
Secondary IgA Nephropathy and IgA-Associated Nephropathy: A Systematic Review of Case Reports

 , , , , , and
, , , , , and
Abstract
1. Introduction
1.1. Primary IgA Nephropathy
1.2. Secondary IgA Nephropathy
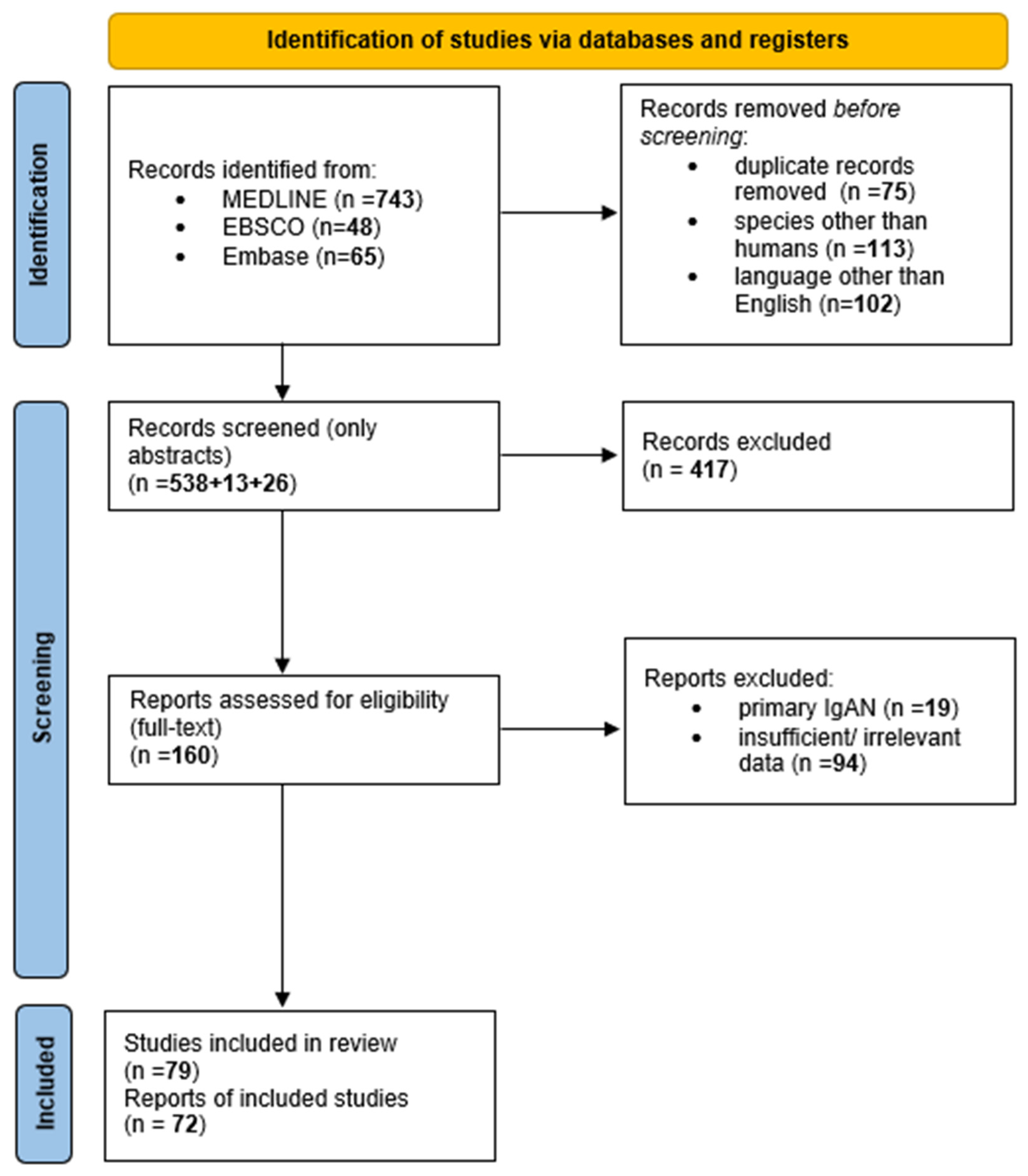
2. Materials and Methods
3. IgA Nephropathy Secondary to Gastrointestinal Diseases
3.1. Inflammatory Bowel Disease
3.2. Celiac Disease
3.3. Dysbiosis
4. IgA Nephropathy Secondary to Infections
4.1. Viral Infections
4.1.1. Hepatitis B Virus
4.1.2. Hepatitis A Virus
4.1.3. Human Immunodeficiency Virus
4.1.4. Epstein–Barr Virus
4.1.5. Severe Acute Respiratory Syndrome Coronavirus 2
4.2. Bacterial Infections
4.2.1. Methicillin-Resistant Staphylococcus Aureus (MRSA)
4.2.2. Methicillin-Sensitive Staphylococcus Aureus (MSSA)
4.2.3. Mycoplasma Pneumoniae
4.2.4. Borrelia Burgdorferi
4.2.5. Bartonella Henselae
4.2.6. Osteomyelitis
4.2.7. Tonsillitis
4.2.8. IgA-Dominant Postinfectious Glomerulonephritis
4.3. Protozoal Infections
Plasmodium Falciparum
4.4. Schostosoma Mansoni
5. IgA Nephropathy Secondary to Autoimmune Diseases
5.1. Sjögren’s Syndrome
5.2. Spondyloarthritis
5.3. Behcęt’s Disease
5.4. Henoch–Schönlein Purpura
6. IgA Nephropathy Secondary to Oncological Diseases
6.1. Renal Cell Carcinoma
6.2. Carcinomas of the Gastrointestinal Tract
6.3. Myeloproliferative Neoplasms
6.4. Hodgkin’s Lymphoma
7. IgA Nephropathy Secondary to Dermatological Conditions
7.1. Psoriasis
7.2. Dystrophic Epidermolysis Bullosa
7.3. Juvenile Dermatomyositis
8. IgA Nephropathy Secondary to Liver Diseases
8.1. Alcoholic Liver Conditions
8.2. Wilson’s Disease
8.3. Hemochromatosis
8.4. Viral Hepatitis
8.5. Autoimmune Hepatitis
8.6. Cirrhosis
9. IgA Nephropathy Secondary to Iatrogenic Causes
9.1. Tumor Necrosis Factor (TNF)-α Inhibitors
9.2. IL-12/IL-23-Inhibitor
9.3. Immune Checkpoint Inhibitors
9.4. CTLA4-Ig
9.5. Oral Anticoagulants
9.6. Anti-Vascular Endothelial Growth Factor
9.7. Thioureylene Derivative
10. IgA Nephropathy Secondary to Environmental Exposure
11. Conclusions
12. Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- D’Amico, G. The Commonest Glomerulonephritis in the World: IgA Nephropathy. Q. J. Med. 1987, 64, 709–727. [Google Scholar] [PubMed]
- Suzuki, H.; Kiryluk, K.; Novak, J.; Moldoveanu, Z.; Herr, A.B.; Renfrow, M.B.; Wyatt, R.J.; Scolari, F.; Mestecky, J.; Gharavi, A.G.; et al. The Pathophysiology of IgA Nephropathy. J. Am. Soc. Nephrol. 2011, 22, 1795–1803. [Google Scholar] [CrossRef] [PubMed]
- McGrogan, A.; Franssen, C.F.M.; De Vries, C.S. The Incidence of Primary Glomerulonephritis Worldwide: A Systematic Review of the Literature. Nephrol. Dial. Transplant. 2011, 26, 414–430. [Google Scholar] [CrossRef] [PubMed]
- Schena, F.P.; Nistor, I. Epidemiology of IgA Nephropathy: A Global Perspective. Semin. Nephrol. 2018, 38, 435–442. [Google Scholar] [CrossRef]
- Jennette, J.C.; Wall, S.D.; Wilkman, A.S. Low Incidence of IgA Nephropathy in Blacks. Kidney Int. 1985, 28, 944–950. [Google Scholar] [CrossRef]
- Coppo, R.; Robert, T. IgA Nephropathy in Children and in Adults: Two Separate Entities or the Same Disease? J. Nephrol. 2020, 33, 1219–1229. [Google Scholar] [CrossRef] [PubMed]
- Boitan, B.; Stancu, S.; Stefan, G.; Mircescu, G. Secondary versus Primary IGA Nephropathy: Are There Any Differences? Nephrol. Dial. Transplant. 2018, 33, i402. [Google Scholar] [CrossRef]
- Pouria, S.; Barratt, J. Secondary IgA Nephropathy. Semin. Nephrol. 2008, 28, 27–37. [Google Scholar] [CrossRef]
- Saha, M.K.; Julian, B.A.; Novak, J.; Rizk, D.V. Secondary IgA Nephropathy. Kidney Int. 2018, 94, 674–681. [Google Scholar] [CrossRef]
- Suzuki, H.; Yasutake, J.; Makita, Y.; Tanbo, Y.; Yamasaki, K.; Sofue, T.; Kano, T.; Suzuki, Y. IgA Nephropathy and IgA Vasculitis with Nephritis Have a Shared Feature Involving Galactose-Deficient IgA1-Oriented Pathogenesis. Kidney Int. 2018, 93, 700–705. [Google Scholar] [CrossRef]
- Cassol, C.A.; Bott, C.; Nadasdy, G.M.; Alberton, V.; Malvar, A.; Nagaraja, H.N.; Nadasdy, T.; Rovin, B.H.; Satoskar, A.A. Immunostaining for Galactose-Deficient Immunoglobulin A Is Not Specific for Primary Immunoglobulin A Nephropathy. Nephrol. Dial. Transplant. 2020, 35, 2123–2129. [Google Scholar] [CrossRef] [PubMed]
- Wang, M.; Lv, J.; Zhang, X.; Chen, P.; Zhao, M.; Zhang, H. Secondary IgA Nephropathy Shares the Same Immune Features with Primary IgA Nephropathy. Kidney Int. Rep. 2020, 5, 165–172. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.; Suzuki, H.; Kato, R.; Fukao, Y.; Nakayama, M.; Kano, T.; Makita, Y.; Suzuki, Y. Renal Pathological Analysis Using Galactose-Deficient IgA1-Specific Monoclonal Antibody Is a Strong Tool for Differentiation of Primary IgA Nephropathy from Secondary IgA Nephropathy. CEN Case Rep. 2021, 10, 17. [Google Scholar] [CrossRef]
- Tang, X.L.; Zheng, J.J.; Jiang, X.; Wan, F.; Hou, X.T.; Liu, S.J.; Zhang, M.F.; Song, Y.; Ye, T.; Yu, J. The Significance of Galactose-Deficient Immunoglobulin A1 Staining in Kidney Diseases with IgA Deposition. Int. Urol. Nephrol. 2023, 10, 14026. [Google Scholar] [CrossRef]
- Ishiko, S.; Horinouchi, T.; Fujimaru, R.; Shima, Y.; Kaito, H.; Tanaka, R.; Ishimori, S.; Kondo, A.; Nagai, S.; Aoto, Y.; et al. Glomerular Galactose-Deficient IgA1 Expression Analysis in Pediatric Patients with Glomerular Diseases. Sci. Rep. 2020, 10, 14026. [Google Scholar] [CrossRef] [PubMed]
- Obrişcă, B.; Ştefan, G.; Gherghiceanu, M.; Mandache, E.; Ismail, G.; Stancu, S.; Boitan, B.; Ion, O.; Mircescu, G. “Associated” or “Secondary” IgA Nephropathy? An Outcome Analysis. PLoS ONE 2019, 14, e0221014. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Moola, S.; Munn, Z.; Tufanaru, C.; Aromataris, E.; Sears, K.; Sfetcu, R.; Currie, M.; Lisy, K.; Qureshi, R.; Mattis, P.; et al. Chapter 7: Systematic Reviews of Etiology and Risk. Available online: https://synthesismanual.jbi.global (accessed on 12 March 2023). [CrossRef]
- Ambruzs, J.M.; Walker, P.D.; Larsen, C.P. The Histopathologic Spectrum of Kidney Biopsies in Patients with Inflammatory Bowel Disease. Clin. J. Am. Soc. Nephrol. 2014, 9, 265–270. [Google Scholar] [CrossRef]
