
Time-Varying Risk Factors for Incident Fractures in Kidney Transplant Recipients: A Nationwide Cohort Study in South Korea
 , , , and
, , , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population and Data Collection
2.2. Comparison of Clinical Characteristics and Cumulative Incidence of Fractures
2.3. Statistical Analysis
3. Results
3.1. Patient Characteristics at Baseline
3.2. Patient Characteristics at 6 Months Post-Transplantation
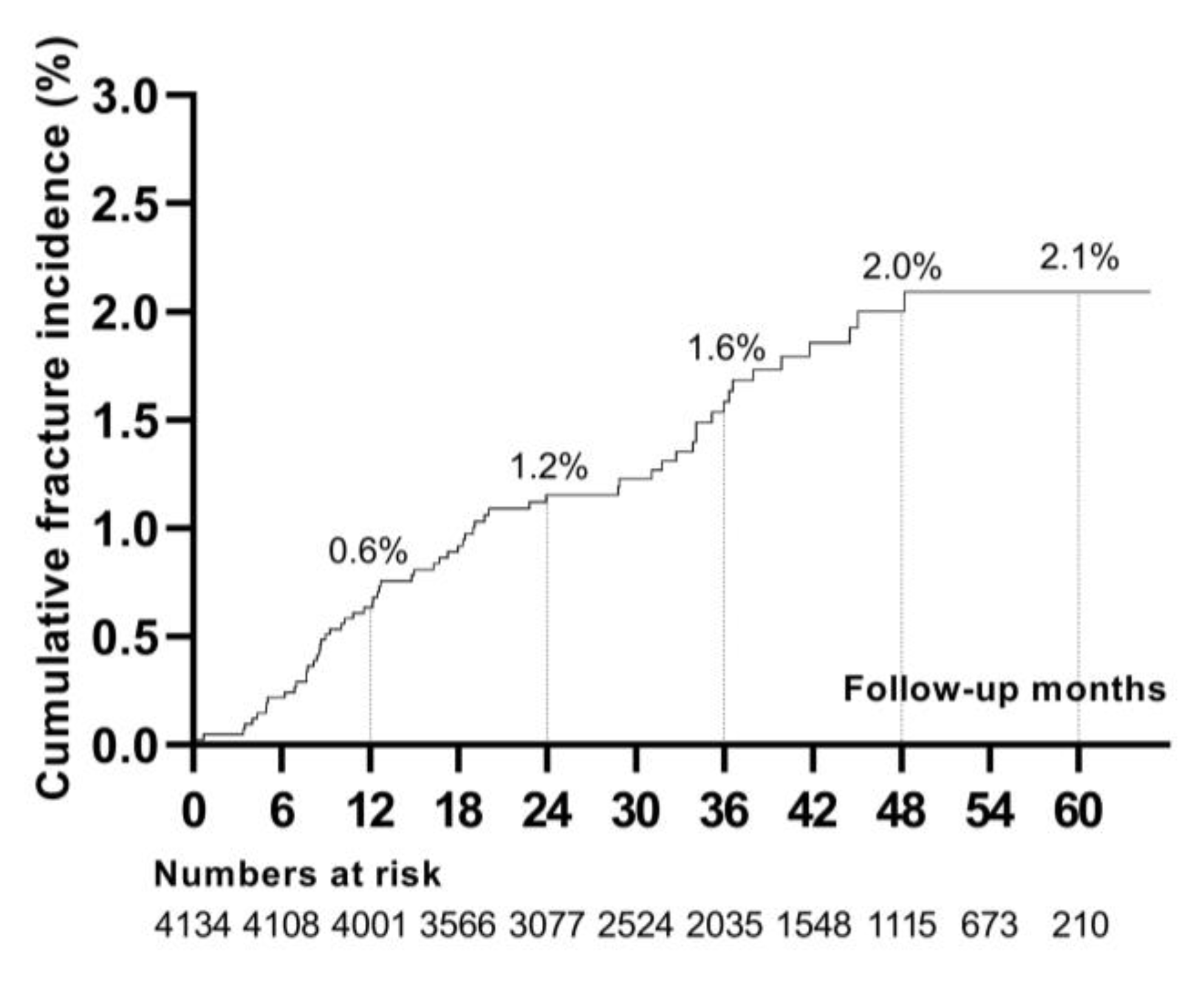
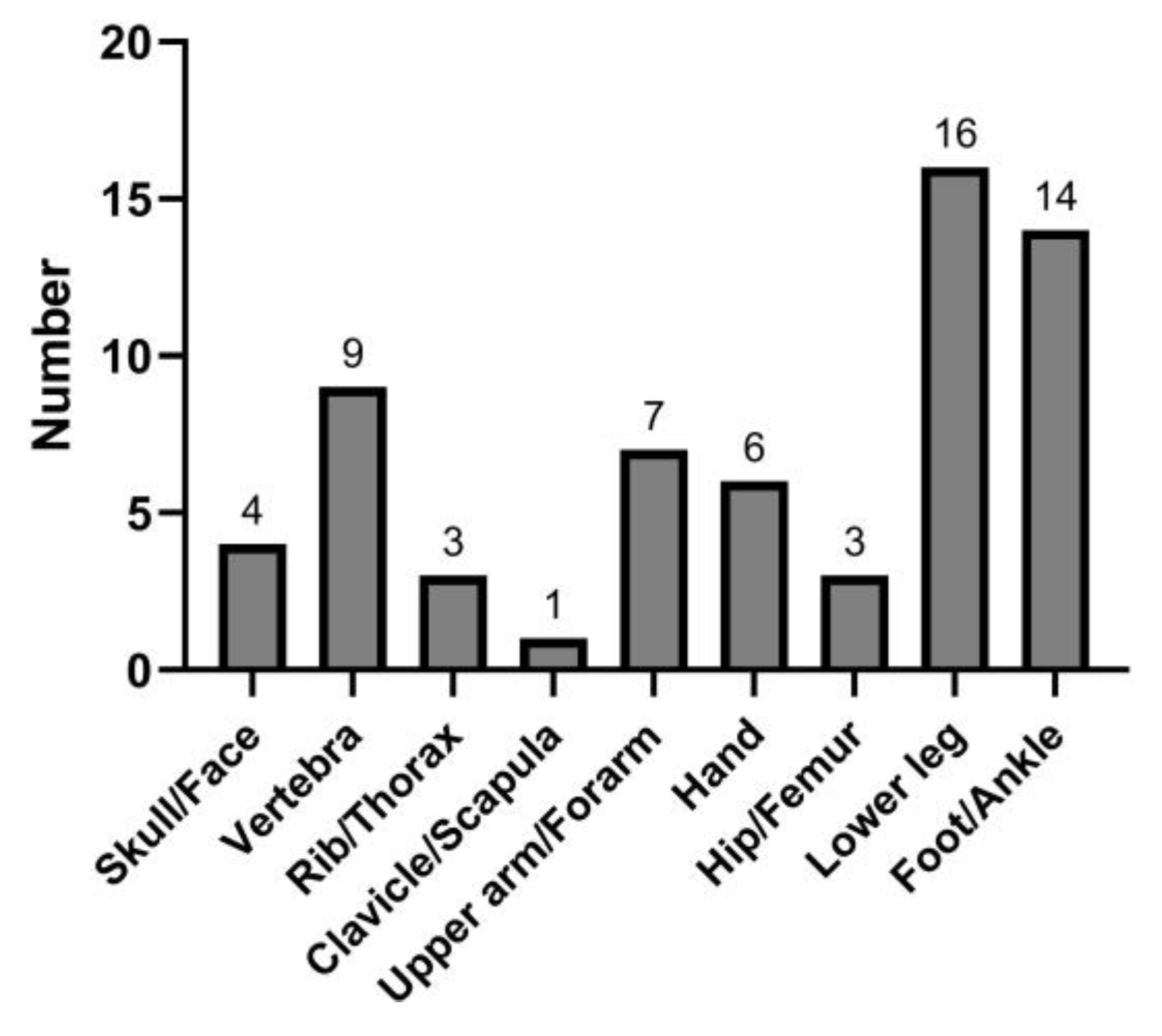
3.3. Fracture Incidence and Location
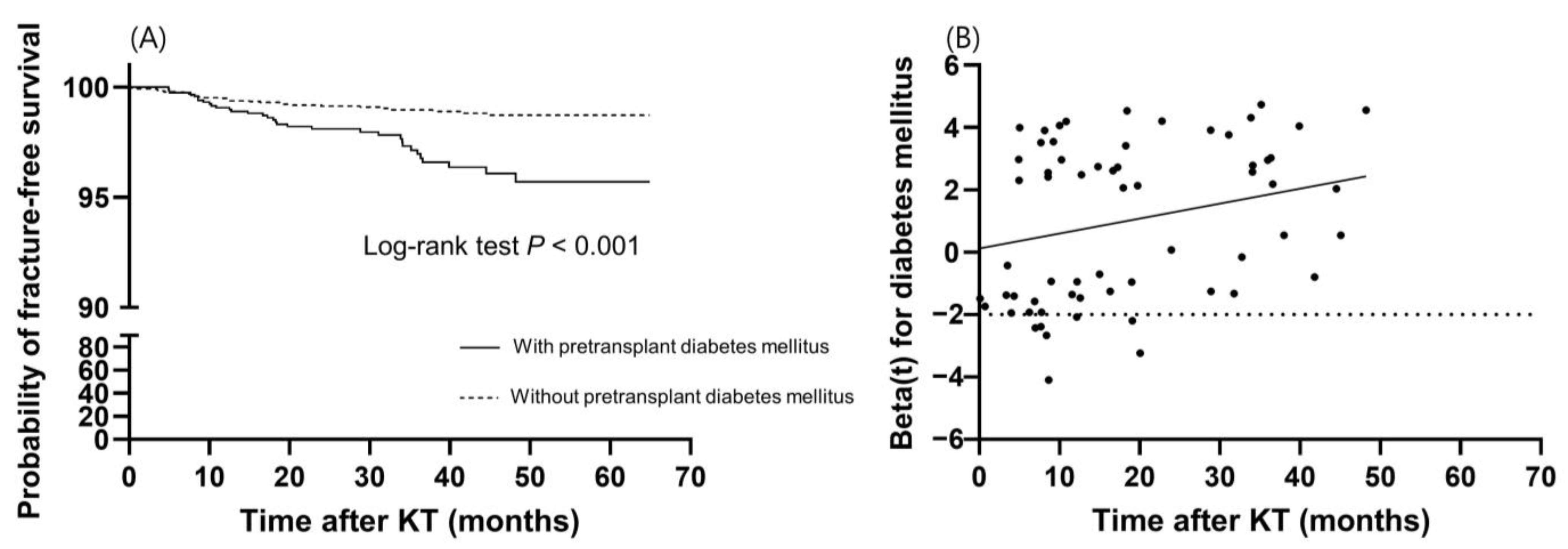
3.4. Predictors of Incident Fractures
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hansen, D.; Olesen, J.B.; Gislason, G.H.; Abrahamsen, B.; Hommel, K. Risk of fracture in adults on renal replacement therapy: A Danish national cohort study. Nephrol. Dial. Transpl. 2016, 31, 1654–1662. [Google Scholar] [CrossRef]
- Ball, A.M.; Gillen, D.L.; Sherrard, D.; Weiss, N.S.; Emerson, S.S.; Seliger, S.L.; Kestenbaum, B.R.; Stehman-Breen, C. Risk of hip fracture among dialysis and renal transplant recipients. JAMA 2002, 288, 3014–3018. [Google Scholar] [CrossRef] [PubMed]
- Nam, Y.J.; Hwang, S.Y.; Kim, D.W.; Kim, D.; Shin, S.J.; Yoon, H.E. Sex-specific relationship between vascular calcification and incident fracture in patients with end-stage renal disease. Kidney Res. Clin. Pract. 2020, 39, 344–355. [Google Scholar] [CrossRef]
- Bouquegneau, A.; Salam, S.; Delanaye, P.; Eastell, R.; Khwaja, A. Bone Disease after Kidney Transplantation. Clin. J. Am. Soc. Nephrol. 2016, 11, 1282–1296. [Google Scholar] [CrossRef]
- Naylor, K.L.; Li, A.H.; Lam, N.N.; Hodsman, A.B.; Jamal, S.A.; Garg, A.X. Fracture risk in kidney transplant recipients: A systematic review. Transplantation 2013, 95, 1461–1470. [Google Scholar] [CrossRef] [PubMed]
- Iseri, K.; Carrero, J.J.; Evans, M.; Felländer-Tsai, L.; Berg, H.E.; Runesson, B.; Stenvinkel, P.; Lindholm, B.; Qureshi, A.R. Fractures after kidney transplantation: Incidence, predictors, and association with mortality. Bone 2020, 140, 115554. [Google Scholar] [CrossRef] [PubMed]
- Dekker, F.W.; de Mutsert, R.; van Dijk, P.C.; Zoccali, C.; Jager, K.J. Survival analysis: Time-dependent effects and time-varying risk factors. Kidney Int. 2008, 74, 994–997. [Google Scholar] [CrossRef]
- Levey, A.S.; Stevens, L.A.; Schmid, C.H.; Zhang, Y.L.; Castro, A.F., 3rd; Feldman, H.I.; Kusek, J.W.; Eggers, P.; Van Lente, F.; Greene, T.; et al. A new equation to estimate glomerular filtration rate. Ann. Intern. Med. 2009, 150, 604–612. [Google Scholar] [CrossRef]
