


The Postoperative Effect of Sugammadex versus Acetylcholinesterase Inhibitors in Colorectal Surgery: An Updated Meta-Analysis



Abstract
:1. Introduction
2. Material and Methods
2.1. Eligibility Criteria and Group Definition
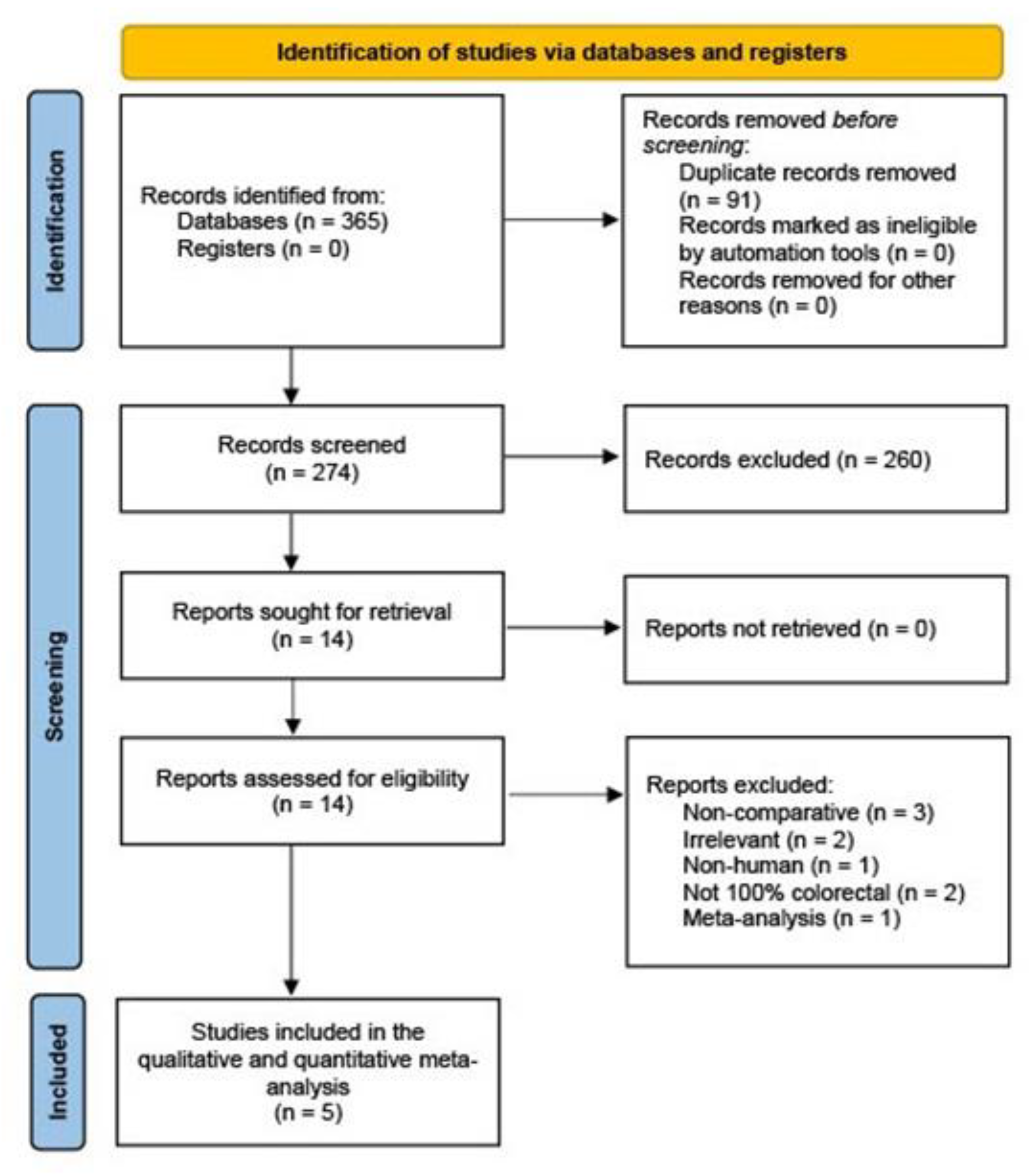
2.2. Literature Search
2.3. Data Extraction and Outcome Measures
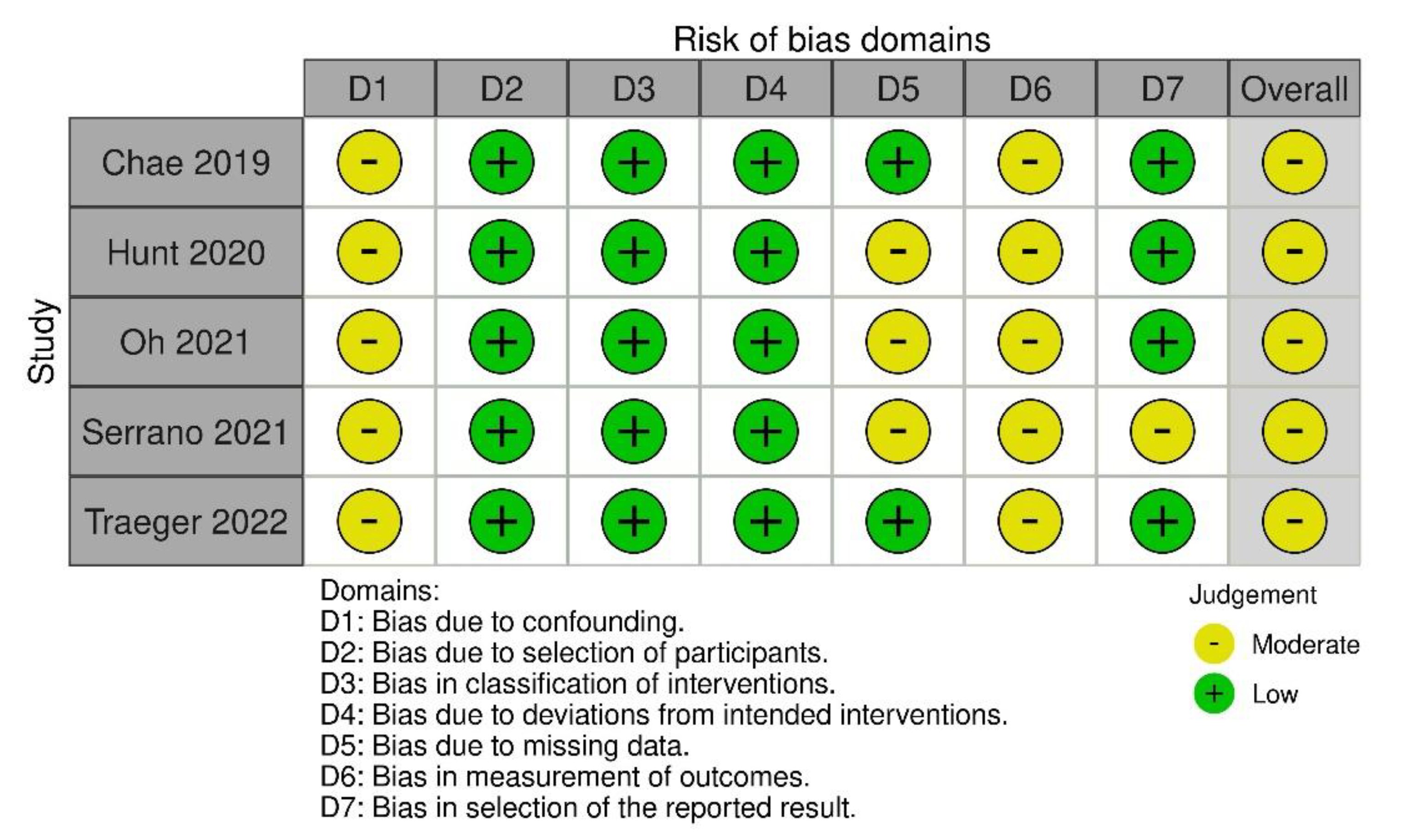
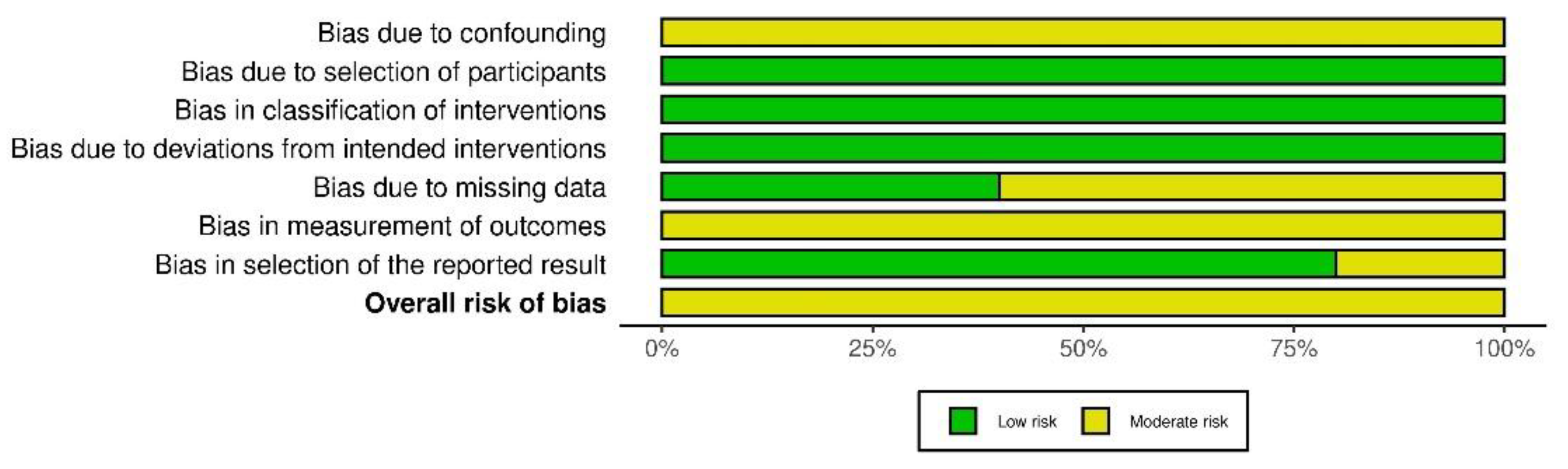
2.4. Quality Assessment
2.5. Statistical Analyses
3. Results
3.1. Study and Patient Characteristics
3.2. Study Quality and Risk of Bias
3.3. Gastrointestinal Motility Outcomes
3.3.1. Time to First Bowel Movement or Flatus
3.3.2. Time to First Oral Diet Intake
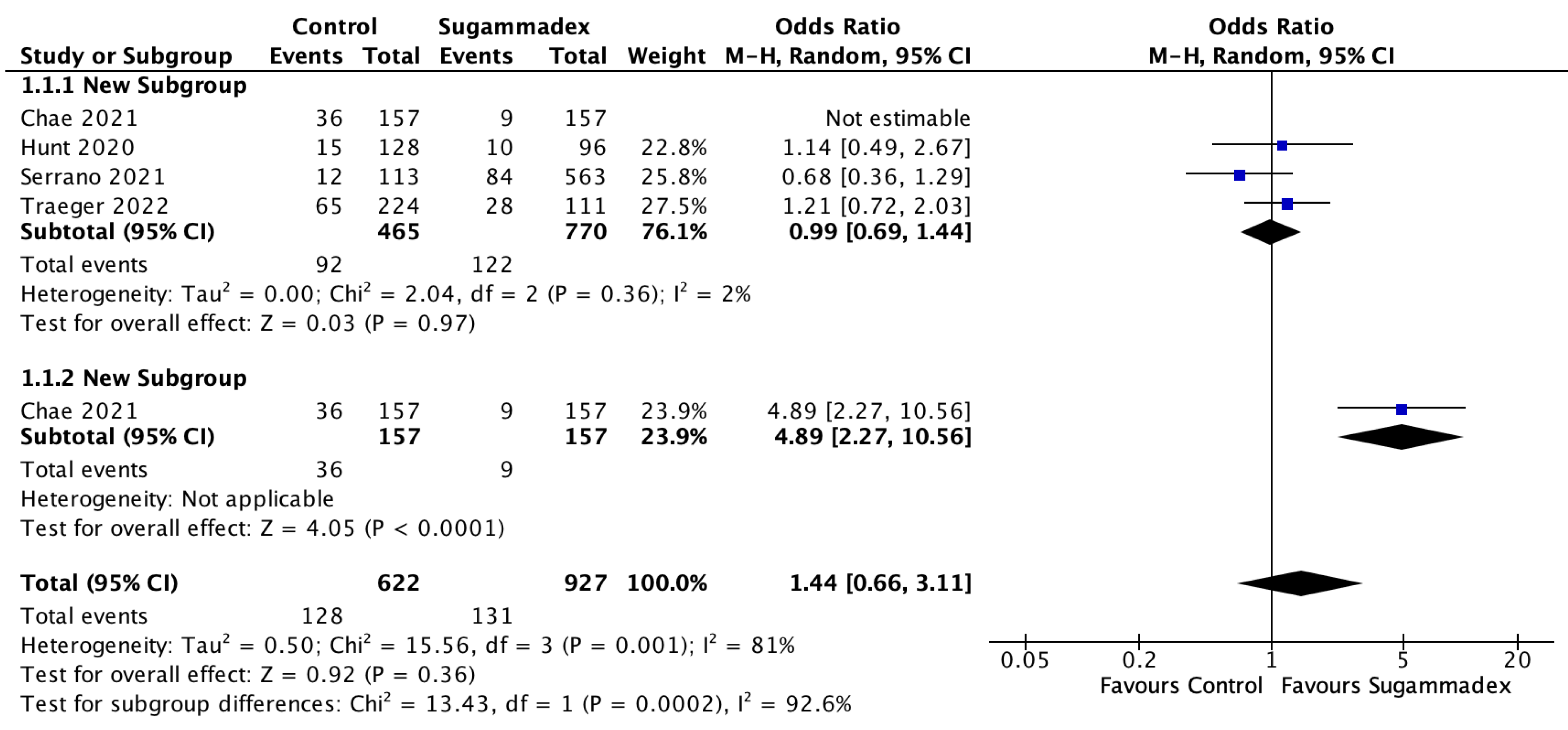
3.3.3. Ileus
3.4. Non-Gastrointestinal Motility Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Senagore, A.J. Pathogenesis and Clinical and Economic Consequences of Postoperative Ileus. Am. J. Health Syst. Pharm. 2007, 64, S3–S7. [Google Scholar] [CrossRef] [PubMed]
- Tevis, S.E.; Carchman, E.H.; Foley, E.F.; Harms, B.A.; Heise, C.P.; Kennedy, G.D. Postoperative Ileus–More than Just Prolonged Length of Stay? J. Gastrointest. Surg. 2015, 19, 1684–1690. [Google Scholar] [CrossRef] [PubMed]
