

Impact of Sarcopenia on Survival in Patients Treated with FOLFIRINOX in a First-Line Setting for Metastatic Pancreatic Carcinoma

 , , and
, , and
Abstract
1. Introduction
2. Material and Methods
2.1. Study Design and Objectives
2.2. Patients and Treatment
2.3. Toxicity Assessment
2.4. Anthropometric Measurement
2.5. Image Analysis
2.6. Statistical Analysis
3. Results
3.1. Patients
3.2. Toxicity
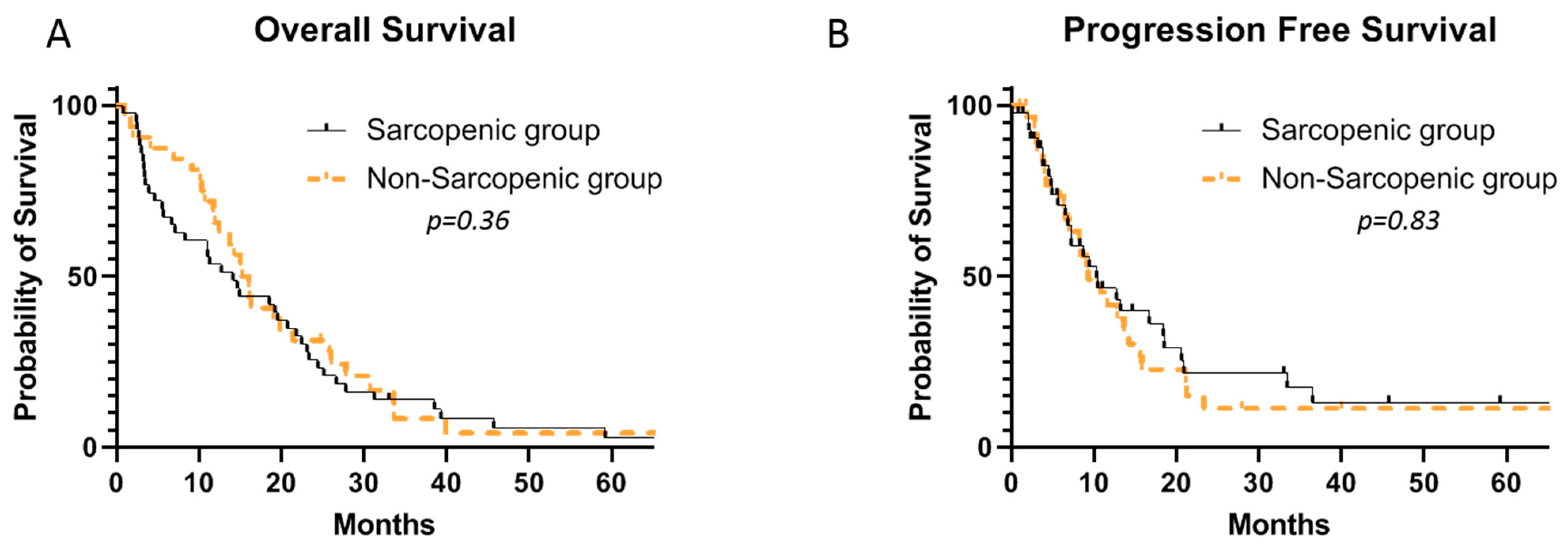
3.3. Survival
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Rahib, L.; Smith, B.D.; Aizenberg, R.; Rosenzweig, A.B.; Fleshman, J.M.; Matrisian, L.M. Projecting Cancer Incidence and Deaths to 2030: The Unexpected Burden of Thyroid, Liver, and Pancreas Cancers in the United States. Cancer Res. 2014, 74, 2913–2921. [Google Scholar] [CrossRef] [PubMed]
- Fogel, E.L.; Shahda, S.; Sandrasegaran, K.; DeWitt, J.; Easler, J.J.; Agarwal, D.M.; Eagleson, M.A.B.; Zyromski, N.J.; House, M.G.; Ellsworth, S.; et al. A Multidisciplinary Approach to Pancreas Cancer in 2016: A Review. Am. J. Gastroenterol. 2017, 112, 537–554. [Google Scholar] [CrossRef] [PubMed]
- Burris, H.A.; Moore, M.J.; Andersen, J.; Green, M.R.; Rothenberg, M.L.; Modiano, M.R.; Cripps, M.C.; Portenoy, R.K.; Storniolo, A.M.; Tarassoff, S.; et al. Improvements in survival and clinical benefit with gemcitabine as first-line therapy for patients with advanced pancreas cancer: A randomized trial. J. Clin. Oncol. 1997, 15, 2403–2413. [Google Scholar] [CrossRef] [PubMed]
- Von Hoff, D.D.; Ervin, T.; Arena, F.P.; Chiorean, E.G.; Infante, J.; Moore, M.; Seay, T.; Tjulandin, S.A.; Ma, W.W.; Saleh, M.N.; et al. Increased Survival in Pancreatic Cancer with nab-Paclitaxel plus Gemcitabine. N. Engl. J. Med. 2013, 369, 1691–1703. [Google Scholar] [CrossRef] [PubMed]
- Conroy, T.; Desseigne, F.; Ychou, M.; Bouché, O.; Guimbaud, R.; Bécouarn, Y.; Adenis, A.; Raoul, J.-L.; Gourgou-Bourgade, S.; de la Fouchardière, C.; et al. FOLFIRINOX versus Gemcitabine for Metastatic Pancreatic Cancer. N. Engl. J. Med. 2011, 364, 1817–1825. [Google Scholar] [CrossRef] [PubMed]
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2019. CA Cancer J. Clin. 2019, 69, 7–34. [Google Scholar] [CrossRef]
- Fearon, K.; Strasser, F.; Anker, S.D.; Bosaeus, I.; Bruera, E.; Fainsinger, R.L.; Jatoi, A.; Loprinzi, C.; MacDonald, N.; Mantovani, G.; et al. Definition and classification of cancer cachexia: An international consensus. Lancet Oncol. 2011, 12, 489–495. [Google Scholar] [CrossRef]
