
BRAF Inhibitors in BRAF-Mutated Colorectal Cancer: A Systematic Review

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Inclusion and Exclusion Criteria
2.3. Data Extraction
2.4. Risk of Bias Assessment
3. Results
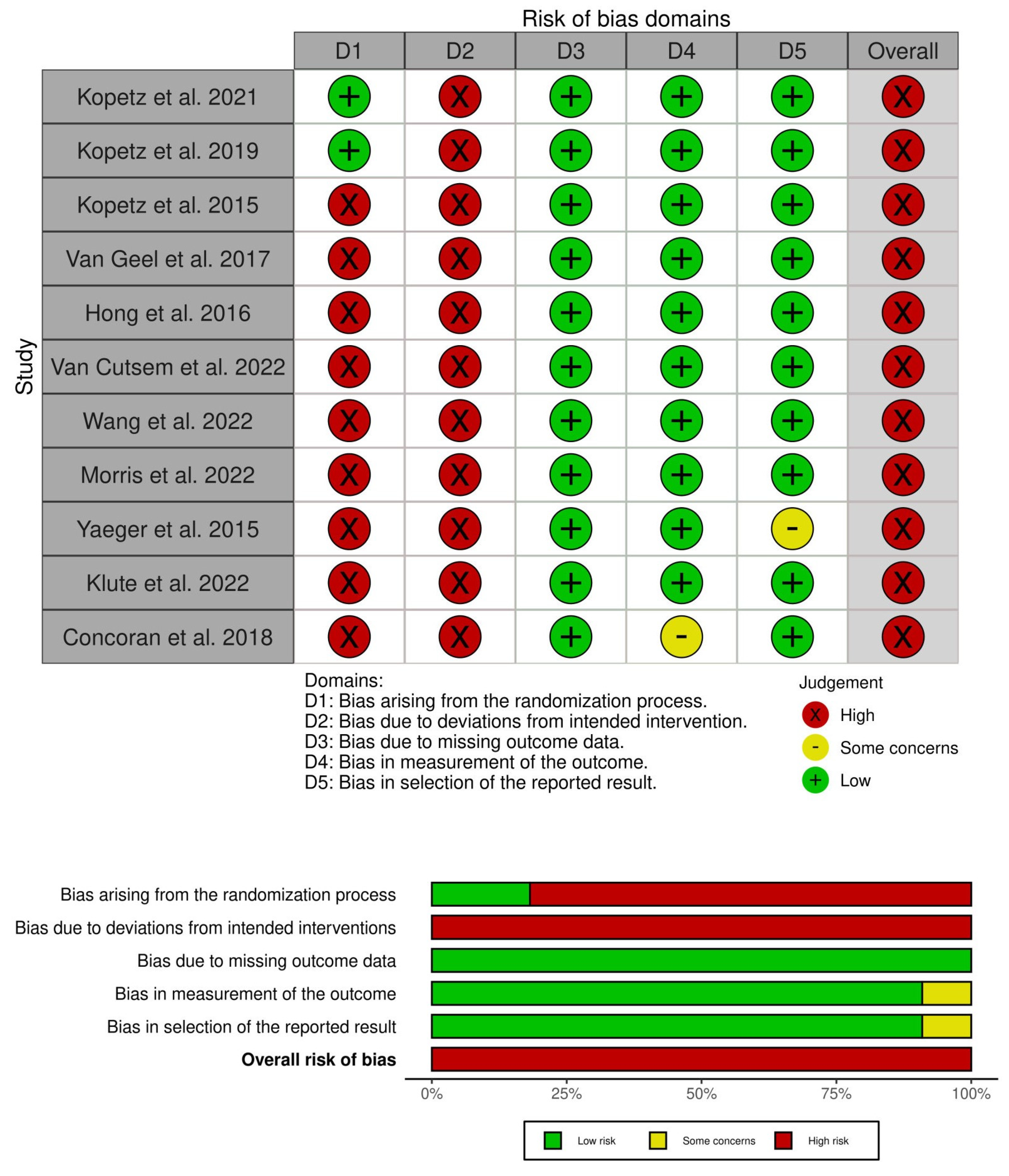
3.1. Risk of Bias
3.2. BRAF Inhibitors in Relapsed/Refractory (R/R) mCRC
3.2.1. Efficacy
3.2.2. Safety
3.3. BRAF Inhibitor as First-Line Therapy in mCRC
3.4. Ongoing Clinical Trials
4. Discussion
5. Conclusions
6. Limitation
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Biller, L.H.; Schrag, D. Diagnosis and Treatment of Metastatic Colorectal Cancer: A Review. Jama 2021, 325, 669–685. [Google Scholar] [CrossRef] [PubMed]
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Qin, B.D.; Ye, C.Y.; Wang, M.M.; Yuan, L.Y.; Dai, W.P.; Sun, L.; Liu, K.; Qin, W.X.; Jiao, X.D.; et al. Cetuximab and vemurafenib plus FOLFIRI (5-fluorouracil/leucovorin/irinotecan) for BRAF V600E-mutated advanced colorectal cancer (IMPROVEMENT): An open-label, single-arm, phase II trial. Eur. J. Cancer 2022, 163, 152–162. [Google Scholar] [CrossRef] [PubMed]
- Guerrero, R.M.; Labajos, V.A.; Ballena, S.L.; Macha, C.A.; Lezama, M.S.; Roman, C.P.; Beltran, P.M.; Torrejon, A.F. Targeting BRAF V600E in metastatic colorectal cancer: Where are we today? Ecancermedicalscience 2022, 16, 1489. [Google Scholar] [CrossRef] [PubMed]
- Mao, M.; Tian, F.; Mariadason, J.M.; Tsao, C.C.; Lemos, R., Jr.; Dayyani, F.; Gopal, Y.N.; Jiang, Z.Q.; Wistuba, I.I.; Tang, X.M.; et al. Resistance to BRAF inhibition in BRAF-mutant colon cancer can be overcome with PI3K inhibition or demethylating agents. Clin. Cancer Res. Off. J. Am. Assoc. Cancer Res. 2013, 19, 657–667. [Google Scholar] [CrossRef] [PubMed]
- Corcoran, R.B.; Atreya, C.E.; Falchook, G.S.; Kwak, E.L.; Ryan, D.P.; Bendell, J.C.; Hamid, O.; Messersmith, W.A.; Daud, A.; Kurzrock, R.; et al. Combined BRAF and MEK Inhibition With Dabrafenib and Trametinib in BRAF V600-Mutant Colorectal Cancer. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2015, 33, 4023–4031. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions; The Cochrane Collaboration: London, UK, 2008; Available online: https://training.cochrane.org/handbook/archive/v5.0.0/ (accessed on 7 October 2023).
- Sarkis-Onofre, R.; Catalá-López, F.; Aromataris, E.; Lockwood, C. How to properly use the PRISMA Statement. Syst. Rev. 2021, 10, 117. [Google Scholar] [CrossRef]