- Ambruzs, J.M.; Larsen, C.P. Renal Manifestations of Inflammatory Bowel Disease. Rheum. Dis. Clin. N. Am. 2018, 44, 699–714. [Google Scholar] [CrossRef]
- Rehnberg, J.; Symreng, A.; Ludvigsson, J.F.; Emilsson, L. Inflammatory Bowel Disease Is More Common in Patients with IgA Nephropathy and Predicts Progression of ESKD: A Swedish Population-Based Cohort Study. J. Am. Soc. Nephrol. 2021, 32, 411–423. [Google Scholar] [CrossRef]
- Trimarchi, H.M.; Iotti, A.; Iotti, R.; Freixas, E.A.R.; Peters, R. Immunoglobulin A Nephropathy and Ulcerative Colitis. A Focus on Their Pathogenesis. Am. J. Nephrol. 2001, 21, 400–405. [Google Scholar] [CrossRef] [PubMed]
- Terasaka, T.; Uchida, H.A.; Umebayashi, R.; Tsukamoto, K.; Tanaka, K.; Kitagawa, M.; Sugiyama, H.; Tanioka, H.; Wada, J. The Possible Involvement of Intestine-Derived IgA 1: A Case of IgA Nephropathy Associated with Crohn’s Disease. BMC Nephrol. 2016, 17, 122. [Google Scholar] [CrossRef] [PubMed]
- Choi, J.Y.; Yu, C.H.; Jung, H.Y.; Jung, M.K.; Kim, Y.J.; Cho, J.H.; Kim, C.D.; Kim, Y.L.; Park, S.H. A Case of Rapidly Progressive IgA Nephropathy in a Patient with Exacerbation of Crohn’s Disease. BMC Nephrol. 2012, 13, 84. [Google Scholar] [CrossRef] [PubMed]
- Mertelj, T.; Smrekar, N.; Kojc, N.; Lindič, J.; Kovač, D. IgA Nephropathy in a Patient Treated with Adalimumab. Case Rep. Nephrol. Dial. 2021, 11, 233–240. [Google Scholar] [CrossRef] [PubMed]
- Kanazawa, N.; Wada, Y.; Akiyama, M.; Shikida, Y.; Sugiyama, M.; Abe, M.; Iyoda, M.; Honda, K.; Shibata, T. Crescentic IgA Nephropathy after Administration of Human Monoclonal Interleukin-12/23p40 Antibody in a Patient with Crohn’s Disease: A Case Report. CEN Case Rep. 2020, 9, 204–209. [Google Scholar] [CrossRef]
- Forshaw, M.J.; Guirguis, O.; Hennigan, T.W. IgA Nephropathy in Association with Crohn’s Disease. Int. J. Color. Dis. 2005, 20, 463–465. [Google Scholar] [CrossRef]
- Pipili, C.; Michopoulos, S.; Sotiropoulou, M.; Mpakirtzi, T.; Grapsa, E. Renal Failure Is There Any Association between IgA Nephropathy, Crohn’s Disease and Helicobacter Pylori Infection? Is There Any Association between IgA Nephropathy, Crohn’s Disease and Helicobacter Pylori Infection? Ren. Fail. 2012, 34, 506–509. [Google Scholar] [CrossRef]
- Ku, E.; Ananthapanyasut, W.; Campese, V.M. IgA Nephropathy in a Patient with Ulcerative Colitis, Graves’ Disease and Positive Myeloperoxidase ANCA. Clin. Nephrol. 2012, 77, 146–150. [Google Scholar] [CrossRef]
- Iida, H.; Asaka, M.; Izumino, K.; Takata, M.; Sasayama, S.; Tanaka, M. IgA Nephropathy Complicated by Ulcerative Colitis. Nephron 1989, 53, 285–286. [Google Scholar] [CrossRef]
- Onime, A.; Agaba, E.I.; Sun, Y.; Parsons, R.B.; Servilla, K.S.; Massie, L.W.; Tzamaloukas, A.H. Immunoglobulin A Nephropathy Complicating Ulcerative Colitis. Int. Urol. Nephrol. 2006, 38, 349–353. [Google Scholar] [CrossRef]
- Woodrow, G.; Innes, A.; Boyd, S.M.; Burden, R.P. A Case of IgA Nephropathy with Coeliac Disease Responding to a Gluten-Free Diet. Nephrol. Dial. Transplant. 1993, 8, 1382–1383. [Google Scholar] [CrossRef] [PubMed]
- Habura, I.; Fiedorowicz, K.; Woźniak, A.; Idasiak-Piechocka, I.; Kosikowski, P.; Oko, A. IgA Nephropathy Associated with Coeliac Disease. Cent. J. Immunol. 2019, 44, 106–108. [Google Scholar] [CrossRef]
- Koivuviita, N.; Tertti, R.; Heiro, M.; Metsärinne, K. A Case Report: A Patient with IgA Nephropathy and Coeliac Disease. Complete Clinical Remission Following Gluten-Free Diet. NDT Plus 2009, 2, 161–163. [Google Scholar] [CrossRef] [PubMed]
- Gupta, A.; Narain, U. IgA Nephropathy, Celiac Disease and Dermatitis Herpetiformis: A Rare Triad. J. Nephrol. Ther. 2016, 7, 2. [Google Scholar] [CrossRef]
- La Villa, G.; Pantaleo, P.; Tarquini, R.; Cirami, L.; Perfetto, F.; Mancuso, F.; Laffi, G. Multiple Immune Disorders in Unrecognized Celiac Disease: A Case Report. World J. Gastroenterol. 2003, 9, 1377–1380. [Google Scholar] [CrossRef]
- Gaughan, W.J.; Hassan, M.H.; McCue, P.A.; Burke, J.F.; Sharma, K. Association of IgA Nephropathy with Clostridium Difficile Colitis. Am. J. Kidney Dis. 1999, 34, e16. [Google Scholar] [CrossRef]
- Kawakita, C.; Kinomura, M.; Otaka, N.; Kitagawa, M.; Sugiyama, H.; Kusano, N.; Mizuno, M.; Wada, J. HIV-Associated Immune Complex Kidney Disease with C3-Dominant Deposition Induced by HIV Infection after Treatment of IgA Nephropathy. Intern. Med. 2019, 58, 3001–3007. [Google Scholar] [CrossRef]
- Hsieh, W.S.; Szukala, S.; Howell, D.N.; Conlon, P.J. Crescentic IgA Nephropathy and Acute Renal Failure in an HIV-Positive Patient with Enteric Salmonella Infection. Nephrol. Dial. Transplant. 1996, 11, 2320–2323. [Google Scholar] [CrossRef]
- Gorriz, J.L.; Rovira, E.; Sancho, A.; Ferrer, R.; Paricio, A.; Pallardo, M. IgA Nephropathy Associated with Human Immuno Deficiency Virus Infection: Antiproteinuric Effect of Captopril. Nephrol. Dial. Transplant. 1997, 12, 2796–2797. [Google Scholar] [CrossRef]
- Jindal, K.K.; Trillo, A.; Bishop, G.; Hirsch, D.; Cohen, A. Crescentic IgA Nephropathy as a Manifestation of Human Immune Deficiency Virus Infection. Am. J. Nephrol. 1991, 11, 147–150. [Google Scholar] [CrossRef]
- Miyasato, Y.; Miyoshi, T.; Fujimoto, D.; Adachi, M.; Kitamura, K.; Mukoyama, M. Successful Treatment of Rapidly Progressive Immunoglobulin A Nephropathy with Human Immunodeficiency Virus Infection by Steroid Pulse Therapy and Tonsillectomy. Nephrology 2016, 21, 159–160. [Google Scholar] [CrossRef] [PubMed]
- Ochi, M.; Toyama, T.; Ando, M.; Sato, K.; Kamikawa, Y.; Sagara, A.; Kitajima, S.; Hara, A.; Iwata, Y.; Sakai, N.; et al. A Case of Secondary IgA Nephropathy Accompanied by Psoriasis Treated with Secukinumab. CEN Case Rep. 2019, 8, 200–204. [Google Scholar] [CrossRef] [PubMed]
- Sakellariou, G.T.; Vounotrypidis, P.; Berberidis, C. Infliximab Treatment in Two Patients with Psoriatic Arthritis and Secondary IgA Nephropathy. Clin. Rheumatol. 2007, 26, 1132–1133. [Google Scholar] [CrossRef] [PubMed]
- Veer Manchanda, B.; Aggarwal, G.; Bhatnagar, M.; Aggarwal, J.; Mehra, S.; Gupta, N. A Case Report of A Patient of Iga Nephropathy Associated with Psoriasis: A Contribution to the Entity of “Psoriatic Nephropathy”. IOSR J. Dent. Med. Sci. 2017, 16, 5–7. [Google Scholar] [CrossRef]
