


Oncological and Functional Outcomes for Horizontal Glottectomy: A Systematic Review

 , , , ,
, , , ,
Abstract
1. Introduction
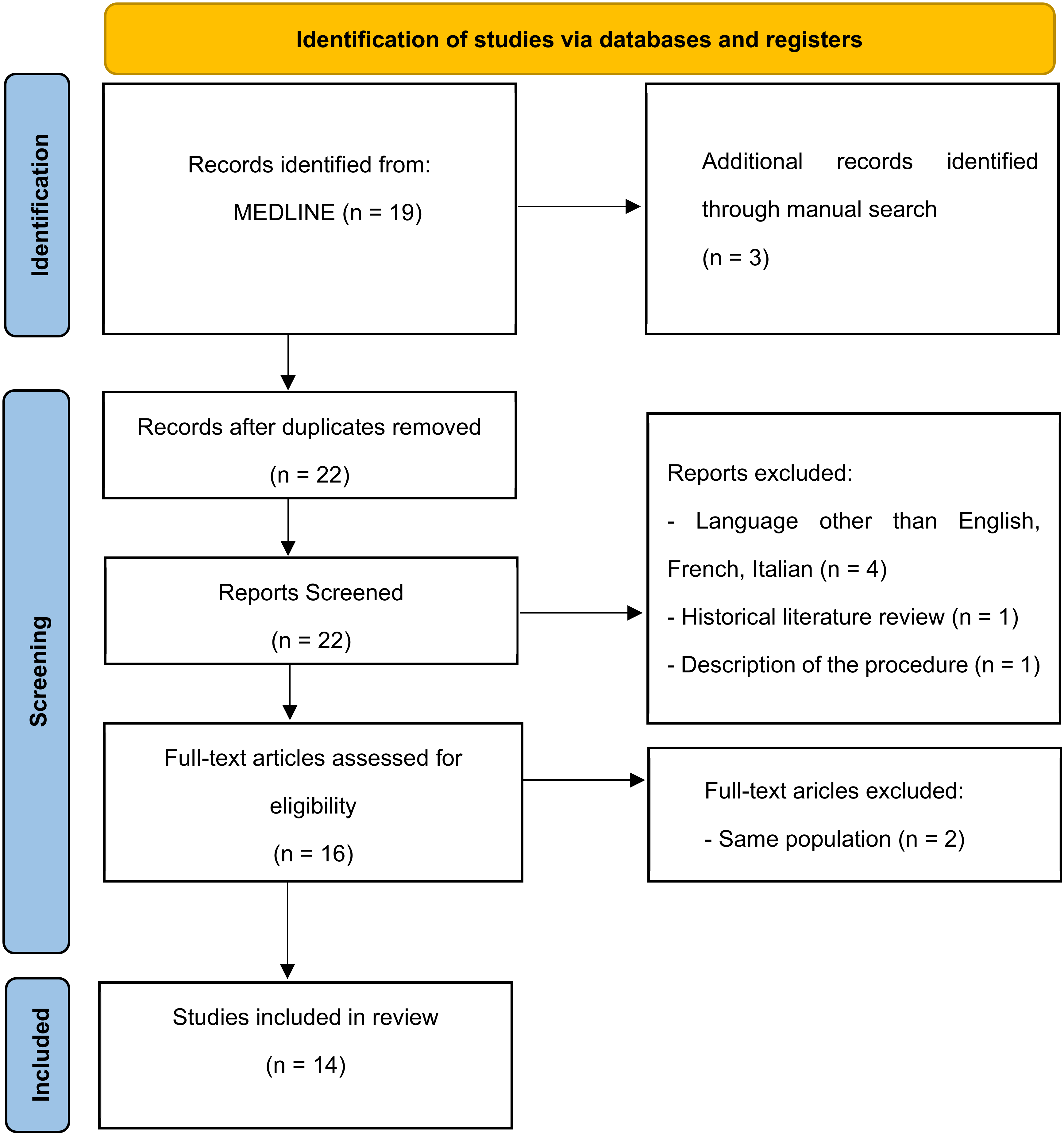
2. Materials and Methods
2.1. Eligibility Criteria
2.2. Information Sources and Search
2.3. Assessment of Quality and Risk of Bias
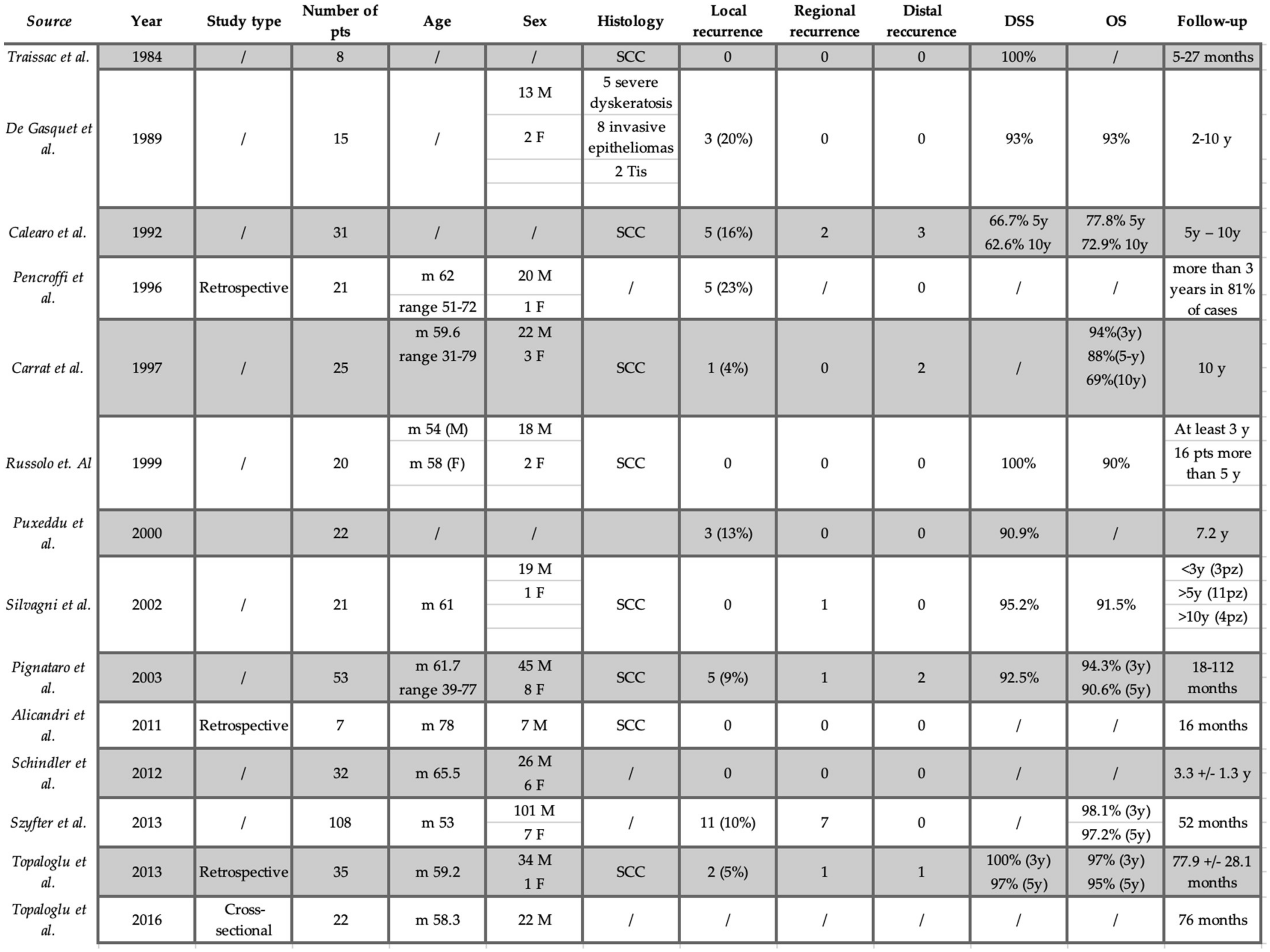
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Calearo, C.V.; Teatini, G. Horizontal Glottectomy. Laryngoscope 1978, 88, 1529–1535. [Google Scholar] [CrossRef]
- Folz, B.J.; Rinaldo, A.; Silver, C.E.; Ferlito, A. The history of horizontal glottectomy. Eur. Arch. Oto-Rhino-Laryngol. 2009, 267, 255–259. [Google Scholar] [CrossRef] [PubMed]
- Liberati, M.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed]
- Alicandri-Ciufelli, M.; Molteni, G.; Mattioli, F.; Bergamini, G.; Tassi, S.; Monzani, D.; Presutti, L.; D’Angeli, I.; Izzo, P.; Izzo, L. Horizontal glottectomy: Is it an out-of-date procedure? Am. J. Otolaryngol. 2011, 32, 578–582. [Google Scholar] [CrossRef] [PubMed]
- Schindler, A.; Mozzanica, F.; Ginocchio, D.; Invernizzi, A.; Peri, A.; Ottaviani, F. Voice-related quality of life in patients after total and partial laryngectomy. Auris Nasus Larynx 2012, 39, 77–83. [Google Scholar] [CrossRef] [PubMed]
