

.png)
Preventive Effect of Local Lidocaine Administration on the Formation of Traumatic Neuroma

 , ,
, , {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Materials and Methods
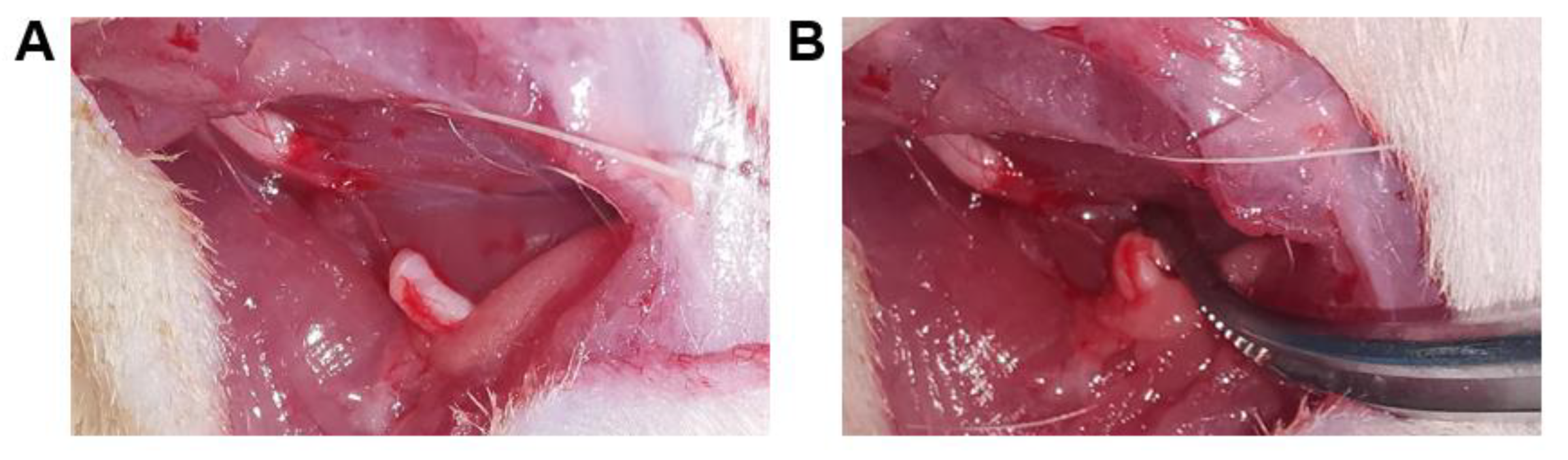
2.1. Animal and Surgical Procedures
2.2. Behavioral Testing
2.3. Quantitative Real-Time PCR
2.4. Histological Evaluation
2.5. Statistical Analysis
3. Results
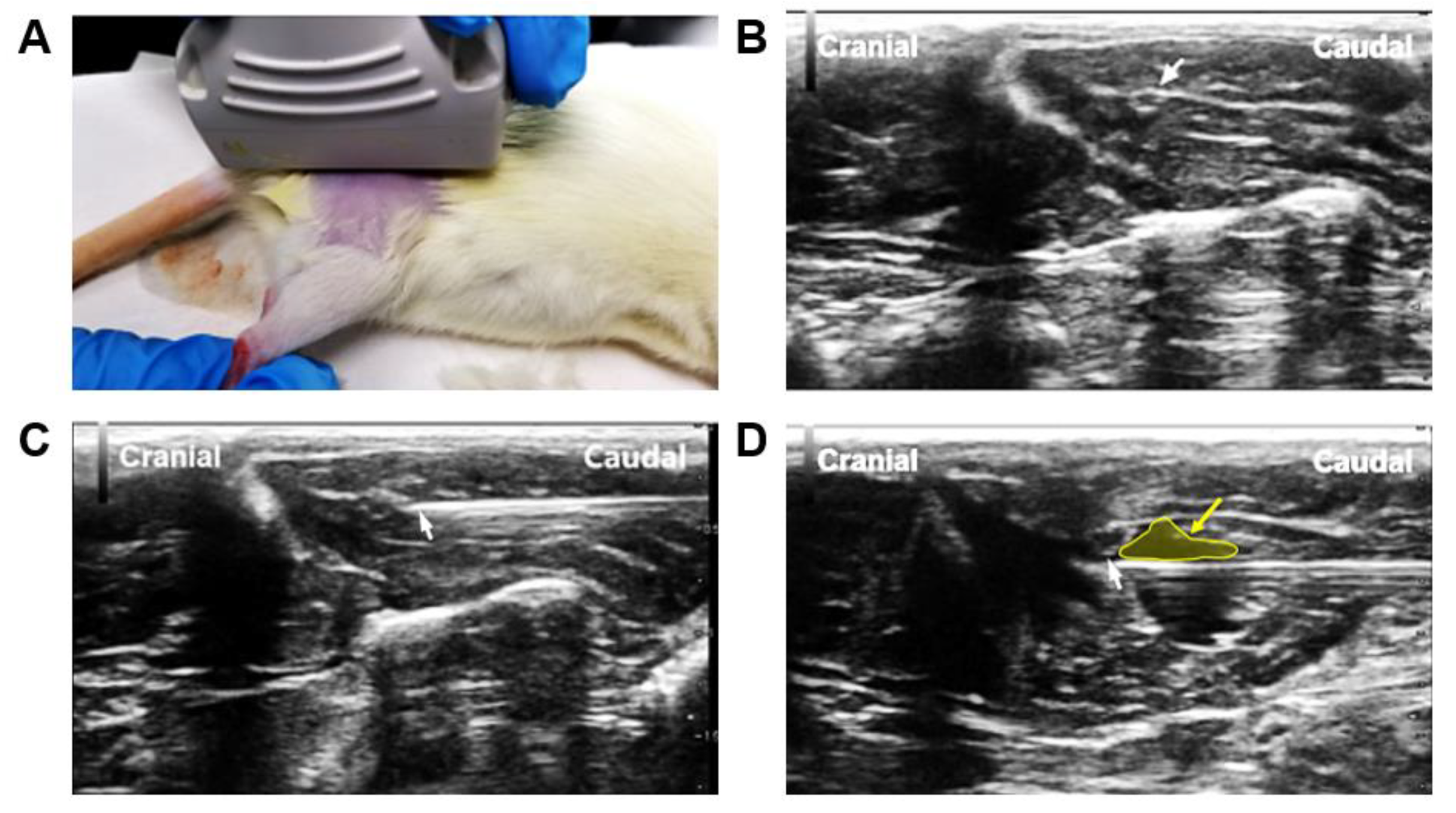
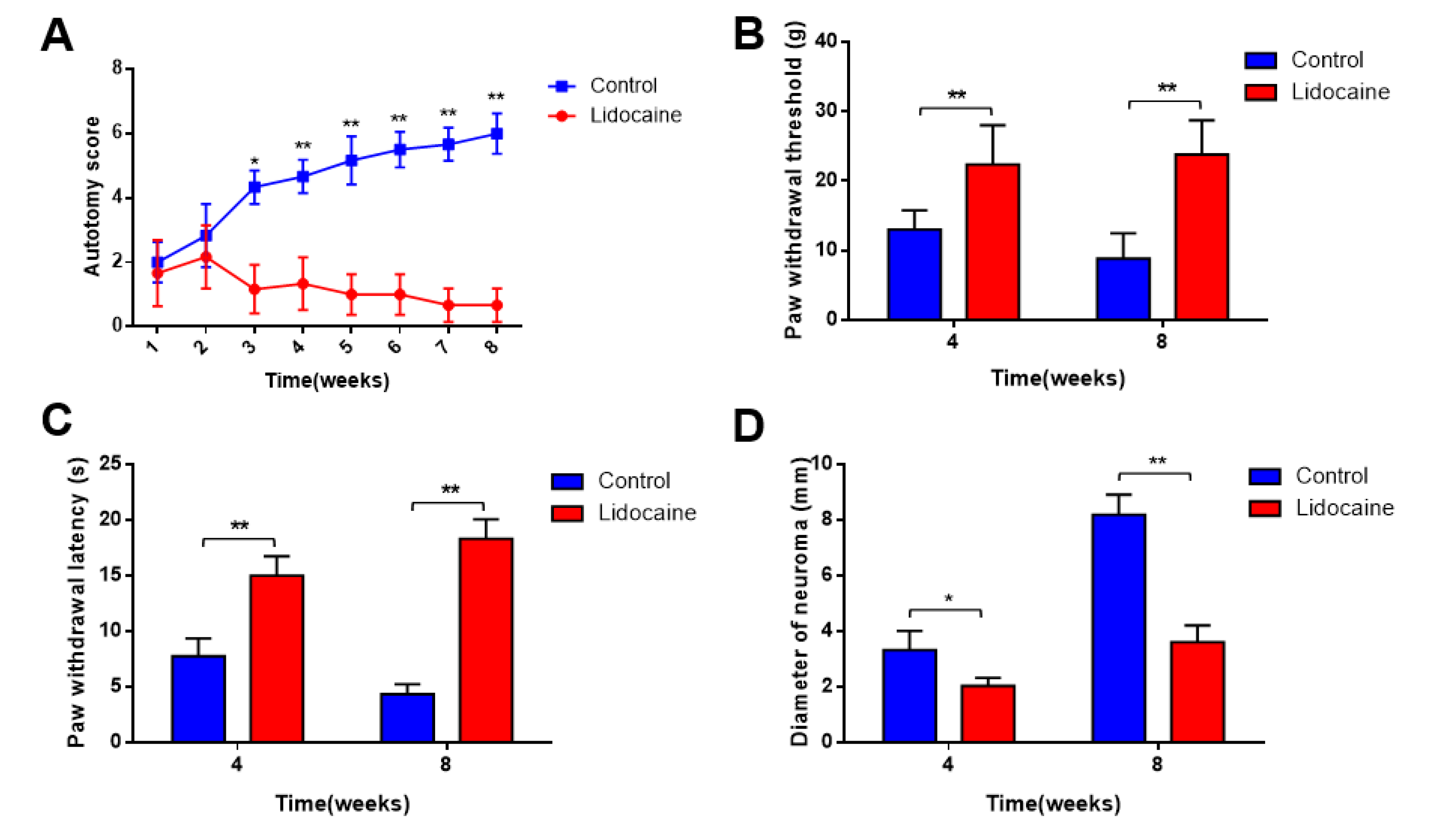
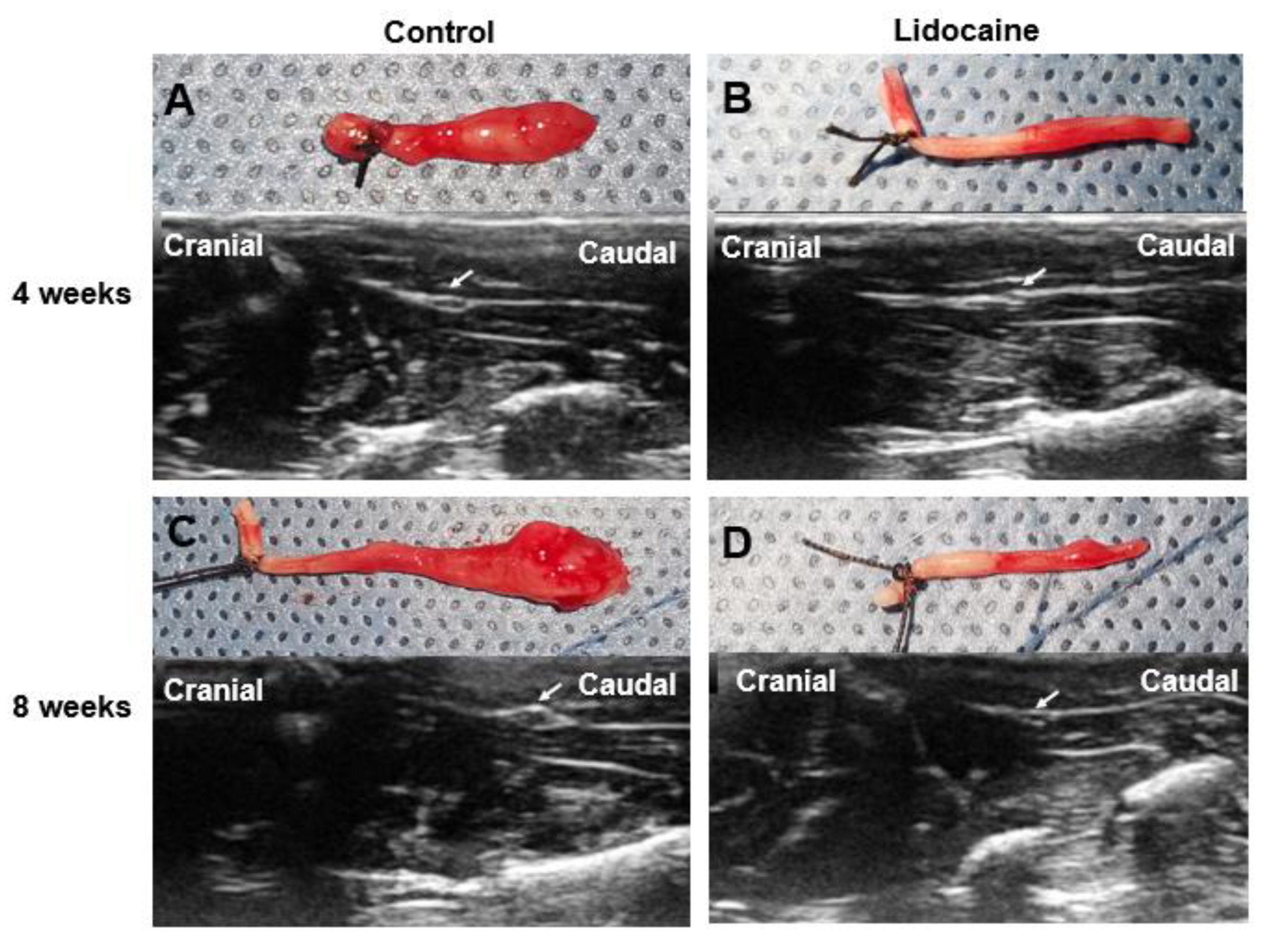
3.1. Assessment of Pain and Neuroma Formation
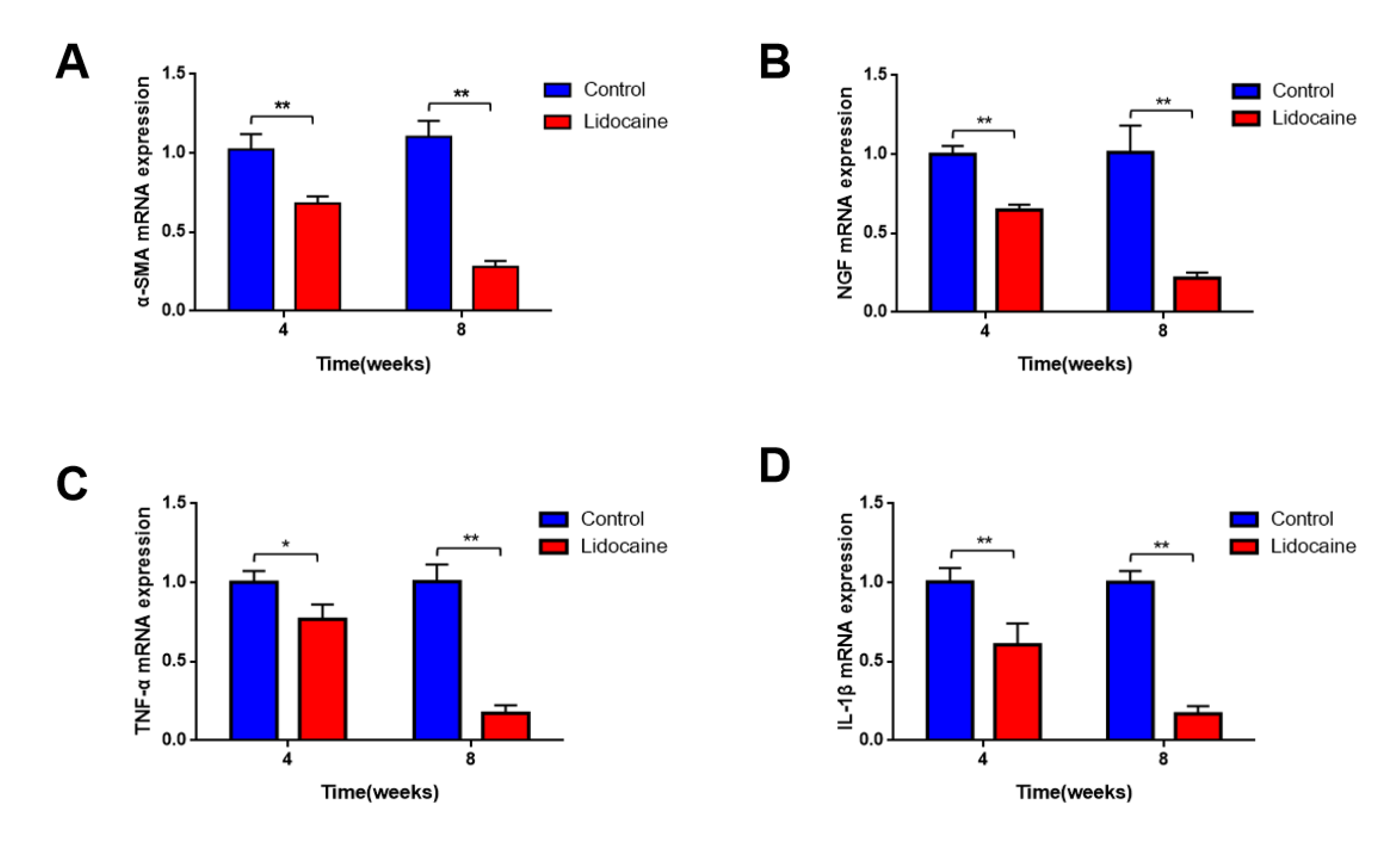
3.2. Expression of Neuroma and Pain-Related Markers
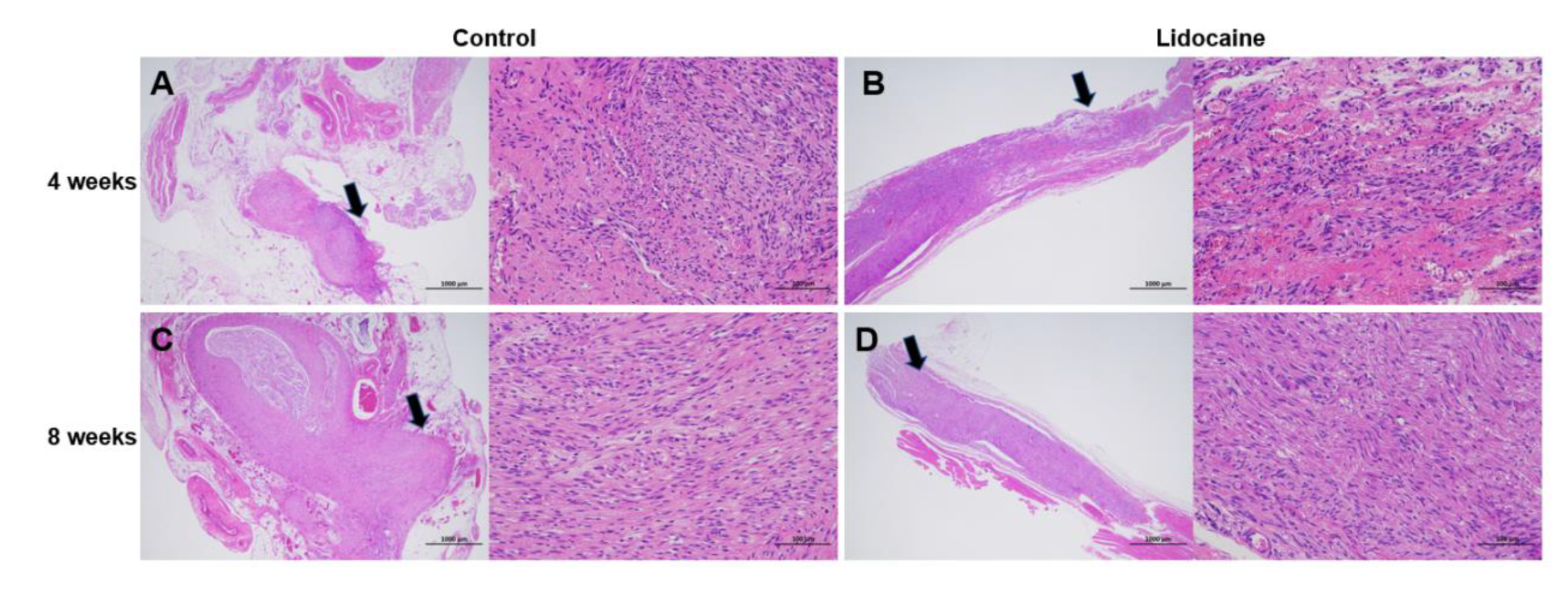
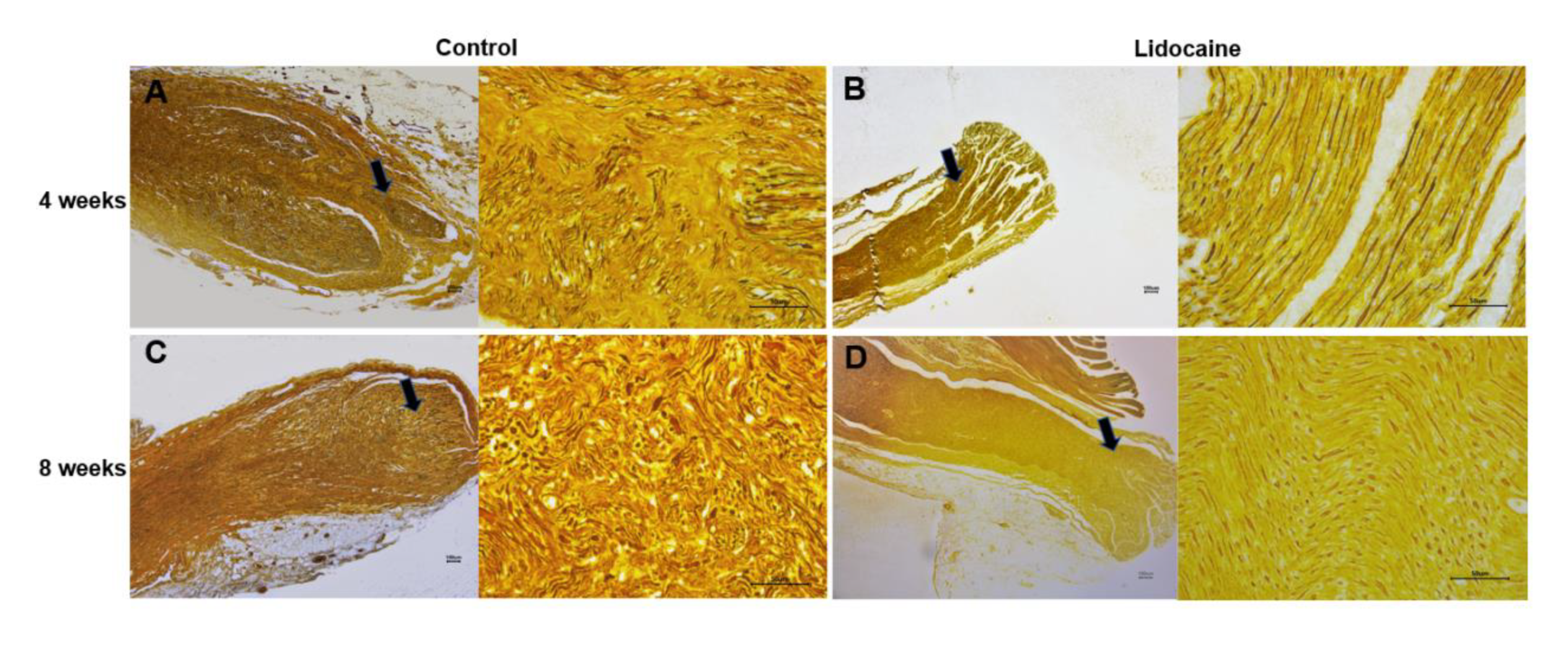
3.3. Histological Evaluation
3.3.1. Formation of Traumatic Neuroma
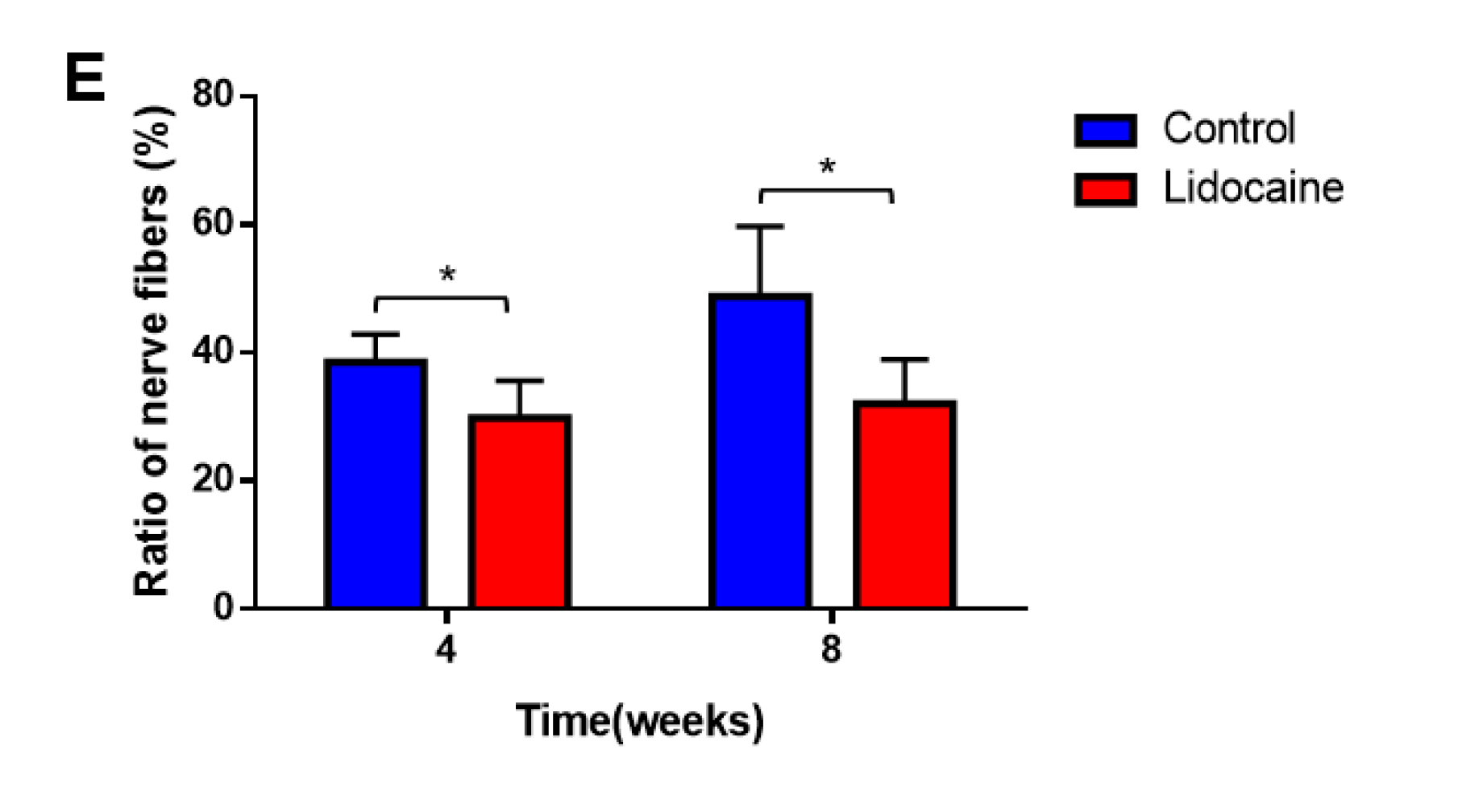
3.3.2. Nerve Fibers
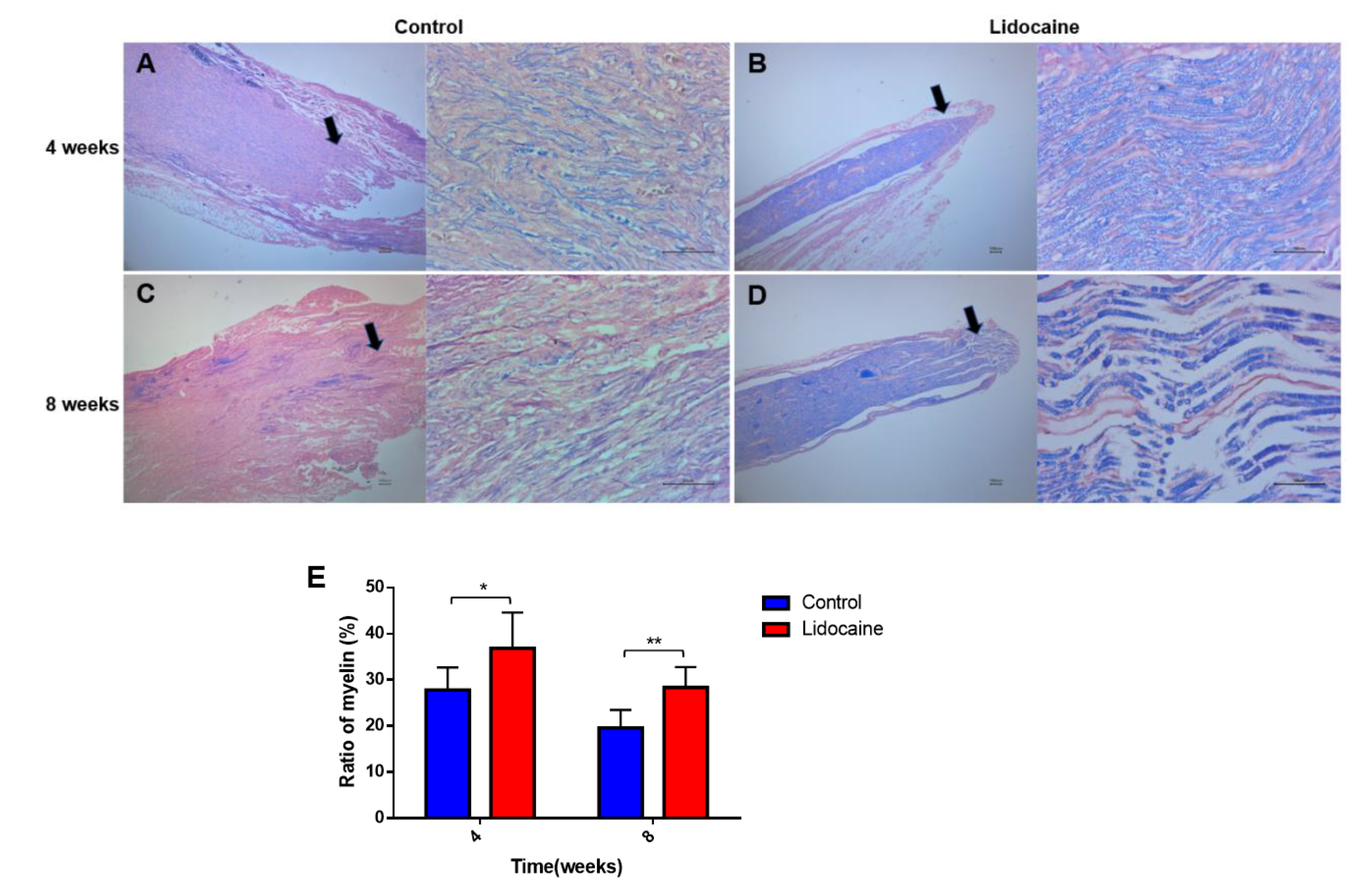
3.3.3. Demyelination
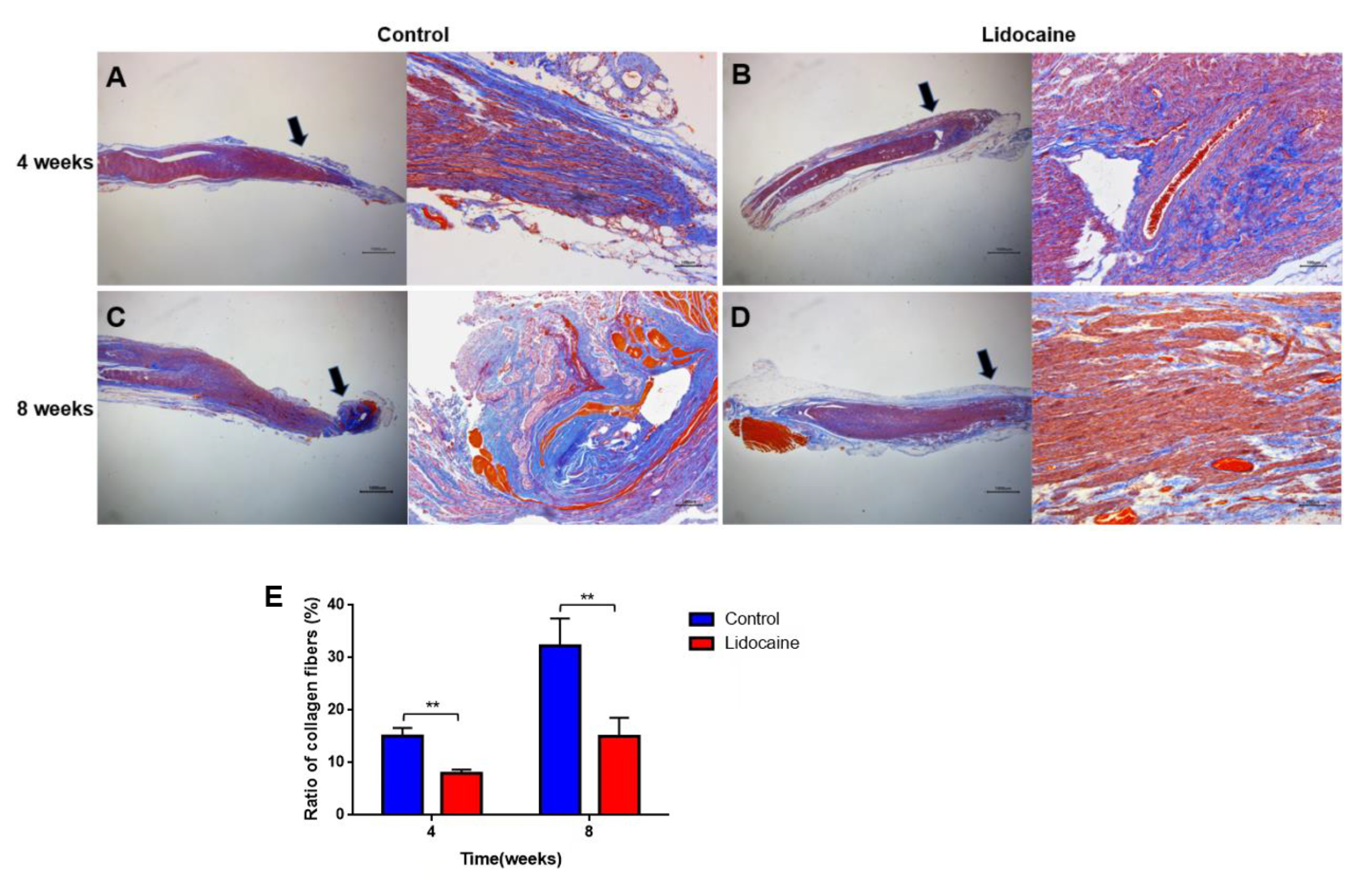
3.3.4. Collagen Hyperplasia and Deposition
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bora, F.W.J.; Pleasure, D.E.; Didizian, N.A. A study of nerve regeneration and neuroma formation after nerve suture by various techniques. J. Hand Surg. 1976, 1, 138–143. [Google Scholar] [CrossRef] [PubMed]