- Amir-Behghadami, M.; Janati, A. Population, Intervention, Comparison, Outcomes and Study (PICOS) design as a framework to formulate eligibility criteria in systematic reviews. Emerg. Med. J. 2020, 37, 386. [Google Scholar] [CrossRef]
- Sterne, J.A.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.-Y.; Corbett, M.S.; Eldridge, S.M. RoB 2: A revised tool for assessing risk of bias in randomised trials. bmj 2019, 366, 14898. [Google Scholar] [CrossRef]
- Kopetz, S.; Grothey, A.; Yaeger, R.; Van Cutsem, E.; Desai, J.; Yoshino, T.; Wasan, H.; Ciardiello, F.; Loupakis, F.; Hong, Y.S.; et al. Encorafenib, Binimetinib, and Cetuximab in BRAF V600E-Mutated Colorectal Cancer. N. Engl. J. Med. 2019, 381, 1632–1643. [Google Scholar] [CrossRef]
- Kopetz, S.; Guthrie, K.A.; Morris, V.K.; Lenz, H.J.; Magliocco, A.M.; Maru, D.; Yan, Y.; Lanman, R.; Manyam, G.; Hong, D.S.; et al. Randomized Trial of Irinotecan and Cetuximab With or Without Vemurafenib in BRAF-Mutant Metastatic Colorectal Cancer (SWOG S1406). J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2021, 39, 285–294. [Google Scholar] [CrossRef] [PubMed]
- Kopetz, S.; Desai, J.; Chan, E.; Hecht, J.R.; O’Dwyer, P.J.; Maru, D.; Morris, V.; Janku, F.; Dasari, A.; Chung, W.; et al. Phase II Pilot Study of Vemurafenib in Patients With Metastatic BRAF-Mutated Colorectal Cancer. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2015, 33, 4032–4038. [Google Scholar] [CrossRef] [PubMed]
- van Geel, R.; Tabernero, J.; Elez, E.; Bendell, J.C.; Spreafico, A.; Schuler, M.; Yoshino, T.; Delord, J.P.; Yamada, Y.; Lolkema, M.P.; et al. A Phase Ib Dose-Escalation Study of Encorafenib and Cetuximab with or without Alpelisib in Metastatic BRAF-Mutant Colorectal Cancer. Cancer Discov. 2017, 7, 610–619. [Google Scholar] [CrossRef] [PubMed]
- Hong, D.S.; Morris, V.K.; El Osta, B.; Sorokin, A.V.; Janku, F.; Fu, S.; Overman, M.J.; Piha-Paul, S.; Subbiah, V.; Kee, B.; et al. Phase IB Study of Vemurafenib in Combination with Irinotecan and Cetuximab in Patients with Metastatic Colorectal Cancer with BRAFV600E Mutation. Cancer Discov. 2016, 6, 1352–1365. [Google Scholar] [CrossRef] [PubMed]
- Morris, V.K.; Parseghian, C.M.; Escano, M.; Johnson, B.; Raghav, K.P.S.; Dasari, A.; Huey, R.; Overman, M.J.; Willis, J.; Lee, M.S.; et al. Phase I/II trial of encorafenib, cetuximab, and nivolumab in patients with microsatellite stable, BRAFV600E metastatic colorectal cancer. J. Clin. Oncol. 2022, 40, 12. [Google Scholar] [CrossRef]
