
Cranial Shape Measurements Obtained Using a Caliper and Elastic Bands Are Useful for Brachycephaly and Deformational Plagiocephaly Screening

 , , , and
, , , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Methods
2.2.1. Parameter Calculation Using the Caliper Method
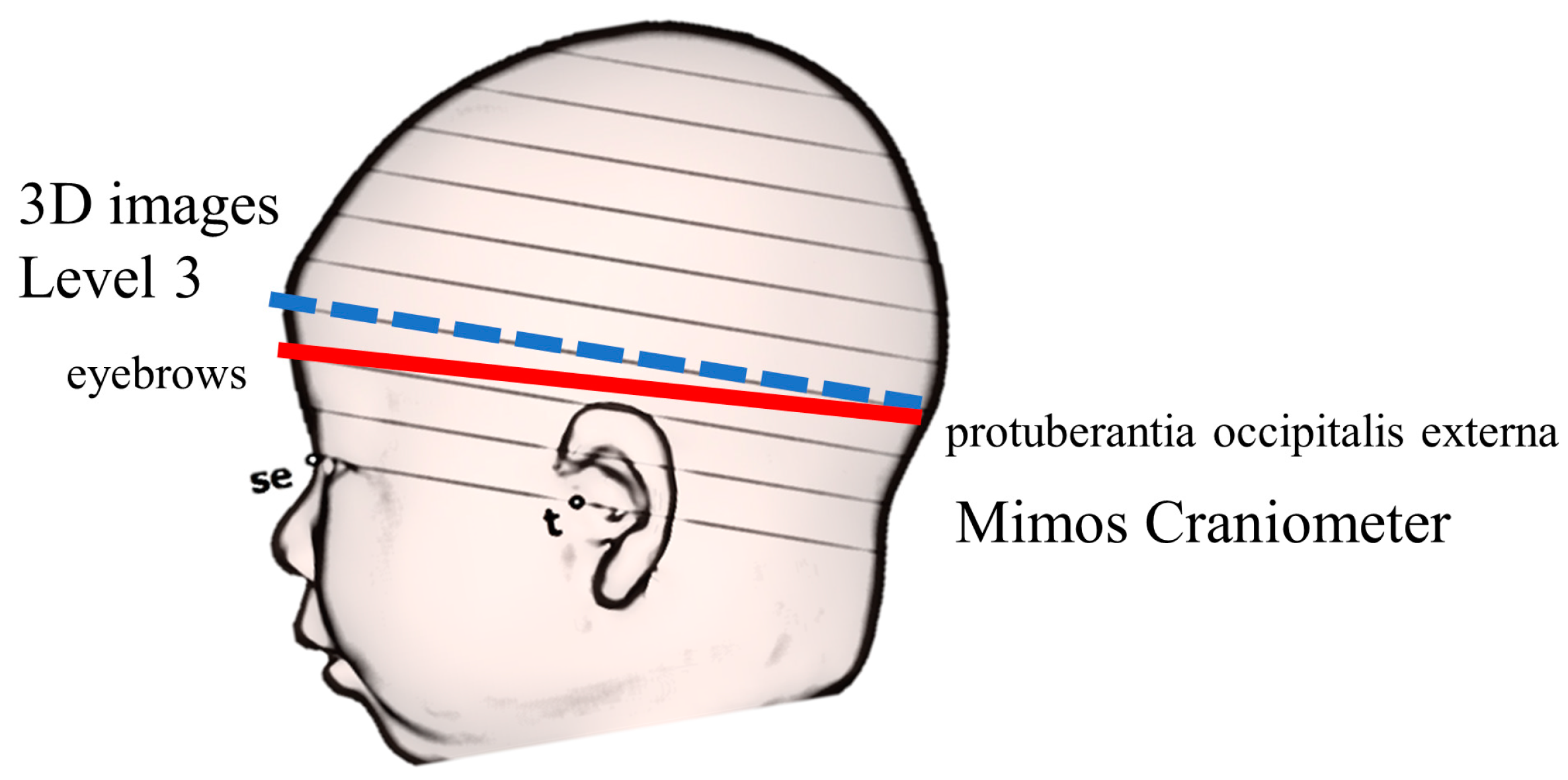
2.2.2. Parameter Calculation from 3D Images
2.2.3. Inspection Accuracy Evaluation Using a Dummy Doll (Study 1)
2.2.4. Measurement Accuracy in 1-Month-Old Infants (Study 2)
2.2.5. Database Comparison (Study 3)
3. Results
3.1. Inspection Accuracy Evaluation Using Dummy Doll (Study 1)
3.2. Measurement Accuracy in 1-Month-Old Infants (Study 2)
3.3. Comparison with the Database (Study 3)
4. Discussion
4.1. Measurement Accuracy Using the Mimos Craniometer
4.2. 3D Image and Caliper Measurement Comparison
4.3. Necessity of Understanding the Cranial Shape at 1 Month of Age
4.4. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Couture, D.E.; Crantford, J.C.; Somasundaram, A.; Sanger, C.; Argenta, A.E.; David, L.R. Efficacy of passive helmet therapy for deformational plagiocephaly: Report of 1050 cases. Neurosurg. Focus 2013, 35, E4. [Google Scholar] [CrossRef] [PubMed]
- Loveday, B.P.; de Chalain, T.B. Active counterpositioning or orthotic device to treat positional plagiocephaly? J. Craniofac. Surg. 2001, 12, 308–313. [Google Scholar] [CrossRef] [PubMed]
- Collett, B.R.; Gray, K.E.; Starr, J.R.; Heike, C.L.; Cunningham, M.L.; Speltz, M.L. Development at age 36 months in children with deformational plagiocephaly. Pediatrics 2013, 131, e109–e115. [Google Scholar] [CrossRef]
- Speltz, M.L.; Collett, B.R.; Stott-Miller, M.; Starr, J.R.; Heike, C.; Wolfram-Aduan, A.M.; King, D.; Cunningham, M.L. Case-control study of neurodevelopment in deformational plagiocephaly. Pediatrics 2010, 125, e537–e542. [Google Scholar] [CrossRef] [PubMed]
- Kordestani, R.K.; Patel, S.; Bard, D.E.; Gurwitch, R.; Panchal, J. Neurodevelopmental delays in children with deformational plagiocephaly. Plast. Reconstr. Surg. 2006, 117, 207–218; discussion 219–220. [Google Scholar] [CrossRef]
- Mawji, A.; Vollman, A.R.; Hatfield, J.; McNeil, D.A.; Sauvé, R. The incidence of positional plagiocephaly: A cohort study. Pediatrics 2013, 132, 298–304. [Google Scholar] [CrossRef]
- Miyabayashi, H.; Nagano, N.; Kato, R.; Noto, T.; Hashimoto, S.; Saito, K.; Morioka, I. Cranial shape in infants aged one month can predict the severity of deformational plagiocephaly at the age of six months. J. Clin. Med. 2022, 11, 1797. [Google Scholar] [CrossRef]