- Segawa, Y.; Ishida, R.; Kanehisa, F.; Nakai, K.; Morimoto, M.; Seno, M.; Nakayama, M.; Kusaba, T.; Katoh, N.; Tamagaki, K. IgA Nephropathy in a Patient Receiving Infliximab for Generalized Pustular Psoriasis. BMC Nephrol. 2020, 21, 366. [Google Scholar] [CrossRef]
- Zadrazil, J.; Tichý, T.; Horák, P.; Nikorjaková, I.; Zíma, P.; Krejcí, K.; Strébl, P. IgA Nephropathy Associated with Psoriasis Vulgaris: A Contribution to the Entity of “Psoriatic Nephropathy”. J. Nephrol. 2006, 19, 382–386. [Google Scholar]
- Ceuppens, S.H.E.; Kimenai, H.J.A.N.; Roodnat, J.I.; Mertens zur Borg, I.R.A.M.; Duipmans, J.C.; IJzermans, J.N.M.; Minnee, R.C. Living Donor Kidney Transplantation in a Patient With Epidermolysis Bullosa: A Case Report. Transplant. Proc. 2019, 51, 3074–3076. [Google Scholar] [CrossRef]
- Kawasaki, Y.; Isome, M.; Takano, K.; Suyama, K.; Imaizumi, T.; Matsuura, H.; Ichii, K.; Hashimoto, K.; Hosoya, M. IgA Nephropathy in a Patient with Dominant Dystrophic Epidermolysis Bullosa. Tohoku J. Exp. Med. 2008, 214, 297–301. [Google Scholar] [CrossRef][Green Version]
- Ungureanu, S.; Adni, T.; Brown, T.; Inston, N.; Heagerty, A. Successful Renal Transplant in a Patient with Non-Herlitz Junctional Epidermolysis Bullosa. Clin. Exp. Dermatol. 2014, 39, 330–332. [Google Scholar] [CrossRef]
- Takada, D.; Sumida, K.; Sekine, A.; Hazue, R.; Yamanouchi, M.; Suwabe, T.; Hayami, N.; Hoshino, J.; Sawa, N.; Takaichi, K.; et al. IgA Nephropathy Featuring Massive Wire Loop-like Deposits in Two Patients with Alcoholic Cirrhosis. BMC Nephrol. 2017, 18, 362. [Google Scholar] [CrossRef]
- Kaneko, T.; Arima, R.; Arakawa, Y.; Aoki, M.; Fukuda, K.; Fukui, M.; Hirama, A.; Fujita, E.; Mii, A.; Utsumi, K.; et al. Two Cases of Rapidly Progressive Nephritic Syndrome Complicated with Alcoholic Liver Cirrhosis. Nihon Jinzo Gakkai Shi 2011, 53, 60–67. [Google Scholar] [PubMed]
- Shimamura, Y.; Maeda, T.; Gocho, Y.; Ogawa, Y.; Tsuji, K.; Takizawa, H. Immunoglobulin A Nephropathy Secondary to Wilson’s Disease: A Case Report and Literature Review. CEN Case Rep. 2019, 8, 61–66. [Google Scholar] [CrossRef]
- Bhandari, G.; Tiwari, V.; Gupta, A.; Gupta, P.; Bhargava, V.; Malik, M.; Gupta, A.; Bhalla, A.; Rana, D. IgA Nephropathy with Wilson’s Disease: A Case Report and Literature Review. Indian J. Nephrol. 2021, 31, 474–477. [Google Scholar] [CrossRef] [PubMed]
- Nakayama, M.; Kaizu, Y.; Uesugi, N.; Nakashita, S.; Suehiro, T. A Case of IgA Nephropathy and Renal Hemosiderosis Associated with Primary Hemochromatosis. Ren. Fail. 2008, 30, 813–817. [Google Scholar] [CrossRef] [PubMed]
- Denha, E.; Rahim, A.; Modi, S.; Oyibo, O.; Scott, M. A 55-Year-Old Male Presenting with a Lower Extremity Rash: A Case of Immunoglobulin A (IgA) Nephropathy. Cureus 2021, 13, e14165. [Google Scholar] [CrossRef]
- Dey, A.K.; Bhattacharya, A.; Majumdar, A. Hepatitis C as a Potential Cause of IgA Nephropathy. Indian J. Nephrol. 2013, 23, 143–145. [Google Scholar] [CrossRef]
- Ji, F.; Li, Z.; Ge, H.; Deng, H. Successful Interferon-α Treatment in a Patient with IgA Nephropathy Associated with Hepatitis C Virus Infection. Intern. Med. 2010, 49, 2531–2532. [Google Scholar] [CrossRef][Green Version]
- Chen, Y.; Zhao, X.; Tang, D.; Xu, C.; Sun, L.; Sun, L.; Wu, J.; Mei, C. IgA Nephropathy in Two Patients with Sjögren’s Syndrome: One with Concomitant Autoimmune Hepatitis. Intern. Med. 2010, 49, 37–43. [Google Scholar] [CrossRef]
- Tsai, T.C.; Chen, C.Y.; Lin, W.T.; Lee, W.J.; Chen, H.C. Sjogren’s Syndrome Complicated with IgA Nephropathy and Leukocytoclastic Vasculitis. Ren. Fail. 2008, 30, 755–758. [Google Scholar] [CrossRef]
- Jacquet, A.; Francois, H.; Frangie, C.; Yahiaoui, Y.; Ferlicot, S.; Micelli, C.; Mariette, X.; Durrbach, A. IgA Nephropathy Associated with Ankylosing Spondylitis Is Not Controlled by Infliximab Therapy. Nephrol. Dial. Transplant. 2009, 24, 3540–3542. [Google Scholar] [CrossRef][Green Version]
- Mimura, I.; Tojo, A.; Kinugasa, S.; Uozaki, H.; Fujita, T. Renal Cell Carcinoma in Association with IgA Nephropathy in the Elderly. Am. J. Med. Sci. 2009, 338, 431–432. [Google Scholar] [CrossRef] [PubMed]
- Kocyigit, I.; Dortdudak, S.; Eroglu, E.; Unal, A.; Sipahioglu, M.H.; Berk, V.; Tokgoz, B.; Oymak, O. Immunoglobulin A Nephropathy Could Be a Clue for the Recurrence of Gastric Adenocarcinoma. Nefrologia 2013, 33, 853–855. [Google Scholar] [CrossRef]
- Yoo, C.; Choi, Y.-J.; In Shim, S.; Lee, K. IgA Nephropathy Encountered in a Patient with Hodgkin Lymphoma. Korean J. Nephrol. 2008, 27, 720–725. [Google Scholar]
- Chen, F.F.; Tang, H.Y.; Yu, F.; Que, C.L.; Zhou, F.-D.; Wang, S.X.; Wang, G.F.; Zhao, M.H. Renal Involvement in a Silicosis Patient—Case Report and Literature Review. Ren. Fail. 2019, 41, 1045–1053. [Google Scholar] [CrossRef] [PubMed]
- Rao, N.; Bendall, A.; Lanteri, M. ANCA Vasculitis and IgA Nephropathy Linked to Silica Exposure. Occup. Med. 2020, 70, 445–448. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Clayton, F.; Shihab, F.; Goldfarb-Rumyantzev, A. Successful Treatment of Recurrent Henoch–Schönlein Purpura in a Renal Allograft with Plasmapheresis. Am. J. Transplant. 2008, 8, 228–231. [Google Scholar] [CrossRef]
- Riley, A.M.; Wall, B.M.; Cooke, C.R. Favorable Outcome After Aggressive Treatment of Infection in a Diabetic Patient With MRSA-Related IgA Nephropathy. Am. J. Med. Sci. 2009, 337, 221–223. [Google Scholar] [CrossRef]
- Javed, Z.A.; Shah, A.F. A Case of Secondary IgA Nephropathy and Response to Steroids. J. Am. Soc. Nephrol. 2020, 31, 98. [Google Scholar]
- Kanayama, Y.; Shiota, K.; Kotumi, K.; Ikuno, Y.; Yasumoto, R.; Ishii, M.; Inoue1, T. Mycoplasma Pneumoniae Pneumonia Associated with Iga Nephropathy. Scand. J. Infect. Dis. 2015, 14, 231–233. [Google Scholar] [CrossRef]
- Suzuki, K.; Hirano, K.; Onodera, N.; Takahashi, T.; Tanaka, H. Acute IgA Nephropathy Associated with Mycoplasma Pneumoniae Infection. Pediatr. Int. 2005, 47, 583–585. [Google Scholar] [CrossRef]
- McCausland, F.R.; Niedermaier, S.; Bijol, V.; Rennke, H.G.; Choi, M.E.; Forman, J.P. Lyme Disease-Associated Glomerulonephritis. Nephrol. Dial. Transplant. 2011, 26, 3054–3056. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Hopp, L.; Eppes, S.C. Development of IgA Nephritis following Cat Scratch Disease in a 13-Year-Old Boy. Pediatr. Nephrol. 2004, 19, 682–684. [Google Scholar] [CrossRef] [PubMed]
