
Clinical Predictors and Prediction Models for rFVIII-Fc Half Life in Real-World People with Severe Hemophilia A
 , , , and
, , , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Patient Characteristics
2.3. Regimen and PK Assessment of rFVIII-Fc
2.4. Predictor Investigation and Prediction Model Development with Internal Validation
2.5. External Validation of the Prediction Models
2.6. Statistics
3. Results
3.1. Patient Characteristics of the Development Cohort and Validation Cohort
3.2. Analysis of the rFVIII-Fc Half Lives in the Development Cohort
3.3. Comparison of the Development Cohort with Blood Group Non-O and Blood Group O
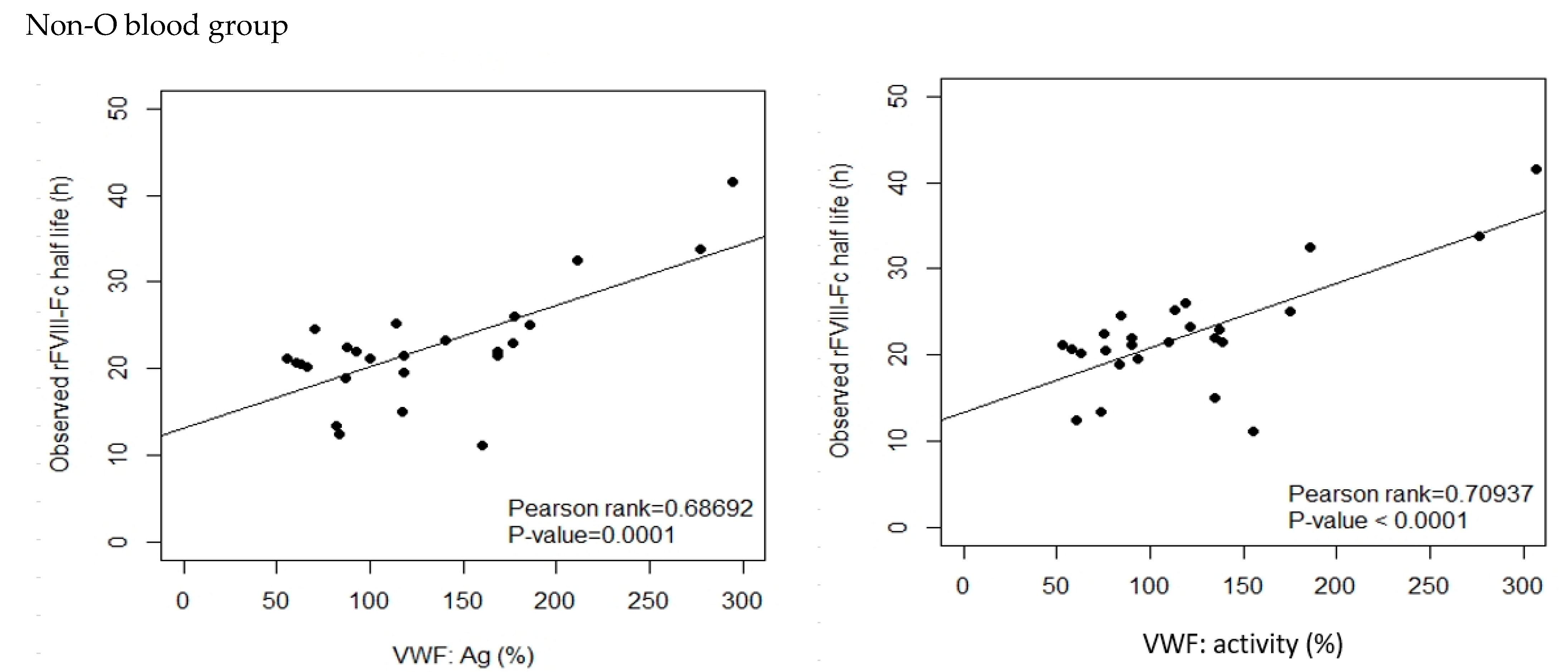
3.4. Correlation Analysis for rFVIII-Fc Half Life
3.5. Univariate Linear Regression (UVLR) Analysis of Parameters with the Potential for Prediction of rFVIII-Fc Half Life
3.6. Multivariate Linear Regression (MVLR) Analysis for Identifying Predictors and Developing Prediction Models
- (1)
- When analyzing non-O blood group PwHA using this method, age, BW, Hct, inhibitor history, HCV infection, HIV infection, baseline VWF:activity, and the VWF:activity/VWF:Ag ratio were eliminated as predictive parameters. The remaining covariates (baseline VWF:Ag and BMI) were proved to be positive predictors and were used to define Equation (1), which explained 51.97% of all the variability in the rFVIII-Fc half life. As per the mathematical modeling, the rFVIII-Fc half life would increase by 6.07 h whenever the baseline VWF:Ag is increased by 1 IU/mL (100%).T (predicted half life of non-O group patients, hrs) = −0.81 + 0.63 × (BMI, kg/m2) + 6.07 × (baseline VWF:Ag, IU/mL)
- (2)
- When analyzing O blood group PwHA using this method, age, Hct, inhibitor history, HCV infection, HIV infection, and baseline VWF:activity were eliminated as predictive parameters. The remaining covariates (BMI, BW, baseline VWF:Ag, and the VWF:activity/VWF:Ag ratio) were proved to be predictors and were used to define Equation (2), which explained 75.17% of all the variability in the rFVIII-Fc half life. As per the mathematical modeling, the rFVIII-Fc half life would increase by at least (for it still needs to be added to the impact of the VWF:activity/VWF:Ag ratio) 13.3 h whenever the baseline VWF:Ag is increased by 1 IU/mL (100%).T (predicted half life of O group patients, hrs) = −0.68 + 13.30 × (baseline VWF:Ag, IU/mL) + 0.27 × (BW, kg) − 1.17 × (BMI, kg/m2) +16.02 × (VWF:activity/VWF:Ag ratio)
- (3)
- When analyzing the overall cohort of PwHA (n = 46) using this method, age, BW, BMI, HIV infection, baseline VWF:activity, and the VWF:activity/VWF:Ag ratio were eliminated as predictive parameters. The remaining covariates (ABO blood group, Hct, baseline VWF:Ag, inhibitor history, and HCV infection) were proved to be predictors and were used to define Equation (3), which explained 66.38% of all the variability in the rFVIII-Fc half-life. As per the mathematical modeling, the rFVIII-Fc half life would increase by 7.24 h whenever the baseline VWF:Ag is increased by 1 IU/mL (100%), decrease by 3.84 h in patients with a positive inhibitor history, increase by 2.99 h in patients with a positive HCV infection test, and decrease by 2.83 h in patients in blood group O.