- Takamatsu, A.; Hikosaka, M.; Kaneko, T.; Mikami, M.; Kaneko, A. Evaluation of the molding helmet therapy for Japanese infants with deformational plagiocephaly. JMAJ 2021, 4, 50–60. [Google Scholar] [CrossRef]
- Koizumi, T.; Komuro, Y.; Hashizume, K.; Yanai, A. Cephalic index of Japanese children with normal brain development. J. Craniofac. Surg. 2010, 21, 1434–1437. [Google Scholar] [CrossRef]
- Miyabayashi, H.; Nagano, N.; Hashimoto, S.; Saito, K.; Kato, R.; Noto, T.; Sasano, M.; Sumi, K.; Yoshino, A.; Morioka, I. Evaluating cranial growth in Japanese infants using a three-dimensional scanner: Relationship between growth-related parameters and deformational plagiocephaly. Neurol. Med. Chir. 2022, 62, 521–529. [Google Scholar] [CrossRef]
- Miyabayashi, H.; Nagano, N.; Kato, R.; Hashimoto, S.; Saito, K.; Noto, T.; Ohashi, S.; Masunaga, K.; Morioka, I. Cranial shapes of Japanese preterm infants at one month of age using a three-dimensional scanner. Brain Dev. 2022, 44, 690–698. [Google Scholar] [CrossRef]
- Choi, H.; Lim, S.H.; Kim, J.S.; Hong, B.Y. Outcome analysis of the effects of helmet therapy in infants with brachycephaly. J. Clin. Med. 2020, 9, 1171. [Google Scholar] [CrossRef]
- Holowka, M.A.; Reisner, A.; Giavedoni, B.; Lombardo, J.R.; Coulter, C. Plagiocephaly severity scale to aid in clinical treatment recommendations. J. Craniofac. Surg. 2017, 28, 717–722. [Google Scholar] [CrossRef]
- Plank, L.H.; Giavedoni, B.; Lombardo, J.R.; Geil, M.D.; Reisner, A. Comparison of infant head shape changes in deformational plagiocephaly following treatment with a cranial remolding orthosis using a noninvasive laser shape digitizer. J. Craniofac. Surg. 2006, 17, 1084–1091. [Google Scholar] [CrossRef]
- Ifflaender, S.; Rüdiger, M.; Koch, A.; Burkhardt, W. Three-dimensional digital capture of head size in neonates—A method evaluation. PLoS ONE 2013, 8, e61274. [Google Scholar] [CrossRef]
- Kunz, F.; Schweitzer, T.; Große, S.; Waßmuth, N.; Stellzig-Eisenhauer, A.; Böhm, H.; Meyer-Marcotty, P.; Linz, C. Head orthosis therapy in positional plagiocephaly: Longitudinal 3D-investigation of long-term outcomes, compared with untreated infants and with a control group. Eur. J. Orthod. 2019, 41, 29–37. [Google Scholar] [CrossRef]
- Kanda, Y. Investigation of the freely available easy-to-use software “EZR” for medical statistics. Bone Marrow Transpl. 2013, 48, 452–458. [Google Scholar] [CrossRef]
- Pastor-Pons, I.; Lucha-López, M.O.; Barrau-Lalmolda, M.; Rodes-Pastor, I.; Rodríguez-Fernández, Á.L.; Hidalgo-García, C.; Tricás-Moreno, J.M. Interrater and intrarater reliability of cranial anthropometric measurements in infants with positional plagiocephaly. Children 2020, 7, 306. [Google Scholar] [CrossRef]