- Topaloglu, I.; Saltürk, Z.; Bal, M.; Atar, Y. Horizontal glottectomy: Oncological results. B-ENT 2013, 9, 313–318. [Google Scholar] [PubMed]
- Topaloğlu, I.; Bal, M.; Salturk, Z.; Berkiten, G.; Atar, Y. Analysis of vocal and swallowing functions after horizontal glottectomy. Ear Nose Throat J. 2016, 95, E8–E13. [Google Scholar]
- Szyfter, W.; Leszczyńska, M.; Wierzbicka, M.; Kopeć, T.; Bartochowska, A. Value of open horizontal glottectomy in the treatment for T1b glottic cancer with anterior commissure involvement: Open Horizontal Glottectomy in T1B Glottic Cancer. Head Neck 2013, 35, 1738–1744. [Google Scholar] [CrossRef]
- Silvagni, C.; Romeo, R.; Grandinetti, P.; Ciofalo, A.; Re, M. Horizontal glottectomy according to Calearo-Teatini for the treatment of tumors involving the anterior commissure of the larynx: Oncological and functional results. Acta Otorhinolaryngol. Ital. 2002, 22, 366–371. [Google Scholar]
- Traissac, L.; Petit, J.; Lecoq, M.; Devars, F. Calearo’s operation or translaryngeal glottic operation. Surgical principles and functional results. Preliminary study. Rev. Laryngol. Otol. Rhinol. 1984, 105, 267–269. [Google Scholar]