- Baracos, V.E.; Martin, L.; Korc, M.; Guttridge, D.C.; Fearon, K.C.H. Cancer-associated cachexia. Nat. Rev. Dis. Prim. 2018, 4, 17105. [Google Scholar] [CrossRef]
- Prado, C.M.M.; Lieffers, J.R.; McCargar, L.J.; Reiman, T.; Sawyer, M.B.; Martin, L.; Baracos, V.E. Prevalence and clinical implications of sarcopenic obesity in patients with solid tumours of the respiratory and gastrointestinal tracts: A population-based study. Lancet Oncol. 2008, 9, 629–635. [Google Scholar] [CrossRef]
- Kazemi-Bajestani, S.M.R.; Mazurak, V.C.; Baracos, V. Computed tomography-defined muscle and fat wasting are associated with cancer clinical outcomes. Semin. Cell Dev. Biol. 2016, 54, 2–10. [Google Scholar] [CrossRef]
- Martin, L.; Birdsell, L.; MacDonald, N.; Reiman, T.; Clandinin, M.T.; McCargar, L.J.; Murphy, R.; Ghosh, S.; Sawyer, M.B.; Baracos, V.E. Cancer Cachexia in the Age of Obesity: Skeletal Muscle Depletion Is a Powerful Prognostic Factor, Independent of Body Mass Index. J. Clin. Oncol. 2013, 31, 1539–1547. [Google Scholar] [CrossRef] [PubMed]
- Bozzetti, F. Forcing the vicious circle: Sarcopenia increases toxicity, decreases response to chemotherapy and worsens with chemotherapy. Ann. Oncol. 2017, 28, 2107–2118. [Google Scholar] [CrossRef] [PubMed]
- Shachar, S.S.; Williams, G.R.; Muss, H.B.; Nishijima, T.F. Prognostic value of sarcopenia in adults with solid tumours: A meta-analysis and systematic review. Eur. J. Cancer 2016, 57, 58–67. [Google Scholar] [CrossRef]
- Mintziras, I.; Miligkos, M.; Wächter, S.; Manoharan, J.; Maurer, E.; Bartsch, D.K. Sarcopenia and sarcopenic obesity are significantly associated with poorer overall survival in patients with pancreatic cancer: Systematic review and meta-analysis. Int. J. Surg. 2018, 59, 19–26. [Google Scholar] [CrossRef] [PubMed]
- Bundred, J.; Kamarajah, S.K.; Roberts, K.J. Body composition assessment and sarcopenia in patients with pancreatic cancer: A systematic review and meta-analysis. HPB 2019, 21, 1603–1612. [Google Scholar] [CrossRef]
- Kurita, Y.; Kobayashi, N.; Tokuhisa, M.; Goto, A.; Kubota, K.; Endo, I.; Nakajima, A.; Ichikawa, Y. Sarcopenia is a reliable prognostic factor in patients with advanced pancreatic cancer receiving FOLFIRINOX chemotherapy. Pancreatology 2019, 19, 127–135. [Google Scholar] [CrossRef]
- National Institutes of Health. Common Terminology Criteria for Adverse Events. Version 4; US Department of Health and Human Services: Bethesda, MD, USA, 2010.
