stay in hospitalized adults. J. Infect. Dis. 2020, 226, 97–108. [Google Scholar] [CrossRef] [PubMed]
- Shirley, M. FebriDx((R)): A Rapid Diagnostic Test for Differentiating Bacterial and Viral Aetiologies in Acute Respiratory Infections. Mol. Diagn. Ther. 2019, 23, 803–809. [Google Scholar] [CrossRef] [PubMed]
- Shapiro, N.I.; Self, W.H.; Rosen, J.; Sharp, S.C.; Filbin, M.R.; Hou, P.C.; Parekh, A.D.; Kurz, M.C.; Sambursky, R. A prospective, multi-centre US clinical trial to determine accuracy of FebriDx point-of-care testing for acute upper respiratory infections with and without a confirmed fever. Ann. Med. 2018, 50, 420–429. [Google Scholar] [CrossRef] [PubMed]
- Bauer, W.; Kappert, K.; Galtung, N.; Lehmann, D.; Wacker, J.; Cheng, H.K.; Liesenfeld, O.; Buturovic, L.; Luethy, R.; Sweeney, T.E.; et al. A Novel 29-Messenger RNA Host-Response Assay from Whole Blood Accurately Identifies Bacterial and Viral Infections in Patients Presenting to the Emergency Department with Suspected Infections: A Prospective Observational Study. Crit. Care Med. 2021, 49, 1664–1673. [Google Scholar] [CrossRef]
- Houston, H.; Deas, G.; Naik, S.; Shah, K.; Patel, S.; Greca Dottori, M.; Tay, M.; Filson, S.A.; Biggin-Lamming, J.; Ross, J.; et al. Utility of the FebriDx point-of-care assay in supporting a triage algorithm for medical admissions with possible COVID-19: An observational cohort study. BMJ Open 2021, 11, e049179. [Google Scholar] [CrossRef]
- Mansbridge, C.T.; Tanner, A.R.; Beard, K.R.; Borca, F.; Phan, H.T.T.; Brendish, N.J.; Poole, S.; Hill, C.; Kiuber, M.; Crouch, R.; et al. FebriDx host response point-of-care testing improves patient triage for COVID-19 in the emergency department. Infect. Control Hosp. Epidemiol. 2022, 43, 979–986. [Google Scholar] [CrossRef]
- Lagi, F.; Trevisan, S.; Piccica, M.; Graziani, L.; Basile, G.; Mencarini, J.; Borchi, B.; Menicacci, L.; Vaudo, M.; Scotti, V.; et al. Use of the FebriDx point-of-care test for the exclusion of SARS-CoV-2 diagnosis in a population with acute respiratory infection during the second (COVID-19) wave in Italy. Int. J. Infect. Dis. 2021, 108, 231–236. [Google Scholar] [CrossRef]
- Karim, N.; Ashraf, M.Z.; Naeem, M.; Anwar, T.; Aung, H.; Mallik, S.; Avraam, E.; Kiran, S.; Bandapaati, S.; Khan, F.; et al. Utility of the FebriDx point-of-care test for rapid triage and identification of possible coronavirus disease 2019 (COVID-19). Int. J. Clin. Pract. 2021, 75, e13702. [Google Scholar] [CrossRef]
- Clark, T.W.; Brendish, N.J.; Poole, S.; Naidu, V.V.; Mansbridge, C.; Norton, N.; Wheeler, H.; Presland, L.; Ewings, S. Diagnostic accuracy of the FebriDx host response point-of-care test in patients hospitalised with suspected COVID-19. J. Infect. 2020, 81, 607–613. [Google Scholar] [CrossRef] [PubMed]