- Nikkel, L.E.; Hollenbeak, C.S.; Fox, E.J.; Uemura, T.; Ghahramani, N. Risk of fractures after renal transplantation in the United States. Transplantation 2009, 87, 1846–1851. [Google Scholar] [CrossRef]
- Mackey, D.C.; Lui, L.Y.; Cawthon, P.M.; Bauer, D.C.; Nevitt, M.C.; Cauley, J.A.; Hillier, T.A.; Lewis, C.E.; Barrett-Connor, E.; Cummings, S.R. High-trauma fractures and low bone mineral density in older women and men. JAMA 2007, 298, 2381–2388. [Google Scholar] [CrossRef]
- Zhang, Z.; Reinikainen, J.; Adeleke, K.A.; Pieterse, M.E.; Groothuis-Oudshoorn, C.G.M. Time-varying covariates and coefficients in Cox regression models. Ann. Transl. Med. 2018, 6, 121. [Google Scholar] [CrossRef] [PubMed]
- Abbott, K.C.; Oglesby, R.J.; Hypolite, I.O.; Kirk, A.D.; Ko, C.W.; Welch, P.G.; Agodoa, L.Y.; Duncan, W.E. Hospitalizations for fractures after renal transplantation in the United States. Ann. Epidemiol. 2001, 11, 450–457. [Google Scholar] [CrossRef] [PubMed]
- Nair, S.S.; Lenihan, C.R.; Montez-Rath, M.E.; Lowenberg, D.W.; Chertow, G.M.; Winkelmayer, W.C. Temporal trends in the incidence, treatment and outcomes of hip fracture after first kidney transplantation in the United States. Am. J. Transpl. 2014, 14, 943–951. [Google Scholar] [CrossRef] [PubMed]
- Castro-Alonso, C.; D’Marco, L.; Pomes, J.; Del Amo Conill, M.; García-Diez, A.I.; Molina, P.; Puchades, M.J.; Valdivielso, J.M.; Escudero, V.; Bover, J.; et al. Prevalence of Vertebral Fractures and Their Prognostic Significance in the Survival in Patients with Chronic Kidney Disease Stages 3–5 Not on Dialysis. J. Clin. Med. 2020, 9, 1604. [Google Scholar] [CrossRef] [PubMed]
- Salter, M.L.; Liu, X.; Bae, S.; Chu, N.M.; Miller Dunham, A.; Humbyrd, C.; Segev, D.L.; McAdams-DeMarco, M.A. Fractures and Subsequent Graft Loss and Mortality among Older Kidney Transplant Recipients. J. Am. Geriatr. Soc. 2019, 67, 1680–1688. [Google Scholar] [CrossRef]
- Naylor, K.L.; Jamal, S.A.; Zou, G.; McArthur, E.; Lam, N.N.; Leslie, W.D.; Hodsman, A.B.; Kim, S.J.; Knoll, G.A.; Fraser, L.A.; et al. Fracture Incidence in Adult Kidney Transplant Recipients. Transplantation 2016, 100, 167–175. [Google Scholar] [CrossRef]
- Nikkel, L.E.; Mohan, S.; Zhang, A.; McMahon, D.J.; Boutroy, S.; Dube, G.; Tanriover, B.; Cohen, D.; Ratner, L.; Hollenbeak, C.S.; et al. Reduced fracture risk with early corticosteroid withdrawal after kidney transplant. Am. J. Transpl. 2012, 12, 649–659. [Google Scholar] [CrossRef]
- Ramsey-Goldman, R.; Dunn, J.E.; Dunlop, D.D.; Stuart, F.P.; Abecassis, M.M.; Kaufman, D.B.; Langman, C.B.; Salinger, M.H.; Sprague, S.M. Increased risk of fracture in patients receiving solid organ transplants. J. Bone Miner. Res. 1999, 14, 456–463. [Google Scholar] [CrossRef]