- Eisenhauer, E.A.; Therasse, P.; Bogaerts, J.; Schwartz, L.H.; Sargent, D.; Ford, R.; Dancey, J.; Arbuck, S.; Gwyther, S.; Mooney, M.; et al. New response evaluation criteria in solid tumours: Revised RECIST guideline (version 1.1). Eur. J. Cancer 2009, 45, 228–247. [Google Scholar] [CrossRef]
- Barat, M.; Jannot, A.S.; Dohan, A.; Soyer, P. How to report and compare quantitative variables in a radiology article. Diagn. Interv. Imaging 2022, 103, 571–573. [Google Scholar] [CrossRef]
- Chow, R.; Chiu, N.; Bruera, E.; Krishnan, M.; Chiu, L.; Lam, H.; DeAngelis, C.; Pulenzas, N.; Vuong, S.; Chow, E.; et al. Inter-rater reliability in performance status assessment among health care professionals: A systematic review. Ann. Palliat. Med. 2016, 5, 83–92. [Google Scholar] [CrossRef]
- Kelly, C.M.; Shahrokni, A. Moving beyond Karnofsky and ECOG Performance Status Assessments with New Technologies. J. Oncol. 2016, 2016, 6186543. [Google Scholar] [CrossRef]
- Portal, A.; Pernot, S.; Tougeron, D.; Arbaud, C.; Bidault, A.T.; de la Fouchardière, C.; Hammel, P.; Lecomte, T.; Dréanic, J.; Coriat, R.; et al. Nab-paclitaxel plus gemcitabine for metastatic pancreatic adenocarcinoma after Folfirinox failure: An AGEO prospective multicentre cohort. Br. J. Cancer 2015, 113, 989–995. [Google Scholar] [CrossRef] [PubMed]
- Neuzillet, C.; Bouché, O.; Tournigand, C.; Chibaudel, B.; Bouguion, L.; Bengrine-Lefevre, L.; Ataz, D.L.-T.; Mabro, M.; Metges, J.-P.; Péré-Vergé, D.; et al. Adapted physical activity in patients (Pts) with advanced pancreatic cancer (APACaP): Results from a prospective national randomized GERCOR trial. J. Clin. Oncol. 2022, 40, 4007. [Google Scholar] [CrossRef]
- Uemura, S.; Iwashita, T.; Ichikawa, H.; Iwasa, Y.; Mita, N.; Shiraki, M.; Shimizu, M. The impact of sarcopenia and decrease in skeletal muscle mass in patients with advanced pancreatic cancer during FOLFIRINOX therapy. Br. J. Nutr. 2021, 125, 1140–1147. [Google Scholar] [CrossRef] [PubMed]
- Prado, C.M.M.; Baracos, V.E.; McCargar, L.J.; Reiman, T.; Mourtzakis, M.; Tonkin, K.; Mackey, J.R.; Koski, S.; Pituskin, E.; Sawyer, M.B. Sarcopenia as a Determinant of Chemotherapy Toxicity and Time to Tumor Progression in Metastatic Breast Cancer Patients Receiving Capecitabine Treatment. Clin. Cancer Res. 2009, 15, 2920–2926. [Google Scholar] [CrossRef] [PubMed]
- Tan, B.H.L.; Brammer, K.; Randhawa, N.; Welch, N.T.; Parsons, S.L.; James, E.J.; Catton, J. Sarcopenia is associated with toxicity in patients undergoing neo-adjuvant chemotherapy for oesophago-gastric cancer. Eur. J. Surg. Oncol. 2015, 41, 333–338. [Google Scholar] [CrossRef]