| T (predicted half life of overall patients, hrs) = −1.76 + 7.24 × (baseline VWF:Ag, IU/mL) − 3.84 × (Inhibitor history) + 2.99 × (HCV infection) − 2.83 × (O blood group) + 0.30 × (Hct, %) | (3) |
| (For the values of covariates in this equation: 0 if the patient has a negative inhibitor history, 1 if the patient has a positive inhibitor history; 0 if the patient has a negative HCV infection test, 1 if the patient has a positive HCV infection test; and 0 if the patient is in the non-O blood group, 1 if the patient is in the O blood group) |
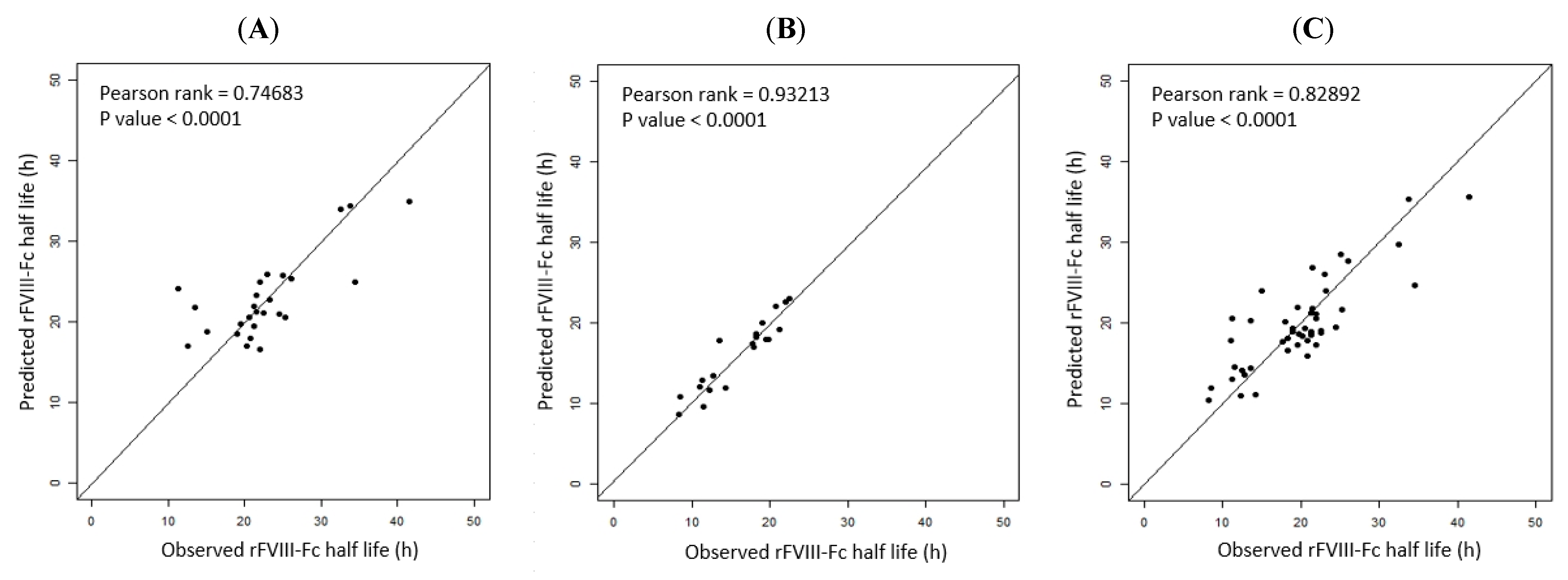
3.7. Internal Validation of the Three Prediction Models
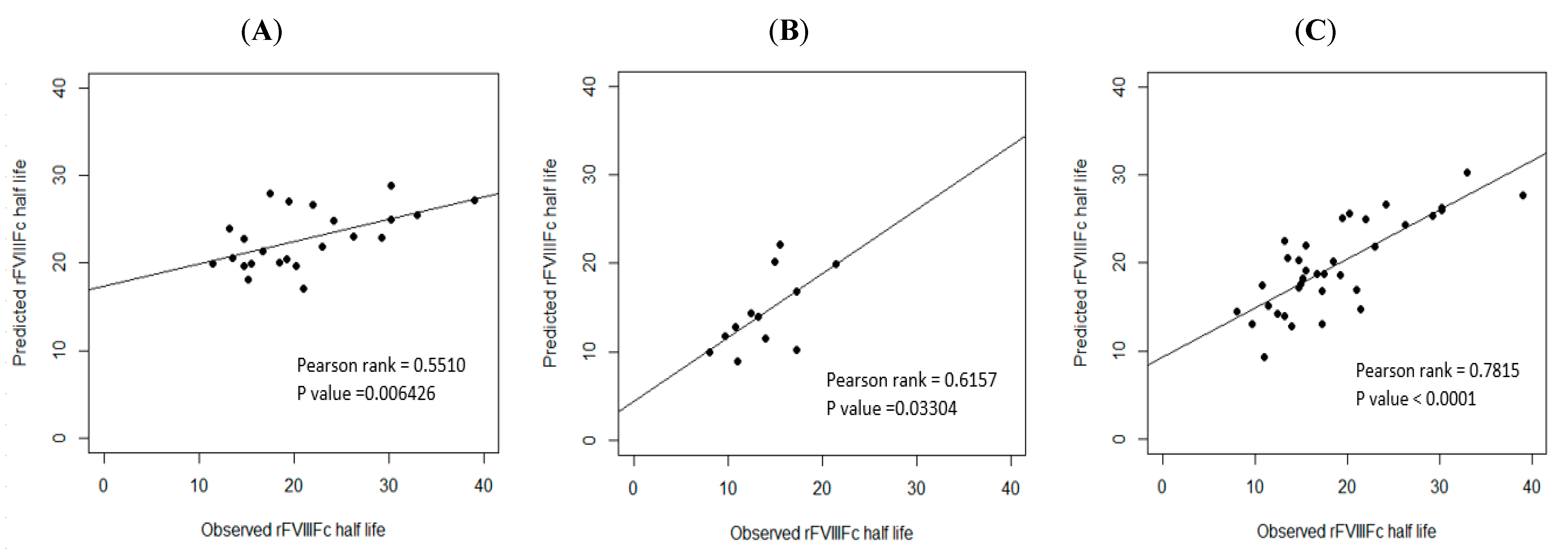
3.8. External Validation of the Three Prediction Models
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Manco-Johnson, M.J.; Abshire, T.C.; Shapiro, A.D.; Riske, B.; Hacker, M.R.; Kilcoyne, R.; Ingram, J.D.; Manco-Johnson, M.L.; Funk, S.; Jacobson, L.; et al. Prophylaxis versus episodic treatment to prevent joint disease in boys with severe hemophilia. N. Engl. J. Med. 2007, 357, 535–544. [Google Scholar] [CrossRef] [PubMed]
- Aledort, L.M.; Haschmeyer, R.H.; Pettersson, H. A longitudinal study of orthopaedic outcomes for severe factor-VIII-deficient haemophiliacs. The Orthopaedic Outcome Study Group. J. Intern. Med. 1994, 236, 391–399. [Google Scholar] [CrossRef] [PubMed]
- Fischer, K.; van der Bom, J.G.; Mauser-Bunschoten, E.P.; Roosendaal, G.; Prejs, R.; de Kleijn, P.; Grobbee, D.E.; van den Berg, M. The effects of postponing prophylactic treatment on long-term outcome in patients with severe hemophilia. Blood 2002, 99, 2337–2341. [Google Scholar] [CrossRef] [PubMed]
- Schrijvers, L.H.; Schuurmans, M.J.; Fischer, K. Promoting self-management and adherence during prophylaxis: Evidence-based recommendations for haemophilia professionals. Haemophilia 2016, 22, 499–506. [Google Scholar] [CrossRef]
- Hermans, C.; Mancuso, M.E.; Nolan, B.; Pasi, K.J. Recombinant factor VIII Fc for the treatment of haemophilia A. Eur. J. Haematol. 2021, 106, 745–761. [Google Scholar] [CrossRef]
- Chang, C.Y.; Lai, S.W.; Cheng, M.M.; Ku, J.T.; Hu, S.H.; Liu, Y.L.; Tsai, J.R.; Tsai, C.H.; Cheng, C.N.; Chen, Y.C. Real-world bleeding outcomes and product utilization in people with severe-type hemophilia A before and after switching to extended half-life rFVIIIFc prophylaxis therapy. Int. J. Hematol. 2022, 117, 378–387. [Google Scholar] [CrossRef]
- Oldenburg, J.; Kulkarni, R.; Srivastava, A.; Mahlangu, J.N.; Blanchette, V.S.; Tsao, E.; Winding, B.; Dumont, J.; Jain, N. Improved joint health in subjects with severe haemophilia A treated prophylactically with recombinant factor VIII Fc fusion protein. Haemophilia 2018, 24, 77–84. [Google Scholar] [CrossRef]
- Cuesta-Barriuso, R.; Pérez-Llanes, R.; Donoso-Úbeda, E.; Ucero-Lozano, R. LongHest project: A prospective, observational study of extended half-life treatment in the musculoskeletal health of patients with severe haemophilia A. Haemophilia 2022, 28, 857–864. [Google Scholar] [CrossRef]
