

Efficacy of PARP Inhibitor, Platinum, and Immunotherapy in BRCA-Mutated HER2-Negative Breast Cancer Patients: A Systematic Review and Network Meta-Analysis



Abstract
1. Introduction
2. Materials and Methods
2.1. Design
2.2. Search Strategy
2.3. Study Selection
2.4. Data Extraction
2.5. Data Analysis
2.6. Bias Assessment
3. Results
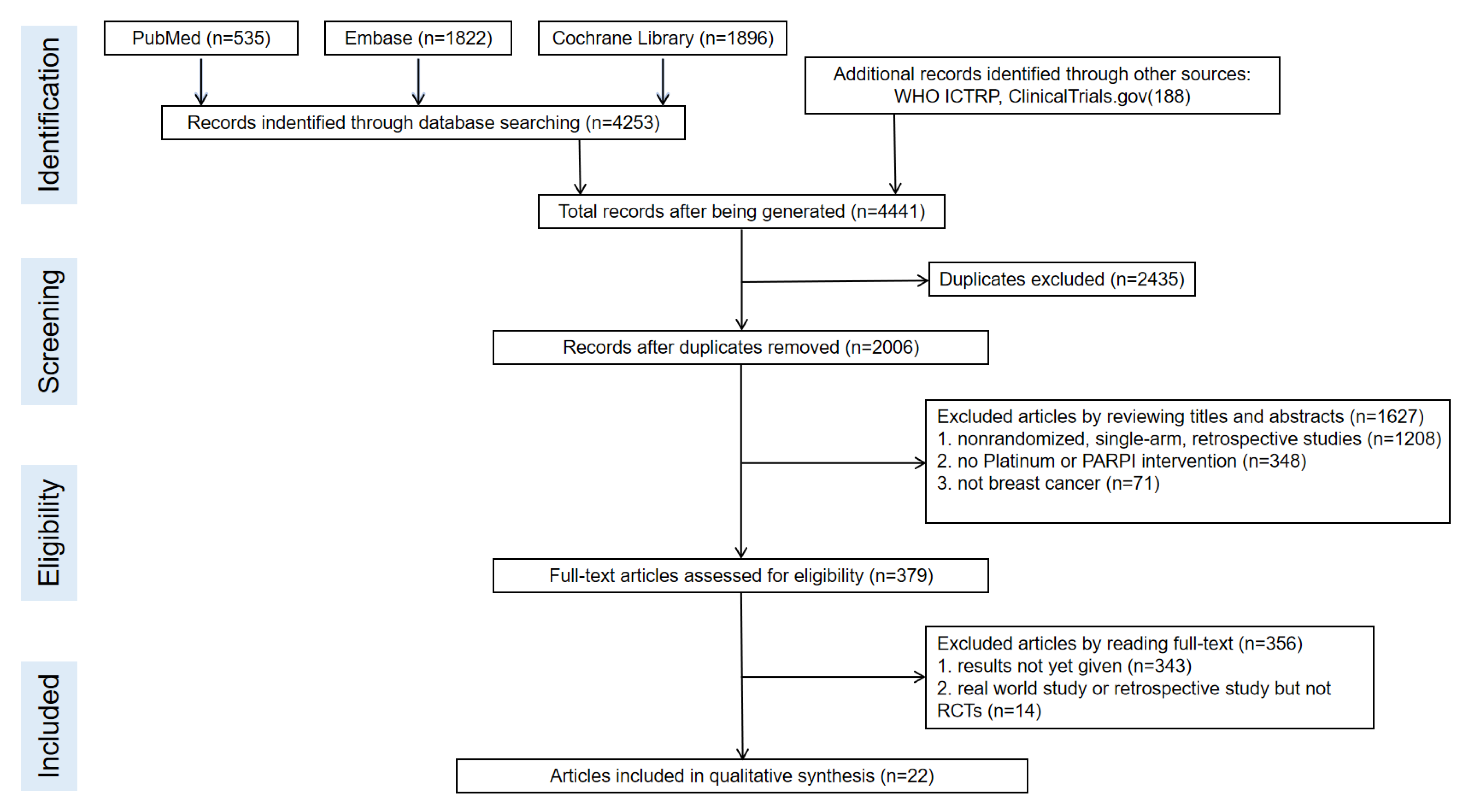
3.1. Search Results and Study Characteristics (Figure 1 and Figure 2, and Table 1)
3.2. Overall Survival (OS) (Figure 2 and Figure 3, Table 2, and Supplementary Materials)
3.3. Progression-Free Survival (PFS) (Figure 2 and Figure 3, Table 2, and Supplementary Materials)
3.4. Disease-Free Survival (DFS) (Figure 2 and Figure 3, Table 2, and Supplementary Materials)
3.5. Overall Response Rate (ORR) (Figure 2 and Figure 3, Table 2, and Supplementary Materials)
3.6. Pathologic Complete Response (pCR) (Figure 2 and Figure 3, Table 2, and Supplementary Materials)
3.7. Subgroup Analysis of TNBC and Hormone Receptor (HR)-Positive (Table 2 and Supplementary Materials)
3.8. Publication Bias and Risk of Bias in Randomized Trials (Figures S1 and S2 in Supplementary Materials)
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics 2022. CA Cancer J. Clin. 2022, 72, 7–33. [Google Scholar] [CrossRef] [PubMed]
- John, E.M.; Miron, A.; Gong, G.; Phipps, A.I.; Felberg, A.; Li, F.P.; West, D.W.; Whittemore, A.S. Prevalence of Pathogenic BRCA1 Mutation Carriers in 5 US Racial/Ethnic Groups. JAMA 2007, 298, 2869–2876. [Google Scholar] [CrossRef] [PubMed]
- Malone, K.E.; Daling, J.R.; Doody, D.R.; Hsu, L.; Bernstein, L.; Coates, R.J.; Marchbanks, P.A.; Simon, M.S.; McDonald, J.A.; Norman, S.A.; et al. Prevalence and Predictors of BRCA1 and BRCA2 Mutations in a Population-Based Study of Breast Cancer in White and Black American Women Ages 35 to 64 Years. Cancer Res. 2006, 66, 8297–8308. [Google Scholar] [CrossRef] [PubMed]
- Neiger, H.; Siegler, E.; Shi, Y. Breast Cancer Predisposition Genes and Synthetic Lethality. Int. J. Mol. Sci. 2021, 22, 5614. [Google Scholar] [CrossRef] [PubMed]
- Zhang, D.; Baldwin, P.; Leal, A.S.M.; Carapellucci, S.; Sridhar, S.; Liby, K.T. A nano-liposome formulation of the PARP inhibitor Talazoparib enhances treatment efficacy and modulates immune cell populations in mammary tumors of BRCA-deficient mice. Theranostics 2019, 9, 6224–6238. [Google Scholar] [CrossRef]
