
A Review, Update, and Commentary for the Cough without a Cause: Facts and Factoids of the Habit Cough


Abstract
1. Introduction
“The morbidity, cost, and impact of somatoform (functional) pediatric respiratory syndromes are far more impactful than that experienced by most of our severe asthmatics and CF patients. These conditions are NOT trivial, ‘just in your head’ conditions. A confident diagnostic approach and an optimistic therapeutic regimen are critically important.” (George Mallory MD)
2. Methods
3. Results
3.1. Chronology of Habit Cough
3.2. Clinical Characteristics of Habit Cough
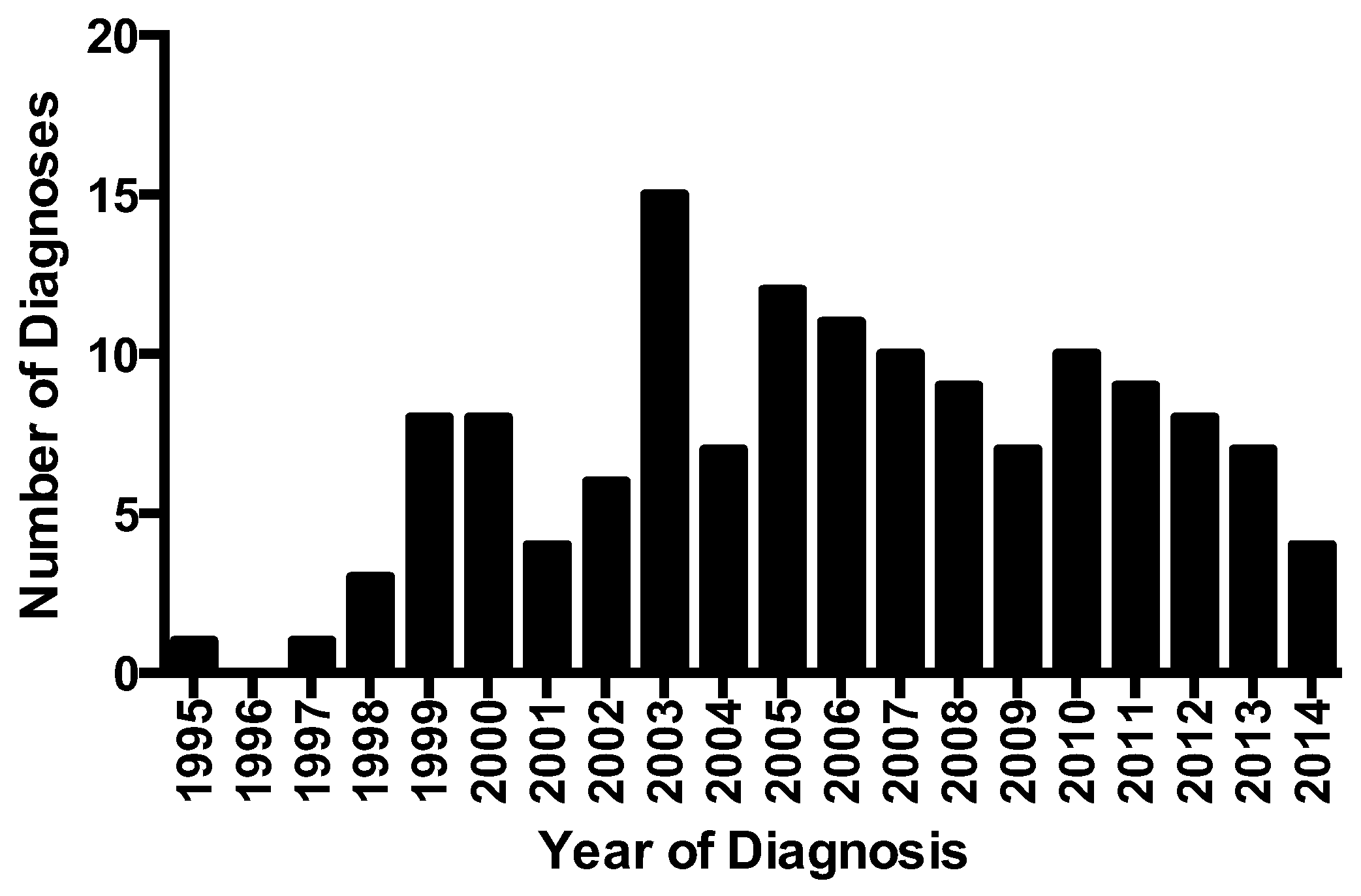
3.3. Epidemiology of Habit Cough
3.4. Etiology of Habit Cough
3.5. Treatment of Habit Cough
- Establish rapport with the patient and parents.