- Ferri Grazzi, E.; Sun, S.X.; Burke, T.; O'Hara, J. The Impact of Pharmacokinetic-Guided Prophylaxis on Clinical Outcomes and Healthcare Resource Utilization in Hemophilia A Patients: Real-World Evidence from the CHESS II Study. J. Blood Med. 2022, 13, 505–516. [Google Scholar] [CrossRef]
- Lissitchkov, T.; Rusen, L.; Georgiev, P.; Windyga, J.; Klamroth, R.; Gercheva, L.; Nemes, L.; Tiede, A.; Bichler, J.; Knaub, S.; et al. PK-guided personalized prophylaxis with Nuwiq® (human-cl rhFVIII) in adults with severe haemophilia A. Haemophilia 2017, 23, 697–704. [Google Scholar] [CrossRef]
- Huang, K.; Zhen, Y.; Li, G.; Wu, X.; Chen, Z.; Wu, R. Pharmacokinetic-guided prophylaxis improved clinical outcomes in paediatric patients with severe haemophilia A. Haemophilia 2021, 27, e450–e457. [Google Scholar] [CrossRef] [PubMed]
- Gringeri, A.; Wolfsegger, M.; Steinitz, K.N.; Reininger, A.J. Recombinant full-length factor VIII (FVIII) and extended half-life FVIII products in prophylaxis--new insight provided by pharmacokinetic modelling. Haemophilia 2015, 21, 300–306. [Google Scholar] [CrossRef] [PubMed]
- Fijnvandraat, K.; Peters, M.; ten Cate, J.W. Inter-individual variation in half-life of infused recombinant factor VIII is related to pre-infusion von Willebrand factor antigen levels. Br. J. Haematol. 1995, 91, 474–476. [Google Scholar] [CrossRef] [PubMed]
- Fischer, K.; Pendu, R.; van Schooten, C.J.; van Dijk, K.; Denis, C.V.; van den Berg, H.M.; Lenting, P.J. Models for prediction of factor VIII half-life in severe haemophiliacs: Distinct approaches for blood group O and non-O patients. PLoS ONE 2009, 4, e6745. [Google Scholar] [CrossRef]
- van Dijk, K.; van der Bom, J.; Lenting, P.J.; de Groot, P.G.; Mauser-Bunschoten, E.P.; Roosendaal, G.; Grobbee, D.E.; van den Berg, H.M. Factor VIII half-life and clinical phenotype of severe hemophilia A. Haematologica 2005, 90, 494–498. [Google Scholar]
- van den Berg, H.M.; De Groot, P.H.; Fischer, K. Phenotypic heterogeneity in severe hemophilia. J. Thromb. Haemost. 2007, 5 (Suppl. S1), 151–156. [Google Scholar] [CrossRef] [PubMed]
- Franchini, M.; Mengoli, C.; Marano, G.; Pupella, S.; Mannucci, P.M.; Liumbruno, G.M. The importance of ABO blood group in pharmacokinetic studies in haemophilia A. Haemophilia 2018, 24, e122–e123. [Google Scholar] [CrossRef] [PubMed]
- McEneny-King, A.; Iorio, A.; Foster, G.; Edginton, A.N. The use of pharmacokinetics in dose individualization of factor VIII in the treatment of hemophilia A. Expert. Opin. Drug Metab. Toxicol. 2016, 12, 1313–1321. [Google Scholar] [CrossRef]
- Hazendonk, H.C.; Lock, J.; Mathot, R.A.; Meijer, K.; Peters, M.; Laros-van Gorkom, B.A.; van der Meer, F.J.; Driessens, M.H.; Leebeek, F.W.; Fijnvandraat, K.; et al. Perioperative treatment of hemophilia A patients: Blood group O patients are at risk of bleeding complications. J. Thromb. Haemost. 2015, 14, 468–478. [Google Scholar] [CrossRef]