- Tevlin, M.T.; Wall, B.M.; Cooke, C.R. Reversible Renal Failure Due to IgA Nephropathy Associated with Osteomyelitis. Am. J. Kidney Dis. 1992, 20, 185–188. [Google Scholar] [CrossRef] [PubMed]
- Liess, B.D.; Mytyk, C.; Calhoun, K.H.; Whaley-Connell, A.T. Tonsillectomy for the Treatment of Tonsillitis-Induced Immunoglobulin A Nephropathy. Am. J. Otolaryngol. 2010, 31, 485–488. [Google Scholar] [CrossRef] [PubMed]
- Yoo, D.E.; Kim, J.H.; Kie, J.H.; Park, Y.; Chang, T.I.; Oh, H.J.; Kim, S.J.; Yoo, T.H.; Choi, K.H.; Kang, S.W.; et al. Immunoglobulin A Nephropathy Associated with Plasmodium Falciparum Malaria. J. Korean Med. Sci. 2012, 27, 446–449. [Google Scholar] [CrossRef]
- Gonçalves, F.O.; de, S. Fontes, T.M.; Canuto, A.P.P.S.L. Schistosoma Mansoni Associated Glomerulopathy with IgA Mesangial Deposits: Case Report. J. Bras. Nefrol. 2017, 39, 86–90. [Google Scholar] [CrossRef]
- Collin, P.; Syrjanen, J.; Partanen, J.; Pasternack, A.; Kaukinen, K.; Mustonen, J. Celiac Disease and HLA DQ in Patients with IgA Nephropathy. Am. J. Gastroenterol. 2002, 97, 2572–2576. [Google Scholar] [CrossRef]
- Welander, A.; Sundelin, B.; Fored, M.; Ludvigsson, J.F. Increased Risk of IgA Nephropathy among Individuals with Celiac Disease. J. Clin. Gastroenterol. 2013, 47, 678–683. [Google Scholar] [CrossRef]
- Ludvigsson, J.F.; Montgomery, S.M.; Olén, O.; Ekbom, A.; Ludvigsson, J.; Fored, M. Coeliac Disease and Risk of Renal Disease-a General Population Cohort Study. Nephrol. Dial. Transplant. 2006, 21, 1809–1815. [Google Scholar] [CrossRef]
- Rani, M.; Sogi, D.S.; Gill, B.S. Characterization of Gliadin, Secalin and Hordein Fractions Using Analytical Techniques. Sci. Rep. 2021, 11, 23135. [Google Scholar] [CrossRef]
- Mäki, M.; Mustalahti, K.; Kokkonen, J.; Kulmala, P.; Haapalahti, M.; Karttunen, T.; Ilonen, J.; Laurila, K.; Dahlbom, I.; Hansson, T.; et al. Prevalence of Celiac Disease among Children in Finland. N. Engl. J. Med. 2003, 348, 2517–2524. [Google Scholar] [CrossRef] [PubMed]
- Abbad, L.; Monteiro, R.C.; Berthelot, L. Food Antigens and Transglutaminase 2 in IgA Nephropathy: Molecular Links between Gut and Kidney. Mol. Immunol. 2020, 121, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Iversen, R.; Fleur du Pre, M.; Di Niro, R.; Sollid, L.M. Igs as Substrates for Transglutaminase 2: Implications for Autoantibody Production in Celiac Disease. J. Immunol. 2015, 195, 5159–5168. [Google Scholar] [CrossRef] [PubMed]
- Cheung, C.K.; Barratt, J. Gluten and IgA Nephropathy: You Are What You Eat? Kidney Int. 2015, 88, 215–218. [Google Scholar] [CrossRef]
- Coppo, R.; Roccatello, D.; Amore, A.; Quattrocchio, G.; Molino, A.; Gianoglio, B.; Amoroso, A.; Bajardi, P.; Piccoli, G. Effects of a Gluten-Free Diet in Primary IgA Nephropathy. Clin. Nephrol. 1990, 33, 72–86. [Google Scholar]
- De Angelis, M.; Montemurno, E.; Piccolo, M.; Vannini, L.; Lauriero, G.; Maranzano, V.; Gozzi, G.; Serrazanetti, D.; Dalfino, G.; Gobbetti, M.; et al. Microbiota and Metabolome Associated with Immunoglobulin A Nephropathy (IgAN). PLoS ONE 2014, 9, e99006. [Google Scholar] [CrossRef]
- Forbes, J.D.; Van Domselaar, G.; Bernstein, C.N. The Gut Microbiota in Immune-Mediated Inflammatory Diseases. Front. Microbiol. 2016, 7, 1081. [Google Scholar] [CrossRef]
- Dong, R.; Bai, M.; Zhao, J.; Wang, D.; Ning, X.; Sun, S. A Comparative Study of the Gut Microbiota Associated With Immunoglobulin a Nephropathy and Membranous Nephropathy. Front. Cell. Infect. Microbiol. 2020, 10, 557368. [Google Scholar] [CrossRef]
- He, J.W.; Zhou, X.J.; Lv, J.C.; Zhang, H. Perspectives on How Mucosal Immune Responses, Infections and Gut Microbiome Shape IgA Nephropathy and Future Therapies. Theranostics 2020, 10, 11462–11478. [Google Scholar] [CrossRef]
- Gesualdo, L.; Di Leo, V.; Coppo, R. The Mucosal Immune System and IgA Nephropathy. Semin. Immunopathol. 2021, 43, 657–668. [Google Scholar] [CrossRef]
- Lai, K.N.; Lai, F.M.; Tam, J.S. IgA Nephropathy Associated with Chronic Hepatitis B Virus Infection in Adults: The Pathogenetic Role of HBsAG. J. Pathol. 1989, 157, 321–327. [Google Scholar] [CrossRef] [PubMed]
- Wang, K.; Yu, Z.; Huang, Y.; Yang, K.; He, T.; Xiao, T.; Yu, Y.; Li, Y.; Liu, L.; Xiong, J.; et al. Clinicopathological Features, Risk Factors, and Outcomes of Immunoglobulin A Nephropathy Associated with Hepatitis B Virus Infection. J. Nephrol. 2021, 34, 1887–1896. [Google Scholar] [CrossRef] [PubMed]
- Al-Homrany, M. Immunoglobulin A Nephropathy Associated with Hepatitis A Virus Infection. J. Nephrol. 2001, 14, 115–119. [Google Scholar] [PubMed]
- Han, S.H.; Kang, E.W.; Kie, J.H.; Yoo, T.H.; Choi, K.H.; Han, D.S.; Kang, S.W. Spontaneous Remission of IgA Nephropathy Associated with Resolution of Hepatitis A. Am. J. Kidney Dis. 2010, 56, 1163–1167. [Google Scholar] [CrossRef] [PubMed]
- Beaufils, H.; Jouanneau, C.; Katlama, C.; Sazdovitch, V.; Hauw, J.J. HIV-Associated IgA Nephropathy—A Post-Mortem Study. Nephrol. Dial. Transplant. 1995, 10, 35–38. [Google Scholar] [PubMed]
- Bene, M.C.; Canton, P.; Amiel, C.; May, T.; Faure, G. Absence of Mesangial IgA in AIDS: A Postmortem Study. Nephron 1991, 58, 240–241. [Google Scholar] [CrossRef]
- Kanno, Y.; Suzuki, H.; Okada, H.; Nakazato, Y.; Saruta, T. Retroviral Infection in Peripheral Mononuclear Cells in Patients with IgA Nephropathy. Clin. Nephrol. 1997, 47, 211–216. [Google Scholar]
- Zachova, K.; Kosztyu, P.; Zadrazil, J.; Matousovic, K.; Vondrak, K.; Hubacek, P.; Julian, B.A.; Moldoveanu, Z.; Novak, Z.; Kostovcikova, K.; et al. Role of Epstein-Barr Virus in Pathogenesis and Racial Distribution of IgA Nephropathy. Front. Immunol. 2020, 11, 267. [Google Scholar] [CrossRef]
- Huang, Y.; Li, X.J.; Li, Y.Q.; Dai, W.; Shao, T.; Liu, W.Y.; Han, M.; Xu, G.; Liu, L. Clinical and Pathological Findings of SARS-CoV-2 Infection and Concurrent IgA Nephropathy: A Case Report. BMC Nephrol. 2020, 21, 504. [Google Scholar] [CrossRef]