- Sprague, S.M.; Belozeroff, V.; Danese, M.D.; Martin, L.P.; Olgaard, K. Abnormal bone and mineral metabolism in kidney transplant patients-a review. Am. J. Nephrol. 2008, 28, 246–253. [Google Scholar] [CrossRef]
- Fusaro, M.; Cosmai, L.; Evenepoel, P.; Nickolas, T.L.; Cheung, A.M.; Aghi, A.; Tripepi, G.; Plebani, M.; Iervasi, G.; Vettor, R.; et al. Vitamin K and Kidney Transplantation. Nutrients 2020, 12, 2717. [Google Scholar] [CrossRef]
- Evenepoel, P.; Claes, K.; Meijers, B.; Laurent, M.; Bammens, B.; Naesens, M.; Sprangers, B.; Pottel, H.; Cavalier, E.; Kuypers, D. Poor Vitamin K Status is Associated with Low Bone Mineral Density and Increased Fracture Risk in End-Stage Renal Disease. J. Bone Miner. Res. 2019, 34, 262–269. [Google Scholar] [CrossRef] [PubMed]
- Malluche, H.H.; Monier-Faugere, M.C.; Herberth, J. Bone disease after renal transplantation. Nat. Rev. Nephrol. 2010, 6, 32–40. [Google Scholar] [CrossRef]
- Rojas, E.; Carlini, R.G.; Clesca, P.; Arminio, A.; Suniaga, O.; De Elguezabal, K.; Weisinger, J.R.; Hruska, K.A.; Bellorin-Font, E. The pathogenesis of osteodystrophy after renal transplantation as detected by early alterations in bone remodeling. Kidney Int. 2003, 63, 1915–1923. [Google Scholar] [CrossRef] [PubMed]
- Schlosberg, M.; Movsowitz, C.; Epstein, S.; Ismail, F.; Fallon, M.D.; Thomas, S. The effect of cyclosporin A administration and its withdrawal on bone mineral metabolism in the rat. Endocrinology 1989, 124, 2179–2184. [Google Scholar] [CrossRef] [PubMed]
- Kirino, S.; Fukunaga, J.; Ikegami, S.; Tsuboi, H.; Kimata, M.; Nakata, N.; Nakano, M.; Ueno, T.; Mizukawa, N.; Sugahara, T. Regulation of bone metabolism in immunosuppressant (FK506)-treated rats. J. Bone Miner. Metab. 2004, 22, 554–560. [Google Scholar] [CrossRef]
- Singha, U.K.; Jiang, Y.; Yu, S.; Luo, M.; Lu, Y.; Zhang, J.; Xiao, G. Rapamycin inhibits osteoblast proliferation and differentiation in MC3T3-E1 cells and primary mouse bone marrow stromal cells. J. Cell. Biochem. 2008, 103, 434–446. [Google Scholar] [CrossRef]
- Kneissel, M.; Luong-Nguyen, N.H.; Baptist, M.; Cortesi, R.; Zumstein-Mecker, S.; Kossida, S.; O’Reilly, T.; Lane, H.; Susa, M. Everolimus suppresses cancellous bone loss, bone resorption, and cathepsin K expression by osteoclasts. Bone 2004, 35, 1144–1156. [Google Scholar] [CrossRef]
- Iyer, S.P.; Nikkel, L.E.; Nishiyama, K.K.; Dworakowski, E.; Cremers, S.; Zhang, C.; McMahon, D.J.; Boutroy, S.; Liu, X.S.; Ratner, L.E.; et al. Kidney transplantation with early corticosteroid withdrawal: Paradoxical effects at the central and peripheral skeleton. J. Am. Soc. Nephrol. 2014, 25, 1331–1341. [Google Scholar] [CrossRef]