- Albanez, S.; Ogiwara, K.; Michels, A.; Hopman, W.; Grabell, J.; James, P.; Lillicrap, D. Aging and ABO blood type influence VWF and FVIII levels through interrelated mechanisms. J. Thromb. Haemost. 2016, 14, 953–963. [Google Scholar] [CrossRef]
- Franchini, M.; Capra, F.; Targher, G.; Montagnana, M.; Lippi, G. Relationship between ABO blood group and von Willebrand factor levels: From biology to clinical implications. Thromb. J. 2007, 5, 14. [Google Scholar] [CrossRef]
- Vlot, A.J.; Mauser-Bunschoten, E.P.; Zarkova, A.G.; Haan, E.; Kruitwagen, C.L.; Sixma, J.J.; van den Berg, H.M. The half-life of infused factor VIII is shorter in hemophiliac patients with blood group O than in those with blood group A. Thromb. Haemost. 2000, 83, 65–69. [Google Scholar]
- Kepa, S.; Horvath, B.; Reitter-Pfoertner, S.; Schemper, M.; Quehenberger, P.; Grundbichler, M.; Heistinger, M.; Neumeister, P.; Mannhalter, C.; Pabinger, I. Parameters influencing FVIII pharmacokinetics in patients with severe and moderate haemophilia A. Haemophilia 2015, 21, 343–350. [Google Scholar] [CrossRef] [PubMed]
- Versloot, O.; Iserman, E.; Chelle, P.; Germini, F.; Edginton, A.N.; Schutgens, R.E.G.; Iorio, A.; Fischer, K.; Pharmacokinetic (PK) Expert Working Group of the International Prophylaxis Study Group (IPSG). Terminal half-life of FVIII and FIX according to age, blood group and concentrate type: Data from the WAPPS database. J. Thromb. Haemost. 2021, 19, 1896–1906. [Google Scholar] [CrossRef] [PubMed]
- Yarnell, J.W.; Sweetnam, P.M.; Rumley, A.; Lowe, G.D. Lifestyle and hemostatic risk factors for ischemic heart disease: The Caerphilly study. Arterioscler. Thromb. Vasc. Biol. 2000, 20, 271–279. [Google Scholar] [CrossRef] [PubMed]
- Shapiro, A.D.; Ragni, M.V.; Kulkarni, R.; Oldenberg, J.; Srivastava, A.; Quon, D.; Pasi, K.J.; Hanabusa, H.; Pabinger, I.; Mahlangu, J.; et al. Recombinant factor VIII Fc fusion protein: Extended-interval dosing maintains low bleeding rates and correlates with von Willebrand factor levels. J. Thromb. Haemost. 2014, 12, 1788–1800. [Google Scholar] [CrossRef] [PubMed]
- Carcao, M.D.; Chelle, P.; Clarke, E.; Kim, L.; Tiseo, L.; Morfini, M.; Hossain, T.; Rand, M.L.; Brown, C.; Edginton, A.N.; et al. Comparative pharmacokinetics of two extended half-life FVIII concentrates (Eloctate and Adynovate) in adolescents with hemophilia A: Is there a difference? J. Thromb. Haemost. 2019, 17, 1085–1096. [Google Scholar] [CrossRef]
- Mahlangu, J.; Powell, J.S.; Ragni, M.V.; Chowdary, P.; Josephson, N.C.; Pabinger, I.; Hanabusa, H.; Gupta, N.; Kulkarni, R.; Fogarty, P.; et al. Phase 3 study of recombinant factor VIII Fc fusion protein in severe hemophilia A. Blood 2014, 123, 317–325. [Google Scholar] [CrossRef]
