
Predictive Power of Oxygen Desaturation Index (ODI) and Apnea-Hypopnea Index (AHI) in Detecting Long-Term Neurocognitive and Psychosocial Outcomes of Sleep-Disordered Breathing in Children: A Questionnaire-Based Study

 ,
,  , and
, and
Abstract
1. Introduction
2. Materials and Methods
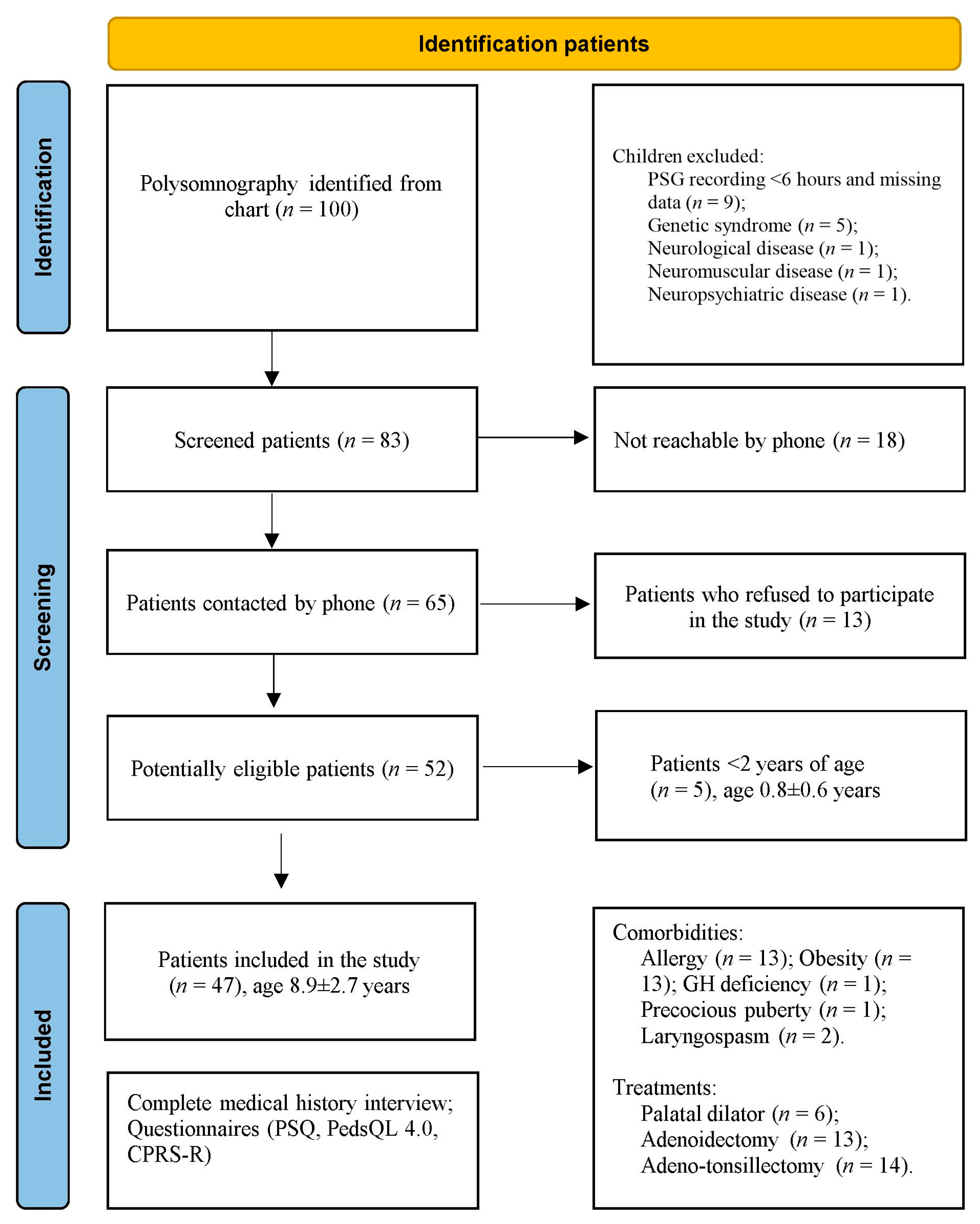
2.1. Study Population
2.2. Anthropometry
2.3. Respiratory Polysomnography
2.4. Telephone Interview
2.5. Questionnaires
2.6. Pediatric Sleep Questionnaire
2.7. Pediatric Quality of Life Inventory
2.8. Conners’ Parent Rating Scales Revised
2.9. Statistics
3. Results
Follow-Up
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gipson, K.; Lu, M.; Kinane, T.B. Sleep-Disordered Breathing in Children. Pediatr. Rev. 2019, 40, 3–13. [Google Scholar] [CrossRef] [PubMed]
- Baker-Smith, C.M.; Isaiah, A.; Melendres, M.C.; Mahgerefteh, J.; Lasso-Pirot, A.; Mayo, S.; Gooding, H.; Zachariah, J.; American Heart Association Athero, Hypertension; Obesity in the Young Committee of the Council on Lifelong Congenital Heart Disease and Heart Health in the Young; et al. Sleep-Disordered Breathing and Cardiovascular Disease in Children and Adolescents: A Scientific Statement From the American Heart Association. J. Am. Heart Assoc. 2021, 10, e022427. [Google Scholar] [CrossRef] [PubMed]
- Torres-Lopez, L.V.; Cadenas-Sanchez, C.; Migueles, J.H.; Esteban-Cornejo, I.; Molina-Garcia, P.; Hillman, C.H.; Catena, A.; Ortega, F.B. Does sleep-disordered breathing add to impairments in academic performance and brain structure usually observed in children with overweight/obesity? Eur. J. Pediatr. 2022, 181, 2055–2065. [Google Scholar] [CrossRef]
- Hunter, S.J.; Gozal, D.; Smith, D.L.; Philby, M.F.; Kaylegian, J.; Kheirandish-Gozal, L. Effect of sleep-disordered breathing severity on cognitive performance measures in a large community cohort of young school-aged children. Am. J. Respir. Crit. Care Med. 2016, 194, 739–747. [Google Scholar] [CrossRef]
- Kaemingk, K.L.; Pasvogel, A.E.; Goodwin, J.L.; Mulvaney, S.A.; Martinez, F.; Enright, P.L.; Rosen, G.M.; Morgan, W.J.; Fregosi, R.F.; Quan, S.F. Learning in children and sleep disordered breathing: Findings of the Tucson Children’s Assessment of Sleep Apnea (tuCASA) prospective cohort study. J. Int. Neuropsychol. Soc. JINS 2003, 9, 1016–1026. [Google Scholar] [CrossRef]
- O’Brien, L.M.; Mervis, C.B.; Holbrook, C.R.; Bruner, J.L.; Smith, N.H.; McNally, N.; McClimment, M.C.; Gozal, D. Neurobehavioral correlates of sleep-disordered breathing in children. J. Sleep Res. 2004, 13, 165–172. [Google Scholar] [CrossRef]