- Vautour, L.M.; Melton, L.J., 3rd; Clarke, B.L.; Achenbach, S.J.; Oberg, A.L.; McCarthy, J.T. Long-term fracture risk following renal transplantation: A population-based study. Osteoporos Int. 2004, 15, 160–167. [Google Scholar] [CrossRef]
- Naylor, K.L.; Zou, G.; Leslie, W.D.; Hodsman, A.B.; Lam, N.N.; McArthur, E.; Fraser, L.A.; Knoll, G.A.; Adachi, J.D.; Kim, S.J.; et al. Risk factors for fracture in adult kidney transplant recipients. World J. Transpl. 2016, 6, 370–379. [Google Scholar] [CrossRef]
- Hong, Y.A.; Ban, T.H.; Kang, C.Y.; Hwang, S.D.; Choi, S.R.; Lee, H.; Jung, H.Y.; Kim, K.; Kwon, Y.E.; Kim, S.H.; et al. Trends in epidemiologic characteristics of end-stage renal disease from 2019 Korean Renal Data System (KORDS). Kidney Res. Clin. Pract. 2021, 40, 52–61. [Google Scholar] [CrossRef] [PubMed]
- Fusaro, M.; Holden, R.; Lok, C.; Iervasi, G.; Plebani, M.; Aghi, A.; Gallieni, M.; Cozzolino, M. Phosphate and bone fracture risk in chronic kidney disease patients. Nephrol. Dial. Transpl. 2021, 36, 405–412. [Google Scholar] [CrossRef] [PubMed]
- Oei, L.; Rivadeneira, F.; Zillikens, M.C.; Oei, E.H. Diabetes, diabetic complications, and fracture risk. Curr. Osteoporos Rep. 2015, 13, 106–115. [Google Scholar] [CrossRef]
- Ziolkowski, S.; Liu, S.; Montez-Rath, M.E.; Denburg, M.; Winkelmayer, W.C.; Chertow, G.M.; O’Shaughnessy, M.M. Association between cause of kidney failure and fracture incidence in a national US dialysis population cohort study. Clin. Kidney J. 2022, 15, 2245–2257. [Google Scholar] [CrossRef]
- Aleksova, J.; Wong, P.; Mulley, W.R.; Choy, K.W.; McLachlan, R.; Ebeling, P.R.; Kerr, P.G.; Milat, F. Serum phosphorus levels and fracture following renal transplantation. Clin. Endocrinol. 2017, 87, 141–148. [Google Scholar] [CrossRef] [PubMed]
- Yuksel, Y.; Yuksel, D.; Yucetin, L.; Erbis, H.; Sarier, M.; Karatas, O.; Emek, M.; Erdogan, M.; Yavuz, A.; Demirbas, A. Use of Tacrolimus During Pregnancy After Kidney Transplantaion. Transpl. Proc. 2019, 51, 2361–2366. [Google Scholar] [CrossRef]
- Edwards, B.J.; Desai, A.; Tsai, J.; Du, H.; Edwards, G.R.; Bunta, A.D.; Hahr, A.; Abecassis, M.; Sprague, S. Elevated incidence of fractures in solid-organ transplant recipients on glucocorticoid-sparing immunosuppressive regimens. J. Osteoporos. 2011, 2011, 591793. [Google Scholar] [CrossRef]
- Cvetkovic, M.; Mann, G.N.; Romero, D.F.; Liang, X.G.; Ma, Y.; Jee, W.S.; Epstein, S. The deleterious effects of long-term cyclosporine A, cyclosporine G, and FK506 on bone mineral metabolism in vivo. Transplantation 1994, 57, 1231–1237. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Total (n = 4134) | No Fracture (n = 4071) | Fracture (n = 63) | p | |