- Dörhage, K. Ursache und Diagnostik der lagebedingten Plagiozephalie. Man. Med. 2010, 48, 125–134. [Google Scholar] [CrossRef]
- Kim, D.G.; Lee, J.S.; Lee, J.W.; Yang, J.D.; Chung, H.Y.; Cho, B.C.; Choi, K.Y. The effects of helmet therapy relative to the size of the anterior fontanelle in nonsynostotic plagiocephaly: A retrospective study. J. Clin. Med. 2019, 8, 1977. [Google Scholar] [CrossRef]
- Skolnick, G.B.; Naidoo, S.D.; Nguyen, D.C.; Patel, K.B.; Woo, A.S. Evidence for use of frontozygomaticus and contralateral eurion as hand-caliper landmarks for assessment of deformational plagiocephaly. J. Craniofac. Surg. 2016, 27, 1498–1500. [Google Scholar] [CrossRef] [PubMed]
- Wu, Z.F.; Fan, Q.L.; Ming, L.; Yang, W.; Lv, K.L.; Chang, Q.; Li, W.Z.; Wang, C.J.; Pan, Q.M.; He, L.; et al. A comparative study between traditional head measurement and structured light three-dimensional scanning when measuring infant head shape. Transl. Pediatr. 2021, 10, 2897–2906. [Google Scholar] [CrossRef] [PubMed]
- Skolnick, G.B.; Naidoo, S.D.; Nguyen, D.C.; Patel, K.B.; Woo, A.S. Comparison of direct and digital measures of cranial vault asymmetry for assessment of plagiocephaly. J. Craniofac. Surg. 2015, 26, 1900–1903. [Google Scholar] [CrossRef] [PubMed]
- Aihara, Y.; Komatsu, K.; Dairoku, H.; Kubo, O.; Hori, T.; Okada, Y. Cranial molding helmet therapy and establishment of practical criteria for management in Asian infant positional head deformity. Childs Nerv. Syst. 2014, 30, 1499–1509. [Google Scholar] [CrossRef]
- Graham, T.; Adams-Huet, B.; Gilbert, N.; Witthoff, K.; Gregory, T.; Walsh, M. Effects of initial age and severity on cranial remolding orthotic treatment for infants with deformational plagiocephaly. J. Clin. Med. 2019, 8, 1097. [Google Scholar] [CrossRef]
- Aarnivala, H.; Vuollo, V.; Harila, V.; Heikkinen, T.; Pirttiniemi, P.; Valkama, A.M. Preventing deformational plagiocephaly through parent guidance: A randomized, controlled trial. Eur. J. Pediatr. 2015, 174, 1197–1208. [Google Scholar] [CrossRef]
- Hewitt, L.; Stephens, S.; Spencer, A.; Stanley, R.M.; Okely, A.D. Weekly group tummy time classes are feasible and acceptable to mothers with infants: A pilot cluster randomized controlled trial. Pilot Feasibility Stud. 2020, 6, 155. [Google Scholar] [CrossRef]
- Kato, R.; Nagano, N.; Hashimoto, S.; Saito, K.; Miyabayashi, H.; Noto, T.; Morioka, I. Three-dimensional versus two-dimensional evaluations of cranial asymmetry in deformational plagiocephaly using a three-dimensional scanner. Children 2022, 9, 788. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Intra-Examiner Analysis | Inter-Examiner Analysis | ||||||