- Farooq, H.; Aemaz Ur Rehman, M.; Asmar, A.; Asif, S.; Mushtaq, A.; Qureshi, M.A. The Pathogenesis of COVID-19-Induced IgA Nephropathy and IgA Vasculitis: A Systematic Review. J. Taibah Univ. Med. Sci. 2022, 17, 1–13. [Google Scholar] [CrossRef]
- Nasr, S.H.; D’Agati, V.D. IgA-Dominant Postinfectious Glomerulonephritis: A New Twist on an Old Disease. Nephron Clin. Pract. 2011, 119, c18–c25. [Google Scholar] [CrossRef] [PubMed]
- Huang, Z.; Chen, B.; Zhou, Y.; Liang, Y.; Qiu, W.; Lv, Y.; Ding, X.; Zhang, J.; Chen, C. Clinicopathological and Prognostic Study of IgA-Dominant Postinfectious Glomerulonephritis. BMC Nephrol. 2021, 22, 248. [Google Scholar] [CrossRef] [PubMed]
- Syrbe, U.; Baraliakos, X. Spondyloarthritis. Z. Rheumatol. 2018, 77, 783–788. [Google Scholar] [CrossRef] [PubMed]
- Zhang, T.; Yang, F.; Zuo, K.; Wang, J.; Cheng, Z.; Zhang, J. HLA-B27 Negativity Is Associated with Renal Function Decline in Patients with Ankylosing Spondylitis and Secondary IgA Nephropathy. Front. Med. 2020, 7, 89. [Google Scholar] [CrossRef] [PubMed]
- Yver, L.; Blanchier, D.; Aouragh, F.; Turpin, Y.; Chaubert, N.; Laregue, M.; Goujon, J.M.; Touchard, G. Renal Involvement in Behçet’s Disease. Case Report and Review of the Literature. Nephron 1996, 73, 689–691. [Google Scholar] [CrossRef]
- Hemmen, T.; Perez-Canto, A.; Distler, A.; Offermann, G.; Braun, J. IgA Nephropathy in a Patient with Behçet’s Syndrome—Case Report and Review of Literature. Br. J. Rheumatol. 1997, 36, 696–699. [Google Scholar] [CrossRef]
- Fernandes, P.F.; Júnior, G.B.; Barros, F.A.; Sousa, D.C.; Franco, L.M.; Patrocínio, R.M. Behcet’s Disease and IgA Nephropathy: Report of This Association in a Patient from Brazil and Literature Review. Investig. Clin. 2006, 47, 405–411. [Google Scholar]
- Hetland, L.E.; Susrud, K.S.; Lindahl, K.H.; Bygum, A. Henoch-Schönlein Purpura: A Literature Review. Acta Derm. Venereol. 2017, 97, 1160–1166. [Google Scholar] [CrossRef]
- Cagnoli, L. Solid Tumors and Paraneoplastic Glomerulonephritis. G. Ital. Nefrol. 2010, 27 (Suppl. S50), S51–S57. [Google Scholar]
- Wang, J.; Liu, Y.; Liu, N.; Gao, M.; Yuan, H. Paraneoplastic Immunoglobulin A Nephropathy in a Patient with Lung Adenocarcinoma: A Case Report and Literature Review. J. Int. Med. Res. 2021, 49. [Google Scholar] [CrossRef]
- Godley, P.A.; Ataga, K.I. Renal Cell Carcinoma. Curr. Opin. Oncol. 2000, 12, 260–264. [Google Scholar] [CrossRef] [PubMed]
- Bacchetta, J.; Juillard, L.; Cochat, P.; Droz, J.P. Paraneoplastic Glomerular Diseases and Malignancies. Crit. Rev. Oncol. Hematol. 2009, 70, 39–58. [Google Scholar] [CrossRef] [PubMed]
- Brown, A.M.; Lally, E.T.; Frankel, A.; Harwick, R.; Davis, L.W.; Rominger, C.J. The Association of the IGA Levels of Serum and Whole Saliva with the Progression of Oral Cancer. Cancer 1975, 35, 1154–1162. [Google Scholar] [CrossRef] [PubMed]
- Sanathkumar, H.; Thirumalvalavan, K.; Raj, T.; Srinivasaprasad, N.; Sujith, S.; Fernando, E. Association of IgA Nephropathy with Squamous Cell Carcinoma of the Tongue: Case Report and Review of Literature. Indian J. Nephrol. 2021, 31, 290–292. [Google Scholar] [CrossRef]
- Cambier, J.F.; Ronco, P. Onco-Nephrology: Glomerular Diseases with Cancer. Clin. J. Am. Soc. Nephrol. 2012, 7, 1701–1712. [Google Scholar] [CrossRef] [PubMed]
- Saeidi, K. Myeloproliferative Neoplasms: Current Molecular Biology and Genetics. Crit. Rev. Oncol. Hematol. 2016, 98, 375–389. [Google Scholar] [CrossRef]
- Said, S.M.; Leung, N.; Sethi, S.; Cornell, L.D.; Fidler, M.E.; Grande, J.P.; Herrmann, S.; Tefferi, A.; D’Agati, V.D.; Nasr, S.H. Myeloproliferative Neoplasms Cause Glomerulopathy. Kidney Int. 2011, 80, 753–759. [Google Scholar] [CrossRef]
- Büyükpamukçu, M.; Hazar, V.; Tinaztepe, K.; Bakkaloğlu, A.; Akyüz, C.; Kutluk, T. Hodgkin’s Disease and Renal Paraneoplastic Syndromes in Childhood. Turk. J. Pediatr. 2000, 42, 109–114. [Google Scholar]
- De Samblanx, H.; Verhoef, G.; Zachée, P.; Vandenberghe, P. A Male with Angioimmunoblastic T-Cell Lymphoma and Proliferative Glomerulonephritis. Ann. Hematol. 2004, 83, 455–459. [Google Scholar] [CrossRef]
- Dervisoglu, E.; Akturk, A.S.; Yildiz, K.; Kiran, R.; Yilmaz, A. The Spectrum of Renal Abnormalities in Patients with Psoriasis. Int. Urol. Nephrol. 2012, 44, 509–514. [Google Scholar] [CrossRef]
- Farhi, D.; Ingen-Housz-Oro, S.; Ducret, F.; Rioux-Leclercq, N.; Cam, G.; Simon, P.; Martinez, F.; Fumeron, C.; Dubertret, L.; Blanchet-Bardon, C. Recessive Dystrophic Epidermolysis Bullosa (Hallopeau-Siemens) with IgA Nephropathy: 4 Cases. Ann. Dermatol. Venereol. 2004, 131, 963–967. [Google Scholar] [CrossRef] [PubMed]
- Ahmadi, J.; Antaya, R. Successful Peritoneal Dialysis in a Patient with Recessive Dystrophic Epidermolysis Bullosa. Pediatr. Dermatol. 2007, 24, 589–590. [Google Scholar] [CrossRef]
- Tammaro, F.; Calabrese, R.; Aceto, G.; Lospalluti, L.; Garofalo, L.; Bonifazi, E.; Piccolo, T.; Pannarale, G.; Penza, R. End-Stage Renal Disease Secondary to IgA Nephropathy in Recessive Dystrophic Epidermolysis Bullosa: A Case Report. Pediatr. Nephrol. 2008, 23, 141–144. [Google Scholar] [CrossRef] [PubMed]
- Mantoo, M.R.; Tripathy, S.K.; Phulware, R.H.; Bagri, N.K.; Hari, P.; Barwad, A. Juvenile Dermatomyositis with IgA Nephropathy: Case-Based Review. Rheumatol. Int. 2019, 39, 577–581. [Google Scholar] [CrossRef] [PubMed]
- Pouria, S.; Feehally, J. Glomerular IgA Deposition in Liver Disease. Nephrol. Dial. Transplant. 1999, 14, 2279–2282. [Google Scholar] [CrossRef]
- Arora, A.; Porwal, Y.C.; Malik, R.; Lall, B. Secondary IgA Nephropathy Presenting as Nephrotic Syndrome with Acute Renal Failure in a Case of Alcoholic Liver Cirrhosis. Indian J. Med. Spec. 2017, 8, 89–91. [Google Scholar] [CrossRef]
- Oygen, S.; Alper, A. A Case of Secondary IgA Nephropathy. J. Investig. Med. 2022, 70, 636–637. [Google Scholar]
- Gouet, D.; Fort, E.; Roblot, P.; Maréchaud, R.; Sudre, Y.; Touchard, G. Glomerulopathy with Mesangial IgA Deposits in Primary Hemochromatosis. La Rev. Med. Interne 1987, 8, 311–312. [Google Scholar] [CrossRef]
- Han, J.S.; Lim, S.D.; Choi, W.H.; Hong, S.C.; Park, J.H.; Park, E.; Hong, M.J.; Lee, C.I.; Park, J.H.; Lee, J.H.; et al. Association of Acute Tubular Necrosis with Gross Hematuria in Cirrhosis-Related Immunoglobulin A Nephropathy. Kidney Res. Clin. Pract. 2013, 32, 43–46. [Google Scholar] [CrossRef][Green Version]