- Be honest and forthright with patients and parents.
- Tell the parents that you want to talk to the patient and ask them to sit quietly in the background, phones turned off.
- Body temperature water should be at the patient’s side or in hand to take small sips in anticipation of a cough.
- Explain the cough as a vicious cycle that started with an initial irritant that is now gone; it is now the cough itself that is causing the feeling that stimulates the coughing.
- Explain that cough is the body’s natural response to feeling that something is in their airway.
- Explain that the brain can control that response, but it takes a lot of concentration.
- Instruct the patient to focus on the provider of the suggestion therapy who is to keep up a relaxed soft patter.
- The patient is instructed to be aware when a cough may be coming and take a small sip of the water and hold the cough back.
- Begin with a request to hold the cough back for a defined period of time, beginning small and progressing as successes occur.
- Tell the patient that each second the cough is delayed makes it easier to suppress further coughing.
- Repeat expressions of confidence that the patient is developing the ability to resist the urge to cough: “It’s becoming easier to hold back the cough, isn’t it?” (Nodding your head generally makes the child nod their head in agreement.)
- When the patient shows that he or she is able to suppress the cough (usually after about 10 min), ask in a rhetorical manner, “You’re beginning to feel that you can resist the urge to cough, aren’t you?” (Say with an affirmative head nod.)
- Express confidence that if the urge to cough recurs, the patient can do the same thing at home (autosuggestion).
3.6. Outcome of Habit Cough
“Our daughter, Riley, is seven years old (will be eight in May). A few months back, she had a really bad cold which led to a bad cough. After a few weeks the cold symptoms went away except for that cough. There was no stop to it. Just so much coughing.I finally decided to just pull your video up on YouTube and we all sat there and watched it. It was very emotional for all of us and at the end Riley was in tears (we all were). We hugged for a time. She said to us “I can hold the cough back. And the…THE COUGHING STOPPED! Like turning off a switch. For four days now, I have not heard her cough except for a few random ones here and there. The cough is GONE!”
“He is doing so much better. He went back to school this week. The first 2 days he had to really work to control the cough and had a few bouts of having a difficult time of doing so. However, the last few days he hasn’t coughed at all and the urge is less and less.”
3.7. Clinical Course of Untreated Habit Cough
3.8. When Suggestion Therapy Is Not Effective
4. Discussion
4.1. What Is the Current Status of Identifying and Treating Habit Cough
4.2. Barriers to Diagnosis and Treatment
4.3. Guidelines for Chronic Cough from Professional Societies
4.4. Strengths and Limitations of This Report
5. Conclusions and Recommendations
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hurvitz, M.; Weinberger, M. Functional respiratory disorders in children. In Pulmonary Manifestations of Pediatric Diseases, Pediatr Clinics of North America. Pediatr. Clin. 2021, 68, 223–237. [Google Scholar]
- Willis, T. The London Practice of Physick, in the Pharmaceutic Rationalis; 1685; p. 265. [Google Scholar]
- Mercurius, F. Habitual Cough, in The Spirit of Diseases; Printed for Sarah Hawkins in George-Yard, in Lombard-Street; 1694; p. 118. [Google Scholar]