- Self, W.H.; Rosen, J.; Sharp, S.C.; Filbin, M.R.; Hou, P.C.; Parekh, A.D.; Kurz, M.C.; Shapiro, N.I. Diagnostic Accuracy of FebriDx: A Rapid Test to Detect Immune Responses to Viral and Bacterial Upper Respiratory Infections. J. Clin. Med. 2017, 6, 94. [Google Scholar] [CrossRef] [PubMed]
- Fattahi, M.; Rezaei, N.; Nematalahi, F.S.; Shaygannejad, V.; Fouladi, S.; Karimi, L.; Fathi, F.; Dehghani, L.; Mirmosayyeb, O.; Eskandari, N. MicroRNA-29b variants and MxA expression change during interferon beta therapy in patients with relapsing-remitting multiple sclerosis. Mult. Scler. Relat. Disord. 2019, 35, 241–245. [Google Scholar] [CrossRef] [PubMed]
- Buonsenso, D.; Sodero, G.; Valentini, P. Transcript host-RNA signatures to discriminate bacterial and viral infections in febrile children. Pediatr. Res. 2022, 91, 454–463. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Non-Infected | Only Bacterial Infection | Only Viral Infection | Detection of Bacterial and Viral Pathogens | All | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Total Cohort | Immunocompetent Acute RTI | Total Cohort | Immunocompetent Acute RTI | Total Cohort | Immunocompetent Acute RTI | Total Cohort | Immunocompetent Acute RTI | Total Cohort | Immunocompetent Acute RTI | ||
| (N = 95) | (N = 43) | (N = 90) | (N = 32) | (N = 49) | (N = 33) | (N = 10) | (N = 6) | (N = 244) | (N = 114) | ||
| Demograpic data | |||||||||||
| Age | median (IQR) | 57.5 (28.0) | 63.0 (27.5) | 64.5 (15.0) | 64.5 (13.8) | 57.0 (16.5) | 57.0 (9.00) | 51.5 (6.25) | 50.5 (6.25) | 59.0 (21.0) | 59.0 (19.8) |
| Sex: male | n (%) | 45 (44.1%) | 23 (53.5%) | 45 (54.9%) | 16 (50.0%) | 32 (64.0%) | 19 (57.6%) | 6 (60.0%) | 5 (83.3%) | 128 (52.5%) | 63 (55.3%) |
| Comorbidity: Cardiovascular disease | n (%) | 39 (38.2%) | 16 (37.2%) | 42 (51.2%) | 15 (46.9%) | 22 (44.0%) | 13 (39.4%) | 4 (40.0%) | 2 (33.3%) | 107 (43.9%) | 46 (40.4%) |
| Comorbidity: Central nervous system diseases | n (%) | 5 (4.9%) | 3 (7.0%) | 8 (9.8%) | 3 (9.4%) | 1 (2.0%) | 1 (3.0%) | 0 (0%) | 0 (0%) | 14 (5.7%) | 7 (6.1%) |
| Comorbidity: pulmonary disease | n (%) | 40 (39.2%) | 14 (32.6%) | 26 (31.7%) | 14 (43.8%) | 18 (36.0%) | 12 (36.4%) | 4 (40.0%) | 2 (33.3%) | 88 (36.1%) | 42 (36.8%) |
| Comorbidity: Diabetes Mellitus | n (%) | 15 (14.7%) | 6 (14.0%) | 23 (28.0%) | 5 (15.6%) | 11 (22.0%) | 8 (24.2%) | 4 (40.0%) | 1 (16.7%) | 53 (21.7%) | 20 (17.5%) |
| Comorbidity: Renal disease | n (%) | 7 (6.9%) | 2 (4.7%) | 17 (20.7%) | 3 (9.4%) | 7 (14.0%) | 2 (6.1%) | 2 (20.0%) | 0 (0%) | 33 (13.5%) | 7 (6.1%) |
| Comorbidity: Liver disease | n (%) | 4 (3.9%) | 1 (2.3%) | 5 (6.1%) | 2 (6.3%) | 4 (8.0%) | 1 (3.0%) | 1 (10.0%) | 0 (0%) | 14 (5.7%) | 4 (3.5%) |
| Comorbidity: Malignancy | n (%) | 30 (29.4%) | 16 (37.2%) | 31 (37.8%) | 16 (50.0%) | 7 (14.0%) | 4 (12.1%) | 1 (10.0%) | 1 (16.7%) | 69 (28.3%) | 37 (32.5%) |
| Comorbidity: Immunodeficiency | n (%) | 7 (6.9%) | 43 (100%) | 1 (1.2%) | 32 (100%) | 1 (2.0%) | 33 (100%) | 1 (10.0%) | 6 (100%) | 10 (4.1%) | 114 (100%) |