- Isaiah, A.; Shikara, M.; Pereira, K.D.; Das, G. Refining screening questionnaires for prediction of sleep apnea severity in children. Sleep Breath. Schlaf. Atm. 2020, 24, 1349–1356. [Google Scholar] [CrossRef]
- Owens, J.; Spirito, A.; Marcotte, A.; McGuinn, M.; Berkelhammer, L. Neuropsychological and Behavioral Correlates of Obstructive Sleep Apnea Syndrome in Children: A Preliminary Study. Sleep Breath. Schlaf. Atm. 2000, 4, 67–77. [Google Scholar] [CrossRef]
- Isaiah, A.; Spanier, A.J.; Grattan, L.M.; Wang, Y.; Pereira, K.D. Predictors of Behavioral Changes After Adenotonsillectomy in Pediatric Obstructive Sleep Apnea: A Secondary Analysis of a Randomized Clinical Trial. JAMA Otolaryngol.-Head Neck Surg. 2020, 146, 900–908. [Google Scholar] [CrossRef]
- Roland, P.S.; Rosenfeld, R.M.; Brooks, L.J.; Friedman, N.R.; Jones, J.; Kim, T.W.; Kuhar, S.; Mitchell, R.B.; Seidman, M.D.; Sheldon, S.H.; et al. Clinical practice guideline: Polysomnography for sleep-disordered breathing prior to tonsillectomy in children. Otolaryngol. Head Neck Surg. 2011, 145, S1–S15. [Google Scholar] [CrossRef]
- Pietropaoli, N.; Supino, M.C.; Vitelli, O.; Rabasco, J.; Evangelisti, M.; Forlani, M.; Parisi, P.; Villa, M.P. Cognitive function in preschool children with sleep-disordered breathing. Sleep Breath 2015, 19, 1431–1437. [Google Scholar] [CrossRef] [PubMed]
- Savini, S.; Ciorba, A.; Bianchini, C.; Stomeo, F.; Corazzi, V.; Vicini, C.; Pelucchi, S. Assessment of obstructive sleep apnoea (OSA) in children: An update. Acta Otorhinolaryngol. Ital. 2019, 39, 289–297. [Google Scholar] [CrossRef] [PubMed]
- Bitners, A.C.; Arens, R. Evaluation and Management of Children with Obstructive Sleep Apnea Syndrome. Lung 2020, 198, 257–270. [Google Scholar] [CrossRef]
- Berry, R.B.; Budhiraja, R.; Gottlieb, D.J.; Gozal, D.; Iber, C.; Kapur, V.K.; Marcus, C.L.; Mehra, R.; Parthasarathy, S.; Quan, S.F.; et al. Rules for scoring respiratory events in sleep: Update of the 2007 AASM manual for the scoring of sleep and associated events. J. Clin. Sleep Med. 2012, 8, 597–619. [Google Scholar] [CrossRef] [PubMed]
- Bonuck, K.A.; Freeman, K.; Henderson, J. Growth and growth biomarker changes after adenotonsillectomy: Systematic review and metaanalysis. Arch. Dis. Child. 2009, 94, 83–91. [Google Scholar] [CrossRef]
- Zaffanello, M.; Piacentini, G.; La Grutta, S. Beyond the growth delay in children with sleep-related breathing disorders: A systematic review. Panminerva Med. 2020, 62, 164–175. [Google Scholar] [CrossRef]
- Smith, C.B.; Walker, K.; Badawi, N.; Waters, K.A.; MacLean, J.E. Impact of sleep and breathing in infancy on outcomes at three years of age for children with cleft lip and/or palate. Sleep 2014, 37, 919–925. [Google Scholar] [CrossRef]