- Creighton, C. Illustrations of Unconscious Memory in Disease; HK Lewis: London, UK, 1886; p. 63. [Google Scholar]
- Berman, B.A. Habit cough in adolescent children. Ann. Allergy 1966, 24, 43–46. [Google Scholar]
- Lokshin, B.; Lindgren, S.; Weinberger, M.; Koviach, J. Outcome of habit cough in children treated with a brief session of suggestion therapy. Ann. Allergy 1991, 67, 579–582. [Google Scholar] [PubMed]
- Kravitz, H.; Gomberg, R.M.; Burnstine, R.C.; Hagler, S.; Korach, A. Psychogenic cough tic in children and adolescents. Nine case histories illustrate the need for re-evaluation of this common but frequently unrecognized problem. Clin. Pediatr. 1969, 8, 580–583. [Google Scholar] [CrossRef] [PubMed]
- Weinberg, E.G. ‘Honking’: Psychogenic cough tic in children. S. Afr. Med. J. 1980, 57, 198–200. [Google Scholar]
- Cohlan, S.Q.; Stone, S.M. The cough and the bedsheet. Pediatrics 1984, 74, 11–15. [Google Scholar] [CrossRef]
- Anbar, R.D.; Hall, H. Childhood habit cough treated with self-hypnosis. J. Pediatr. 2004, 144, 213–217. [Google Scholar] [CrossRef]
- Weinberger, M.; Hoegger, M. The cough without a cause: Habit cough syndrome. J. Allergy Clin. Immunol. 2015, 137, 930–931. [Google Scholar] [CrossRef]
- Wright, M.F.A.; Balfour-Lynn, I.M. Habit-tic cough: Presentation and outcome with simple reassurance. Pediatr. Pulmonol. 2018, 53, 512–516. [Google Scholar] [CrossRef]
- Papadopoulou, A.; Mermiri, D.-Z.T.; Gritzelas, G.; Tsouridi, O.; Dimara, D.; Yapijakis, C.; Chrousos, G.P. Increased incidence of stress-related tic habit cough in children during the recent Greek financial crisis. In Vivo 2021, 35, 1811–1820. [Google Scholar] [CrossRef]
- Chang, A.B.; Robertson, C.F.; Van Asperen, E.P. A multicenter study on chronic cough in children: Buren and etiologies based on a standardized management pathway. CHEST 2012, 1442, 943–950. [Google Scholar] [CrossRef]
- Rouadi, P.W.; Idriss, S.A.; Bousquet, J.; Laidlaw, T.M.; Azar, C.R.; Al-Ahmad, M.S.; Yañez, A.; Al-Nesf, M.A.Y.; Nsouli, T.M.; Bahna, S.L.; et al. WAO-ARIA consensus on chronic cough—Part II: Phenotypes and mechanisms of abnormal cough presentation—Updates in COVID-19. World Allergy Organ. J. 2021, 14, 24–26. [Google Scholar] [CrossRef] [PubMed]
- Di Cicco, M.; Tozzi, M.G.; Ragazzo, V.; Peroni, D.; Kantar, A. Chronic respiratory diseases other than asthma in children: The COVID-19 tsunami. Ital. J. Pediatr. 2021, 47, 220. [Google Scholar] [CrossRef] [PubMed]
- Doležalová, K.; Tuková, J.; Pohunek, P. The respiratory consequences of COVID-19 lasted for a median of 4 months in a cohort of children aged 2–18 years of age. Acta Paediatr. 2022, 111, 1201–1206. [Google Scholar] [CrossRef]
- Morice, A.H.; Millqvist, E.; Belvisi, M.G.; Bieksiene, K.; Birring, S.S.; Chung, K.F.; Negro, R.W.D.; Dicpinigaitis, P.; Kantar, A.; McGarvey, L.P.; et al. Expert opinion on the cough hypersensitivity syndrome in respiratory medicine. Eur. Respir. J. 2014, 44, 1132–1148. [Google Scholar] [CrossRef] [PubMed]
- Irwin, R.S.; Ownbey, R.; Cagle, P.T.; Stephen Baker, S.; Fraire, A.E. Interpreting the histopathology of chronic cough: A prospective, controlled, comparative study. CHEST 2006, 130, 362–370. [Google Scholar] [CrossRef] [PubMed]
- Shapiro, C.O.; Proskocil, B.J.; Oppegard, L.J.; Blum, E.D.; Kappel, N.L.; Chang, C.H.; Fryer, A.D.; Jacoby, D.B.; Costello, R.W.; Drake, M.G. Airway sensory nerve density is increased in chronic cough. Am. J. Respir. Crit. Care Med. 2021, 203, 348–355. [Google Scholar] [CrossRef] [PubMed]