- Venara, A.; Meillat, H.; Cotte, E.; Ouaissi, M.; Duchalais, E.; Mor-Martinez, C.; Wolthuis, A.; Regimbeau, J.M.; Ostermann, S.; Hamel, J.F.; et al. Incidence and Risk Factors for Severity of Postoperative Ileus After Colorectal Surgery: A Prospective Registry Data Analysis. World J. Surg. 2020, 44, 957–966. [Google Scholar] [CrossRef] [PubMed]
- Dai, X.; Ge, X.; Yang, J.; Zhang, T.; Xie, T.; Gao, W.; Gong, J.; Zhu, W. Increased Incidence of Prolonged Ileus after Colectomy for Inflammatory Bowel Diseases under ERAS Protocol: A Cohort Analysis. J. Surg. Res. 2017, 212, 86–93. [Google Scholar] [CrossRef]
- Brusasco, C.; Germinale, F.; Dotta, F.; Benelli, A.; Guano, G.; Campodonico, F.; Ennas, M.; Di Domenico, A.; Santori, G.; Introini, C.; et al. Low Intra-Abdominal Pressure with Complete Neuromuscular Blockage Reduces Post-Operative Complications in Major Laparoscopic Urologic Surgery: A before-after Study. J. Clin. Med. 2022, 11, 7201. [Google Scholar] [CrossRef]
- Lowen, D.J.; Hodgson, R.; Tacey, M.; Barclay, K.L. Does Deep Neuromuscular Blockade Provide Improved Outcomes in Low Pressure Laparoscopic Colorectal Surgery? A Single Blinded Randomized Pilot Study. ANZ J. Surg. 2022, 92, 1447–1453. [Google Scholar] [CrossRef]