- Gozal, D.; Tan, H.L.; Kheirandish-Gozal, L. Treatment of Obstructive Sleep Apnea in Children: Handling the Unknown with Precision. J. Clin. Med. 2020, 9, 888. [Google Scholar] [CrossRef]
- Nosetti, L.; Zaffanello, M.; Katz, E.S.; Vitali, M.; Agosti, M.; Ferrante, G.; Cilluffo, G.; Piacentini, G.; La Grutta, S. Twenty-year follow-up of children with obstructive sleep apnea. J. Clin. Sleep Med. 2022, 18, 1573–1581. [Google Scholar] [CrossRef]
- Chuang, H.H.; Hsu, J.F.; Wang, C.Y.; Chuang, L.P.; Chen, M.C.; Chen, N.H.; Huang, Y.S.; Li, H.Y.; Lee, L.A. Hypertension in Children with Obstructive Sleep Apnea Syndrome-Age, Weight Status, and Disease Severity. Int. J. Environ. Res. Public Health 2021, 18, 9602. [Google Scholar] [CrossRef]
- Tsai, C.M.; Kang, C.H.; Su, M.C.; Lin, H.C.; Huang, E.Y.; Chen, C.C.; Hung, J.C.; Niu, C.K.; Liao, D.L.; Yu, H.R. Usefulness of desaturation index for the assessment of obstructive sleep apnea syndrome in children. Int. J. Pediatr. Otorhinolaryngol. 2013, 77, 1286–1290. [Google Scholar] [CrossRef] [PubMed]
- Saxby, C.; Stephenson, K.A.; Steele, K.; Ifeacho, S.; Wyatt, M.E.; Samuels, M. The Effect of Midface Advancement Surgery on Obstructive Sleep Apnoea in Syndromic Craniosynostosis. J. Craniofac. Surg. 2018, 29, 92–95. [Google Scholar] [CrossRef] [PubMed]
- Di Mauro, P.; Cocuzza, S.; Maniaci, A.; Ferlito, S.; Rasà, D.; Anzivino, R.; Vicini, C.; Iannella, G.; La Mantia, I. The Effect of Adenotonsillectomy on Children’s Behavior and Cognitive Performance with Obstructive Sleep Apnea Syndrome: State of the Art. Children 2021, 8, 921. [Google Scholar] [CrossRef] [PubMed]
- Zaffanello, M.; Piacentini, G.; La Grutta, S. The cardiovascular risk in paediatrics: The paradigm of the obstructive sleep apnoea syndrome. Blood Transfus 2020, 3, 217–225. [Google Scholar] [CrossRef]
- Lo Bue, A.; Salvaggio, A.; Insalaco, G. Obstructive sleep apnea in developmental age. A narrative review. Eur. J. Pediatr. 2020, 179, 357–365. [Google Scholar] [CrossRef]
- Zaffanello, M.; Piacentini, G.; Pietrobelli, A.; Fava, C.; Lippi, G.; Maffeis, C.; Gasperi, E.; Nosetti, L.; Bonafini, S.; Tagetti, A.; et al. Ambulatory clinical parameters and sleep respiratory events in a group of obese children unselected for respiratory problems. World J. Pediatr. 2017, 13, 577–583. [Google Scholar] [CrossRef]
- Moss, D.; Urschitz, M.S.; von Bodman, A.; Eitner, S.; Noehren, A.; Urschitz-Duprat, P.M.; Schlaud, M.; Poets, C.F. Reference values for nocturnal home polysomnography in primary schoolchildren. Pediatr. Res. 2005, 58, 958–965. [Google Scholar] [CrossRef]