|---|---|---|---|---|---|---|---|
| Mean | SD | CV | Mean | SD | CV | ||
| Cranial length | mm | 107.3 | 0.64 | 0.006 | 107.0 | 1.11 | 0.01 |
| Cranial width | mm | 100.6 | 0.49 | 0.005 | 100.0 | 1.73 | 0.017 |
| Longer diagonal A | mm | 107.4 | 0.49 | 0.005 | 107.0 | 1.34 | 0.013 |
| Shorter diagonal B | mm | 106.7 | 0.46 | 0.004 | 105.9 | 1.37 | 0.013 |
| A | Intra-Examiner Analysis (Craniometer) n:22 | |||||
| First Time | Second Time | ICC (1.1) | 95% Confidence Interval | p-Value | ||
| Cranial length | mm | 120.3 ± 4.1 | 120.3 ± 4.8 | 0.838 | 0.654–0.929 | <0.01 |
| Cranial width | mm | 104.2 ± 4.4 | 104.2 ± 4.8 | 0.928 | 0.838–0.969 | <0.01 |
| Longer diagonal A | mm | 118.6 ± 4.3 | 118.3 ± 4.4 | 0.964 | 0.916–0.985 | <0.01 |
| Shorter diagonal B | mm | 113.3 ± 3.5 | 113.6 ± 3.6 | 0.904 | 0.786–0.959 | <0.01 |
| Cephalic index | % | 86.7 ± 4.9 | 86.8 ± 5.7 | 0.862 | 0.700–0.940 | <0.01 |
| Cranial asymmetry | mm | 5.7 ± 4.0 | 5.2 ± 3.6 | 0.898 | 0.773–0.956 | <0.01 |
| B | Inter-examiner analysis (Craniometer) n:11 | |||||
| Examiner 1 | Examiner 2 | ICC (2.1) | 95% Confidence Interval | p-value | ||
| Cranial length | mm | 120.3 ± 4.0 | 120.3 ± 4.7 | 0.845 | 0.516–0.956 | <0.01 |
| Cranial width | mm | 104.4 ± 4.4 | 104.0 ± 4.8 | 0.927 | 0.759–0.960 | <0.01 |
| Longer diagonal A | mm | 118.4 ± 4.4 | 118.5 ± 4.5 | 0.870 | 0.584–0.963 | <0.01 |
| Shorter diagonal B | mm | 113.8 ± 3.3 | 113.4 ± 3.7 | 0.701 | 0.203–0.910 | <0.01 |
| Cephalic index | % | 86.9 ± 5.1 | 86.6 ± 5.4 | 0.938 | 0.791–0.983 | <0.01 |
| Cranial asymmetry | mm | 4.6 ± 3.4 | 5.1 ± 3.9 | 0.860 | 0.577–0.996 | <0.01 |
| C | Inter-device analysis (Craniometer vs. VECTRA H2) n:11 | |||||
| Craniometer | VECTRA H2 | ICC (3.1) | 95% Confidence Interval | p-value | ||
| Cranial length | mm | 120.3 ± 4.2 | 125.9 ± 4.9 | 0.718 | 0.243–0.915 | <0.01 |
| Cranial width | mm | 104.2 ± 4.5 | 109.3 ± 4.8 | 0.939 | 0.789–0.983 | <0.01 |
| Longer diagonal A | mm | 118.4 ± 4.3 | 118.8 ± 10 | 0.253 | −0.378–0.723 | 0.21 |
| Shorter diagonal B | mm | 113.6 ± 3.2 | 114.6 ± 8.7 | 0.086 | −0.516–0.631 | 0.40 |
| Cephalic index | % | 86.7 ± 5.2 | 86.9 ± 5.2 | 0.931 | 0.764–0.981 | <0.01 |
| Cranial asymmetry | mm | 4.8 ± 3.5 | 4.1 ± 3.4 | 0.738 | 0.283–0.922 | <0.01 |
| Craniometer | VECTRA H2 | Cohen’s Kappa Coefficient | 95% Confidence Interval | ||
|---|---|---|---|---|---|
| Number | 11 | 11 | |||
| Brachycephaly | n (%) | 4 (36.4) | 4 (36.4) | 1.000 | 1.000–1.000 |
| Deformational plagiocephaly | n (%) | 5 (45.5) | 4 (36.4) | 0.814 | 0.465–1.162 |