- Yan, H.; Zhang, F.; Kolkin, J.; Wang, C.; Xia, Z.; Fan, C. Mechanisms of nerve capping technique in prevention of painful neuroma formation. PLoS ONE 2014, 9, e93973. [Google Scholar] [CrossRef] [PubMed]
- Oliveira, K.M.C.; Pindur, L.; Han, Z.; Bhavsar, M.B.; Barker, J.H.; Leppik, L. Time course of traumatic neuroma development. PLoS ONE 2018, 13, e0200548. [Google Scholar] [CrossRef] [PubMed]
- Powers, C.J.; Friedman, A.H. A brief history of surgery for peripheral nerve sheath tumors. Neurosurg. Focus 2007, 22, E1. [Google Scholar] [CrossRef] [PubMed]
- Stokvis, A.; Coert, J.H.; van Neck, J.W. Insufficient pain relief after surgical neuroma treatment: Prognostic factors and central sensitisation. J. Plast. Reconstr. Aesthetic Surg. JPRAS 2010, 63, 1538–1543. [Google Scholar] [CrossRef]
- Yi, J.; Jiang, N.; Li, B.; Yan, Q.; Qiu, T.; Iyer, K.S.; Yin, Y.; Dai, H.; Yetisen, A.K.; Li, S. Painful Terminal Neuroma Prevention by Capping PRGD/PDLLA Conduit in Rat Sciatic Nerves. Adv. Sci. (Weinh. Baden-Wurtt. Ger.) 2018, 5, 1700876. [Google Scholar] [CrossRef]
- Galeano, M.; Manasseri, B.; Risitano, G.; Geuna, S.; Di Scipio, F.; La Rosa, P.; Delia, G.; D’Alcontres, F.S.; Colonna, M.R. A free vein graft cap influences neuroma formation after nerve transection. Microsurgery 2009, 29, 568–572. [Google Scholar] [CrossRef]