- Russolo, M.; Giacomarra, V.; Tirelli, G. Oncological and functional results by horizontal glottectomy in laryngeal carcinomas. Anticancer. Res. 2000, 19, 4459–4461. [Google Scholar]
- Puxeddu, R.; Argiolas, F.; Bielamowicz, S.; Satta, M.; Ledda, G.P.; Puxeddu, P. Surgical Therapy of T1 and Selected Cases of T2 Glottic Carcinoma: Cordectomy, Horizontal Glottectomy and CO2 Laser Endoscopic Resection. Tumori J. 2000, 86, 277–282. [Google Scholar] [CrossRef] [PubMed]
- Pignataro, L.; Capaccio, P.; Neglia, C.B.; Ottaviani, A. Clinical experience with the treatment of T1b glottic cancer by means of horizontal glottectomy. Eur. Arch. Oto-Rhino-Laryngol. 2000, 257, 216–218. [Google Scholar] [CrossRef] [PubMed]
- Pencroffi, E.; Chays, A.; Lepette-Gillot, C.; Locatelli, P.; Heuillet, G.; Magnan, J. Laryngectomie horizontale glottique: A propos de 21 cas. J. franç. Oto-Rhino-Laryngol. 1996, 45, 98–106. [Google Scholar]
- De Gasquet, R.; Chays, A.; Magnan, J.; Bremond, G.A. La laryngectomie horizontale de Caléaro et Téatini. J. Français D’oto-Rhino-Laryngol. 1989, 38, 459–462. Available online: http://pascal-francis.inist.fr/vibad/index.php?action=getRecordDetail&idt=6859860 (accessed on 13 November 2022).