| Control (3DS) | Caliper | p-Value | |||
|---|---|---|---|---|---|
| Participants, n | 165 | 123 | |||
| Age of the mother | years | 33.1 ± 5.2 | 33.2 ± 5.3 | 0.94 | * |
| First child | n (%) | 80 (48.5) | 53 (43.1) | 0.40 | *** |
| Gestational age | weeks | 39.0 (37.9–40.0) | 38.9 (37.8–39.9) | 0.44 | ** |
| Birth weight | g | 3008 (2820–3260) | 3005 (2726–3238) | 0.34 | ** |
| Male | n (%) | 89 (53.9) | 61 (49.6) | 0.48 | *** |
| Measurement day age | days | 34 (31–40) | 31 (30–34) | <0.01 | ** |
| Weight on measurement day | g | 4291 ± 529 | 4133 ± 508 | 0.01 | * |
| Control (3DS) | Caliper | p-Value | |||
|---|---|---|---|---|---|
| n | 113 | 113 | |||
| Measurement day age | days | 32 (30–34) | 32 (30–34) | 0.98 | ** |
| Weight on measurement day | g | 4166 ± 739 | 4139 ± 509 | 0.48 | * |
| Cephalic index | % | 85.0 (80.8–89.0) | 85.2 (80.6–89.1) | 0.98 | ** |
| Cranial asymmetry | mm | 5.9 (3.5–8.4) | 6.0 (3.0–9.0) | 0.48 | ** |
| Brachycephaly | n (%) | 14 (12.4) | 20 (17.7) | 0.35 | *** |
| Deformational plagiocephaly | n (%) | 66 (58.4) | 64 (56.6) | 0.89 | *** |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Maedomari, T.; Miyabayashi, H.; Tanaka, Y.; Mukai, C.; Nakanomori, A.; Saito, K.; Kato, R.; Noto, T.; Nagano, N.; Morioka, I. Cranial Shape Measurements Obtained Using a Caliper and Elastic Bands Are Useful for Brachycephaly and Deformational Plagiocephaly Screening. J. Clin. Med. 2023, 12, 2787. https://doi.org/10.3390/jcm12082787
Maedomari T, Miyabayashi H, Tanaka Y, Mukai C, Nakanomori A, Saito K, Kato R, Noto T, Nagano N, Morioka I. Cranial Shape Measurements Obtained Using a Caliper and Elastic Bands Are Useful for Brachycephaly and Deformational Plagiocephaly Screening. Journal of Clinical Medicine. 2023; 12(8):2787. https://doi.org/10.3390/jcm12082787
Chicago/Turabian StyleMaedomari, Taishin, Hiroshi Miyabayashi, Yukari Tanaka, Chihiro Mukai, Aya Nakanomori, Katsuya Saito, Risa Kato, Takanori Noto, Nobuhiko Nagano, and Ichiro Morioka. 2023. "Cranial Shape Measurements Obtained Using a Caliper and Elastic Bands Are Useful for Brachycephaly and Deformational Plagiocephaly Screening" Journal of Clinical Medicine 12, no. 8: 2787. https://doi.org/10.3390/jcm12082787
APA StyleMaedomari, T., Miyabayashi, H., Tanaka, Y., Mukai, C., Nakanomori, A., Saito, K., Kato, R., Noto, T., Nagano, N., & Morioka, I. (2023). Cranial Shape Measurements Obtained Using a Caliper and Elastic Bands Are Useful for Brachycephaly and Deformational Plagiocephaly Screening. Journal of Clinical Medicine, 12(8), 2787. https://doi.org/10.3390/jcm12082787