- Iorio, A.; Keepanasseril, A.; Foster, G.; Navarro-Ruan, T.; McEneny-King, A.; Edginton, A.N.; Thabane, L.; WAPPS-Hemo co-investigator network. Development of a Web-Accessible Population Pharmacokinetic Service-Hemophilia (WAPPS-Hemo): Study Protocol. JMIR Res. Protoc. 2016, 5, e239. [Google Scholar] [CrossRef]
- van Leeuwen, F.H.P.; van Bergen, E.P.D.; Timmer, M.A.; van Vulpen, L.F.D.; Schutgens, R.E.G.; de Jong, P.A.; Fischer, K.; Foppen, W. MRI evidence for subclinical joint bleeding in a Dutch population of people with severe hemophilia on prophylaxis. J. Thromb. Haemost. 2023. [Google Scholar] [CrossRef]
- De la Corte-Rodriguez, H.; Rodriguez-Merchan, E.C.; Alvarez-Roman, M.T.; Martin-Salces, M.; Martinoli, C.; Jimenez-Yuste, V. The value of HEAD-US system in detecting subclinical abnormalities in joints of patients with hemophilia. Expert. Rev. Hematol. 2018, 11, 253–261. [Google Scholar] [CrossRef]
- Gooding, R.; Thachil, J.; Alamelu, J.; Motwani, J.; Chowdary, P. Asymptomatic Joint Bleeding and Joint Health in Hemophilia: A Review of Variables, Methods, and Biomarkers. J. Blood Med. 2021, 12, 209–220. [Google Scholar] [CrossRef] [PubMed]
- Leiderman, K.; Sindi, S.S.; Monroe, D.M.; Fogelson, A.L.; Neeves, K.B. The Art and Science of Building a Computational Model to Understand Hemostasis. Semin. Thromb. Hemost. 2021, 47, 129–138. [Google Scholar] [CrossRef]
- Iorio, A.; Edginton, A.N.; Blanchette, V.; Blatny, J.; Boban, A.; Cnossen, M.; Collins, P.; Croteau, S.E.; Fischer, K.; Hart, D.P.; et al. Performing and interpreting individual pharmacokinetic profiles in patients with Hemophilia A or B: Rationale and general considerations. Res. Pract. Thromb. Haemost. 2018, 2, 535–548. [Google Scholar] [CrossRef]
- Blanchette, V.S.; Zunino, L.; Grassmann, V.; Barnes, C.; Carcao, M.D.; Curtin, J.; Jackson, S.; Khoo, L.; Komrska, V.; Lillicrap, D.; et al. A Practical, One-Clinic Visit Protocol for Pharmacokinetic Profile Generation with the ADVATE myPKFiT Dosing Tool in Severe Hemophilia A Subjects. Thromb. Haemost. 2021, 121, 1326–1336. [Google Scholar] [CrossRef] [PubMed]
- Young, G.; Mahlangu, J.; Kulkarni, R.; Nolan, B.; Liesner, R.; Pasi, J.; Barnes, C.; Neelakantan, S.; Gambino, G.; Cristiano, L.M.; et al. Recombinant factor VIII Fc fusion protein for the prevention and treatment of bleeding in children with severe hemophilia A. J. Thromb. Haemost. 2015, 13, 967–977. [Google Scholar] [CrossRef] [PubMed]
- Konkle, B.A. Von Willebrand factor and aging. Semin Thromb. Hemost. 2014, 40, 640–644. [Google Scholar] [CrossRef] [PubMed]
- Lalezari, S.; Martinowitz, U.; Windyga, J.; Enriquez, M.M.; Delesen, H.; Schwartz, L.; Scharrer, I. Correlation between endogenous VWF: Ag and PK parameters and bleeding frequency in severe haemophilia A subjects during three-times-weekly prophylaxis with rFVIII-FS. Haemophilia 2014, 20, e15–e22. [Google Scholar] [CrossRef] [PubMed]
- Liumbruno, G.M.; Franchini, M. Beyond immunohaematology: The role of the ABO blood group in human diseases. Blood Transfus. 2013, 11, 491–499. [Google Scholar]