- Maeshima, Y.; Oseto, K.; Katsuragi, R.; Yoshimoto, Y.; Takahara, S.; Yamauchi, A. Experience with Bilateral Risk-Reducing Mastectomy for an Unaffected BRCA Mutation Carrier. J. Breast Cancer 2016, 19, 218–221. [Google Scholar] [CrossRef]
- Mavaddat, N.; Barrowdale, D.; Andrulis, I.L.; Domchek, S.M.; Eccles, D.; Nevanlinna, H.; Ramus, S.J.; Spurdle, A.; Robson, M.; Sherman, M.; et al. Pathology of breast and ovarian cancers among BRCA1 and BRCA2 mutation carriers: Results from the Consortium of Investigators of Modifiers of BRCA1/2 (CIMBA). Cancer Epidemiol. Biomark. Prev. 2012, 21, 134–147. [Google Scholar] [CrossRef]
- Cao, X.; Ren, X.; Zhou, Y.; Mao, F.; Lin, Y.; Wu, H.; Sun, Q. VISTA Expression on Immune Cells Correlates With Favorable Prognosis in Patients With Triple-Negative Breast Cancer. Front. Oncol. 2021, 10, 583966. [Google Scholar] [CrossRef]
- De Talhouet, S.; Peron, J.; Vuilleumier, A.; Friedlaender, A.; Viassolo, V.; Ayme, A.; Bodmer, A.; Treilleux, I.; Lang, N.; Tille, J.C.; et al. Clinical outcome of breast cancer in carriers of BRCA1 and BRCA2 mutations according to molecular subtypes. Sci. Rep. 2020, 10, 7073. [Google Scholar] [CrossRef]
- Van den Broek, A.J.; Schmidt, M.K.; van’t Veer, L.J.; Tollenaar, R.A.; Leeuwen, F.E. Worse breast cancer prognosis of BRCA1/BRCA2 mutation carriers: What’s the evidence? A sys-tematic review with meta-analysis. PLoS ONE 2015, 10, e0120189. [Google Scholar] [CrossRef]
- Tarsounas, M.; Sung, P. The antitumorigenic roles of BRCA1–BARD1 in DNA repair and replication. Nat. Rev. Mol. Cell Biol. 2020, 21, 284–299. [Google Scholar] [CrossRef] [PubMed]
- Konstantinopoulos, P.A.; Spentzos, D.; Karlan, B.Y.; Taniguchi, T.; Fountzilas, E.; Francoeur, N.; Levine, D.A.; Cannistra, S.A. Gene Expression Profile ofBRCAness That Correlates with Responsiveness to Chemotherapy and with Outcome in Patients with Epithelial Ovarian Cancer. J. Clin. Oncol. 2010, 28, 3555–3561. [Google Scholar] [CrossRef] [PubMed]
- Easton, D.F. How many more breast cancer predisposition genes are there? Breast Cancer Res. 1999, 1, 14–17. [Google Scholar] [CrossRef] [PubMed]
- Amé, J.C.; Spenlehauer, C.; de Murcia, G. The PARP superfamily. Bioessays 2004, 26, 882–893. [Google Scholar] [CrossRef] [PubMed]