- Alday, E.; Muñoz, M.; Planas, A.; Mata, E.; Alvarez, C. Effects of Neuromuscular Block Reversal with Sugammadex versus Neostigmine on Postoperative Respiratory Outcomes after Major Abdominal Surgery: A Randomized-Controlled Trial. Can. J. Anaesth. 2019, 66, 1328–1337. [Google Scholar] [CrossRef]
- Murphy, G.S.; Szokol, J.W.; Avram, M.J.; Greenberg, S.B.; Shear, T.; Vender, J.S.; Gray, J.; Landry, E. Postoperative Residual Neuromuscular Blockade Is Associated with Impaired Clinical Recovery. Anesth. Analg. 2013, 117, 133–141. [Google Scholar] [CrossRef]
- Colović, M.B.; Krstić, D.Z.; Lazarević-Pašti, T.D.; Bondžić, A.M.; Vasić, V.M. Acetylcholinesterase Inhibitors: Pharmacology and Toxicology. Curr. Neuropharmacol. 2013, 11, 315–335. [Google Scholar] [CrossRef]
- Mirakhur, R.K.; Briggs, L.P.; Clarke, R.S.; Dundee, J.W.; Johnston, H.M. Comparison of Atropine and Glycopyrrolate in a Mixture with Pyridostigmine for the Antagonism of Neuromuscular Block. Br. J. Anaesth. 1981, 53, 1315–1320. [Google Scholar] [CrossRef]
- Keating, G.M. Sugammadex: A Review of Neuromuscular Blockade Reversal. Drugs 2016, 76, 1041–1052. [Google Scholar] [CrossRef] [PubMed]