- Gill, J.C.; Endres-Brooks, J.; Bauer, P.J.; Marks, W.J., Jr.; Montgomery, R.R. The effect of ABO blood group on the diagnosis of von Willebrand disease. Blood 1987, 69, 1691–1695. [Google Scholar] [CrossRef]
- James, P.D.; Connell, N.T.; Ameer, B.; Di Paola, J.; Eikenboom, J.; Giraud, N.; Haberichter, S.; Jacobs-Pratt, V.; Konkle, B.; McLintock, C.; et al. ASH ISTH NHF WFH 2021 guidelines on the diagnosis of von Willebrand disease. Blood Adv. 2021, 5, 280–300. [Google Scholar] [CrossRef] [PubMed]
- Mehic, D.; Hofer, S.; Jungbauer, C.; Kaider, A.; Haslacher, H.; Eigenbauer, E.; Rejtő, J.; Schwartz, D.; Jilma, B.; Ay, C.; et al. Association of ABO blood group with bleeding severity in patients with bleeding of unknown cause. Blood Adv. 2020, 4, 5157–5164. [Google Scholar] [CrossRef] [PubMed]
- Shipe, M.E.; Deppen, S.A.; Farjah, F.; Grogan, E.L. Developing prediction models for clinical use using logistic regression: An overview. J. Thorac. Dis. 2019, 11 (Suppl. 4), S574–S584. [Google Scholar] [CrossRef] [PubMed]
- Grant, S.W.; Collins, G.S.; Nashef, S.A.M. Statistical Primer: Developing and validating a risk prediction model. Eur. J. Cardiothorac. Surg. 2018, 54, 203–208. [Google Scholar] [CrossRef]
- Altman, D.G.; Vergouwe, Y.; Royston, P.; Moons, K.G. Prognosis and prognostic research: Validating a prognostic model. BMJ 2009, 338, b605. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Clinical Variables Mean ± SD, Range /Case Number (%) | Development Cohort 2019–2020 (N = 50) | Validation Cohort 2021 (N = 35) | p Value |
|---|---|---|---|
| Age (year) † mean ± SD | 34.6 ± 15.9 | 35.5 ± 14.2 | 0.7999 |
| median, range (y) | 33.5, range 8–64 | 33, range 13–61 | |
| Age § < 20 | 10 (20) | 5 (14.3) | 0.4964 |
| ≥20 | 40 (80) | 30 (85.7) | |
| BMI (kg/m2) † | 24.1 ± 3.4, range 17.1–35 | 24.4 ± 4.1, range 15.5–33 | 0.7845 |
| Body weight (kg) † | 67.6 ± 14.6, range 31.3–35 | 70.7 ± 13.2, range 48.3–102 | 0.3152 |
| ABO blood group ‡ | |||
| Non-O group | 29 (58) | 23 (65.7) | 0.007 ** |
| O group | 21 (42) | 12 (34.3) | |
| Inhibitor history ‡ | |||
| Negative | 43 (86) | 32 (91.4) | 0.5143 |
| Positive | 7 (14) | 3 (8.6) | |
| HCV infection § | |||
| Negative | 20 (40) | 21 (60) | 0.0694 |
| Positive | 30 (60) | 14 (40) | |
| HIV infection ‡ | |||
| Negative | 47 (94) | 35 (100) | 0.2647 |
| Positive | 3 (6) | 0 (0) | |
| Hct (%) † | 43.8 ± 4.3, range 29.9–52.6 | 44.7 ± 3.7, range 37.4–52.1 | 0.3283 |
| Baseline VWF:Ag (%) † | 112.5 ± 54.1, range 50–294.7 ¶ | 112.8 ± 43.0, range 48.8–241 | 0.9750 |
| Baseline VWF:activity (%) † | 103.4 ± 52.3, range 41.3–307 ¶ | 97.3 ± 48.7, range 41–243 | 0.5937 |
| VWF:activity/VWF:Ag ratio † | 0.93 ± 0.12, range 0.67–1.21 ¶ | 0.85 ± 0.18, range 0.4–1.25 | 0.0245 * |
| rFVIII-Fc half life (h) † | 20.1 ± 6.58 | 18.7 ± 7.1 | 0.3615 |
| median, range (h) | 20.75, range 8.25–41.5 | 17.3, range 8–39 |
| Case Number (%) | rFVIII-Fc Half Life (h) (Mean ± SD) | p Value | |
