
Relationship between Postoperative Anterior Chamber Depth and Refraction Based on the Haptic Fix Position in Intraocular Lens Intrascleral Fixation


Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gabor, S.G.; Pavlidis, M.M. Sutureless intrascleral posterior chamber intraocular lens fixation. J. Cataract. Refract. Surg. 2007, 33, 1851–1854. [Google Scholar] [CrossRef] [PubMed]
- Yamane, S.; Inoue, M.; Arakawa, A.; Kadonosono, K. Sutureless 27-gauge needle-guided intrascleral intraocular lens implantation with lamellar scleral dissection. Ophthalmology 2014, 121, 61–66. [Google Scholar] [CrossRef] [PubMed]
- Yamane, S.; Sato, S.; Maruyama-Inoue, M.; Kadonosono, K. Flanged intrascleral intraocular lens fixation with double-needle technique. Ophthalmology 2017, 124, 1136–1142. [Google Scholar] [CrossRef] [PubMed]
- Abbey, A.M.; Hussain, R.M.; Shah, A.R.; Faia, L.J.; Wolfe, J.D.; Williams, G.A. Sutureless scleral fixation of intraocular lenses: Outcomes of two approaches. The 2014 Yasuo Tano Memorial Lecture. Graefes Arch. Clin. Exp. Ophthalmol. 2015, 253, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Ni, S.; Li, S.; Zheng, Q.; Wu, J.; Liang, G.; Xu, W. Comparison of three intraocular lens implantation procedures for aphakic eyes with insufficient capsular support: A network meta-analysis. Am. J. Ophthalmol. 2018, 192, 10–19. [Google Scholar] [CrossRef] [PubMed]
- Higashide, T.; Shimizu, F.; Nishimura, A.; Sugiyama, K. Anterior segment optical coherence tomography findings of reverse pupillary block after scleral-fixated sutured posterior chamber intraocular lens implantation. J. Cataract Refract. Surg. 2009, 35, 1540–1547. [Google Scholar] [CrossRef] [PubMed]