- Poppler, L.H.; Parikh, R.P.; Bichanich, M.J.; Rebehn, K.; Bettlach, C.R.; Mackinnon, S.E.; Moore, A.M. Surgical interventions for the treatment of painful neuroma: A comparative meta-analysis. Pain 2018, 159, 214–223. [Google Scholar] [CrossRef]
- Pet, M.A.; Ko, J.H.; Friedly, J.L.; Mourad, P.D.; Smith, D.G. Does targeted nerve implantation reduce neuroma pain in amputees? Clin. Orthop. Relat. Res. 2014, 472, 2991–3001. [Google Scholar] [CrossRef]
- Attal, N.; Rouaud, J.; Brasseur, L.; Chauvin, M.; Bouhassira, D. Systemic lidocaine in pain due to peripheral nerve injury and predictors of response. Neurology 2004, 62, 218–225. [Google Scholar] [CrossRef]
- Viola, V.; Newnham, H.H.; Simpson, R.W. Treatment of intractable painful diabetic neuropathy with intravenous lignocaine. J. Diabetes Its Complicat. 2006, 20, 34–39. [Google Scholar] [CrossRef]
- Tremont-Lukats, I.W.; Hutson, P.R.; Backonja, M.-M. A randomized, double-masked, placebo-controlled pilot trial of extended IV lidocaine infusion for relief of ongoing neuropathic pain. Clin. J. Pain 2006, 22, 266–271. [Google Scholar] [CrossRef]