|---|---|---|---|
| Age (year) † | 50 (100) | ||
| <20 | 10 (20) | 13.68 ± 4.09 | 0.0005 *** |
| ≥20 | 40 (80) | 21.67 ± 6.11 | |
| BMI (kg/m2) †,‡ | 50 (100) | ||
| <24 | 25 (50) | 17.52 ± 4.74 | 0.0078 ** |
| ≥24 | 25 (50) | 22.62 ± 7.23 | |
| Body weight (kg) †,‡ | 50 (100) | ||
| <67.6 | 28 (56) | 18.29 ± 5.82 | 0.1498 |
| ≥67.6 | 22 (44) | 22.34 ± 6.91 | |
| ABO blood group † | 50 (100) | ||
| Non-O group | 29 (58) | 22.83 ± 6.46 | 0.0003 *** |
| O group | 21 (42) | 16.26 ± 4.61 | |
| Hct (%) †,‡ | 50 (100) | ||
| <43.8 | 22 (44) | 18.42 ± 5.92 | 0.3251 |
| ≥43.8 | 28 (56) | 21.37 ± 6.88 | |
| Inhibitor history † | 50 (100) | ||
| Negative | 43 (86) | 20.80 ± 6.47 | 0.0878 |
| Positive | 7 (14) | 15.61 ± 5.78 | |
| HCV infection † | 50 (100) | ||
| Negative | 20 (40) | 16.93 ± 4.88 | 0.0079 ** |
| Positive | 30 (60) | 22.17 ± 6.79 | |
| HIV infection † | 50 (100) | ||
| Negative | 47 (94) | 19.90 ± 6.74 | 0.205 |
| Positive | 3 (6) | 22.75 ± 1.98 | |
| Baseline VWF:Ag (%) † | 46 (100) | ||
| <100 ‡ | 24 (52) | 16.58 ± 4.90 | 0.0108 * |
| ≥100 | 22 (48) | 23.44 ± 6.88 | |
| Baseline VWF: activity (%) † | 46 (100) | ||
| <100 | 29 (63) | 17.07 ± 4.59 | 0.0014 ** |
| ≥100 | 17 (37) | 24.63 ± 7.44 | |
| VWF: activity/VWF:Ag ratio †,‡ | 46 (100) | ||
| <0.93 | 23 (50) | 19.13 ± 6.87 | 0.7835 |
| ≥0.93 | 23 (50) | 20.60 ± 6.82 |
| Parameter | Coefficient | 95% CI | p-Value | |
|---|---|---|---|---|
| Age (year) | 0.254 | 0.110 | 0.398 | 0.0013 ** |
| BMI (kg/m2) | 1.054 | 0.347 | 1.761 | 0.0052 ** |
| Body weight (kg) | 0.233 | 0.041 | 0.425 | 0.0194 * |
| Hct (%) | 0.211 | −0.520 | 0.942 | 0.5562 |
| Inhibitor history † | −4.986 | −13.549 | 3.578 | 0.2413 |
| HCV infection † | 5.481 | −0.435 | 11.397 | 0.0679 |
| HIV infection † | −0.087 | −8.904 | 8.730 | 0.9839 |
| Baseline VWF:Ag (IU/mL) | 7.351 | 4.075 | 10.628 | 0.0001 *** |
| Baseline VWF:activity (IU/mL) | 5.638 | 1.848 | 9.427 | 0.0052 ** |
| VWF:activity/VWF:Ag ratio | 5.036 | −16.959 | 27.031 | 0.6408 |
| Parameter | Coefficient | 95% CI | p-Value | |
|---|---|---|---|---|
| Age (year) | 0.172 | 0.050 | 0.294 | 0.0084 ** |
| BMI (kg/m2) | −0.120 | −0.766 | 0.526 | 0.7017 |
| Body weight (kg) | 0.065 | −0.066 | 0.195 | 0.3119 |
| Hct (%) | 0.247 | −0.272 | 0.766 | 0.3307 |
| Inhibitor history † | −3.141 | −8.446 | 2.165 | 0.2296 |
| HCV infection † | 4.375 | 0.519 | 8.231 | 0.0284 * |
| HIV infection † | 0 | - | - | - |
| Baseline VWF:Ag (IU/mL) | 17.572 | 9.67 | 25.475 | 0.0002 *** |
| Baseline VWF:activity (IU/mL) | 17.793 | 10.076 | 25.51 | 0.0001 *** |
| VWF: activity/VWF: Ag ratio | 9.295 | −12.657 | 31.248 | 0.3854 |
| Parameter | Coefficient | 95% CI | p-Value | |
|---|---|---|---|---|
| ABO blood group † | −6.814 | −10.385 | −3.244 | 0.0004 *** |
| Age (year) | 0.261 | 0.161 | 0.362 | <0.0001 *** |
| BMI (kg/m2) | 0.756 | 0.222 | 1.291 | 0.0066 ** |
| Body weight (kg) | 0.181 | 0.055 | 0.306 | 0.0058 ** |