- Yaeger, R.; Cercek, A.; O’Reilly, E.M.; Reidy, D.L.; Kemeny, N.; Wolinsky, T.; Capanu, M.; Gollub, M.J.; Rosen, N.; Berger, M.F.; et al. Pilot trial of combined BRAF and EGFR inhibition in BRAF-mutant metastatic colorectal cancer patients. Clin. Cancer Res. 2015, 21, 1313–1320. [Google Scholar] [CrossRef] [PubMed]
- Klute, K.A.; Rothe, M.; Garrett-Mayer, E.; Mangat, P.K.; Nazemzadeh, R.; Yost, K.J.; Duvivier, H.L.; Ahn, E.R.; Cannon, T.L.; Alese, O.B.; et al. Cobimetinib Plus Vemurafenib in Patients With Colorectal Cancer With BRAF Mutations: Results From the Targeted Agent and Profiling Utilization Registry (TAPUR) Study. JCO Precis. Oncol. 2022, 6, e2200191. [Google Scholar] [CrossRef]
- Corcoran, R.B.; André, T.; Atreya, C.E.; Schellens, J.H.M.; Yoshino, T.; Bendell, J.C.; Hollebecque, A.; McRee, A.J.; Siena, S.; Middleton, G.; et al. Combined BRAF, EGFR, and MEK Inhibition in Patients with BRAFV600E-Mutant Colorectal Cancer. Cancer Discov. 2018, 8, 428–443. [Google Scholar] [CrossRef]
- Van Cutsem, E.; Taieb, J.; Yaeger, R.; Yoshino, T.; Grothey, A.; Maiello, E.; Elez, E.; Dekervel, J.; Ross, P.; Ruiz-Casado, A.; et al. ANCHOR CRC: Results From a Single-Arm, Phase II Study of Encorafenib Plus Binimetinib and Cetuximab in Previously Untreated BRAF(V600E)-Mutant Metastatic Colorectal Cancer. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2023, 41, 2628–2637. [Google Scholar] [CrossRef]
- Robert, C.; Karaszewska, B.; Schachter, J.; Rutkowski, P.; Mackiewicz, A.; Stroiakovski, D.; Lichinitser, M.; Dummer, R.; Grange, F.; Mortier, L.; et al. Improved Overall Survival in Melanoma with Combined Dabrafenib and Trametinib. N. Engl. J. Med. 2014, 372, 30–39. [Google Scholar] [CrossRef]
- Pietrantonio, F.; Petrelli, F.; Coinu, A.; Di Bartolomeo, M.; Borgonovo, K.; Maggi, C.; Cabiddu, M.; Iacovelli, R.; Bossi, I.; Lonati, V.; et al. Predictive role of BRAF mutations in patients with advanced colorectal cancer receiving cetuximab and panitumumab: A meta-analysis. Eur. J. Cancer 2015, 51, 587–594. [Google Scholar] [CrossRef] [PubMed]
- Stintzing, S.; Heinrich, K.; Tougeron, D.; Modest, D.P.; Schwaner, I.; Eucker, J.; Pihusch, R.; Stauch, M.; Kaiser, F.; Kahl, C.; et al. FOLFOXIRI Plus Cetuximab or Bevacizumab as First-Line Treatment of BRAF(V600E)-Mutant Metastatic Colorectal Cancer: The Randomized Phase II FIRE-4.5 (AIO KRK0116) Study. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2023, 41, 4143–4153. [Google Scholar] [CrossRef] [PubMed]