- Carrat, X.; Francois, J.-M.; Devars, F.; Carles, D.; Traissac, L. Horizontal glottectomy: Functional and oncological results. J. Laryngol. Otol. 1997, 111, 833–838. [Google Scholar] [CrossRef] [PubMed]
- Calearo, C.; Merlo, R. Personal Experience on Horizontal Glottectomy. ORL J. Otorhinolaryngol. Relat. Spec. 1992, 54, 100–102. [Google Scholar] [CrossRef]
- Schindler, A.; Cuccarini, V.; Bottero, A.; Dobrea, C.; Capaccio, P.; Ottaviani, F. Long-term vocal functional results after glottectomy: A multi-dimensional analysis. Eur. Arch. Oto-Rhino-Laryngol. 2007, 264, 1039–1044. [Google Scholar] [CrossRef]
- Jacobson, B.H.; Johnson, A.; Grywalski, C.; Silbergleit, A.; Jacobson, G.P.; Benninger, M.S.; Newman, C.W. The Voice Handicap Index (VHI). Am. J. Speech-Language Pathol. 1997, 6, 66–70. [Google Scholar] [CrossRef]
- Yanagihara, N. Significance of Harmonic Changes and Noise Components in Hoarseness. J. Speech Hear. Res. 1967, 10, 531–541. [Google Scholar] [CrossRef]
- Pearson, B.W. Subtotal Laryngectomy. Laryngoscope 1981, 91, 1904–1912. [Google Scholar] [CrossRef] [PubMed]
- Leipzig, B. Neoglottic Reconstruction following Total Laryngectomy. Ann. Otol. Rhinol. Laryngol. 1980, 89, 534–537. [Google Scholar] [CrossRef] [PubMed]
- Fermi, M.; Manto, A.L.; Di Massa, G.; Gallo, G.; Lupi, M.; Maiolo, V.; Montrone, G.; Lovato, L.; Presutti, L.; Mattioli, F. Paraglottic Space Invasion in Glottic Laryngeal Cancer: A Clinical-Pathological Study. Laryngoscope, 2022; ahead of print. [Google Scholar] [CrossRef]
- Mannelli, G.; Comini, L.V.; Santoro, R.; Bettiol, A.; Vannacci, A.; Desideri, I.; Bonomo, P.; Piazza, C. T1 Glottic Cancer: Does Anterior Commissure Involvement Worsen Prognosis? Cancers 2020, 12, 1485. [Google Scholar] [CrossRef] [PubMed]
- Piazza, C.; Mangili, S.; Del Bon, F.; Paderno, A.; Grazioli, P.; Barbieri, D.; Perotti, P.; Garofolo, S.; Nicolai, P.; Peretti, G. Preoperative clinical predictors of difficult laryngeal exposure for microlaryngoscopy: The laryngoscore. Laryngoscope 2014, 124, 2561–2567. [Google Scholar] [CrossRef] [PubMed]
- Piazza, C.; Paderno, A.; Grazioli, P.; Del Bon, F.; Montalto, N.; Perotti, P.; Morello, R.; Filauro, M.; Nicolai, P.; Peretti, G. Laryngeal exposure and margin status in glottic cancer treated by transoral laser microsurgery. Laryngoscope 2017, 128, 1146–1151. [Google Scholar] [CrossRef]
- Chone, C.T.; Yonehara, E.; Martins, J.E.F.; Altemani, A.; Crespo, A.N. Importance of Anterior Commissure in Recurrence of Early Glottic Cancer After Laser Endoscopic Resection. Arch. Otolaryngol. Neck Surg. 2007, 133, 882–887. [Google Scholar] [CrossRef]
- Casiano, R.R.; Cooper, J.D.; Lundy, D.S.; Chandler, J.R. Laser cordectomy for T1 glottic carcinoma: A 10-year experience and videostroboscopic findings. Otolaryngol. Neck Surg. 1991, 104, 831–837. [Google Scholar] [CrossRef]
- Pradhan, S.A.; Pai, P.S.; Neeli, S.I.; D’Cruz, A.K. Transoral Laser Surgery for Early Glottic Cancers. Arch. Otolaryngol. Neck Surg. 2003, 129, 623–625. [Google Scholar] [CrossRef]