- Kakisu, M.; Baba, T.; Tatsumi, T.; Iwase, T.; Nizawa, T.; Miura, G.; Yamamoto, S. Refractive errors after sutureless intrascleral fixation of intraocular lens. Graefes Arch. Clin. Exp. Ophthalmol. 2021, 259, 3003–3009. [Google Scholar] [CrossRef] [PubMed]
- Aykut, V.; Esen, F.; Sali, F.; Oguz, H. Refractive outcome of trocar-assisted sutureless scleral fixation with 3-piece intraocular lenses. Int. Ophthalmol. 2021, 41, 2689–2694. [Google Scholar] [CrossRef] [PubMed]
- Retzlaff, J.A.; Sanders, D.R.; Kraff, M.C. Development of the SRK/T intraocular lens implant power calculation formula. J. Cataract Refract. Surg. 1990, 16, 333–340. [Google Scholar] [CrossRef] [PubMed]
- Holladay, J.T.; Piers, P.A.; Koranyi, G.; van der Mooren, M.; Norrby, N.S. A new intraocular lens design to reduce spherical aberration of pseudophakic eyes. J. Refract. Surg. 2002, 18, 683–691. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| ISF 1.5 | ISF 2.0 | ZCB | p | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Mean | SD | ISF 1.5 vs. ISF 2.0 | ISF 1.5 vs. ZCB | ISF 2.0 vs. ZCB | |
| n | 45 | 55 | 50 | ||||||
| Female | 19 | 16 | 20 | ||||||
| Age (years) | 73.13 | 1.75 | 70.67 | 1.58 | 66.96 | 1.66 | 0.55 | 0.03 * | 0.24 |
| Kf (mm) | 7.69 | 0.27 | 7.75 | 0.34 | 7.82 | 0.28 | 0.11 | 0.59 | 0.51 |
| Ks (mm) | 7.55 | 0.04 | 7.57 | 0.04 | 7.67 | 0.04 | 0.96 | 0.12 | 0.16 |
| Axial length (mm) | 23.98 | 0.25 | 24.38 | 0.22 | 24.15 | 0.23 | 0.46 | 0.88 | 0.75 |
| CDVA (LogMAR(Snellen)) | 0.3(20/39.9) | 0.53 | 0.24(20/34.8) | 0.55 | −0.12(20/15.2) | 0.1 | 0.79 | <0.01 * | <0.01 * |
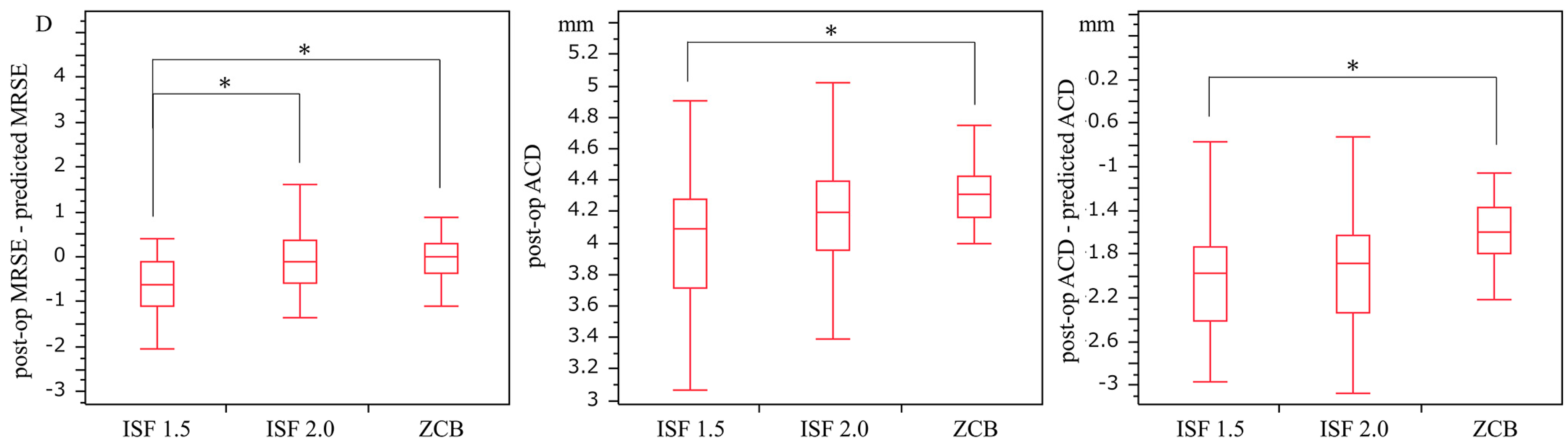
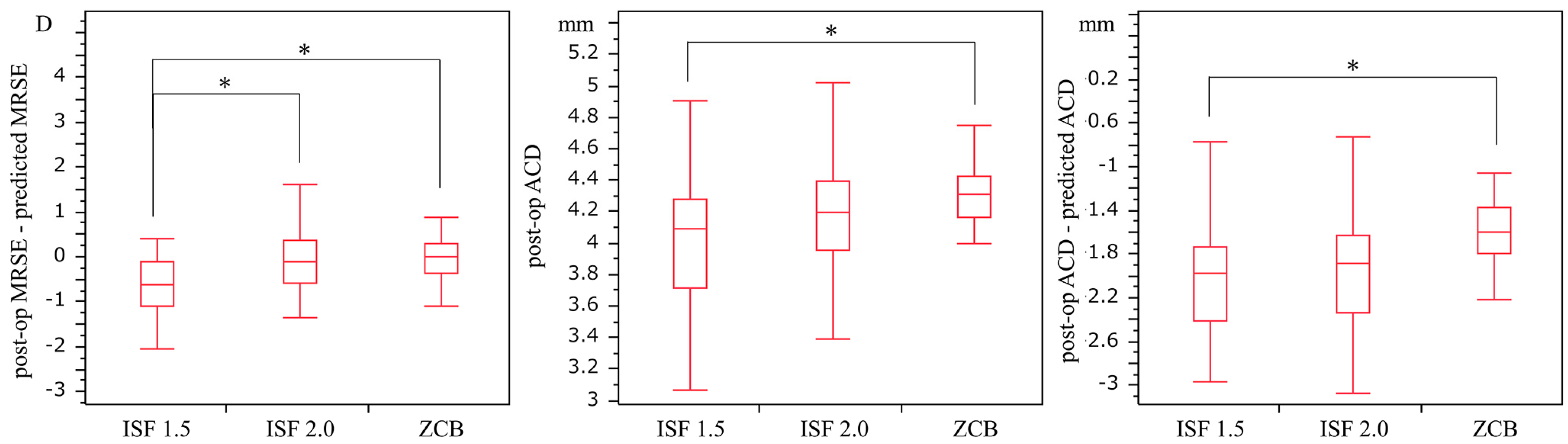
| post-op MRSE (D) | −0.76 | 1.37 | −0.57 | 1.18 | −0.05 | 0.43 | 0.65 | <0.01 * | 0.05 |
| Sex | Age | L or R | ISF | IOL Power | Axial Length | Kf | Ks | Post-Op ACD | Medical History |