- Hermanns, H.; Hollmann, M.W.; Stevens, M.F.; Lirk, P.; Brandenburger, T.; Piegeler, T.; Werdehausen, R. Molecular mechanisms of action of systemic lidocaine in acute and chronic pain: A narrative review. Br. J. Anaesth. 2019, 123, 335–349. [Google Scholar] [CrossRef]
- Kirillova, I.; Teliban, A.; Gorodetskaya, N.; Grossmann, L.; Bartsch, F.; Rausch, V.H.; Struck, M.; Tode, J.; Baron, R.; Jänig, W. Effect of local and intravenous lidocaine on ongoing activity in injured afferent nerve fibers. Pain 2011, 152, 1562–1571. [Google Scholar] [CrossRef]
- Xiao, W.H.; Bennett, G.J. C-fiber spontaneous discharge evoked by chronic inflammation is suppressed by a long-term infusion of lidocaine yielding nanogram per milliliter plasma levels. Pain 2008, 137, 218–228. [Google Scholar] [CrossRef]
- Takatori, M.; Kuroda, Y.; Hirose, M. Local Anesthetics Suppress Nerve Growth Factor-Mediated Neurite Outgrowth by Inhibition of Tyrosine Kinase Activity of TrkA. Anesth. Analg. 2006, 102, 462–467. [Google Scholar] [CrossRef]
- Zhang, J.-M.; Li, H.; Munir, M.A. Decreasing sympathetic sprouting in pathologic sensory ganglia: A new mechanism for treating neuropathic pain using lidocaine. Pain 2004, 109, 143–149. [Google Scholar] [CrossRef]