- Cousin, S.; Hollebecque, A.; Koscielny, S.; Mir, O.; Varga, A.; Baracos, V.E.; Soria, J.C.; Antoun, S. Low skeletal muscle is associated with toxicity in patients included in phase I trials. Investig. New Drugs 2014, 32, 382–387. [Google Scholar] [CrossRef]
- Anandavadivelan, P.; Brismar, T.B.; Nilsson, M.; Johar, A.M.; Martin, L. Sarcopenic obesity: A probable risk factor for dose limiting toxicity during neo-adjuvant chemotherapy in oesophageal cancer patients. Clin. Nutr. 2016, 35, 724–730. [Google Scholar] [CrossRef]
- Carneiro, I.P.; Mazurak, V.C.; Prado, C.M. Clinical Implications of Sarcopenic Obesity in Cancer. Curr. Oncol. Rep. 2016, 18, 62. [Google Scholar] [CrossRef]
- Baracos, V.E.; Arribas, L. Sarcopenic obesity: Hidden muscle wasting and its impact for survival and complications of cancer therapy. Ann. Oncol. 2018, 29, ii1–ii9. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Patients’ Characteristics | All Patients | Non-Sarcopenic Patients | Sarcopenic Patients | p-Value |
|---|---|---|---|---|
| Patients, n (%) | 75 | 32 (42.7) | 43 (57.3) | |
| Sex, n (%) | 0.98 | |||
| Women | 38 (51) | 13 (34.2) | 25 (65) | |
| Men | 37 (49.3) | 19 (51.3) | 18 (48.7) | |
| Age, mean (SD) | 64 (11.2) | 63.4 (11.7) | 64.4 (11) | 0.68 |
| Weight (kg), mean (SD) | 67.9 (13,5) | 73 (12.4) | 64 (13) | 0.002 |
| BMI, mean (SD) | 23.6 (4.4) | 25.3 (5.1) | 22.3 (3.3) | 0.005 |
| Underweight (BMI < 18.5), n (%) | 3 (4) | 0 (0) | 3 (7) | |
| Normalweight (18.5 ≤ BMI < 25), n (%) | 49 (65.3) | 18 (56.2) | 31 (72) | |
| Overweight (25 ≤ BMI < 30), n (%) | 17 (22.7) | 10 (31.2) | 7 (16.3) | |
| Obese (30 ≤ BMI), n (%) | 4 (5.3) | 3 (9.4) | 1 (2.3) | |
| Skeletal muscle L3 area (cm2), mean (SD) | 123.3 (31.5) | 144.5 (24.5) | 107.6 (26.7) | <0.001 |
| SMI (cm2/m2) (men), mean (SD) | 45.3 (7.5) | 49.6 (4.7) | 40.8 (7.3) | <0.001 |
| SMI (cm2/m2) (women), mean (SD) | 39.6 (9.1) | 48.9 (8.8) | 34.7 (4.3) | <0.001 |
| ECOG PS, n (%) | 0.2 | |||
| 0 | 14 (18.7) | 8 (25) | 6 (14) | |
| 1 | 31 (41.3) | 16 (50) | 15 (34.9) | |
| 2 | 11 (14.7) | 3 (9.4) | 8 (18.6) | |
| 3 | 2 (2.6) | 0 (0) | 2 (4.6) | |
| Unknown | 17 (22.6) | 5 (15.6) | 12 (28) | |
| Site of tumor, n (%) | 0.36 | |||
| Head | 40 (53.3) | 16 (50) | 24 (55.8) | |
| Body or tail | 33 (44) | 16 (50) | 17 (39.5) | |
| Unknown | 2 (2.6) | 0 (0) | 2 (4.6) | |