- Lito, P.; Rosen, N.; Solit, D.B. Tumor adaptation and resistance to RAF inhibitors. Nat. Med. 2013, 19, 1401–1409. [Google Scholar] [CrossRef] [PubMed]
- Boccaccino, A.; Borelli, B.; Intini, R.; Antista, M.; Bensi, M.; Rossini, D.; Passardi, A.; Tamberi, S.; Giampieri, R.; Antonuzzo, L.; et al. Encorafenib plus cetuximab with or without binimetinib in patients with BRAF V600E-mutated metastatic colorectal cancer: Real-life data from an Italian multicenter experience. ESMO Open 2022, 7, 100506. [Google Scholar] [CrossRef] [PubMed]
- Loupakis, F.; Intini, R.; Cremolini, C.; Orlandi, A.; Sartore-Bianchi, A.; Pietrantonio, F.; Pella, N.; Spallanzani, A.; Dell’Aquila, E.; Scartozzi, M.; et al. A validated prognostic classifier for V600EBRAF-mutated metastatic colorectal cancer: The ‘BRAF BeCool’ study. Eur. J. Cancer 2019, 118, 121–130. [Google Scholar] [CrossRef] [PubMed]
- Elez, E.; Ros, J.; Fernández, J.; Villacampa, G.; Moreno-Cárdenas, A.B.; Arenillas, C.; Bernatowicz, K.; Comas, R.; Li, S.; Kodack, D.P.; et al. RNF43 mutations predict response to anti-BRAF/EGFR combinatory therapies in BRAFV600E metastatic colorectal cancer. Nat. Med. 2022, 28, 2162–2170. [Google Scholar] [CrossRef]
- Ros, J.; Matito, J.; Villacampa, G.; Comas, R.; Garcia, A.; Martini, G.; Baraibar, I.; Saoudi, N.; Salvà, F.; Martin, Á.; et al. Plasmatic BRAF-V600E allele fraction as a prognostic factor in metastatic colorectal cancer treated with BRAF combinatorial treatments. Ann. Oncol. 2023, 34, 543–552. [Google Scholar] [CrossRef]
- Kopetz, S.; Murphy, D.A.; Pu, J.; Ciardiello, F.; Desai, J.; Grothey, A.; Van Cutsem, E.; Wasan, H.S.; Yaeger, R.; Yoshino, T.; et al. Molecular correlates of clinical benefit in previously treated patients (pts) with BRAF V600E-mutant metastatic colorectal cancer (mCRC) from the BEACON study. J. Clin. Oncol. 2021, 39, 3513. [Google Scholar] [CrossRef]
- Michael, T.P.; Daniel, D.B.; Bryony, T.; Joanne, P.Y.; Amanda, B.S. Correlation of tumour BRAF mutations and methylation with germline mismatch repair (MMR) gene mutation status: A literature review assessing utility of tumour features for MMR variant classification. J. Med. Genet. 2012, 49, 151. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Author et al. | NCT | Phase of Trial | Treatment Regimen | Participants (n) | Age Median (Years) | Sex | ECOG Performance | Location of Primary Tumor | Involvement of ≥3 Organs (and/or Locations Involved) | Number of Previous Lines of Therapies | High MSI | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Male | Female | Left Side of Colon (or Rectum) | Right Side of Colon (or Appendix) | Colon | Rectal | ||||||||||