- Dehlink, E.; Tan, H.L. Update on paediatric obstructive sleep apnoea. J. Thorac. Dis 2016, 8, 224–235. [Google Scholar] [CrossRef]
- Chervin, R.D.; Weatherly, R.A.; Garetz, S.L.; Ruzicka, D.L.; Giordani, B.J.; Hodges, E.K.; Dillon, J.E.; Guire, K.E. Pediatric sleep questionnaire: Prediction of sleep apnea and outcomes. Arch. Otolaryngol.-Head Neck Surg. 2007, 133, 216–222. [Google Scholar] [CrossRef]
- Ward, T.M.; Chen, M.L.; Landis, C.A.; Ringold, S.; Beebe, D.W.; Pike, K.C.; Wallace, C.A. Congruence between polysomnography obstructive sleep apnea and the pediatric sleep questionnaire: Fatigue and health-related quality of life in juvenile idiopathic arthritis. Qual. Life Res. 2017, 26, 779–788. [Google Scholar] [CrossRef]
- Varni, J.W.; Seid, M.; Kurtin, P.S. PedsQL 4.0: Reliability and validity of the Pediatric Quality of Life Inventory version 4.0 generic core scales in healthy and patient populations. Med. Care 2001, 39, 800–812. [Google Scholar] [CrossRef]
- Hullmann, S.E.; Ryan, J.L.; Ramsey, R.R.; Chaney, J.M.; Mullins, L.L. Measures of general pediatric quality of life: Child Health Questionnaire (CHQ), DISABKIDS Chronic Generic Measure (DCGM), KINDL-R, Pediatric Quality of Life Inventory (PedsQL) 4.0 Generic Core Scales, and Quality of My Life Questionnaire (QoML). Arthritis Care Res. 2011, 63 (Suppl. 11), S420–S430. [Google Scholar] [CrossRef]
- Amiri, S.; AbdollahiFakhim, S.; Lotfi, A.; Bayazian, G.; Sohrabpour, M.; Hemmatjoo, T. Effect of adenotonsillectomy on ADHD symptoms of children with adenotonsillar hypertrophy and sleep disordered breathing. Int. J. Pediatr. Otorhinolaryngol. 2015, 79, 1213–1217. [Google Scholar] [CrossRef] [PubMed]
- Bergeron, M.; Duggins, A.L.; Cohen, A.P.; Ishman, S.L. Comparison of Patient- and Parent-Reported Quality of Life for Patients Treated for Persistent Obstructive Sleep Apnea. Otolaryngol.–Head Neck Surg. 2018, 159, 789–795. [Google Scholar] [CrossRef]
- Conners, C.K.; Sitarenios, G.; Parker, J.D.; Epstein, J.N. The revised Conners’ Parent Rating Scale (CPRS-R): Factor structure, reliability, and criterion validity. J. Abnorm. Child Psychol. 1998, 26, 257–268. [Google Scholar] [CrossRef] [PubMed]
- Tabone, L.; Khirani, S.; Amaddeo, A.; Emeriaud, G.; Fauroux, B. Cerebral oxygenation in children with sleep-disordered breathing. Paediatr. Respir. Rev. 2020, 34, 18–23. [Google Scholar] [CrossRef] [PubMed]
- Tamanyan, K.; Walter, L.M.; Weichard, A.; Davey, M.J.; Nixon, G.M.; Biggs, S.N.; Horne, R.S.C. Age Effects on Cerebral Oxygenation and Behavior in Children with Sleep-disordered Breathing. Am. J. Respir. Crit. Care Med. 2018, 197, 1468–1477. [Google Scholar] [CrossRef] [PubMed]