- Hristovska, A.-M.; Duch, P.; Allingstrup, M.; Afshari, A. Efficacy and Safety of Sugammadex versus Neostigmine in Reversing Neuromuscular Blockade in Adults. Cochrane Database Syst. Rev. 2017, 8, CD012763. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.K. Limited Advantage of Sugammadex Reversal over the Traditional Neuromuscular Reversal Technique in Terms of Postoperative Recovery of Bowel Function. Korean J. Anesthesiol. 2020, 73, 87–88. [Google Scholar] [CrossRef] [PubMed]
- Traeger, L.; Kroon, H.M.; Bedrikovetski, S.; Moore, J.W.; Sammour, T. The Impact of Acetylcholinesterase Inhibitors on Ileus and Gut Motility Following Abdominal Surgery: A Clinical Review. ANZ J. Surg. 2022, 92, 69–76. [Google Scholar] [CrossRef]
- Chapman, S.J.; Thorpe, G.; Vallance, A.E.; Harji, D.P.; Lee, M.J.; Fearnhead, N.S. Association of Coloproctology of Great Britain and Ireland Gastrointestinal Recovery Group Systematic Review of Definitions and Outcome Measures for Return of Bowel Function after Gastrointestinal Surgery. BJS Open 2019, 3, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. PRISMA Group Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed]
- Cochrane Handbook for Systematic Reviews of Interventions. Available online: https://training.cochrane.org/handbook (accessed on 2 February 2023).