| Randomized clinical trials on relapsed/refractory patients | |||||||||||||||
| Kopetz et al., 2019 [11] | NCT02928224 | Phase III | Encorafenib + Binimetinib + Cetuximab | 224 | 62 | 105 | 119 | 0 = 116 1 = 108 | 79 | 126 | 19 | NA | Involvement of ≥3 organs = 110, Liver = 144 | 1 = 146 2 = 78 | 22 |
| Encorafenib + Cetuximab | 220 | 61 | 115 | 105 | 0 = 112 1 = 104 | 83 | 110 | 27 | NA | Involvement of ≥3 organs = 103, Liver = 134 | 1 = 123 2 = 97 | 19 | |||
| Cetuximab and Irinotecan OR Cetuximab and FOLFIRI (Control) | 221 | 60 | 94 | 127 | 0 = 108 1 = 113 | 68 | 119 | 34 | NA | Involvement of ≥3 organs = 98, Liver = 128 | 1 = 145 2 = 76 | 12 | |||
| Kopetz et al., 2021 [12] | NCT02164916 | Phase II | Cetuximab + Irinotecan | 50 | 61.9 | 13 | 37 | 0 = 23 1 = 27 | 17 | 30 | NA | 3 | Distant Lymph Nodes = 14, Lung = 21, Liver = 28, Bone = 2, Peritoneum = 16 | 1 = 25 2 = 17 | 7 |
| Vemurafenib + Cetuximab + Irinotecan | 50 | 59.7 | 29 | 21 | 0 = 24 1 = 26 | 8 | 36 | NA | 6 | Distant Lymph Nodes = 13, Lung = 21, Liver = 33, Bone = 2, Peritoneum = 16 | 1 = 27 2 = 20 | 6 | |||
| Non-randomized clinical trials on relapsed/refractory patients | |||||||||||||||
| Hong et al., 2016 [15] | NCT01787500 | Phase IB | Cetuximab and Irinotecan with escalating doses of Vemurafenib | 19 | 63 | 10 | 9 | 0 = 4 1 = 14 | NA | 1 | 18 | NA | NA | Median = 2, 14 = Irinotecan, 8 = Cetuximab, 1 = BRAF | 3 |
| Klute et al., 2022 [18] | NA | Phase II | Cobimetinib + Vemurafenib | 30 | 62 | 11 | 19 | 0 = 12 1 = 13 | 10 | 15 | NA | NA | NA | Radiation = 7 Systemic = 7 | 1 |
| Wang et al., 2022 [3] | NCT03727763 | Phase II | Vemurafenib + Cetuximab + FOLFIRI | 21 | 49 | 13 | 8 | 0 = 4 1 = 7 | 4 | 11 | NA | 6 | Liver = 5, Lung = 5, Distant Lymph Nodes = 8, Abdominopelvic Cavity = 11, Other = 4 | 1 = 12, 2 = 8, 3 = 1 | NA |
| Yaeger et al., 2015 [17] | NA | Pilot Trial | Vemurafenib + Panitumumab | 15 | 62 | 7 | 8 | 0 = 4 1 = 11 | 4 | 10 | NA | NA | NA | 1 = 7, 2 = 8 | NA |
| Kopetz et al., 2015 [13] | NCT00405587 | Phase II Pilot | Vemurafenib as Single Agent | 21 | 65 | 11 | 10 | 0 = 11 1 = 10 | NA | NA | 20 | 1 | NA | 0 = 1, 1 = 1 2+ = 17 | NA |
| Corcoran et al., 2018 [19] | NCT01750918 | Phase I | Dabrafenib + Panitumomab | 20 | 58 | 9 | 11 | 0 = 13 1 = 7 | 4 | 14 | 18 | 2 | NA | 0 = 4, 1 = 8, 2+ = 8 | NA |