- Brockmann, P.E.; Gozal, D. Neurocognitive Consequences in Children with Sleep Disordered Breathing: Who Is at Risk? Children 2022, 9, 1278. [Google Scholar] [CrossRef]
- Urbano, G.L.; Tablizo, B.J.; Moufarrej, Y.; Tablizo, M.A.; Chen, M.L.; Witmans, M. The Link between Pediatric Obstructive Sleep Apnea (OSA) and Attention Deficit Hyperactivity Disorder (ADHD). Children 2021, 8, 824. [Google Scholar] [CrossRef] [PubMed]
- Karimzadeh, P. Psycho-cognitive behavioral problems in sleep disordered children. Neural. Regen. Res. 2012, 7, 635–639. [Google Scholar]
- Goodwin, J.L.; Babar, S.I.; Kaemingk, K.L.; Rosen, G.M.; Morgan, W.J.; Sherrill, D.L.; Quan, S.F. Symptoms related to sleep-disordered breathing in white and hispanic children: The Tucson Children’s Assessment of Sleep Apnea study. Chest 2003, 124, 196–203. [Google Scholar] [CrossRef] [PubMed]
- Hvolby, A. Associations of sleep disturbance with ADHD: Implications for treatment. Atten Defic. Hyperact. Disord. 2015, 7, 1–18. [Google Scholar] [CrossRef]
- Kheirandish-Gozal, L.; Sahib, A.K.; Macey, P.M.; Philby, M.F.; Gozal, D.; Kumar, R. Regional brain tissue integrity in pediatric obstructive sleep apnea. Neurosci. Lett. 2018, 682, 118–123. [Google Scholar] [CrossRef] [PubMed]
- Operto, F.F.; Precenzano, F.; Bitetti, I.; Lanzara, V.; Fontana, M.L.; Pastorino, G.M.G.; Carotenuto, M.; Pisani, F.; Polito, A.N.; Smirni, D.; et al. Emotional Intelligence in Children with Severe Sleep-Related Breathing Disorders. Behav. Neurol. 2019, 2019, 6530539. [Google Scholar] [CrossRef]
- Bhattacharjee, R.; Kheirandish-Gozal, L.; Spruyt, K.; Mitchell, R.B.; Promchiarak, J.; Simakajornboon, N.; Kaditis, A.G.; Splaingard, D.; Splaingard, M.; Brooks, L.J.; et al. Adenotonsillectomy outcomes in treatment of obstructive sleep apnea in children: A multicenter retrospective study. Am. J. Respir. Crit. Care Med. 2010, 182, 676–683. [Google Scholar] [CrossRef] [PubMed]
- Section on Pediatric Pulmonology, Subcommittee on Obstructive Sleep Apnea Syndrome. Clinical practice guideline: Diagnosis and management of childhood obstructive sleep apnea syndrome. Pediatrics 2002, 109, 704–712. [Google Scholar] [CrossRef]
- Schechter, M.S.; Section on Pediatric Pulmonology, Subcommittee on Obstructive Sleep Apnea Syndrome. Technical report: Diagnosis and management of childhood obstructive sleep apnea syndrome. Pediatrics 2002, 109, e69. [Google Scholar] [CrossRef]