|---|---|---|---|---|
| Recipient age (years) | 49.00 ± 11.50 | 48.92 ± 11.51 | 54.18 ± 9.49 | <0.001 |
| Recipient sex, male (%) | 2447 (59.19) | 2405 (59.08) | 42 (66.67) | 0.224 |
| Donor age (years) | 46.64 ± 13.03 | 46.65 ± 13.03 | 45.87 ± 13.05 | 0.640 |
| Donor sex, male (%) | 2201 (53.24) | 2168 (53.25) | 33 (52.38) | 0.890 |
| Deceased donor (%) | 1533 (37.08) | 1505 (36.97) | 28 (44.44) | 0.223 |
| BMI, kg/m2 | 23.09 ± 3.57 | 23.09 ± 3.57 | 22.92 ± 3.81 | 0.700 |
| Smoking (%) | 935 (22.62) | 920 (22.60) | 15 (23.81) | 0.804 |
| Pretransplant diabetes mellitus (%) | 1197 (28.96) | 1164 (28.59) | 33 (52.38) | <0.001 |
| Hypertension (%) | 3709 (89.72) | 3654 89.76 | 55 (87.30) | 0.516 |
| History of CVD (%) | 429 (10.38) | 419 (10.29) | 10 (15.87) | 0.150 |
| Primary renal disease (%) | 0.003 | |||
| Diabetes | 950 (22.98) | 923 (22.67) | 27 (42.86) | |
| Hypertension | 654 (15.82) | 643 (15.79) | 11 (17.46) | |
| Glomerulonephritis | 1373 (33.21) | 1361 (33.43) | 12 (19.05) | |
| Others | 324 (7.84) | 320 (7.86) | 4 (6.35) | |
| Unknown | 833 (20.15) | 824 (20.24) | 9 (14.29) | |
| RRT before KT | 0.052 | |||
| Hemodialysis (%) | 2943 (71.20) | 2891 (71.01) | 52 (82.54) | |
| Peritoneal dialysis (%) | 523 (12.65) | 517 (12.70) | 6 (9.52) | |
| KT (%) | 54 (1.31) | 52 (1.28) | 2 (3.17) | |
| Preemptive KT (%) | 614 (14.85) | 611 (15.01) | 3 (4.76) | |
| Dialysis vintage (months) | 30.33 (3.87–85.25) | 30.33 (3.84–84.91) | 31.56 (5.80–61.73) | 0.344 |
| Retransplant (%) | 326 (7.89) | 318 (78.11) | 8 (12.70) | 0.153 |
| Mean arterial pressure (mmHg) | 102.16 ± 14.10 | 102.19 ± 14.10 | 100.23 ± 13.74 | 0.270 |
| Hemoglobin (g/dL) | 10.73 ± 1.60 | 10.73 ± 1.60 | 10.78 ± 1.48 | 0.800 |
| Albumin (g/dL) | 3.93 ± 0.52 | 3.93 ± 0.52 | 3.92 ± 0.56 | 0.840 |
| Corrected calcium (mg/dL) | 9.06 ± 0.89 | 9.05 ± 0.90 | 9.11 ± 0.73 | 0.620 |
| Phosphorus (mg/dL) | 5.11 ± 1.54 | 5.11 ± 1.54 | 4.99 ± 1.56 | 0.540 |
| Ca × P product (g2/dL2) | 45.96 ± 14.29 | 45.97 ± 14.28 | 45.43 ± 14.80 | 0.770 |
| Intact PTH (pg/mL) | 245.0 (128.0–407.0) | 246.0 (128.0–408.0) | 138.0 (83.0–316.0) | 0.008 |
| Vitamin D analogs (%) | 730 (17.66) | 722 (17.74) | 8 (12.70) | 0.279 |
| Panel reactive antibody ≥ 50% (%) | 167 (4.04) | 166 (4.08) | 1 (1.59) | 0.319 |
| HLA-DSA (%) | 265 (6.41) | 261 (6.50) | 4 (6.35) | 0.984 |
| Positive cross-match (%) | 218 (5.27) | 215 (5.35) | 3 (4.76) | 0.855 |
| ABO incompatibility (%) | 643 (15.55) | 637 (15.65) | 6 (9.52) | 0.183 |