| Comorbidity: Auto-immune diseases | 18 (17.6%) | 2 (4.7%) | 15 (18.3%) | 3 (9.4%) | 5 (10.0%) | 3 (9.1%) | 2 (20.0%) | 0 (0%) | 40 (16.4%) | 8 (7.0%) | |
| Comorbidity: Solid organ transplantation | 13 (12.7%) | 3 (7.0%) | 16 (19.5%) | 0 (0%) | 12 (24.0%) | 2 (6.1%) | 1 (10.0%) | 0 (0%) | 42 (17.2%) | 5 (4.4%) | |
| Vital signs | |||||||||||
| Heartrate | Mean (SD) | 90.2 (16.6) | 93.1 (19.2) | 98.5 (19.7) | 99.7 (17.5) | 96.3 (16.1) | 94.4 (15.8) | 101 (22.5) | 103 (24.0) | 94.7 (18.2) | 95.8 (18.1) |
| Systolic blood pressure | Mean (SD) | 141 (22.9) | 139 (21.3) | 135 (24.1) | 134 (21.7) | 137 (20.0) | 136 (19.3) | 132 (17.0) | 142 (20.7) | 138 (22.6) | 137 (20.7) |
| Diastolic blood pressure | Mean (SD) | 85.6 (14.9) | 82.9 (16.7) | 82.0 (15.9) | 81.5 (14.0) | 84.0 (13.9) | 83.2 (14.1) | 84.4 (18.7) | 84.2 (8.45) | 84.0 (15.2) | 82.6 (14.8) |
| Temperature (Celcius) | Mean (SD) | 37.0 (0.706) | 37.1 (0.723) | 37.6 (0.820) | 37.7 (0.875) | 37.5 (0.807) | 37.4 (0.851) | 37.7 (0.650) | 37.7 (0.417) | 37.4 (0.810) | 37.4 (0.822) |
| Respiratory rate | Mean (SD) | 19.7 (5.09) | 19.4 (5.09) | 21.2 (6.46) | 23.0 (7.49) | 21.1 (5.46) | 22.1 (5.44) | 22.8 (5.01) | 22.0 (4.38) | 20.6 (5.69) | 21.4 (6.05) |
| SpO2 | median (IQR) | 95.2 (8.93) | 96.0 (2.00) | 95.3 (3.22) | 95.5 (2.25) | 95.0 (5.22) | 95.0 (3.00) | 95.0 (3.62) | 96.5 (1.00) | 95.2 (6.53) | 96.0 (3.00) |
| Laboratory tests | |||||||||||
| CRP | median (IQR) | 36.3 (53.9) | 10.0 (41.7) | 131 (112) | 104 (132) | 56.0 (67.5) | 33.0 (51.2) | 82.9 (65.6) | 70.0 (95.5) | 74.1 (90.9) | 34.5 (93.9) |
| WBC | median (IQR) | 12.0 (40.9) | 8.40 (4.45) | 103 (135) | 12.2 (6.08) | 42.5 (52.5) | 7.10 (3.10) | 81.0 (112) | 6.30 (5.68) | 42.5 (92.7) | 8.60 (5.58) |
| PCT | median (IQR) | 0.0500 (0.0775) | 0.0600 (0.160) | 0.290 (0.730) | 0.150 (0.475) | 0.0700 (0.0675) | 0.0600 (0.0600) | 0.365 (0.518) | 0.140 (0.163) | 0.100 (0.250) | 0.0900 (0.215) |
| Disposition and severity | |||||||||||
| Discharge home | n (%) | 61 (64.2%) | 25 (58.1%) | 15 (16.4%) | 5 (15.6%) | 18 (36.7%) | 11 (33.3%) | 4 (36.4%) | 3 (50.0%) | 98 (40.2%) | 44 (38.6%) |
| Admission to general ward | n (%) | 34 (35.8%) | 18 (41.9%) | 74 (83.1%) | 27 (84.4%) | 30 (61.2%) | 21 (63.6%) | 7 (63.6%) | 3 (50.0%) | 145 (59.4%) | 69 (60.5%) |
| Admission to intensive care unit | n (%) | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) | 1 (2.0%) | 1 (3.0%) | 0 (0%) | 0 (0%) | 1 (0.4%) | 1 (0.9%) |
| Admission duration | median (IQR) | 0 (3.00) | 0 (3.50) | 6.00 (6.00) | 8.00 (7.25) | 5.00 (8.00) | 5.00 (8.00) | 3.00 (8.00) | 1.50 (6.75) | 3.00 (7.00) | 3.00 (8.00) |
| 30-day mortality | n (%) | 1 (1.1%) | 1 (2.3%) | 5 (5.6%) | 4 (12.5%) | 1 (2.0%) | 0 (0%) | 0 (0%) | 0 (0%) | 7 (2.9%) | 5 (4.5%) |
| All Patients N = 244 | RTI Immunocompetent Patients N = 114 | ||
|---|---|---|---|
| Microbiological Results | Number of Patients | Microbiological Results | Number of Patients |