- Staal, R.; Khayrullina, T.; Christensen, R.; Hestehave, S.; Zhou, H.; Cajina, M.; Nattini, M.E.; Gandhi, A.; Fallon, S.M.; Schmidt, M.; et al. P2X7 receptor-mediated release of microglial prostanoids and miRNAs correlates with reversal of neuropathic hypersensitivity in rats. Eur. J. Pain (Lond. Engl.) 2022, 26, 1304–1321. [Google Scholar] [CrossRef]
- Pandit, J.J.; McGuire, N. Unlicensed intravenous lidocaine for postoperative pain: Always a safer “licence to stop” than to start. Anaesthesia 2021, 76, 156–160. [Google Scholar] [CrossRef]
- Miclescu, A.; Schmelz, M.; Gordh, T. Differential analgesic effects of subanesthetic concentrations of lidocaine on spontaneous and evoked pain in human painful neuroma: A randomized, double blind study. Scand. J. Pain 2015, 8, 37–44. [Google Scholar] [CrossRef]
- Lee, F.C.; Singh, H.; Nazarian, L.N.; Ratliff, J.K. High-resolution ultrasonography in the diagnosis and intraoperative management of peripheral nerve lesions. J. Neurosurg. 2011, 114, 206–211. [Google Scholar] [CrossRef] [PubMed]
- Chiou, H.J.; Chou, Y.H.; Chiou, S.Y.; Liu, J.B.; Chang, C.Y. Peripheral nerve lesions: Role of high-resolution US. Radiographics 2003, 23, e15. [Google Scholar] [CrossRef] [PubMed]
- Nazarian, L.N. The top 10 reasons musculoskeletal sonography is an important complementary or alternative technique to MRI. AJR Am. J. Roentgenol. 2008, 190, 1621–1626. [Google Scholar] [CrossRef] [PubMed]