| Trametinib + Panitumomab | 31 | 57 | 13 | 18 | 0 = 17 1 = 14 | 10 | 16 | 26 | 5 | NA | 0 = 1, 1 = 14, 2+ = 16 | NA | |||
| Dabrafenib + Trametinib + Panitumomab | 91 | 60 | 33 | 58 | 0 = 47 1 = 44 | 19 | 57 | 76 | 15 | NA | 0 = 21, 1 = 27, 2+ = 43 | 11 | |||
| Morris et al., 2022 [16] | NCT04017650 | Phase I/II | Encorafenib, Cetuximab, and Nivolumab | 26 | 59 | 12 | 14 | NA | NA | NA | NA | NA | NA | NA | NA |
| Van Geel et al., 2017 [14] | NCT01719380 | Phase IB | Encorafenib + Cetuximab | 26 | 63 | 11 | 15 | 0 = 8 1 = 16 | NA | NA | 24 | 2 | Liver = 15, Peritoneum = 5 | 1 = 7, 2+ = 19 | NA |
| Encorafenib + Cetuximab + Alpelisib | 28 | 59 | 10 | 18 | 0 = 18 1 = 10 | NA | NA | 25 | 3 | Liver = 16, Peritoneum = 8 | 1 = 10, 2+ = 18 | NA | |||
| Non-randomized clinical trial on newly diagnosed patients | |||||||||||||||
| Van Cutsem et al., 2023 [20] | NCT03693170 | Phase II | Encorafenib + Binimetinib + Cetuximab | 95 | 65 | 44 | 51 | 0 = 43, 1 = 52 | 37 | 57 | NA | NA | Peritoneal = 46, Liver = 52, Lung = 35 | 19% Received Prior Adjuvant Systemic Treatment | NA |
| Author | Regimen | Median OS | Median PFS | ORR | CR | PR | PD | SD |
|---|---|---|---|---|---|---|---|---|
| Randomized clinical trials on relapsed/refractory patients | ||||||||
| S. Kopetz et al., 2019 [11] | Encorafenib + Binimetinib + Cetuximab | 9.0 months | 4.3 months | 29/111 (26%) | 4/111 (4%) | 25/111 (23%) | 11/111 (10%) | 47/111 (42%) |
| Encorafenib + Cetuximab | 8.4 months | 4.2 months | 23/113 (20%) | 6/113 (5%) | 17/113 (15%) | 8/113 (7%) | 61/113 (54%) | |
| Cetuximab and Irinotecan OR Cetuximab and FOLFIRI | 5.4 months | 1.5 months | 2/107 (2%) | 0/107 | 2/107 (2%) | 36/107 (34%) | 31/107 (29%) | |
| Kopetz et al., 2021 [12] | Cetuximab + Irinotecan | 5.9 months | 2 months | 2 (4%) | NA | NA | 38/50 (76%) | NA |
| Vemurafenib + Cetuximab + Irinotecan | 9.6 months | 4.2 months | 8 (17%) | NA | NA | 31/50 (62%) | NA | |
| Non-randomized clinical trials on relapsed/refractory patients | ||||||||
| Hong D.S., et al., 2016 [15] | Cetuximab and Irinotecan with escalating doses of Vemurafenib | NA | 7.7 months | 6/17 (35%) | 0 | 6/17 (35%) | 2/17 (12%) | 9/17 (53%) |
| Klute K. A. et al., 2022 [18] | Cobimetinib + Vemurafenib | 8.95 months | 3.6 months | 8/27 (30%) | 0 | 8/27 (30%) | NA | 6/27 (22%) |
| Wang, Z. et al., 2022 [3] | Vemurafenib + Cetuximab + FOLFIRI | 15.4 months | 9.7 months | 17/21 (81%) | 2/21 (9.5%) | 15/21 (71%) | 10/21 (47%) | 3/21 (14%) |