| Hct (%) | 0.123 | −0.388 | 0.633 | 0.6302 |
| Inhibitor history ‡ | −5.021 | −10.510 | 0.468 | 0.0720 |
| HCV infection ‡ | 6.316 | 2.536 | 10.096 | 0.0016 ** |
| HIV infection ‡ | 3.087 | −5.147 | 11.321 | 0.4539 |
| Baseline VWF: Ag (IU/mL) | 9.256 | 6.664 | 11.849 | <0.0001 *** |
| Baseline VWF: activity (IU/mL) | 7.697 | 4.397 | 10.997 | <0.0001 *** |
| VWF: activity/VWF: Ag ratio | 7.127 | −10.402 | 24.656 | 0.4170 |
| Parameter | Coefficient | 95% CI | p-Value | |
|---|---|---|---|---|
| Intercept | −0.812 | −15.133 | 13.508 | 0.9076 |
| Baseline VWF:Ag (IU/mL) | 6.065 | 2.749 | 9.380 | 0.0010 ** |
| BMI (kg/m2) | 0.629 | 0.015 | 1.243 | 0.0451 * |
| Adjusted-R2 = 0.5197 | ||||
| Parameter | Coefficient | 95% CI | p-Value | |
|---|---|---|---|---|
| Intercept | −0.683 | −15.650 | 14.285 | 0.9238 |
| Baseline VWF:Ag (IU/mL) | 13.301 | 6.815 | 19.787 | 0.0005 *** |
| Body weight (kg) | 0.268 | 0.118 | 0.419 | 0.0018 ** |
| BMI (kg/m2) | −1.166 | −1.911 | −0.421 | 0.0045 ** |
| VWF:activity/VWF:Ag ratio | 16.023 | 4.605 | 27.440 | 0.0091 ** |
| Adjusted-R2 = 0.7517 | ||||
| Parameter | Coefficient | 95% CI | p-Value | |
|---|---|---|---|---|
| Intercept | −1.760 | −15.900 | 12.381 | 0.8027 |
| Baseline VWF:Ag (IU/mL) | 7.243 | 4.632 | 9.855 | <0.0001 *** |
| Inhibitor history † | −3.844 | −7.229 | −0.459 | 0.0270 * |
| HCV infection † | 2.985 | 0.273 | 5.698 | 0.0319 * |
| O blood group ‡ | −2.826 | −5.512 | −0.140 | 0.0397 * |
| Hct (%) | 0.304 | 0.0003 | 0.608 | 0.0498 * |
| Adjusted-R2 = 0.6538 | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chang, C.-Y.; Chiou, S.-S.; Weng, T.-F.; Lin, P.-C.; Lai, S.-W.; Tsai, C.-H.; Liu, Y.-L.; Ku, J.-T.; Liao, Y.-M.; Tsai, J.-R.; et al. Clinical Predictors and Prediction Models for rFVIII-Fc Half Life in Real-World People with Severe Hemophilia A. J. Clin. Med. 2023, 12, 2207. https://doi.org/10.3390/jcm12062207
Chang C-Y, Chiou S-S, Weng T-F, Lin P-C, Lai S-W, Tsai C-H, Liu Y-L, Ku J-T, Liao Y-M, Tsai J-R, et al. Clinical Predictors and Prediction Models for rFVIII-Fc Half Life in Real-World People with Severe Hemophilia A. Journal of Clinical Medicine. 2023; 12(6):2207. https://doi.org/10.3390/jcm12062207
Chicago/Turabian StyleChang, Chia-Yau, Shyh-Shin Chiou, Te-Fu Weng, Pei-Chin Lin, Shiue-Wei Lai, Chen-Hua Tsai, Yen-Lin Liu, Jung-Tzu Ku, Yu-Mei Liao, Jia-Ruey Tsai, and et al. 2023. "Clinical Predictors and Prediction Models for rFVIII-Fc Half Life in Real-World People with Severe Hemophilia A" Journal of Clinical Medicine 12, no. 6: 2207. https://doi.org/10.3390/jcm12062207
APA StyleChang, C.-Y., Chiou, S.-S., Weng, T.-F., Lin, P.-C., Lai, S.-W., Tsai, C.-H., Liu, Y.-L., Ku, J.-T., Liao, Y.-M., Tsai, J.-R., Hu, S.-H., Cheng, C.-N., & Chen, Y.-C. (2023). Clinical Predictors and Prediction Models for rFVIII-Fc Half Life in Real-World People with Severe Hemophilia A. Journal of Clinical Medicine, 12(6), 2207. https://doi.org/10.3390/jcm12062207