- Mackinnon, S.E.; Dellon, A.L.; Hudson, A.R.; Hunter, D.A. Alteration of neuroma formation by manipulation of its microenvironment. Plast. Reconstr. Surg. 1985, 76, 345–353. [Google Scholar] [CrossRef] [PubMed]
- Yan, H.; Gao, W.; Pan, Z. The expression of α-SMA in the painful traumatic neuroma: Potential role in the pathobiology of neuropathic pain. J. Neurotrauma 2012, 29, 2791–2797. [Google Scholar] [CrossRef]
- Desmoulière, A.; Redard, M.; Darby, I.; Gabbiani, G. Apoptosis mediates the decrease in cellularity during the transition between granulation tissue and scar. Am. J. Pathol. 1995, 146, 56–66. [Google Scholar]
- Koplovitch, P.; Devor, M. Dilute lidocaine suppresses ectopic neuropathic discharge in dorsal root ganglia without blocking axonal propagation: A new approach to selective pain control. Pain 2018, 159, 1244–1256. [Google Scholar] [CrossRef]
- März, P.; Heese, K.; Dimitriades-Schmutz, B.; Rose-John, S.; Otten, U. Role of interleukin-6 and soluble IL-6 receptor in region-specific induction of astrocytic differentiation and neurotrophin expression. Glia 1999, 26, 191–200. [Google Scholar] [CrossRef]
- Woolf, C.J.; Allchorne, A.; Safieh-Garabedian, B.; Poole, S. Cytokines, nerve growth factor and inflammatory hyperalgesia: The contribution of tumour necrosis factor alpha. Br. J. Pharmacol. 1997, 121, 417–424. [Google Scholar] [CrossRef]