- Rödel, R.M.W.; Steiner, W.; Müller, R.M.; Kron, M.; Matthias, C. Endoscopic laser surgery of early glottic cancer: Involvement of the anterior commissure. Head Neck 2009, 31, 583–592. [Google Scholar] [CrossRef]
- Lei, L.; Zhong, D.; Zou, J.; Wang, H.; Yang, H.; Zhao, Y.; Liu, J.; Cheng, D.; Wu, F. Oncological outcomes of early stage glottic squamous cell carcinoma treated with transoral laser microsurgery. Am. J. Otolaryngol. 2019, 41, 102364. [Google Scholar] [CrossRef]
- Zhou, J.; Wen, Q.; Wang, H.; Li, B.; Liu, J.; Hu, J.; Liu, S.; Zou, J. Prognostic comparison of transoral laser microsurgery for early glottic cancer with or without anterior commissure involvement: A meta-analysis. Am. J. Otolaryngol. 2020, 42, 102787. [Google Scholar] [CrossRef] [PubMed]
- Mucha-Małecka, A.; Chrostowska, A.; Urbanek, K.; Małecki, K. Prognostic factors in patients with T1 glottic cancer treated with radiotherapy. Strahlenther. Onkol. 2019, 195, 792–804. [Google Scholar] [CrossRef] [PubMed]
- Cellai, E.; Frata, P.; Magrini, S.M.; Paiar, F.; Barca, R.; Fondelli, S.; Polli, C.; Livi, L.; Bonetti, B.; Vitali, E.; et al. Radical radiotherapy for early glottic cancer: Results in a series of 1087 patients from two Italian radiation oncology centers. I. The case of T1N0 disease. Int. J. Radiat. Oncol. 2005, 63, 1378–1386. [Google Scholar] [CrossRef] [PubMed]
- Tong, C.-C.; Au, K.-H.; Ngan, R.K.; Chow, S.-M.; Cheung, F.-Y.; Fu, Y.-T.; Au, J.S.; Law, S.C. Impact and relationship of anterior commissure and time-dose factor on the local control of T1N0 glottic cancer treated by 6 MV photons. Radiat. Oncol. 2011, 6, 53. [Google Scholar] [CrossRef] [PubMed]
- Chen, M.-F.; Chang, J.T.-C.; Liao, C.-T.; Tsang, N.-M.; Chen, W.-C. Radiotherapy of early-stage glottic cancer: Analysis of factors affecting prognosis. Ann. Otol. Rhinol. Laryngol. 2003, 112, 904–911. [Google Scholar] [CrossRef]
- Nozaki, M.; Furuta, M.; Murakami, Y.; Izawa, Y.; Iwasaki, N.; Takahashi, H.; Watanabe, K. Radiation therapy for T1 glottic cancer: Involvement of the anterior commissure. Anticancer. Res. 2000, 20, 1121–1124. [Google Scholar] [PubMed]
- Lim, Y.J.; Wu, H.-G.; Kwon, T.-K.; Hah, J.H.; Sung, M.-W.; Kim, K.H.; Park, C.I. Long-Term Outcome of Definitive Radiotherapy for Early Glottic Cancer: Prognostic Factors and Patterns of Local Failure. Cancer Res. Treat. 2015, 47, 862–870. [Google Scholar] [CrossRef]
- Eskiizmir, G.; Baskın, Y.; Yalçın, F.; Ellidokuz, H.; Ferris, R.L. Risk factors for radiation failure in early-stage glottic carcinoma: A systematic review and meta-analysis. Oral Oncol. 2016, 62, 90–100. [Google Scholar] [CrossRef]
- Bron, L.P.; Soldati, D.; Zouhair, A.; Ozsahin, M.; Brossard, E.; Monnier, P.; Pasche, P. Treatment of early stage squamous-cell carcinoma of the glottic larynx: Endoscopic surgery or cricohyoidoepiglottopexy versus radiotherapy. Head Neck 2001, 23, 823–829. [Google Scholar] [CrossRef]
- Mesolella, M.; Iorio, B.; Buono, S.; Cimmino, M.; Motta, G. Supracricoid Partial Laryngectomy: Oncological and Functional Outcomes. Int. Arch. Otorhinolaryngol. 2021, 26, e075–e084. [Google Scholar] [CrossRef] [PubMed]