- Sterne, J.A.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A Tool for Assessing Risk of Bias in Non-Randomised Studies of Interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef]
- Guyatt, G.H.; Oxman, A.D.; Kunz, R.; Woodcock, J.; Brozek, J.; Helfand, M.; Alonso-Coello, P.; Glasziou, P.; Jaeschke, R.; Akl, E.A.; et al. GRADE Guidelines: 7. Rating the Quality of Evidence–Inconsistency. J. Clin. Epidemiol. 2011, 64, 1294–1302. [Google Scholar] [CrossRef]
- Malmivaara, A. Methodological Considerations of the GRADE Method. Ann. Med. 2015, 47, 1–5. [Google Scholar] [CrossRef]
- Luo, D.; Wan, X.; Liu, J.; Tong, T. Optimally Estimating the Sample Mean from the Sample Size, Median, Mid-Range, and/or Mid-Quartile Range. Stat. Methods Med. Res. 2018, 27, 1785–1805. [Google Scholar] [CrossRef]
- Wan, X.; Wang, W.; Liu, J.; Tong, T. Estimating the Sample Mean and Standard Deviation from the Sample Size, Median, Range and/or Interquartile Range. BMC Med. Res. Methodol. 2014, 14, 135. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring Inconsistency in Meta-Analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [PubMed]
- Chae, Y.J.; Joe, H.B.; Oh, J.; Lee, E.; Yi, I.K. Thirty-Day Postoperative Outcomes Following Sugammadex Use in Colorectal Surgery Patients; Retrospective Study. J. Clin. Med. 2019, 8, 97. [Google Scholar] [CrossRef] [PubMed]
- Hunt, M.E.; Yates, J.R.; Vega, H.; Heidel, R.E.; Buehler, J.M. Effects on Postoperative Gastrointestinal Motility After Neuromuscular Blockade Reversal With Sugammadex Versus Neostigmine/Glycopyrrolate in Colorectal Surgery Patients. Ann. Pharmacother. 2020, 54, 1165–1174. [Google Scholar] [CrossRef] [PubMed]
- Oh, C.; Jo, Y.; Sim, S.; Yun, S.; Jeon, S.; Chung, W.; Yoon, S.-H.; Lim, C.; Hong, B. Post-Operative Respiratory Outcomes Associated with the Use of Sugammadex in Laparoscopic Colorectal Cancer Surgery: A Retrospective, Propensity Score Matched Cohort Study. Available online: https://www.signavitae.com/articles/10.22514/sv.2020.16.0116#CiteAndShare (accessed on 2 February 2023).
- Serrano, A.B.; DÍaz-Cambronero, Ó.; Melchor-RipollÉs, J.; Abad-Gurumeta, A.; Ramirez-Rodriguez, J.M.; MartÍnez-Ubieto, J.; SÁnchez-Merchante, M.; Rodriguez, R.; JordÁ, L.; Gil-Trujillo, S.; et al. Neuromuscular Blockade Management and Postoperative Outcomes in Enhanced Recovery Colorectal Surgery: Secondary Analysis of POWER Trial. Minerva Anestesiol. 2021, 87, 13–25. [Google Scholar] [CrossRef] [PubMed]
- Traeger, L.; Hall, T.D.; Bedrikovetski, S.; Kroon, H.M.; Dudi-Venkata, N.N.; Moore, J.W.; Sammour, T. Effect of Neuromuscular Reversal with Neostigmine/Glycopyrrolate versus Sugammadex on Postoperative Ileus Following Colorectal Surgery. Tech. Coloproctol. 2022, 27, 217–226. [Google Scholar] [CrossRef]
- Ripollés-Melchor, J.; Ramírez-Rodríguez, J.M.; Casans-Francés, R.; Aldecoa, C.; Abad-Motos, A.; Logroño-Egea, M.; García-Erce, J.A.; Camps-Cervantes, Á.; Ferrando-Ortolá, C.; Suarez de la Rica, A.; et al. Association between Use of Enhanced Recovery After Surgery Protocol and Postoperative Complications in Colorectal Surgery: The Postoperative Outcomes Within Enhanced Recovery After Surgery Protocol (POWER) Study. JAMA Surg. 2019, 154, 725–736. [Google Scholar] [CrossRef]
- Gustafsson, U.O.; Scott, M.J.; Hubner, M.; Nygren, J.; Demartines, N.; Francis, N.; Rockall, T.A.; Young-Fadok, T.M.; Hill, A.G.; Soop, M.; et al. Guidelines for Perioperative Care in Elective Colorectal Surgery: Enhanced Recovery After Surgery (ERAS®) Society Recommendations: 2018. World J. Surg. 2019, 43, 659–695. [Google Scholar] [CrossRef]
- Greco, M.; Capretti, G.; Beretta, L.; Gemma, M.; Pecorelli, N.; Braga, M. Enhanced Recovery Program in Colorectal Surgery: A Meta-Analysis of Randomized Controlled Trials. World J. Surg. 2014, 38, 1531–1541. [Google Scholar] [CrossRef]
- Nag, K.; Singh, D.R.; Shetti, A.N.; Kumar, H.; Sivashanmugam, T.; Parthasarathy, S. Sugammadex: A Revolutionary Drug in Neuromuscular Pharmacology. Anesth. Essays Res. 2013, 7, 302–306. [Google Scholar] [CrossRef]