- Shan, S.; Wang, S.; Yang, X.; Liu, F.; Xiu, L. Effect of adenotonsillectomy on the growth, development, and comprehensive cognitive abilities of children with obstructive sleep apnea: A prospective single-arm study. BMC Pediatr. 2022, 22, 41. [Google Scholar] [CrossRef] [PubMed]
- Ajith, A.; Balu, R.; Kumar, M.; Panikkar, S. The Impact of Adenotonsillectomy on Sleep and Behavior of Children with Obstructive Sleep Apnea. Indian J. Otolaryngol. Head Neck Surg. 2022, 74, 329–333. [Google Scholar] [CrossRef]
- Bottle, A.; Neale, F.K.; Foley, K.A.; Viner, R.M.; Kenny, S.; Aylin, P.; Saxena, S.; Hargreaves, D.S. Impact of COVID-19 on outpatient appointments in children and young people in England: An observational study. BMJ Open 2022, 12, e060961. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Mean (SD) | Minimum | Maximum | Mean (SD) | Minimum | Maximum | p-Value (Mann–Whitney Test) | |
|---|---|---|---|---|---|---|---|
| Patients Contacted | Patients Included (*) | Patients Included Versus Excluded | |||||
| N. (males %) | 83 (59) | 47 (66) | - | - | 0.205 | ||
| Age at PSG (years) | 7.0 (3.5) | 2.1 | 14.5 | 5.8 (2.8) | 2.0 | 13.8 | 0.022 |
| Weight (kg) | 27.0 (21.7) | 4.1 | 125.0 | 24.4 (15.4) | 6.5 | 102.0 | 0.200 |
| Height (cm) | 112.0 (36.4) | 13.1 | 173.0 | 113.0 (19.8) | 62.0 | 173,0 | 0.047 |
| BMI (kg/m2) | 19.2 (7.2) | 12.5 | 56.0 | 17.6 (4.4) | 12.5 | 34.1 | 0.952 |
| BMI z-score | 0.3 (2.1) | −9.0 | 4.1 | 0.3 (1.7) | −3.8 | 2.9 | 0.830 |
| BMI percentile | 61.9 (36.4) | 0.1 | 99.9 | 59.4 (36.2) | 0.1 | 99.8 | 0.857 |
| Cardiorespiratory PSG (T0) | |||||||
| Duration of registration (h) | 9.2 (1.1) | 6.1 | 13.2 | 9.3 (0.9) | 7.2 | 11 | 0.823 |
| OA (events/h) | 3.4 (5.5) | 0.0 | 29.3 | 3.2 (4.6) | 0 | 22 | 0.705 |
| oAHI (events/h) | 5.9 (7.6) | 0.0 | 37.2 | 4.9 (5.7) | 0.0 | 24.6 | 0.578 |
| ODI (events/h) | 5.4 (7.3) | 0.0 | 36.0 | 3.2 (4.1) | 0.1 | 23.4 | 0.354 |
| SpO2 mean (%) | 96.0 (9.8) | 8.0 | 99.0 | 97.0 (1.0) | 95.0 | 99.0 | 0.628 |
| SpO2 minimum (%) | 85.8 (10.0) | 36.0 | 96.0 | 88.0 (7.0) | 51.0 | 95.0 | 0.263 |
| SpO2 < 90% (% eTST) | 0.7 (1.8) | 0.0 | 13.8 | 0.3 (0.8) | 0.0 | 4.2 | 0.600 |
| Snoring (% eTST) | 1.6 (3.9) | 0.0 | 22.1 | 1.5 (4.6) | 0.0 | 22.1 | 0.986 |
| T0 | oAHI > 1 event/h | ODI > 1 event/h | ||||
|---|---|---|---|---|---|---|
| T1 | PSQ − (n = 12) | PSQ + (n = 22) | PSQ − (n = 11) | PSQ + (n = 21) | ||
| Mean (SD) | Mean (SD) | p-Value (Mann-Whitney Test) | Mean (SD) | Mean (SD) | p-Value (Mann–Whitney Test) | |
| Physical results % | 92.7 (10.7) | 82.4 (13.9) | 0.015 | 92.9 (11.0) | 83.2 (14.4) | 0.034 |
| Emotional results % | 67.9 (15.3) | 61.9 (14.7) | 0.245 | 69.5 (14.2) | 62.9 (16.8) | 0.238 |