- Wynn, T.A.; Ramalingam, T.R. Mechanisms of fibrosis: Therapeutic translation for fibrotic disease. Nat. Med. 2012, 18, 1028–1040. [Google Scholar] [CrossRef]
- Joo, J.D.; Choi, J.W.; In, J.H.; Jung, H.S.; Lee, J.A.; Kim, Y.S.; Kim, D.W.; Yeom, J.H.; Shin, E.Y.; Jeon, Y.S. Lidocaine suppresses the increased extracellular signal-regulated kinase/cyclic AMP response element-binding protein pathway and pro-inflammatory cytokines in a neuropathic pain model of rats. Eur. J. Anaesthesiol. EJA 2011, 28, 106–111. [Google Scholar] [CrossRef]
- Lahat, A.; Ben-Horin, S.; Lang, A.; Fudim, E.; Picard, O.; Chowers, Y. Lidocaine down-regulates nuclear factor-kappaB signalling and inhibits cytokine production and T cell proliferation. Clin. Exp. Immunol. 2008, 152, 320–327. [Google Scholar] [CrossRef]
- Mirsky, R.; Jessen, K.R. The neurobiology of Schwann cells. Brain Pathol. (Zur. Switz.) 1999, 9, 293–311. [Google Scholar] [CrossRef]
- Rogister, B.; Delrée, P.; Leprince, P.; Martin, D.; Sadzot, C.; Malgrange, B.; Munaut, C.; Rigo, J.M.; Lefebvre, P.P.; Octave, J.N. Transforming growth factor beta as a neuronoglial signal during peripheral nervous system response to injury. J. Neurosci. Res. 1993, 34, 32–43. [Google Scholar] [CrossRef]