| Blood Cultures | Blood Cultures | ||
| Escherichia coli (E. coli) Staphylococcus epidermidis (S. epidermidis) Klebsiella pneumoniae (K. pneumoniae) Staphylococcus hominis (S. hominis) Staphylococcus aureus (S. aureus) Staphylococcus capitis (S. capitis) Streptococcus pneumoniae (S.pneumoniae) Streptococcus Hemolyticus Micrococcus luteus (M. luteus) Parabacteroides distasonis Rothia mucilaginosa Stenotrophomonas maltophilia | 4 3 3 2 1 1 1 2 1 1 1 1 | Escherichia coli (E. coli) Staphylococcus epidermidis (S. epidermidis) Klebsiella pneumoniae (K. pneumoniae) Staphylococcus hominis (S. hominis) Staphylococcus aureus (S. aureus) Staphylococcus capitis (S. capitis) Streptococcus pneumoniae (S. pneumoniae) Streptococcus Hemolyticus Micrococcus luteus (M. luteus) Parabacteroides distasonis Rothia mucilaginosa Stenotrophomonas maltophilia | 0 2 0 2 0 1 1 1 0 0 1 0 |
| Urine antigen testing | Urine antigen testing | ||
| Streptococcus pneumoniae (S. pneumoniae) | 1 | Streptococcus pneumoniae (S. pneumoniae) | 0 |
| Sputum cultures | Sputum cultures | ||
| Staphylococcus aureus (S. aureus) Pseudomonas aeruginosa Aspergillus fumigatus Achromobacter xylosoxidans Burkholderia cenocepacia Mycoplasma pneumoniae Proteus mirabilis Serratia marcescens Alcaligenes faecalis Pneumocystis jirovecii | 3 2 1 1 1 1 1 1 1 1 | Staphylococcus aureus (S. aureus) Pseudomonas aeruginosa Aspergillus fumigatus Achromobacter xylosoxidans Burkholderia cenocepacia Mycoplasma pneumoniae Proteus mirabilis Serratia marcescens Alcaligenes faecalis Pneumocystis jirovecii | 1 1 1 1 1 0 1 1 1 1 |
| Urine cultures | Urine cultures | ||
| Escherichia coli (E. coli) Actinotignum schaalii Enterococcus faecalis (E. faecalis) Pseudomonas species Acinetobacter baumannii calcoaceticus complex Enterococcus cloacae (E. cloacae) Staphylococcus aureus (S. aureus) Serratia marcescens Achromobacter xylosoxidans | 7 2 2 1 1 1 2 1 1 | Escherichia coli (E. coli) Actinotignum schaalii Enterococcus faecalis (E. faecalis) Pseudomonas species Acinetobacter baumannii calcoaceticus complex Enterococcus cloacae (E. cloacae) Staphylococcus aureus (S. aureus) Serratia marcescens Achromobacter xylosoxidans | 1 1 0 0 0 0 0 0 0 |
| Other cultures | Other cultures | ||
| Pseudomona aeruginosa Streptococcus pneumoniae (S.pneumoniae) Streptococcus dysgalactiae (S. dysgalactiae) Staphylococcus aureus (S. aureus) Clostridium difficile (C. difficile) Campylobacter jejuni | 3 1 1 1 2 1 | Pseudomona aeruginosa Streptococcus pneumoniae (S.pneumoniae) Streptococcus dysgalactiae (S. dysgalactiae) Staphylococcus aureus (S. aureus) Clostridium difficile (C. difficile) Campylobacter jejuni | 3 1 1 0 1 0 |
| Molecular diagnostics | Molecular diagnostics | ||