- Dhoonmoon, A.; Schleicher, E.M.; Clements, K.E.; Nicolae, C.M.; Moldovan, G.-L. Genome-wide CRISPR synthetic lethality screen identifies a role for the ADP-ribosyltransferase PARP14 in DNA replication dynamics controlled by ATR. Nucleic Acids Res. 2020, 48, 7252–7264. [Google Scholar] [CrossRef]
- Bryant, H.E.; Schultz, N.; Thomas, H.D.; Parker, K.M.; Flower, D.; Lopez, E.; Kyle, S.; Meuth, M.; Curtin, N.J.; Helleday, T. Specific killing of BRCA2-deficient tumours with inhibitors of poly(ADP-ribose) polymerase. Nature 2005, 434, 913–917. [Google Scholar] [CrossRef]
- Robson, M.E.; Tung, N.; Conte, P.; Im, S.-A.; Senkus, E.; Xu, B.; Masuda, N.; Delaloge, S.; Li, W.; Armstrong, A.; et al. OlympiAD final overall survival and tolerability results: Olaparib versus chemotherapy treatment of physician’s choice in patients with a germline BRCA mutation and HER2-negative metastatic breast cancer. Ann. Oncol. 2019, 30, 558–566. [Google Scholar] [CrossRef]
- Litton, J.K.; Hurvitz, S.A.; Mina, L.A.; Rugo, H.S.; Lee, K.H.; Gonçalves, A.; Diab, S.; Woodward, N.; Goodwin, A.; Yerushalmi, R.; et al. Talazoparib versus chemotherapy in patients with germline BRCA1/2-mutated HER2-negative advanced breast cancer: Final overall survival results from the EMBRACA trial. Ann. Oncol. 2020, 31, 1526–1535. [Google Scholar] [CrossRef]
- Telli, M.L.; Timms, K.M.; Reid, J.; Hennessy, B.; Mills, G.B.; Jensen, K.C.; Szallasi, Z.; Barry, W.T.; Winer, E.P.; Tung, N.M.; et al. Homologous Recombination Deficiency (HRD) Score Predicts Response to Platinum-Containing Neoadjuvant Chemotherapy in Patients with Triple-Negative Breast Cancer. Clin. Cancer Res. 2016, 22, 3764–3773. [Google Scholar] [CrossRef]
- Byrski, T.; Gronwald, J.; Huzarski, T.; Grzybowska, E.; Budryk, M.; Stawicka, M.; Mierzwa, T.; Szwiec, M.; Wiśniowski, R.; Siolek, M.; et al. Pathologic Complete Response Rates in Young Women with BRCA1-Positive Breast Cancers After Neoadjuvant Chemotherapy. J. Clin. Oncol. 2010, 28, 375–379. [Google Scholar] [CrossRef]
- Yu, K.D.; Ye, F.G.; He, M.; Fan, L.; Ma, D.; Mo, M.; Wu, J.; Liu, G.Y.; Di, G.H.; Zeng, X.H.; et al. Effect of Adjuvant Paclitaxel and Carboplatin on Survival in Women With Triple-Negative Breast Cancer: A Phase 3 Randomized Clinical Trial. JAMA Oncol. 2020, 6, 1390–1396. [Google Scholar] [CrossRef] [PubMed]