| Yaeger, R. et al., 2015 [17] | Vemurafenib + Panitumumab | 7.6 months | 3.2 months | 2/15 (13%) | 0 | 2/15 (13%) | 2/15 (13%) | 2/15 (13%) |
| Kopetz et al., 2015 [13] | Vemurafenib as Single Agent | 7.7 months | 2.1 months | 1/21 (5%) | 0 | 1/21 (5%) | NA | 7/21 (33%) |
| Corcoran et al., 2018 [19] | Dabrafenib + Panitumomab | 13.2 months | 3.5 months | 2/31 (10%) | 1/31 (5%) | 1/31 (5%) | 2/31 (10%) | 16 (80%) |
| Trametinib + Panitumomab | 8.2 months | 2.6 months | 0 | 0 | 0 | 12/31 (39%) | 17/31 (55%) | |
| Dabrafenib + Trametinib + Panitumomab | 9.1 months | 4.2 months | 19/91 (21%) | 1/91 (1%) | 18/91 (20%) | 8/91 (9%) | 59/91 (65%) | |
| Morris et al., 2022 [16] | Encorafenib, Cetuximab, and Nivolumab | 11.4 months | 7.3 months | 12/26 (45%) | NA | NA | NA | NA |
| Van Geel R. et al., 2017 [14] | Encorafenib + Cetuximab | NA | 3.7 months | 5/26 (19%) | 1/26 (4%) | 4/26 (15.5%) | 4/26 (15.5%) | 15/26 (58%) |
| Encorafenib + Cetuximab + Alpelisib | NA | 4.2 months | 5/28 (18%) | 0 | 5/28 (18%) | 1/28 (3.6%) | 21/28 (75%) | |
| Non-randomized clinical trial on newly diagnosed patients | ||||||||
| Van Cutsem et al., 2023 [20] | Encorafenib + Binimetinib + Cetuximab | 18.3 months | 5.8 months | 45/95 (47%) | 0 | 45/95 (47%) | 48/95 (50%) | 37/95 (41%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aiman, W.; Ali, M.A.; Jumean, S.; Asfeen, U.; Garcia, J.; Quirem, M.; Ahmad, A.; Rayad, M.N.; Alkhlaifat, O.; Al Omour, B.; et al. BRAF Inhibitors in BRAF-Mutated Colorectal Cancer: A Systematic Review. J. Clin. Med. 2024, 13, 113. https://doi.org/10.3390/jcm13010113
Aiman W, Ali MA, Jumean S, Asfeen U, Garcia J, Quirem M, Ahmad A, Rayad MN, Alkhlaifat O, Al Omour B, et al. BRAF Inhibitors in BRAF-Mutated Colorectal Cancer: A Systematic Review. Journal of Clinical Medicine. 2024; 13(1):113. https://doi.org/10.3390/jcm13010113
Chicago/Turabian StyleAiman, Wajeeha, Muhammad Ashar Ali, Samer Jumean, Ummul Asfeen, Jose Garcia, Murad Quirem, Amaar Ahmad, Mohammad Nabil Rayad, Osama Alkhlaifat, Bader Al Omour, and et al. 2024. "BRAF Inhibitors in BRAF-Mutated Colorectal Cancer: A Systematic Review" Journal of Clinical Medicine 13, no. 1: 113. https://doi.org/10.3390/jcm13010113
APA StyleAiman, W., Ali, M. A., Jumean, S., Asfeen, U., Garcia, J., Quirem, M., Ahmad, A., Rayad, M. N., Alkhlaifat, O., Al Omour, B., Chemarthi, V. S., Maroules, M., Guron, G., & Shaaban, H. (2024). BRAF Inhibitors in BRAF-Mutated Colorectal Cancer: A Systematic Review. Journal of Clinical Medicine, 13(1), 113. https://doi.org/10.3390/jcm13010113