- Francisco, S.; Wall, B.M.; Cooke, C.R. Immunoglobulin A Nephropathy in a Renal Allograft of a Black Transplant Recipient. Am. J. Nephrol. 1992, 12, 121–125. [Google Scholar] [CrossRef]
- Singhal, J.; Sharma, J. IgA Nephropathy Secondary to Liver Disease. Pediatr. Nephrol. 2018, 33, 2393. [Google Scholar] [CrossRef]
- Knoppova, B.; Reily, C.; Maillard, N.; Rizk, D.V.; Moldoveanu, Z.; Mestecky, J.; Raska, M.; Renfrow, M.B.; Julian, B.A.; Novak, J. The Origin and Activities of IgA1-Containing Immune Complexes in IgA Nephropathy. Front. Immunol. 2016, 7, 117. [Google Scholar] [CrossRef] [PubMed]
- Albillos, A.; Lario, M.; Álvarez-Mon, M. Cirrhosis-Associated Immune Dysfunction: Distinctive Features and Clinical Relevance. J. Hepatol. 2014, 61, 1385–1396. [Google Scholar] [CrossRef]
- Yousaf, H.; Bhatt, J.; Wadud, M.H.; Horton, E.; Patel, S.; Sarguroh, T.A. Bloody Tubules: Is It the Warfarin? J. Am. Soc. Nephrol. 2020, 31, 836. [Google Scholar]
- Di Lernia, V. IgA Nephropathy during Treatment with TNF-Alpha Blockers: Could It Be Predicted? Med. Hypotheses 2017, 107, 12–13. [Google Scholar] [CrossRef]
- Davide, D.; Marta, P.; Antonella, B.; Simone, P.; Loredana, C.; Luigi, B.; Enrico, F. Double Glomerulonephritis in a Patient with Ankylosing Spondylitis Treated with Biologic Agent: Extrarticolar Involvement or Anti-Tumor Necrosis Factor Alpha Injury? A Case-Based Review. Clin. Med. Insights Case Rep. 2020, 13. [Google Scholar] [CrossRef]
- Wei, S.S.; Sinniah, R. Adalimumab (TNF α Inhibitor) Therapy Exacerbates IgA Glomerulonephritis Acute Renal Injury and Induces Lupus Autoantibodies in a Psoriasis Patient. Case Rep. Nephrol. 2013, 2013, 812781. [Google Scholar] [CrossRef] [PubMed]
- Kluger, N.; Du-Thanh, A.; Bessis, D.; Servel, M.F.; Mourad, G. Psoriasis-Associated IgA Nephropathy under Infliximab Therapy. Int. J. Dermatol. 2015, 54, e79–e80. [Google Scholar] [CrossRef]
- Mamlouk, O.; Selamet, U.; Machado, S.; Abdelrahim, M.; Glass, W.F.; Tchakarov, A.; Gaber, L.; Lahoti, A.; Workeneh, B.; Chen, S.; et al. Nephrotoxicity of Immune Checkpoint Inhibitors beyond Tubulointerstitial Nephritis: Single-Center Experience. J. Immunother. Cancer 2019, 7, 2. [Google Scholar] [CrossRef]
- Tanabe, K.; Kanzaki, H.; Wada, T.; Nakashima, Y.; Sugiyama, H.; Okada, H.; Wada, J. Nivolumab-Induced IgA Nephropathy in a Patient with Advanced Gastric Cancer: A Case Report. Medicine 2020, 99, e20464. [Google Scholar] [CrossRef]
- Kishi, S.; Minato, M.; Saijo, A.; Murakami, N.; Tamaki, M.; Matsuura, M.; Murakami, T.; Nagai, K.; Abe, H.; Nishioka, Y.; et al. IgA Nephropathy after Nivolumab Therapy for Postoperative Recurrence of Lung Squamous Cell Carcinoma. Intern. Med. 2018, 57, 1259–1263. [Google Scholar] [CrossRef] [PubMed]
- Jung, K.; Zeng, X.; Bilusic, M. Nivolumab-Associated Acute Glomerulonephritis: A Case Report and Literature Review. BMC Nephrol. 2016, 17, 188. [Google Scholar] [CrossRef] [PubMed]
- Michel, M.; Henri, P.; Vincent, F.B.; Leon, N.; Marcelli, C. Mesangial Immunoglobulin (Ig)A Glomerulonephritis in a Patient with Rheumatoid Arthritis Treated with Abatacept. Jt. Bone Spine 2013, 80, 660–663. [Google Scholar] [CrossRef] [PubMed]
- Chung, E.Y.M.; Chen, J.; Roxburgh, S. A Case Report of Henoch–Schonlein Purpura and IgA Nephropathy Associated with Rivaroxaban. Nephrology 2018, 23, 289–290. [Google Scholar] [CrossRef]
- Li, X.; Cheung, C.Y. Dabigatran Causing Severe Acute Kidney Injury in a Patient with Liver Cirrhosis. CEN Case Rep. 2019, 8, 125–127. [Google Scholar] [CrossRef] [PubMed]
- Trujillo, H.; Sandino, J.; Cavero, T.; Caravaca-Fontán, F.; Gutiérrez, E.; Sevillano, Á.M.; Shabaka, A.; Fernández-Juárez, G.; Rodríguez Doyágüez, P.; Gimena Muñoz, R.; et al. IgA Nephropathy Is the Most Common Underlying Disease in Patients with Anticoagulant-Related Nephropathy. Kidney Int. Rep. 2022, 7, 831–840. [Google Scholar] [CrossRef]
- Ishii, H.; Hirai, K.; Yanai, K.; Kitano, T.; Shindo, M.; Miyazawa, H.; Ito, K.; Ueda, Y.; Kaku, Y.; Hoshino, T.; et al. Warfarin-Related Nephropathy with Acute Kidney Injury in a Patient with Immunoglobulin A Nephropathy. CEN Case Rep. 2018, 7, 198–203. [Google Scholar] [CrossRef]
- Yahata, M.; Nakaya, I.; Sakuma, T.; Sato, H.; Aoki, S.; Soma, J. Immunoglobulin A Nephropathy with Massive Paramesangial Deposits Caused by Anti-Vascular Endothelial Growth Factor Therapy for Metastatic Rectal Cancer: A Case Report and Review of the Literature. BMC Res. Notes 2013, 6, 450. [Google Scholar] [CrossRef]
- Winters, M.J.; Hurley, R.M.; Lirenman, D.S. ANCA-Positive Glomerulonephritis and IgA Nephropathy in a Patient on Propylthiouracil. Pediatr. Nephrol. 2002, 17, 257–260. [Google Scholar] [CrossRef]
- Ronco, P.; Rovin, B.H.; Adler, S.G.; Barratt, J.; Bridoux, F.; Burdge, K.A.; Mao Chan, T.; Terence Cook, H.; Fervenza, F.C.; Gibson, K.L.; et al. Clinical Practice Guideline for the Management of Glomerular Diseases. Kidney Int. 2021, 100, 115–127. [Google Scholar] [CrossRef]


{kind=link}
| Primary Disease | IgAN Phenotype | No. of Case Reports | Introduced Treatment | Response to Treatment | References |
|---|---|---|---|---|---|
| Crohn’s disease | subnephrotic proteinuria, microscopic hematuria | 6 | mesalazine, prednisolone, AZA, infliximab; ileum resection | remission | Terasaka et al. [23] |
| subnephrotic proteinuria, microscopic hematuria | mesalazine, loperamide, deflazacort, cyclophosphamide → AZA → mycophenolate sodium; right hemicolectomy | AZA caused bone marrow suppression; after four months of treatment with mycophenolate sodium and deflazacort, renal functions were maintained | Choi et al. [24] | ||
| nephrotic proteinuria, gross hematuria | mesalazine, methylprednisolone, adalimumab (potentially triggered IgAN), vedolizumab | remission | Mertelj et al. [25] | ||
| subnephrotic proteinuria, microscopic hematuria | infliximab → ustekinumab (UST) due to therapy-resistant diarrhea and bloody stools (UST potentially triggered IgAN), prednisolone, methylprednisolone, losartan | improvement | Kanazawa et al. [26] | ||