- Sen, A.; Erdivanli, B.; Tomak, Y.; Pergel, A. Reversal of Neuromuscular Blockade with Sugammadex or Neostigmine/Atropine: Effect on Postoperative Gastrointestinal Motility. J. Clin. Anesth. 2016, 32, 208–213. [Google Scholar] [CrossRef] [PubMed]
- Deljou, A.; Schroeder, D.R.; Ballinger, B.A.; Sprung, J.; Weingarten, T.N. Effects of Sugammadex on Time of First Postoperative Bowel Movement: A Retrospective Analysis. Mayo Clin. Proc. Innov. Qual. Outcomes 2019, 3, 294–301. [Google Scholar] [CrossRef] [PubMed]
- Cho, H.-Y.; Kim, H.; Yoon, S.; Lee, H.-J.; Kim, H.; Lee, H.-C.; Kim, W.-H.; Jang, J.-Y. Effect of Sugammadex on the Recovery of Gastrointestinal Motility after Open Pancreaticoduodenectomy: A Single-Center Retrospective Study. Minerva Anestesiol. 2021, 87, 1100–1108. [Google Scholar] [CrossRef] [PubMed]
- An, J.; Noh, H.; Kim, E.; Lee, J.; Woo, K.; Kim, H. Neuromuscular Blockade Reversal with Sugammadex versus Pyridostigmine/Glycopyrrolate in Laparoscopic Cholecystectomy: A Randomized Trial of Effects on Postoperative Gastrointestinal Motility. Korean J. Anesthesiol. 2020, 73, 137–144. [Google Scholar] [CrossRef] [PubMed]
- Claroni, C.; Covotta, M.; Torregiani, G.; Marcelli, M.E.; Tuderti, G.; Simone, G.; Scotto di Uccio, A.; Zinilli, A.; Forastiere, E. Recovery from Anesthesia after Robotic-Assisted Radical Cystectomy: Two Different Reversals of Neuromuscular Blockade. J. Clin. Med. 2019, 8, 1774. [Google Scholar] [CrossRef]
- Bragg, D.; El-Sharkawy, A.M.; Psaltis, E.; Maxwell-Armstrong, C.A.; Lobo, D.N. Postoperative Ileus: Recent Developments in Pathophysiology and Management. Clin. Nutr. 2015, 34, 367–376. [Google Scholar] [CrossRef]
- Seo, S.H.B.; Carson, D.A.; Bhat, S.; Varghese, C.; Wells, C.I.; Bissett, I.P.; O’Grady, G. Prolonged Postoperative Ileus Following Right- versus Left-Sided Colectomy: A Systematic Review and Meta-Analysis. Color. Dis. 2021, 23, 3113–3122. [Google Scholar] [CrossRef]
- Kheterpal, S.; Vaughn, M.T.; Dubovoy, T.Z.; Shah, N.J.; Bash, L.D.; Colquhoun, D.A.; Shanks, A.M.; Mathis, M.R.; Soto, R.G.; Bardia, A.; et al. Sugammadex versus Neostigmine for Reversal of Neuromuscular Blockade and Postoperative Pulmonary Complications (STRONGER): A Multicenter Matched Cohort Analysis. Anesthesiology 2020, 132, 1371–1381. [Google Scholar] [CrossRef]
- Chen, A.T.; Patel, A.; McKechnie, T.; Lee, Y.; Doumouras, A.G.; Hong, D.; Eskicioglu, C. Sugammadex in Colorectal Surgery: A Systematic Review and Meta-Analysis. J. Surg. Res. 2022, 270, 221–229. [Google Scholar] [CrossRef]
- Piccioni, F.; Mariani, L.; Bogno, L.; Rivetti, I.; Tramontano, G.T.A.; Carbonara, M.; Ammatuna, M.; Langer, M. An Acceleromyographic Train-of-Four Ratio of 1.0 Reliably Excludes Respiratory Muscle Weakness after Major Abdominal Surgery: A Randomized Double-Blind Study. Can. J. Anaesth. 2014, 61, 641–649. [Google Scholar] [CrossRef]
- Wachtendorf, L.J.; Tartler, T.M.; Ahrens, E.; Witt, A.S.; Azimaraghi, O.; Fassbender, P.; Suleiman, A.; Linhardt, F.C.; Blank, M.; Nabel, S.Y.; et al. Comparison of the Effects of Sugammadex versus Neostigmine for Reversal of Neuromuscular Block on Hospital Costs of Care. Br. J. Anaesth. 2023, 130, 133–141. [Google Scholar] [CrossRef] [PubMed]
- Ren, M.; Wang, Y.; Luo, Y.; Fang, J.; Lu, Y.; Xuan, J. Economic Analysis of Sugammadex versus Neostigmine for Reversal of Neuromuscular Blockade for Laparoscopic Surgery in China. Health Econ. Rev. 2020, 10, 35. [Google Scholar] [CrossRef] [PubMed]
- Carron, M.; Baratto, F.; Zarantonello, F.; Ori, C. Sugammadex for Reversal of Neuromuscular Blockade: A Retrospective Analysis of Clinical Outcomes and Cost-Effectiveness in a Single Center. Clinicoecon. Outcomes Res. 2016, 8, 43–52. [Google Scholar] [CrossRef] [PubMed]