| SARS-CoV-2 Rhinovirus Human metapneumovirus (hMPV) hMPV + Rhinovirus Influenza (A or B) Adenovirus Bocavirus Cytomegalovirus (CMV) Respiratory syncytial virus (RSV) | 28 7 3 1 5 1 1 2 1 | SARS-CoV-2 Rhinovirus Human metapneumovirus (hMPV) hMPV + Rhinovirus Influenza (A or B) Adenovirus Bocavirus Cytomegalovirus (CMV) Respiratory syncytial virus (RSV) | 22 3 3 1 4 0 1 0 1 |
| Diagnostic Accuracy of FebriDx in RTI Different Subgroups | Infection Type | Number of Patients in Analysis | Sensitivity | Specificity | Positive Predictive Value | Negative Predictive Value |
|---|---|---|---|---|---|---|
| All patients | Bacterial infections | 244 | 87% (78–90%) | 62% (56–72%) | 60% (51–68%) | 89% (82–94%) |
| Viral infections | 244 | 49% (36–63%) | 94% (90–97%) | 72% (56–85%) | 85% (80–90%) | |
| RTI immunocompetent | Bacterial infections | 114 | 87% (72–96%) | 67% (55–77%) | 57% (43–70%) | 91% (80–97%) |
| Viral infections | 114 | 56% (40–72%) | 92% (83–97%) | 79% (59–92%) | 80% (70–92%) | |
| RTI immunocompromised | Bacterial infections | 50 | 71% (49–87%) | 81% (61–93%) | 77% (55–92%) | 75% (55–92%) |
| Viral infections | 50 | 44% (20–70%) | 100% (90–100%) | 100% (59–100%) | 79% (64–90%) | |
| RTI immunocompetent confirmed infections | Bacterial infections | 57 | 85% (55–98%) | 71% (57–83%) | 44% (24–65%) | 95% (82–99%) |
| Viral infections | 98 | 58% (39–75%) | 97% (89–100%) | 90% (70–99%) | 82% (71–90%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tong-Minh, K.; Daenen, K.; Endeman, H.; Ramakers, C.; Gommers, D.; van Gorp, E.; van der Does, Y. Performance of the FebriDx Rapid Point-of-Care Test for Differentiating Bacterial and Viral Respiratory Tract Infections in Patients with a Suspected Respiratory Tract Infection in the Emergency Department. J. Clin. Med. 2024, 13, 163. https://doi.org/10.3390/jcm13010163
Tong-Minh K, Daenen K, Endeman H, Ramakers C, Gommers D, van Gorp E, van der Does Y. Performance of the FebriDx Rapid Point-of-Care Test for Differentiating Bacterial and Viral Respiratory Tract Infections in Patients with a Suspected Respiratory Tract Infection in the Emergency Department. Journal of Clinical Medicine. 2024; 13(1):163. https://doi.org/10.3390/jcm13010163
Chicago/Turabian StyleTong-Minh, Kirby, Katrijn Daenen, Henrik Endeman, Christian Ramakers, Diederik Gommers, Eric van Gorp, and Yuri van der Does. 2024. "Performance of the FebriDx Rapid Point-of-Care Test for Differentiating Bacterial and Viral Respiratory Tract Infections in Patients with a Suspected Respiratory Tract Infection in the Emergency Department" Journal of Clinical Medicine 13, no. 1: 163. https://doi.org/10.3390/jcm13010163
APA StyleTong-Minh, K., Daenen, K., Endeman, H., Ramakers, C., Gommers, D., van Gorp, E., & van der Does, Y. (2024). Performance of the FebriDx Rapid Point-of-Care Test for Differentiating Bacterial and Viral Respiratory Tract Infections in Patients with a Suspected Respiratory Tract Infection in the Emergency Department. Journal of Clinical Medicine, 13(1), 163. https://doi.org/10.3390/jcm13010163