- Tutt, A.; Tovey, H.; Cheang, M.C.U.; Kernaghan, S.; Kilburn, L.; Gazinska, P.; Owen, J.; Abraham, J.; Barrett, S.; Barrett-Lee, P.; et al. Carboplatin in BRCA1/2-mutated and triple-negative breast cancer BRCAness subgroups: The TNT Trial. Nat. Med. 2018, 24, 628–637. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.-J.; Xu, Y.; Lin, Y.; Zhu, H.-J.; Zhou, Y.-D.; Mao, F.; Zhang, X.-H.; Huang, X.; Zhong, Y.; Sun, Q.; et al. Platinum-Based Neoadjuvant Chemotherapy for Breast Cancer With BRCA Mutations: A Meta-Analysis. Front. Oncol. 2020, 10, 592998. [Google Scholar] [CrossRef] [PubMed]
- Caramelo, O.; Silva, C.; Caramelo, F.; Frutuoso, C.; Santos, T.A. The effect of neoadjuvant platinum-based chemotherapy in BRCA mutated triple negative breast cancers -systematic review and meta-analysis. Hered. Cancer Clin. Pr. 2019, 17, 1–10. [Google Scholar] [CrossRef]
- Wang, J.; Zhang, Y.; Yuan, L.; Ren, L.; Zhang, Y.; Qi, X. Comparative efficacy, safety, and acceptability of single-agent poly (ADP-ribose) polymerase (PARP) inhibitors in BRCA-mutated HER2-negative metastatic or advanced breast cancer: A network meta-analysis. Aging (Albany NY) 2020, 13, 450–459. [Google Scholar] [CrossRef]
- Achana, F.A.; Cooper, N.J.; Dias, S.; Lu, G.; Rice, S.J.C.; Kendrick, D.; Sutton, A.J. Extending methods for investigating the relationship between treatment effect and baseline risk from pairwise meta-analysis to network meta-analysis. Stat. Med. 2012, 32, 752–771. [Google Scholar] [CrossRef]
- Waks, A.G.; Cohen, O.; Kochupurakkal, B.; Kim, D.; Dunn, C.E.; Buendia, J.B.; Wander, S.; Helvie, K.; Lloyd, M.R.; Marini, L.; et al. Reversion and non-reversion mechanisms of resistance to PARP inhibitor or platinum chemotherapy in BRCA1/2-mutant metastatic breast cancer. Ann. Oncol. 2020, 31, 590–598. [Google Scholar] [CrossRef]
- Arun, B.K.; Han, H.S.; Kaufman, B.; Wildiers, H.; Friedlander, M.; Ayoub, J.-P.; Puhalla, S.L.; Bell-McGuinn, K.M.; Bach, B.A.; Kundu, M.G.; et al. Efficacy and safety of first-line veliparib and carboplatin–paclitaxel in patients with HER2− advanced germline BRCA+ breast cancer: Subgroup analysis of a randomised clinical trial. Eur. J. Cancer 2021, 154, 35–45. [Google Scholar] [CrossRef]
- Han, H.S.; Diéras, V.; Robson, M.; Palácová, M.; Marcom, P.K.; Jager, A.; Bondarenko, I.; Citrin, D.; Campone, M.; Telli, M.L.; et al. Veliparib with temozolomide or carboplatin/paclitaxel versus placebo with carboplatin/paclitaxel in patients with BRCA1/2 locally recurrent/metastatic breast cancer: Randomized phase II study. Ann. Oncol. 2018, 29, 154–161. [Google Scholar] [CrossRef]