- Slinger, C.; Mehdi, S.B.; Milan, S.J.; Dodd, S.; Matthews, J.; Vyas, A.; Marsden, P.A. Speech and language therapy for management of chronic cough. Cochrane Database Syst Rev. 2019, 7, CD013067. [Google Scholar] [CrossRef]
- Weinberger, M.; Buettner, D. Cures of the cough without a cause. Ann Allergy Asthma Immunol. 2021, 127, 381–383. [Google Scholar] [CrossRef]
- Weinberger, M. Commentary: The habit cough: Diagnosis and treatment. Pediatr. Pulmonol. 2018, 53, 535–537. [Google Scholar] [CrossRef]
- Weinberger, M. The habit cough syndrome and its variations. Lung 2012, 190, 45–53. [Google Scholar] [CrossRef]
- Rojas, A.R.; Sachs, M.I.; Yunginger, J.W.; O’Connell, E.J. Childhood involuntary cough syndrome: A long-term follow-up study. Ann Allergy 1991, 66, 106. [Google Scholar]
- Anbar, R.D. Changing Children’s Lives with Hypnosis: A Journey to the Center; Rowman & Littlefield: New York, NY, USA, 2021; Chapter 12. [Google Scholar]
- Chang, A.B.; Oppenheimer, J.J.; Irwin, R.S.; CHEST Expert Cough Panel. Managing chronic cough as a symptom in children and management algorithms—CHEST guideline and expert panel report. Chest 2020, 158, 303–329. [Google Scholar] [CrossRef] [PubMed]
- Bhatia, M.S.; Chandra, R.; Vaid, L. Psychogenic cough: A profile of 32 cases. Int. J. Psychiatry Med. 2002, 32, 353–360. [Google Scholar] [CrossRef] [PubMed]
- Gibson, P.G. Management of cough. J. Allergy Clin. Immunol. Pract. 2019, 7, 1724–1729. [Google Scholar] [CrossRef]
- Smith, J.A.; Woodcock, A. Chronic cough. N. Engl. J. Med. 2016, 375, 1544–1551. [Google Scholar] [CrossRef] [PubMed]
- Dicpinigaitis, P.V. Thoughts on one thousand chronic cough patients. Lung 2012, 190, 593–596. [Google Scholar] [CrossRef][Green Version]
- Lai, K.; Peng, W.; Zhan, W.; Xie, J.-X.; Tian, J.; Zuo, X.-P.; Long, L.; Tang, J.-M.; Pan, J.-Y.; Jiang, M.; et al. Clinical characteristics in adult patients with somatic cough syndrome. Ther. Adv. Respir. Dis. 2022, 16, 17534666221092993. [Google Scholar] [CrossRef]
- Gay, M.; Blager, F.; Bartsch, K.; Emery, C.F.; Rosenstiel-Gross, A.K.; Spears, J. Psychogenic habit cough: Review and case reports. J. Clin. Psychiatry 1987, 48, 483–486. [Google Scholar]
- Mastrovich, J.D.; Greenberger, P.A. Psychogenic cough in adults: A report of two cases and review of the literature. Allergy Asthma Proc. 2003, 23, 27–33. [Google Scholar]
- Lajonchere, C.; Nortz, M.; Finger, S. Gillles de la Tourette and the discovery of Tourette syndrome. Includes a translation of his 1884 article. Arch Neurol. 1996, 53, 567–574. [Google Scholar] [CrossRef]
- Weinberger, M.; Pringsheim, T. Point-counterpoint and rebuttals: Is the term habit cough an inaccurate use of the term? Chest 2019, 156, 821–825. [Google Scholar] [CrossRef] [PubMed]
- Duncan, K.L.; Faust, R.A. Tourette syndrome manifest as chronic cough. Int. J. Pediatr. Otorhinolaryngol. 2002, 65, 65–68. [Google Scholar] [CrossRef]
- Tan, H.; Büyükavci, M.; Arık, A. Tourette’s syndrome manifests as chronic persistent cough. Yonsei Med. J. 2004, 45, 145–149. [Google Scholar] [CrossRef] [PubMed]
- Morice, A.H.; Millqvist, E.; Bieksiene, K.; Birring, S.S.; Dicpinigaitis, P.; Ribas, C.D.; Boon, M.H.; Kantar, A.; Lai, K.; McGarvey, L.; et al. ERS guidelines on the diagnosis and treatment of chronic cough in adults and children. Eur. Respir. J. 2019, 55, 1901136. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
|
| It has been suggested that children with habit cough appear to not care about their cough. While children may adapt to living with a chronic cough, few if any have appeared to us content about their cough. It is life-altering for the child and their family and, if asked, the children express concern about their cough. They are not indifferent to their cough. |