| Desensitization (%) | 922 (22.30) | 911 (22.68) | 11 (17.46) | 0.352 |
| IL-2 receptor antibody (%) | 3326 (80.45) | 3268 (80.28) | 58 (92.06) | 0.004 |
| ATG (%) | 844 (20.42) | 841 (20.66) | 3 (4.76) | 0.002 |
| Tacrolimus (%) | 3989 (96.49) | 3926 (96.44) | 63 (100.00) | 0.172 |
| Cyclosporine (%) | 134 (3.24) | 134 (3.29) | 0 (0.00) | 0.270 |
| Mycophenolic acid (%) | 3812 (92.21) | 3754 (92.21) | 58 (92.06) | 0.816 |
| mTOR inhibitor (%) | 48 (1.16) | 47 (1.15) | 1 (1.59) | 0.524 |
| Corticosteroid (%) | 4067 (98.38) | 4006 (98.40) | 61 (96.83) | 0.272 |
| Follow-up months | 36.51 (24.23–49.73) | 35.77 (24.07–49.56) | 46.13 (35.40–55.54) | <0.001 |
| Total (n = 4134) | No Fracture (n = 4071) | Fracture (n = 63) | p | |
|---|---|---|---|---|
| Hemoglobin (g/dL) | 12.92 ± 1.80 | 12.93 ± 1.80 | 12.61 ± 1.62 | 0.168 |
| Albumin (g/dL) | 4.27 ± 0.37 | 4.27 ± 0.37 | 4.23 ± 0.34 | 0.376 |
| Corrected calcium (mg/dL) | 9.39 ± 0.74 | 9.39 ± 0.74 | 9.41 ± 0.55 | 0.840 |
| Phosphorus (mg/dL) | 3.23 ± 0.71 | 3.23 ± 0.71 | 3.03 ± 0.66 | 0.024 |
| Ca × P product (g2/dL2) | 30.12 ± 6.07 | 30.15 ± 6.07 | 28.40 ± 5.85 | 0.023 |
| eGFR (mL/min/1.73 m2) | 67.36 ± 20.02 | 67.34 ± 20.03 | 68.99 ± 19.13 | 0.516 |
| Vitamin D analogs (%) | 657 (15.95) | 644 (15.88) | 13 (20.63) | 0.307 |
| Tacrolimus (%) | 3919 (94.80) | 3856(94.72) | 63 (100.00) | 0.077 |
| Tacrolimus dose (mg) | 4.20 ± 2.41 | 4.21 ± 2.42 | 3.64 ± 1.90 | 0.064 |
| Tacrolimus dose per body weight (mg/10 kg) | 0.69 ± 0.42 | 0.69 ± 0.42 | 0.60 ± 0.32 | 0.106 |
| Tacrolimus level (mg/dL) | 6.69 ± 2.52 | 6.68 ± 2.49 | 7.56 ± 3.65 | 0.006 |
| Cyclosporine (%) | 176 (4.26) | 176 (4.32) | 0 (0.00) | 0.113 |
| Mycophenolic acid (%) | 3446 (83.36) | 3389 (83.25) | 57 (90.48) | 0.126 |
| mTOR inhibitor (%) | 215 (5.20) | 211 (5.18) | 4 (6.35) | 0.568 |
| Corticosteroid (%) | 4036 (97.63) | 3974 (97.62) | 62 (98.42) | 1.000 |
| Corticosteroid dose (mg) | 6.99 ± 3.55 | 6.99 ± 3.53 | 6.65 ± 4.75 | 0.455 |
| Death-censored graft loss (%) | 14 (0.34) | 14 (0.34) | 0 (0.00) | 1.000 |
| Rejection treatment (%) | 698 (16.88) | 686 (16.85) | 12 (19.05) | 0.644 |
| Univariable | Stratified Multivariable | |||
|---|---|---|---|---|
| HR (95% CI) | p | HR (95% CI) | p | |
| Variables at baseline | ||||
| Recipient age | 1.050 (1.024–1.076) | <0.001 | 1.035 (1.007–1.064) | 0.013 |
| Recipient sex, female | 0.716 (0.424–1.210) | 0.212 | ||
| Donor age | 0.998 (0.979–1.017) | 0.806 | ||
| Donor sex, female | 1.064 (0.649–1.745) | 0.806 | ||
| Deceased donor | 1.306 (0.794–2.147) | 0.293 | ||
| BMI (kg/m2) | 1.010 (0.923–1.062) | 0.773 | ||