- Han, H.; Arun, B.; Kaufman, B.; Wildiers, H.; Friedlander, M.; Ayoub, J.; Puhalla, S.; Bach, B.; Kundu, M.; Khandelwal, N.; et al. Veliparib monotherapy following carboplatin/paclitaxel plus veliparib combination therapy in patients with germline BRCA-associated advanced breast cancer: Results of exploratory analyses from the phase III BROCADE3 trial. Ann. Oncol. 2022, 33, 299–309. [Google Scholar] [CrossRef]
- González-Martín, A.; Pothuri, B.; Vergote, I.; DePont Christensen, R.; Graybill, W.; Mirza, M.R.; McCormick, C.; Lorusso, D.; Hoskins, P.; Freyer, G.; et al. Niraparib in Patients with Newly Diagnosed Advanced Ovarian Cancer. N. Engl. J. Med. 2019, 381, 2391–2402. [Google Scholar] [CrossRef] [PubMed]
- Golan, T.; Hammel, P.; Reni, M.; van Cutsem, E.; Macarulla, T.; Hall, M.J.; Park, J.-O.; Hochhauser, D.; Arnold, D.; Oh, D.-Y.; et al. Maintenance Olaparib for Germline BRCA-Mutated Metastatic Pancreatic Cancer. N. Engl. J. Med. 2019, 381, 317–327. [Google Scholar] [CrossRef] [PubMed]
- Isakoff, S.J.; Mayer, E.L.; He, L.; Traina, T.A.; Carey, L.A.; Krag, K.J.; Rugo, H.S.; Liu, M.C.; Stearns, V.; Come, S.E.; et al. TBCRC009: A Multicenter Phase II Clinical Trial of Platinum Monotherapy With Biomarker Assessment in Metastatic Triple-Negative Breast Cancer. J. Clin. Oncol. 2015, 33, 1902–1909. [Google Scholar] [CrossRef] [PubMed]
- Fasching, P.; Link, T.; Hauke, J.; Seither, F.; Jackisch, C.; Klare, P.; Schmatloch, S.; Hanusch, C.; Huober, J.; Stefek, A.; et al. Neoadjuvant paclitaxel/olaparib in comparison to paclitaxel/carboplatinum in patients with HER2-negative breast cancer and homologous recombination deficiency (GeparOLA study). Ann. Oncol. 2021, 32, 49–57. [Google Scholar] [CrossRef] [PubMed]
- Pitt, J.M.; Marabelle, A.; Eggermont, A.; Soria, J.C.; Kroemer, G.; Zitvogel, L. Targeting the tumor microenvironment: Removing obstruction to anticancer immune responses and immuno-therapy. Ann. Oncol. 2016, 27, 1482–1492. [Google Scholar] [CrossRef] [PubMed]
- Cimino-Mathews, A.; Thompson, E.; Taube, J.M.; Ye, X.; Lu, Y.; Meeker, A.; Xu, H.; Sharma, R.; Lecksell, K.; Cornish, T.C.; et al. PD-L1 (B7-H1) expression and the immune tumor microenvironment in primary and metastatic breast carcinomas. Hum. Pathol. 2016, 47, 52–63. [Google Scholar] [CrossRef]