| Biliary drainage, n (%) | 19 (25.3) | 9 (28) | 10 (23.2) | 0.6 |
| Liver metastasis, n (%) | 54 (72) | 23 (71.9) | 31 (72) | 0.98 |
| Pulmonary metastasis, n (%) | 24 (32) | 11 (34.4) | 13 (30) | 0.7 |
| Peritoneum metastasis, n (%) | 18 (24) | 6 (18.7) | 12 (28) | 0.35 |
| Previous therapy for localized cancer | ||||
| Adjuvant chemotherapy, n (%) | 9 (12.0) | 6 (18.7) | 3 (7) | 0.12 |
| Pancreatic surgery, n (%) | 10 (13.3) | 6 (18.7) | 4 (9.3) | 0.23 |
| CRP (mg/L), median (IQR) | 13.6 (3.9–33.9) | 13.5 (3.4–32.3) | 15.1 (4.9–35.2) | 0.8 |
| Ca 19.9 (U/mL), median (IQR) | 462.5 (48.9–3910.7) | 425 (87.4–5179.5) | 500 (39.2–1823) | 0.08 |
| CEA (ng/mL), median (IQR) | 7 (3.8–29.7) | 5.5 (3.3–12.6) | 17.1 (6.3–36.6) | 0.25 |
| Total bilirubin (umol/L), median (IQR) | 8.3 (5.5–16) | 9.7 (6–16.5) | 7.35 (5.3–15) | 0.69 |
| Albumin (g/L), median (IQR) | 38.5 (34–41) | 39 (36–42) | 38 (33–40) | 0.22 |
| All Patients (n = 75) | Non-Sarcopenic Patients (n = 32) | Sarcopenic Patients (n = 43) | p-Value | |
|---|---|---|---|---|
| Neutropenia | ||||
| Any grade | 14 (18.6) | 7 (21.9) | 7 (16.3) | 0.53 |
| Grade ≥ 3 | 6 (8) | 3 (9.4) | 3 (7) | 1 |
| Febrile neutropenia | ||||
| Any grade | NA | NA | NA | |
| Grade ≥ 3 | 3 (4) | 2 (6.2) | 1 (2.3) | 0.57 |
| Thrombopenia | ||||
| Any grade | 19 (25.3) | 11 (34.4) | 8 (18.6) | 0.12 |
| Grade ≥ 3 | 3 (4) | 2 (6.2) | 1 (2.3) | 0.57 |
| Anemia | ||||
| Any grade | 30 (40) | 17 (53) | 13 (30) | 0.045 |
| Grade ≥ 3 | 5 (6) | 2 (6.2) | 3 (7) | 1 |
| Diarrhea | ||||
| Any grade | 42 (56) | 19 (59) | 23 (53.5) | 0.61 |
| Grade ≥ 3 | 10 (13.3) | 3 (9.4) | 7 (16.3) | 0.38 |
| Nausea | ||||
| Any grade | 34 (45.3) | 17 (53) | 17 (39.5) | 0.24 |
| Grade ≥ 3 | 5 (6.7) | 2 (6.2) | 3 (6.9) | 0.90 |
| Vomiting | ||||
| Any grade | 21 (28) | 9 (28.1) | 12 (27.9) | 0.98 |
| Grade ≥ 3 | 3 (4) | 1 (3.1) | 2 (4.7) | 1 |
| Peripheral neuropathy | ||||
| Any grade | 51 (68) | 24 (75) | 27 (62.8) | 0.26 |
| Grade ≥ 3 | 2 (2.6) | 2 (6.2) | 0 (0) | 0.17 |
| All Patients n = 75 | Non-Sarcopenic Patients n = 32 | Sarcopenic Patients n = 43 | p-Value | |
|---|---|---|---|---|
| Oxaliplatin, n (%) | ||||
| Dose reduction | 38 (50.7) | 18 (56.2) | 20 (46.5) | 0.4 |
| Discontinuation | 33 (44) | 15 (46.9) | 18 (41.9) | 0.66 |
| Irinotecan, n (%) | ||||
| Dose reduction | 29 (38.7) | 10 (31.2) | 19 (44.2) | 0.25 |
| Discontinuation | 14 (18.7) | 5 (15.6) | 9 (20.9) | 0.55 |
| 5-fluorouracil, n (%) | ||||
| Dose reduction | 14 (18.7) | 5 (15.6) | 9 (20.9) | 0.55 |
| Discontinuation | 0 | 0 | 0 | NA |