- Lan, W.; Tam, K.-W.; Chen, J.-T.; Cata, J.P.; Cherng, Y.-G.; Chou, Y.-Y.; Chien, L.-N.; Chang, C.-L.; Tai, Y.-H.; Chu, L.-M. Cost-Effectiveness of Sugammadex Versus Neostigmine to Reverse Neuromuscular Blockade in a University Hospital in Taiwan: A Propensity Score-Matched Analysis. Healthcare 2023, 11, 240. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author | Year | Origin | Study Design | Recruitment Period | Sample Size | Exclusion Criteria | Colorectal Cases (%) | Reversal agents | Follow-Up Period | Primary Outcome |
|---|---|---|---|---|---|---|---|---|---|---|
| Chae et al. [24] | 2019 | Republic of Korea | Single-center, retrospective | 2012–2017 | 314 | Age < 21 years, neuromuscular disease, impaired hepatic and renal function, combined or emergency procedures, non-malignant disease | 314 (100) | Sugammadex vs. Pyridostigmine | 30 days | Total and postoperative length of hospital stay; delayed discharge rate and readmission rate |
| Hunt et al. [25] | 2020 | USA | Single-center, retrospective | 2014–2017 | 224 | Age < 18 years, preoperative renal or hepatic failure, bowel obstruction, conversion laparotomy, postoperative mechanical ventilation, emergency surgery, ASA class > III, combination of sugammadex and neostigmine, glycopyrrolate use with sugammadex but without neostigmine, epidural anesthesia, bowel obstruction, open surgery, no documented postoperative bowel movement | 224 (100) | Sugammadex vs. Neostigmine/Glycopyrrolate | In hospital | Time to first bowel movement (in hours) after reversal |
| Oh et al. [26] | 2021 | Republic of Korea | Single-center, retrospective | 2014–2018 | 420 | Robotic surgery, combined surgeries, non-malignant disease, direct postoperative ICU transfer, incomplete medical records, neuromuscular blockade other than rocuronium, deep neuromuscular blockade | 420 (100) | Sugammadex vs. Pyridostigmine | In hospital | Postoperative respiratory adverse events |
| Serrano et al. [27] | 2021 | Spain | Multi-center, prospective (sub-study of POWER trial) | 2017 | 676 | Age < 18 years, emergency surgery, non-ERAS adherence | 676 (100) | Sugammadex vs. Neostigmine | 30 days | Moderate–severe postoperative complications, length of hospital stay |
| Traeger et al. [28] | 2022 | Australia | Single-center, retrospective | 2019–2021 | 335 | Age < 18 years, pelvic exenteration, robotic surgery, no reversal agent, combination of sugammadex and neostigmine, pyridostigmine prescription | 335 (100) | Sugammadex vs. Neostigmine/Glycopyrrolate | 30 days | Gastrointestinal recovery (GI-2): time of first bowel movement and tolerance of solid diet |
| Author | Reversal Agent | No. of Patients | Age (Years) | Sex (Male/Female) | BMI (kg/m2) | ASA Class (%) | Diabetes Mellitus (%) | Smoking History (%) | Cardiac Disease (%) | Pulmonary Disease (%) | Arterial Hypertension (%) |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Chae et al. [24] | Sugammadex | 157 | 62.5 ± 11.5 * | 86/71 | 23.8 ± 3.3 * | ASA I 67 (43) ASA II 90 (57) | 30 (19) | NS | 76 (48) | 6 (4) | NS |
| Pyridostigmine | 157 | 63.1 ± 11.8 | 83/74 | 23.4 ± 3.4 | ASA I 77 (49) ASA II 80 (51) | 26 (17) | NS | 70 (45) | 2 (1) | NS | |
| Hunt et al. [25] | Sugammadex | 96 | 60.68 (14.64) * | 36/60 | 29.3 (6.09) * | ASA I-III 96 (100) | NS | 16 (16.7) | NS | NS | NS |
| Neostigmine/ Glycopyrrolate | 128 | 60.34 (14.08) | 58/70 | 29.6 (6.19) | ASA I-III 128 (100) | NS | 36 (28.1) | NS | NS | NS | |
| Oh et al. [26] | Sugammadex | 210 | 68.0 [61.0;75.0] # | 129/81 | 24.0 ± 3.3 * | ASA III-IV 32 (15.2) | NS | 49 (23.3) | NS | 27 (12.9) | NS |
| Pyridostigmine | 210 | 68.0 [60.0;74.0] | 133/77 | 24.2 ± 3.4 | ASA III-IV 28 (13.3) | NS | 45 (21.4) | NS | 21 (10.0) | NS | |
| Serrano et al. [27] | All patients | All patients | All patients | All patients | All patients | All patients | All patients | All patients | All patients | ||
| Sugammadex | 563 | 67.9 (12.8) * | 398/278 | 27.0 (4.7) * | ASA I 54 (8.0) ASA II 360 (53.3) ASA III 245 (36.2) ASA IV 17 (2.5) | 141 (20.9) | 126 (18.6) | 108 (15.9) | 104 (15.4) | 348 (51.5) | |
| Neostigmine | 113 | ||||||||||
| Traeger et al. [28] | Sugammadex | 111 | 67 (57–76 [18–94]) † | 62/49 | 28.7 (24.7–32.9 [18.2–73.0]) † | ASA I 3 (2.7) ASA II 41 (36.9) ASA III 62 (55.9) ASA IV 5 (4.5) | 26 (23.4) | 57 (51.4) | 4 (3.6) | 17 (15.3) | 63 (56.8) |