|---|---|---|---|---|---|---|---|---|---|
| M | 55 | R | ISF 1.5 | 10 | 27.76 | 7.95 | 7.84 | 3.92 | Asthma |
| M | 75 | R | ISF 1.5 | 10 | 26.45 | 7.43 | 7.26 | 3.99 | |
| M | 66 | L | ISF 1.5 | 21 | 23.19 | 7.55 | 7.37 | 4.24 | |
| M | 37 | L | ISF 1.5 | 16.5 | 28.32 | 8.31 | 9.07 | 3.51 | Atopic dermatitis |
| M | 52 | R | ISF 2.0 | 10 | 25.59 | 7.13 | 6.92 | 4.52 | |
| F | 63 | L | ISF 2.0 | 10 | 30.44 | 8.33 | 8.09 | 4.16 | |
| M | 47 | L | ISF 2.0 | 21.5 | 23.96 | 7.89 | 7.89 | 4.07 | Atopic dermatitis, diabetic mellitus |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Noguchi, S.; Nakakura, S.; Noguchi, A.; Tabuchi, H. Relationship between Postoperative Anterior Chamber Depth and Refraction Based on the Haptic Fix Position in Intraocular Lens Intrascleral Fixation. J. Clin. Med. 2023, 12, 1815. https://doi.org/10.3390/jcm12051815
Noguchi S, Nakakura S, Noguchi A, Tabuchi H. Relationship between Postoperative Anterior Chamber Depth and Refraction Based on the Haptic Fix Position in Intraocular Lens Intrascleral Fixation. Journal of Clinical Medicine. 2023; 12(5):1815. https://doi.org/10.3390/jcm12051815
Chicago/Turabian StyleNoguchi, Santaro, Shunsuke Nakakura, Asuka Noguchi, and Hitoshi Tabuchi. 2023. "Relationship between Postoperative Anterior Chamber Depth and Refraction Based on the Haptic Fix Position in Intraocular Lens Intrascleral Fixation" Journal of Clinical Medicine 12, no. 5: 1815. https://doi.org/10.3390/jcm12051815
APA StyleNoguchi, S., Nakakura, S., Noguchi, A., & Tabuchi, H. (2023). Relationship between Postoperative Anterior Chamber Depth and Refraction Based on the Haptic Fix Position in Intraocular Lens Intrascleral Fixation. Journal of Clinical Medicine, 12(5), 1815. https://doi.org/10.3390/jcm12051815