| All Patients (n = 75) | Non-Sarcopenic Patients (n = 32) | Sarcopenic Patients (n = 43) | p-Value | |
|---|---|---|---|---|
| Death within 4 months from diagnosis, n (%) | ||||
| Death before confirmed radiological progression | 10 (13.3) | 2 (6.2) | 8 (18.6) | 0.08 |
| Death before or after confirmed radiological progression | 14 (18.6) | 3 (9.4) | 11 (25.6) | 0.07 |
| Death within 12 months from diagnosis, n (%) | ||||
| Death before confirmed radiological progression | 12 (16) | 4 (12.5) | 8 (18.6) | 0.54 |
| Death before or after radiological progression | 32 (42.7) | 11 (34) | 21 (48) | 0.24 |
| All Patients n = 75 | Non-Sarcopenic Patients n = 32 | Sarcopenic Patients n = 43 | p-Value | |
|---|---|---|---|---|
| Best supportive care | 44 (58.7) | 12 (43.7) | 30 (69.8) | 0.02 |
| Second-line therapy | 31 (41.3) | 18 (56.3) | 13 (30.2) | 0.02 |
| Gemcitabine monotherapy, n (%) | 11 (14.7) | 6 (18.7) | 5 (11.6) | 0.38 |
| Gemcitabine plus nab-paclitaxel, n (%) | 20 (26.7) | 12 (37.5) | 8 (18.6) | 0.06 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lellouche, L.; Barat, M.; Pellat, A.; Leroux, J.; Corre, F.; Hallit, R.; Assaf, A.; Brezault, C.; Dhooge, M.; Soyer, P.; et al. Impact of Sarcopenia on Survival in Patients Treated with FOLFIRINOX in a First-Line Setting for Metastatic Pancreatic Carcinoma. J. Clin. Med. 2023, 12, 2211. https://doi.org/10.3390/jcm12062211
Lellouche L, Barat M, Pellat A, Leroux J, Corre F, Hallit R, Assaf A, Brezault C, Dhooge M, Soyer P, et al. Impact of Sarcopenia on Survival in Patients Treated with FOLFIRINOX in a First-Line Setting for Metastatic Pancreatic Carcinoma. Journal of Clinical Medicine. 2023; 12(6):2211. https://doi.org/10.3390/jcm12062211
Chicago/Turabian StyleLellouche, Lisa, Maxime Barat, Anna Pellat, Juliette Leroux, Felix Corre, Rachel Hallit, Antoine Assaf, Catherine Brezault, Marion Dhooge, Philippe Soyer, and et al. 2023. "Impact of Sarcopenia on Survival in Patients Treated with FOLFIRINOX in a First-Line Setting for Metastatic Pancreatic Carcinoma" Journal of Clinical Medicine 12, no. 6: 2211. https://doi.org/10.3390/jcm12062211
APA StyleLellouche, L., Barat, M., Pellat, A., Leroux, J., Corre, F., Hallit, R., Assaf, A., Brezault, C., Dhooge, M., Soyer, P., & Coriat, R. (2023). Impact of Sarcopenia on Survival in Patients Treated with FOLFIRINOX in a First-Line Setting for Metastatic Pancreatic Carcinoma. Journal of Clinical Medicine, 12(6), 2211. https://doi.org/10.3390/jcm12062211