| gross hematuria | oral steroids, right hemicolectomy, and resection of the terminal ileum | IgAN improvement only after surgery | Forshaw et al. [27] | ||
| subnephrotic proteinuria, gross hematuria | methylprednisolone, AZA | improvement | Pipili et al. [28] | ||
| Ulcerative colitis | subnephrotic proteinuria, microscopic hematuria | 4 | metoprolol, methimazole (potentially triggered IgAN and ANCA-vasculitis), prednisone, mesalazine; intravenous steroids | improvement | Ku et al. [29] |
| subnephrotic proteinuria, microscopic hematuria | sulfasalazine: IgA-associated nephropathy required no medication | improvement | Iida et al. [30] | ||
| subnephrotic proteinuria, gross hematuria | resection of ileorectal pouch; IgA-associated nephropathy required no medication | improvement of UC and IgAN; hematuria and proteinuria gradually decreased without IgAN therapy | Onime et al. [31] | ||
| gross hematuria | mesalazine | improvement, microscopic hematuria persisted | Trimarchi et al. [22] | ||
| Celiac disease | nephrotic proteinuria, microscopic hematuria | 5 | large doses of furosemide and metolazone; gluten-free diet | improvement | Woodrow et al. [32] |
| nephrotic proteinuria | ACE inhibitor, oral iron; gluten-free diet | remission | Habura et al. [33] | ||
| nephrotic proteinuria, microscopic hematuria | enalapril, valsartan, prednisone, azathioprine → mycophenolate; gluten-free diet | improvement | Koivuviita et al. [34] | ||
| subnephrotic proteinuria | ramipril, prednisolone, mycophenolate sodium, dapsone; gluten-free diet | initial improvement after a gluten-free diet; six months later: proteinuria relapse, dermatitis herpetiformis development, septicemia leading to death | Gupta et al. [35] | ||
| subnephrotic proteinuria, microscopic hematuria | gluten-free diet | improvement | La Villa et al. [36] | ||
| C. difficile colitis | subnephrotic proteinuria, gross hematuria | 1 | vancomycin; methylprednisolone, cyclophosphamide | remission | Gaughan et al. [37] |
| HIV infection | subnephrotic proteinuria, microscopic hematuria | 5 | raltegravir, abacavir, lamivudine, pulse following oral steroid therapy; tonsillectomy | improvement | Kawakita et al. [38] |
| nephrotic proteinuria, gross hematuria | the patient refused antiretroviral therapy, prednisone | improvement | Hsieh et al. [39] | ||
| nephrotic proteinuria, microscopic hematuria | didanosine, captopril | improvement | Gorriz et al. [40] | ||
| subnephrotic proteinuria, microscopic hematuria | methylprednisolone | improvement: proteinuria and microscopic hematuria persisted | Jindal et al. [41] | ||
| nephrotic proteinuria, microscopic hematuria | antiretroviral therapy, 3x methylprednisolone pulses, oral prednisolone therapy; tonsillectomy | improvement | Miyasato et al. [42] | ||
| Psoriasis | proteinuria, hematuria | 6 | secukinumab, tonsillectomy | remission | Ochi et al. [43] |
| proteinuria, microscopic hematuria, | infliximab | remission | Sakellariou et al. [44] | ||
| proteinuria, hematuria | infliximab, methotrexate, cyclosporin | improvement | |||
| nephrotic syndrome, microscopic hematuria | diuretics, antihypertensive, hemodialysis, cyclophosphamide, steroids | improvement | Manchanda et al. [45] | ||
| proteinuria, gross hematuria | steroids, tonsillectomy, IL17-α inhibitor | improvement | Segawa et al. [46] | ||
| nephrotic proteinuria | prednisone | improvement | Zadrazil et al. [47] | ||
| Dystrophic epidermolysis bullosa—recessive | rapidly progressive GN | 1 | steroids in the pre-dialysis period, then dialysis and kidney transplantation | deteriorated to ESRD (steroid-resistant GN) | Ceuppens et al. [48] |
| Epidermolysis bullosa—dominant | proteinuria, hematuria | 1 | steroids, mizoribine, dilazep dihydrochloride, warfarin | improvement | Kawasaki et al. [49] |
| Non-Herlitz junctional epidermolysis bullosa | rapidly progressive GN, nephrotic proteinuria | 1 | unknown | deteriorated to ESRD, kidney transplant performed | Ungureanu et al. [50] |
| Alcoholic cirrhosis | (a), (b) proteinuria and hematuria | 4 | steroids | (a), (b) proteinuria resolved | Takada et al. [51] |
| (a) rapidly progressive nephritic syndrome, gross hematuria (b) subnephrotic proteinuria | (a) bilateral tonsillectomy, steroids, mizoribine (b) steroids and mizoribine | (a) resolution of hematuria, proteinuria, improvement of renal function (b) proteinuria and serum creatinine decreased | Kaneko et al. [52] | ||
| Wilson’s Disease | microscopic hematuria, proteinuria, renal dysfunction | 2 | trientere HCl, zinc acetate | renal manifestations improved | Shimamura et al. [53] |
| proteinuria, gross hematuria | D-penicillamine | hematuria resolved; proteinuria reduced | Bhandari et al. [54] | ||
| Hemochromatosis | proteinuria, gross hematuria | 1 | steroids | improvement in renal function; however, due to a cerebral hemorrhage, steroids were discontinued; cardiopulmonary arrest 10 days later | Nakayama et al. [55] |
| Hepatitis | GFR decline | 5 | conservation management, sofosbuvir/velpatasvir | improvement | Denha et al. [56] |
| proteinuria | ribavirin, pegylated INF-α | reduction of proteinuria | Dey et al. [57] | ||
| proteinuria, hematuria | ribavirin and INF- α | resolution | Ji et al. [58] | ||
| (a) proteinuria, macroscopic hematuria (b) microscopic hematuria | (a) methylprednisolone, polyene phosphatidylcholine, ursodeoxycholic acid, methotrexate (b) methylprednisolone, methotrexate | (a) progression stopped (b) persistence of microscopic hematuria | Chen et al. [59] | ||
| Sjorgen syndrome | nephrotic syndrome, microscopic hematuria, vasculitis | 1 | glucocorticoids and treatment of local symptoms (ocular and oral dryness); hemodialysis | despite receiving hemodialysis, the patient’s renal function showed no improvement | Tsai et al. [60] |
| Spondyloarthritis | subnephrotic proteinuria, microscopic hematuria | 1 | irbesartan | renal function and proteinuria remained stable | Jacquet et al. [61] |
| Renal cell carcinoma | subnephrotic proteinuria, microscopic hematuria | 3 | nephrectomy | after nephrectomy, proteinuria and hematuria were decreased or resolved | Mimura et al. [62] |