- Atallah, I.; Berta, E.; Coffre, A.; Villa, J.; Reyt, E.; Righini, C. Supracricoid partial laryngectomy with crico-hyoido-epiglottopexy for glottic carcinoma with anterior commissure involvement. Acta Otorhinolaryngol. Ital. 2017, 37, 188–194. [Google Scholar] [CrossRef] [PubMed]
- Laccourreye, H.; Laccourreye, O.; Menard, M.; Weinstein, G.; Brasnu, D. Supracricoid Laryngectomy with Cricohyoidoepiglottopexy: A Partial Laryngeal Procedure for Glottic Carcinoma. Ann. Otol. Rhinol. Laryngol. 1990, 99, 421–426. [Google Scholar] [CrossRef]
- Pinar, E.; Imre, A.; Calli, C.; Oncel, S.; Katilmis, H. Supracricoid Partial Laryngectomy: Analyses of Oncologic and Functional Outcomes. Otolaryngol. Neck Surg. 2012, 147, 1093–1098. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Author | N. | Preoperative Staging |
|---|---|---|
| L. Traissac, 1984 | 8 | 3 T1a–5 T1b |
| De Gasquet, 1989 | 15 | 15 T1b |
| Calearo, 1992 | 31 | 3 diffuse hyperkeratosis |
| 6 Tis | ||
| 14 T1a | ||
| 8 T1b | ||
| Pencroffi, 1996 | 21 | 21 T1b N0 M0 |
| Carrat, 1997 | 25 | 13 T1a |
| 12 T1b | ||
| N0 | ||
| M. Russolo, 1999 | 20 | 15 T1b |
| 5 T1A | ||
| N0 | ||
| Puxeddu, 2000 | 22 | Non |
| C. Silvagni, 2002 | 21 | 3 T1a |
| 18 T1b | ||
| N0M0 | ||
| Pignataro, 2003 | 53 | 53 T1b |
| N0 | ||
| Alicandri, 2011 | 7 | Non |
| Antonio Schindler, 2012 | 32 | Non |
| Witold Szyfter, 2013 | 108 | 108 T1b |
| 10 positivi al II livello | ||
| İlhan Topaloğlu, 2013 | 35 | 26 T1b N0 |
| 2 T1b N1 | ||
| 6 T2 N0 | ||
| 1 T2 N1 | ||
| İlhan Topaloğlu, 2016 | 22 | 16 T1b N0M0 |
| 2 T1b N1M0 | ||
| 3 T2 N0M0 | ||
| 1 T2 N1M0 |
| Study | MINORS |
|---|---|
| Traissac et al. | 6 |
| De Gasquet et al. | 4 |
| Calearo et al. | 9 |
| Pencroffi et al. | 7 |
| Carrat et al. | 9 |
| Russolo et. al. | 9 |
| Puxeddu et al. | 11 |
| Silvagni et al. | 11 |
| Pignataro et al. | 11 |
| Alicandri et al. | 11 |
| Schindler et al. | 11 |
| Szyfter et al. | 11 |
| Topaloglu et al. | 11 |
| Topaloglu et al. | 11 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fermi, M.; Lo Manto, A.; Lotto, C.; Cianci, G.; Mattioli, F.; Marchioni, D.; Presutti, L.; Fernandez, I.J. Oncological and Functional Outcomes for Horizontal Glottectomy: A Systematic Review. J. Clin. Med. 2023, 12, 2261. https://doi.org/10.3390/jcm12062261
Fermi M, Lo Manto A, Lotto C, Cianci G, Mattioli F, Marchioni D, Presutti L, Fernandez IJ. Oncological and Functional Outcomes for Horizontal Glottectomy: A Systematic Review. Journal of Clinical Medicine. 2023; 12(6):2261. https://doi.org/10.3390/jcm12062261
Chicago/Turabian StyleFermi, Matteo, Alfredo Lo Manto, Cecilia Lotto, Giulia Cianci, Francesco Mattioli, Daniele Marchioni, Livio Presutti, and Ignacio Javier Fernandez. 2023. "Oncological and Functional Outcomes for Horizontal Glottectomy: A Systematic Review" Journal of Clinical Medicine 12, no. 6: 2261. https://doi.org/10.3390/jcm12062261
APA StyleFermi, M., Lo Manto, A., Lotto, C., Cianci, G., Mattioli, F., Marchioni, D., Presutti, L., & Fernandez, I. J. (2023). Oncological and Functional Outcomes for Horizontal Glottectomy: A Systematic Review. Journal of Clinical Medicine, 12(6), 2261. https://doi.org/10.3390/jcm12062261