| Social results % | 82.1 (17.5) | 79.1 (21.0) | 0.292 | 85.5 (16.0) | 78.1 (20.9) | 0.481 |
| Academic achievement % | 90.9 (8.8) | 74.8 (21.1) | 0.048 | 90.5 (8.8) | 71.2 (20.5) | 0.009 |
| Psychosocial outcomes % | 80.0 (11.1) | 71.9 (16.2) | 0.169 | 81.8 (9.3) | 70.7 (16.1) | 0.056 |
| QoL total % | 84.5 (9.9) | 75.6 (14.0) | 0.063 | 85.7 (9.1) | 75.1 (14.3) | 0.038 |
| Objectivity (T-points) | 59.3 (13.5) | 67.3 (16.0) | 0.245 | 60.5 (14.0) | 64.9 (16.1) | 0.639 |
| Cognitive disorders (T-points) | 55.3 (14.4) | 59.7 (15.6) | 0.511 | 54.6 (15.2) | 62.3 (15.1) | 0.144 |
| Hyperactivity (T-points) | 58.5 (15.2) | 64.1 (12.8) | 0.217 | 57.2 (16.3) | 65.7 (12.6) | 0.113 |
| ADHD index (T-points) | 61.8 (13.0) | 68.0 (12.6) | 0.179 | 58.7 (11.8) | 70.7 (12.4) | 0.011 |
| T1 | oAHI > 1 event/h | ODI > 1 event/h | ||||
|---|---|---|---|---|---|---|
| T0 | PSQ − (n = 10) | PSQ + (n = 12) | PSQ − (n = 8) | PSQ + (n = 12) | ||
| Mean (SD) | Mean (SD) | p-Value (Mann–Whitney test) | Mean (SD) | Mean (SD) | p-Value (Mann-Whitney Test) | |
| Physical results (%) | 97.2 (4.3) | 82.6 (16.0) | 0.007 | 98.4 (2.9) | 83.1 (16.5) | 0.012 |
| Emotional results (%) | 69.5 (15.7) | 60.5 (15.5) | 0.180 | 74.4 (13.4) | 63.8 (19.3) | 0.157 |
| Social outcomes (%) | 86.5 (14.9) | 80.0 (21.2) | 0.771 | 91.3 (10.6) | 80.0 (21.2) | 0.473 |
| Educational attainment (%) | 90.0 (8.5) | 74.2 (21.2) | 0.123 | 91.3 (8.8) | 72.5 (19.7) | 0.039 |
| Psychosocial outcomes (%) | 82.0 (10.1) | 71.6 (14.8) | 0.123 | 85.6 (5.6) | 72.1 (15.6) | 0.057 |
| QoL total score (%) | 87.3 (7.9) | 75.4 (14.3) | 0.030 | 90.1 (4.3) | 75.9 (14.9) | 0.020 |
| Objectivity (T-score) | 57.2 (9.7) | 70.5 (19.6) | 0.203 | 56.8 (9.8) | 67.3 (19.7) | 0.473 |
| Cognitive disorders (T-score) | 51.0 (7.5) | 61.5 (17.7) | 0.203 | 50.4 (8.0) | 62.2 (17.2) | 0.135 |
| Hyperactivity (T-score) | 57.1 (13.9) | 66.1 (13.7) | 0.159 | 56.4 (15.7) | 66.5 (13.7) | 0.157 |
| ADHD index (T-score) | 59.5 (10.8) | 69.2 (15.1) | 0.159 | 55.9 (7.1) | 71.5 (14.7) | 0.020 |
| Dependent Variable | Variables Included in the Model | T | S.E. | Beta | t | Significance (p) | C.I. for B 95% (Lower Limit) | C.I. for B 95% (Upper Limit) |
|---|---|---|---|---|---|---|---|---|
| PSQ score (%), T0 | Physical results (%) | −0.543 | 0.226 | −0.360 | −2.406 | 0.021 | −0.998 | −0.087 |
| Emotional results (%) | −0.353 | 0.153 | −0.288 | −0.304 | 0.026 | −0.662 | −0.044 | |
| Social results (%) | 0.316 | 0.169 | 0.295 | 1.864 | 0.069 | −0.026 | 0.658 | |
| School results (%) | −0.435 | 0.139 | −0.429 | −3.125 | 0.003 | −0.716 | −0.154 | |
| Opposition (T-points) | 0.323 | 0.14 | 0.238 | 2.230 | 0.031 | 0.030 | 0.626 | |