- Bentov, I.; Damodarasamy, M.; Spiekerman, C.; Reed, M.J. Lidocaine Impairs Proliferative and Biosynthetic Functions of Aged Human Dermal Fibroblasts. Anesth. Analg. 2016, 123, 616–623. [Google Scholar] [CrossRef]










Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ji, F.; Zhang, Y.; Cui, P.; Li, Y.; Li, C.; Du, D.; Xu, H. Preventive Effect of Local Lidocaine Administration on the Formation of Traumatic Neuroma. J. Clin. Med. 2023, 12, 2476. https://doi.org/10.3390/jcm12072476
Ji F, Zhang Y, Cui P, Li Y, Li C, Du D, Xu H. Preventive Effect of Local Lidocaine Administration on the Formation of Traumatic Neuroma. Journal of Clinical Medicine. 2023; 12(7):2476. https://doi.org/10.3390/jcm12072476
Chicago/Turabian StyleJi, Feng, Yongyan Zhang, Peng Cui, Ying Li, Caixia Li, Dongping Du, and Hua Xu. 2023. "Preventive Effect of Local Lidocaine Administration on the Formation of Traumatic Neuroma" Journal of Clinical Medicine 12, no. 7: 2476. https://doi.org/10.3390/jcm12072476
APA StyleJi, F., Zhang, Y., Cui, P., Li, Y., Li, C., Du, D., & Xu, H. (2023). Preventive Effect of Local Lidocaine Administration on the Formation of Traumatic Neuroma. Journal of Clinical Medicine, 12(7), 2476. https://doi.org/10.3390/jcm12072476