| Smoking | 1.065 (0.595–1.904) | 0.832 | ||
| Pretransplant diabetes mellitus | 2.847 (1.736–4.669) | <0.001 | – | – |
| Hypertension | 0.779 (0.371–1.634) | 0.508 | ||
| History of CVD | 1.676 (0.853–3.294) | 0.134 | 0.903 (0.444–1.834) | 0.777 |
| RRT before KT | ||||
| Hemodialysis | 1.000 (Reference) | 1.000 (Reference) | ||
| Peritoneal dialysis | 0.607 (0.261–1.414) | 0.248 | ||
| KT | 2.011 (0.490–8.259) | 0.332 | ||
| Preemptive KT | 0.274 (0.086–0.878) | 0.030 | 0.360 (0.111–1.166) | 0.088 |
| Dialysis vintage (month) | 1.002 (0.998–1.006) | 0.340 | ||
| Retransplant | 1.646 (0.784–3.455) | 0.188 | 2.102 (0.981–4.506) | 0.056 |
| Mean arterial pressure | 0.990 (0.973–1.008) | 0.282 | ||
| Hemoglobin (g/dL) | 1.019 (0.873–1.190) | 0.811 | ||
| Albumin (g/dL) | 0.967 (0.603–1.550) | 0.888 | ||
| Corrected calcium (mg/dL) | 1.062 (0.808–1.350) | 0.666 | ||
| Phosphorus (mg/dL) | 0.950 (0.807–1.120) | 0.543 | ||
| Ca × P product (mg2/dL2) | 0.997 (0.980–1.015) | 0.755 | ||
| Intact PTH | 1.000 (0.999–1.001) | 0.478 | ||
| Vitamin D analogs | 0.676 (0.322–1.420) | 0.301 | ||
| Desensitization | 0.760 (0.397–1.457) | 0.409 | ||
| IL-2 receptor antibody | 4.513 (1.415–14.390) | 0.011 | 1.140 (0.155–8.357) | 0.898 |
| Anti-thymocyte globulin | 0.203 (0.064–0.646) | 0.007 | 0.160 (0.021–1.200) | 0.075 |
| Tacrolimus | N/A | N/A | ||
| Cyclosporine | N/A | N/A | ||
| Mycophenolic acid | 1.132 (0.454–2.828) | 0.790 | ||
| mTOR inhibitor | 1.077 (0.149–7.776) | 0.942 | ||
| Corticosteroid | 0.539 (0.132–2.206) | 0.390 | ||
| Variables at 6 months post-transplantation | ||||
| Hemoglobin | 0.902 (0.784–1.037) | 0.146 | 0.880 (0.762–1.018) | 0.085 |
| eGFR | 1.004 (0.991–1.016) | 0.574 | ||
| Albumin | 0.684 (0.348–1.344) | 0.271 | ||
| Corrected calcium | 1.035 (0.743–1.441) | 0.839 | ||
| Phosphorus | 0.651 (0.452–0.938) | 0.021 | 0.717 (0.215–2.398) | 0.590 |
| Ca × P product | 0.950 (0.910–0.992) | 0.020 | 0.970 (0.844–1.115) | 0.667 |
| Vitamin D analogs | 1.521 (0.825–2.801) | 0.179 | 1.304 (0.698–2.437) | 0.405 |
| Tacrolimus | N/A | N/A | ||
| Tacrolimus dose | 0.889 (0.784–1.008) | 0.067 | 0.779 (0.548–1.107) | 0.164 |
| Tacrolimus dose per body weight | 0.551 (0.271–1.121) | 0.100 | 2.621 (0.368–18.697) | 0.336 |
| Tacrolimus trough level | 1.121 (1.04–1.208) | 0.003 | 1.112 (1.028–1.202) | 0.008 |
| Cyclosporine | N/A | N/A | ||
| Mycophenolic acid | 1.853 (0.799–4.296) | 0.151 | 2.222 (0.884–5.588) | 0.090 |
| mTOR inhibitor | 1.243 (0.451–3.421) | 0.674 | ||
| Corticosteroid | 1.496 (0.207–10.790) | 0.689 | ||
| Corticosteroid dose | 0.970 (0.892–1.054) | 0.469 | ||
| Death-censored graft loss | N/A | N/A | ||