| Neostigmine/ Glycopyrrolate | 224 | 64 (53–72 [19–90]) | 129/95 | 26.8 (23.4–30.4 [15.9–58.8]) | ASA I 5 (2.2) ASA II 118 (52.7) ASA III 101 (45.1) ASA IV 0 (0) | 39 (17.4) | 112 (50) | 7 (3.1) | 15 (6.7) | 93 (41.5) |
| Author | Reversal Agent | NMBA | Anesthesia Time (min) | Laparoscopic Approach (%) | Cancer Surgery (%) |
|---|---|---|---|---|---|
| Chae et al. [24] | Sugammadex | Rocuronium | 176.0 ± 46.7 * | 32 (20) | 157 (100) |
| Pyridostigmine | Rocuronium | 175.1 ± 41.0 | 34 (22) | 157 (100) | |
| Hunt et al. [25] | Sugammadex | Rocuronium or Vercuronium | 229.8 (166.2) # | 96 (100) | 52 (54.2) |
| Neostigmine/ Glycopyrrolate | Rocuronium or Vercuronium | 214.2 (127.8) | 128 (100) | 67 (52.3) | |
| Oh et al. [26] | Sugammadex | Rocuronium | 202.5 [177.0; 240.0] # | 210 (100) | 210 (100) |
| Pyridostigmine | Rocuronium | 201.5 [170.0; 238.0] | 210 (100) | 210 (100) | |
| Serrano et al. [27] | All patients | All patients | All patients | All patients | |
| Sugammadex | NS | NS | 471 (69.7) | NS | |
| Neostigmine | |||||
| Traeger et al. [28] | Sugammadex | NS | 170 (120–215 [29–443]) † | 74 (66.7) | 73 (65.8) |
| Neostigmine/ Glycopyrrolate | NS | 157 (110–194 [42–378]) | 111 (50.9) | 123 (54.9) |
| Outcomes | No. of Studies | No. of Included Patients | SMD/OR [95% CI] | Quality Assessment | Quality | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| Sugammadex | Control | Risk of Bias a | Inconsistency | Indirectness | Imprecision | Publication Bias | ||||
| Time to first postoperative bowel movement or flatus | 2 [25,28] | 207 | 352 | SMD 13.01 [6.55–19.46] | Serious (−1) | Serious (−1) | No indirectness | No imprecision | NA | Very low |
| Heterogeneity Level | ||||||
|---|---|---|---|---|---|---|
| Outcomes | No. of Included Studies | No. of Included Patients | SMD/OR [95% CI] | p-Value | I2 (%) | p-Value |
| Urinary tract infection | 2 [24,27] | 990 | 0.37 [0.07–2.04] | 0.25 | 0 | 0.63 |
| Pulmonary morbidity | 3 [24,26,27] | 1410 | 0.77 [0.46–1.29] | 0.32 | 0 | 0.41 |
| PONV | 2 [25,26] | 644 | 0.91 [0.59–1.41] | 0.67 | 0 | 0.59 |
| Length of postoperative hospital stay | 4 [24,25,26,28] | 1293 | −0.03 [−0.27–0.21] | 0.80 | 0 | 0.87 |
| Anastomotic leak | 2 [27,28] | 970 | 1.11 [0.31–3.94] | 0.87 | 61 | 0.11 |
| Bleeding | 2 [24,27] | 990 | 0.76 [0.24–2.43] | 0.64 | 3 | 0.31 |
| Surgical site infection | 2 [24,27] | 990 | 0.65 [0.40–1.07] | 0.09 | 0 | 0.74 |
| PACU stay | 2 [24,26] | 734 | −0.95 [−3.04–1.14] | 0.37 | 0 | 0.91 |
| Reoperation | 3 [26,27,28] | 1431 | 0.89 [0.54–1.48] | 0.66 | 0 | 0.73 |
| ICU readmission | 2 [24,28] | 649 | 1.16 [0.44–3.06] | 0.76 | 32 | 0.23 |
| Hospital readmission | 3 [24,27,28] | 1325 | 1.07 [0.68–1.67] | 0.78 | 0 | 0.80 |
| Mortality | 2 [24,27] | 990 | 1.89 [0.19–18.81] | 0.59 | 61 | 0.11 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vaghiri, S.; Prassas, D.; Krieg, S.; Knoefel, W.T.; Krieg, A. The Postoperative Effect of Sugammadex versus Acetylcholinesterase Inhibitors in Colorectal Surgery: An Updated Meta-Analysis. J. Clin. Med. 2023, 12, 3235. https://doi.org/10.3390/jcm12093235
Vaghiri S, Prassas D, Krieg S, Knoefel WT, Krieg A. The Postoperative Effect of Sugammadex versus Acetylcholinesterase Inhibitors in Colorectal Surgery: An Updated Meta-Analysis. Journal of Clinical Medicine. 2023; 12(9):3235. https://doi.org/10.3390/jcm12093235
Chicago/Turabian StyleVaghiri, Sascha, Dimitrios Prassas, Sarah Krieg, Wolfram Trudo Knoefel, and Andreas Krieg. 2023. "The Postoperative Effect of Sugammadex versus Acetylcholinesterase Inhibitors in Colorectal Surgery: An Updated Meta-Analysis" Journal of Clinical Medicine 12, no. 9: 3235. https://doi.org/10.3390/jcm12093235
APA StyleVaghiri, S., Prassas, D., Krieg, S., Knoefel, W. T., & Krieg, A. (2023). The Postoperative Effect of Sugammadex versus Acetylcholinesterase Inhibitors in Colorectal Surgery: An Updated Meta-Analysis. Journal of Clinical Medicine, 12(9), 3235. https://doi.org/10.3390/jcm12093235