| oAHI (events/h), T0 | Physical results (%) | −0.092 | 0.064 | −0.209 | −1.432 | 0.015 | −0.221 | 0.037 |
| ODI (events/h), T0 | Physical results (%) | 0.029 | 0.047 | 0.093 | 0.624 | 0.536 | −0.065 | 0.123 |
| Tempo SpO2 (%), T0 | Physical results (%) | 0.010 | 0.009 | 0.163 | 1.111 | 0.272 | −0.008 | 0.028 |
| SpO2 min (%), T0 | PSQ (%) | −0.161 | 0.062 | −0.439 | −2.605 | 0.013 | −0.286 | −0.036 |
| Physical abilities (%) | −0.257 | 0.104 | −0.464 | −2.475 | 0.018 | −0.467 | −0.047 | |
| Social abilities (%) | 0.190 | 0.074 | 0.483 | 2.552 | 0.015 | 0.040 | 0.340 | |
| School abilities (%) | 0.159 | 0.071 | 0.429 | 2.235 | 0.031 | 0.015 | 0.304 | |
| Index ADHD (T-points) | 0.259 | 0.092 | 0.536 | 2.810 | 0.008 | 0.073 | 0.445 | |
| BMI z-score, T0 | Social results (%) | −0.013 | 0.014 | −0.142 | −0.963 | 0.341 | −0.041 | 0.015 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zaffanello, M.; Ferrante, G.; Zoccante, L.; Ciceri, M.L.; Nosetti, L.; Tenero, L.; Piazza, M.; Piacentini, G. Predictive Power of Oxygen Desaturation Index (ODI) and Apnea-Hypopnea Index (AHI) in Detecting Long-Term Neurocognitive and Psychosocial Outcomes of Sleep-Disordered Breathing in Children: A Questionnaire-Based Study. J. Clin. Med. 2023, 12, 3060. https://doi.org/10.3390/jcm12093060
Zaffanello M, Ferrante G, Zoccante L, Ciceri ML, Nosetti L, Tenero L, Piazza M, Piacentini G. Predictive Power of Oxygen Desaturation Index (ODI) and Apnea-Hypopnea Index (AHI) in Detecting Long-Term Neurocognitive and Psychosocial Outcomes of Sleep-Disordered Breathing in Children: A Questionnaire-Based Study. Journal of Clinical Medicine. 2023; 12(9):3060. https://doi.org/10.3390/jcm12093060
Chicago/Turabian StyleZaffanello, Marco, Giuliana Ferrante, Leonardo Zoccante, Marco Luigi Ciceri, Luana Nosetti, Laura Tenero, Michele Piazza, and Giorgio Piacentini. 2023. "Predictive Power of Oxygen Desaturation Index (ODI) and Apnea-Hypopnea Index (AHI) in Detecting Long-Term Neurocognitive and Psychosocial Outcomes of Sleep-Disordered Breathing in Children: A Questionnaire-Based Study" Journal of Clinical Medicine 12, no. 9: 3060. https://doi.org/10.3390/jcm12093060
APA StyleZaffanello, M., Ferrante, G., Zoccante, L., Ciceri, M. L., Nosetti, L., Tenero, L., Piazza, M., & Piacentini, G. (2023). Predictive Power of Oxygen Desaturation Index (ODI) and Apnea-Hypopnea Index (AHI) in Detecting Long-Term Neurocognitive and Psychosocial Outcomes of Sleep-Disordered Breathing in Children: A Questionnaire-Based Study. Journal of Clinical Medicine, 12(9), 3060. https://doi.org/10.3390/jcm12093060