| Rejection treatment | 1.172 (0.625–2.198) | 0.621 | ||
| HR (95% CI) | p | |
|---|---|---|
| Variables at baseline | ||
| Recipient age | 1.035 (1.007–1.064) | 0.013 |
| Pretransplant diabetes mellitus | 1.115 (0.439–2.832) | 0.818 |
| Diabetes Mellitus × time | 1.049 (1.007–1.094) | 0.022 |
| History of CVD | 0.898 (0.442–1.824) | 0.766 |
| RRT before KT | ||
| Hemodialysis | 1.000 (Reference) | |
| Preemptive KT | 0.358 (0.111–1.160) | 0.087 |
| Retransplant | 2.100 (0.980–4.502) | 0.057 |
| IL-2 receptor antibody | 1.134 (0.156–8.253) | 0.901 |
| Anti-thymocyte globulin | 0.158 (0.021–1.181) | 0.072 |
| Variables at 6 months post-transplantation | ||
| Hemoglobin | 0.881 (0.762–1.018) | 0.086 |
| Phosphorus | 0.722 (0.216–2.412) | 0.596 |
| Ca × P product | 0.969 (0.762–1.018) | 0.661 |
| Vitamin D analogs | 1.310 (0.701–2.448) | 0.397 |
| Tacrolimus dose | 0.777 (0.546–1.104) | 0.159 |
| Tacrolimus dose per body weight | 2.653 (0.373–18.883) | 0.330 |
| Tacrolimus trough level | 1.112 (1.029–1.202) | 0.008 |
| Mycophenolic acid | 2.224 (0.885–5.592) | 0.089 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Eum, S.H.; Kim, D.W.; Lee, J.-H.; Jeon, J.S.; Jun, H.; Yang, J.; Kim, M.S.; Yoon, H.E.; on Behalf of the Korean Organ Transplantation Registry Study Group. Time-Varying Risk Factors for Incident Fractures in Kidney Transplant Recipients: A Nationwide Cohort Study in South Korea. J. Clin. Med. 2023, 12, 2337. https://doi.org/10.3390/jcm12062337
Eum SH, Kim DW, Lee J-H, Jeon JS, Jun H, Yang J, Kim MS, Yoon HE, on Behalf of the Korean Organ Transplantation Registry Study Group. Time-Varying Risk Factors for Incident Fractures in Kidney Transplant Recipients: A Nationwide Cohort Study in South Korea. Journal of Clinical Medicine. 2023; 12(6):2337. https://doi.org/10.3390/jcm12062337
Chicago/Turabian StyleEum, Sang Hun, Da Won Kim, Jeong-Hoon Lee, Jin Seok Jeon, Heungman Jun, Jaeseok Yang, Myoung Soo Kim, Hye Eun Yoon, and on Behalf of the Korean Organ Transplantation Registry Study Group. 2023. "Time-Varying Risk Factors for Incident Fractures in Kidney Transplant Recipients: A Nationwide Cohort Study in South Korea" Journal of Clinical Medicine 12, no. 6: 2337. https://doi.org/10.3390/jcm12062337
APA StyleEum, S. H., Kim, D. W., Lee, J.-H., Jeon, J. S., Jun, H., Yang, J., Kim, M. S., Yoon, H. E., & on Behalf of the Korean Organ Transplantation Registry Study Group. (2023). Time-Varying Risk Factors for Incident Fractures in Kidney Transplant Recipients: A Nationwide Cohort Study in South Korea. Journal of Clinical Medicine, 12(6), 2337. https://doi.org/10.3390/jcm12062337