|
| This claim was made in a 2020 Chest publication [27]. The reference used to support that claim was a case series of adults at a psychiatric facility [28]. While there are occasional patients with school phobia as a factor, our experience does not support the assertion that school phobia is a common concern as a cause of habit cough. We have observed that the children with habit cough are generally concerned about missing school. Those who had been out of school because of the cough are generally enthusiastic about returning. |
|
| We have been contacted by 20 adults from eight countries with chronic cough who reported to us by email that their coughing was stopped by suggestion therapy from viewing the video made available by coauthor DB (see Figure 2). In addition, three adults had their chronic cough resolved by hypnosis therapy performed by coauthor RA. It is not known how many with habit cough are among the 40% of adults with idiopathic or refractory cough [29,30]. Our serendipitous experience identified 20 adults with the same clinical characteristics as the children with habit cough who described cessation of cough by suggestion therapy. Interestingly, Peter Dicpinigaitis, editor of the journal Lung, states in a publication that among 1000 patients he has never seen psychogenic cough (a euphemism for habit cough) [31]. However, Dr. Kefang Lai described 23 adults that he termed “somatic cough syndrome” (another euphemism for habit cough) [32]. Other case reports of psychogenic cough in adults also has been described [33,34]. |
|
| While this has been stated without support in guidelines for chronic cough, habit cough has a sufficiently distinctive clinical presentation that major centers experienced with this disorder make the diagnosis with little testing or therapeutic trials. Efforts to examine for other causes of cough only add to the morbidity and cost [11,12]. Treating habit cough early in the course of its clinical presentation can prevent unnecessary and expensive investigations that delay resolution. |
|
| This was claimed by Dr. Alyn Morice, a prominent cough specialist, who wrote in an email, “You are describing, but failing to recognize, a forme fruste of Tourette’s syndrome”. However, cough is not supported as a usual finding in Tourette’s 1884 publication [35]. Moreover, during interviews with parents of children with Tourette’s, cough was readily recognized as cough and not a tic and was regarded as separate from the symptoms of Tourette’s in their child. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Weinberger, M.; Buettner, D.; Anbar, R.D. A Review, Update, and Commentary for the Cough without a Cause: Facts and Factoids of the Habit Cough. J. Clin. Med. 2023, 12, 1970. https://doi.org/10.3390/jcm12051970
Weinberger M, Buettner D, Anbar RD. A Review, Update, and Commentary for the Cough without a Cause: Facts and Factoids of the Habit Cough. Journal of Clinical Medicine. 2023; 12(5):1970. https://doi.org/10.3390/jcm12051970
Chicago/Turabian StyleWeinberger, Miles, Dennis Buettner, and Ran D. Anbar. 2023. "A Review, Update, and Commentary for the Cough without a Cause: Facts and Factoids of the Habit Cough" Journal of Clinical Medicine 12, no. 5: 1970. https://doi.org/10.3390/jcm12051970
APA StyleWeinberger, M., Buettner, D., & Anbar, R. D. (2023). A Review, Update, and Commentary for the Cough without a Cause: Facts and Factoids of the Habit Cough. Journal of Clinical Medicine, 12(5), 1970. https://doi.org/10.3390/jcm12051970