| Gastric adenocarcinoma | nephrotic syndrome, microscopic hematuria | 1 | methylprednisolone, losartan | improvement | Kocyigit et al. [63] |
| Hodgkin’s lymphoma | hematuria, elevated creatinine | 1 | chemotherapy | after 8th cycle of chemotherapy, renal function improved; however, patient died due to ARDS | Yoo et al. [64] |
| Silicosis | nephrotic proteinuria, gross hematuria | 1 | steroids, ACE inhibitors | improvement | Chen et al. [65] |
| Silica exposure ANCA-associated vasculitis | subnephrotic proteinuria, gross hematuria | 1 | steroids, cyclophosphamide | improvement | Rao et al. [66] |
| Henoch–Schönlein purpura | nephrotic proteinuria, microscopic hematuria | 1 | PA | after 4th PA, creatinine levels were stable | Lee et al. [67] |
| MRSA infection | nephrotic proteinuria, gross hematuria | 1 | vancomycin, rifampin, ciprofloxacin, linezolid | improvement | Riley et al. [68] |
| MSSA infection | nephrotic proteinuria, no hematuria | 1 | methylprednisolone | improvement | Javed et al. [69] |
| M. pneumoniae infection | subnephrotic proteinuria, gross hematuria | 2 | erythromycin | remission | Kanayama et al. [70] |
| subnephrotic proteinuria, gross hematuria | minocyclin, steroids, furosemide, catecholamine, clarithromycin | improvement | Suzuki et al. [71] | ||
| Lyme disease | new proteinuria, gross hematuria | 1 | steroids, doxycycline | improvement | McCausland et al. [72] |
| Cat scratch disease | subnephrotic proteinuria, gross hematuria | 1 | amoxicillin/clavulanic acid, azithromycin, rifampin | improvement | Hopp et al. [73] |
| Osteomyelitis | subnephrotic proteinuria, microscopic hematuria | 1 | amputation | improvement | Tevlin et al. [74] |
| Tonsillitis | hematuria | 1 | tonsillectomy | remission | Liess et al. [75] |
| Malaria | subnephrotic proteinuria, microscopic hematuria | 1 | quinine dihydrochloride, doxycycline, hemodialysis | improvement | Yoo et al. [76] |
| Schistosomiasis | nephrotic proteinuria, no hematuria | 1 | losartan, atenolol | improvement | Gonçalves et al. [77] |
| Medication | Primary Disease/Diseases | IgAN Phenotype | Suggested Treatment | Remission after Withdrawal | Reference |
|---|---|---|---|---|---|
| TNF-α inhibitors | |||||
| Infliximab | ankylosing spondylitis | nephrotic proteinuria, microscopic hematuria | steroids, ACE inhibitors | partial remission | Diena et al. [137] |
| Infliximab | pustular psoriasis | subnephrotic proteinuria, gross hematuria | steroids, secukinumab, bilateral tonsillectomy | partial remission | Segawa et al. [46] |
| Infliximab | psoriasis, peripheral arthritis | subnephrotic proteinuria, microscopic hematuria | ACE inhibitors, ustekinumab | partial remission | Kluger et al. [139] |
| Adalimumab | plaque psoriasis | subnephrotic proteinuria, microscopic hematuria | steroids, amlodipine candesartan + hydrochlorothiazide lincosa | remission | Wei et al. [138] |
| Immune checkpoint inhibitors | |||||
| Pembrolizumab | HT, GERD, asthma | no proteinuria, 2 RBC/HPF | steroids, mycophenolate mofetil, infliximab | partial remission | Mamlouk et al. [140] |
| Nivolumab + Ipilimumab | HT, GERD, CKD stage 3. | nephrotic proteinuria 11 RBC/HPF | steroids | remission | Mamlouk et al. [140] |
| Nivolumab | lung squamous cell carcinoma | subnephrotic proteinuria, gross hematuria | N.D. | partial remission | Kishi et al. [142] |
| Nivolumab | gastric cancer, portal thrombosis, DM type 2. | nephrotic proteinuria, gross hematuria | steroids | partial remission | Tanabe et al. [141] |
| Nivolumab | metastatic clear cell renal cell carcinoma | subnephrotic proteinuria, gross hematuria | steroids, hemodialysis | partial remission | Jung et al. [143] |
| CTLA4-Ig | |||||
| Abatacept | rheumatoid arthritis | subnephrotic proteinuria, microscopic hematuria | steroids | partial remission | Michel et al. [144] |
| Oral anticoagulants | |||||
| Dabigatran | HT, alcoholic liver cirrhosis paroxysmal atrial fibrillation | subnephrotic proteinuria, gross hematuria | vitamin K, hemodialysis, steroids | remission | Li et al. [146] |
| Rivaroxaban | pulmonary emboli, DVT | nephrotic proteinuria, microscopic hematuria | apixaban ramipril | partial remission | Chung et al. [145] |
| Warfarin | Marfan syndrome, aortic valve regurgitation | subnephrotic proteinuria | infusion of extracellular fluid solution | partial remission | Ishii et al. [148] |
| IL-12/IL-23-inhibitor | |||||
| Ustekinumab | Crohn’s disease | subnephrotic proteinuria, microscopic hematuria | steroids losartan | partial remission | Kanazawa et al. [26] |
| Anti-vascular endothelial growth factor | |||||
| Bevacizumab | metastatic rectal cancer | nephrotic proteinuria, microscopic hematuria | cessation of bevacizumab | improvement | Yahata et al. [149] |
| Thioureylene derivative | |||||
| Propylthiouracil | Graves’ disease | nephrotic proteinuria, microscopic hematuria | prednisolone, cyclophosphamide, fish oil (Maxepa), enalapril | improvement | Winters et al. [150] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tota, M.; Baron, V.; Musial, K.; Derrough, B.; Konieczny, A.; Krajewska, M.; Turkmen, K.; Kusztal, M. Secondary IgA Nephropathy and IgA-Associated Nephropathy: A Systematic Review of Case Reports. J. Clin. Med. 2023, 12, 2726. https://doi.org/10.3390/jcm12072726
Tota M, Baron V, Musial K, Derrough B, Konieczny A, Krajewska M, Turkmen K, Kusztal M. Secondary IgA Nephropathy and IgA-Associated Nephropathy: A Systematic Review of Case Reports. Journal of Clinical Medicine. 2023; 12(7):2726. https://doi.org/10.3390/jcm12072726
Chicago/Turabian StyleTota, Maciej, Vanessa Baron, Katie Musial, Bouchra Derrough, Andrzej Konieczny, Magdalena Krajewska, Kultigin Turkmen, and Mariusz Kusztal. 2023. "Secondary IgA Nephropathy and IgA-Associated Nephropathy: A Systematic Review of Case Reports" Journal of Clinical Medicine 12, no. 7: 2726. https://doi.org/10.3390/jcm12072726
APA StyleTota, M., Baron, V., Musial, K., Derrough, B., Konieczny, A., Krajewska, M., Turkmen, K., & Kusztal, M. (2023). Secondary IgA Nephropathy and IgA-Associated Nephropathy: A Systematic Review of Case Reports. Journal of Clinical Medicine, 12(7), 2726. https://doi.org/10.3390/jcm12072726