- Denkert, C.; von Minckwitz, G.; Darb-Esfahani, S.; Lederer, B.; Heppner, B.I.; Weber, K.E.; Budczies, J.; Huober, J.; Klauschen, F.; Furlanetto, J.; et al. Tumour-infiltrating lymphocytes and prognosis in different subtypes of breast cancer: A pooled analysis of 3771 patients treated with neoadjuvant therapy. Lancet Oncol. 2018, 19, 40–50. [Google Scholar] [CrossRef]
- Emens, L.A.; Cruz, C.; Eder, J.P.; Braiteh, F.; Chung, C.; Tolaney, S.M.; Kuter, I.; Nanda, R.; Cassier, P.A.; Delord, J.P.; et al. Long-term Clinical Outcomes and Biomarker Analyses of Atezolizumab Therapy for Patients With Metastatic Triple-Negative Breast Cancer: A Phase 1 Study. JAMA Oncol. 2019, 5, 74–82. [Google Scholar] [CrossRef]
- Adams, S.; Loi, S.; Toppmeyer, D.; Cescon, D.W.; de Laurentiis, M.; Nanda, R.; Winer, E.P.; Mukai, H.; Tamura, K.; Armstrong, A.; et al. Pembrolizumab monotherapy for previously untreated, PD-L1-positive, metastatic triple-negative breast cancer: Cohort B of the phase II KEYNOTE-086 study. Ann. Oncol. 2019, 30, 405–411. [Google Scholar] [CrossRef]
- Emens, L.A.; Molinero, L.; Loi, S.; Rugo, H.S.; Schneeweiss, A.; Diéras, V.; Iwata, H.; Barrios, C.H.; Nechaeva, M.; Nguyen-Duc, A.; et al. Atezolizumab and nab-Paclitaxel in Advanced Triple-Negative Breast Cancer: Biomarker Evaluation of the IMpassion130 Study. J. Natl. Cancer Inst. 2021, 113, 1005–1016. [Google Scholar] [CrossRef]
- Danza, K.; Pilato, B.; Lacalamita, R.; Addati, T.; Giotta, F.; Bruno, A.; Paradiso, A.; Tommasi, S. Angiogenetic axis angiopoietins/Tie2 and VEGF in familial breast cancer. Eur. J. Hum. Genet. 2013, 21, 824–830. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Study Abbr. | Phase | Region | Stage | Patients | Treatment Regimen | Sample Size | Median Age (Range) |
|---|---|---|---|---|---|---|---|---|
| Byrski, T. 2010 | NA | 2 | Canada | Neoadjuvant | HER2-negative BC | Platinum (Cisplatin) | 12 | 43 (37–50) |
| Chemo (Doxorubicin + Cyclophosphamide) | 90 | 42 (25–50) | ||||||
| Arun, B. K. 2021 | BROCADE3 | 3 | Multicenter | Advanced | HER2-negative BC | PARPi + Platinum + Chemo (Veliparib + Carboplatin + Paclitaxel) | 274 | 47 (24–82) |
| Platinum + Chemo (Placebo + Carboplatin + Paclitaxel) | 139 | 44 (28–75) | ||||||
| Han, H. S. 2018 | BROCADE | 2 | Multicenter | Advanced | HER2-negative BC | PARPi + Platinum + Chemo (Veliparib + Carboplatin + Paclitaxel) | 95 | 44 (25–65) |
| PARPi + Chemo (Veliparib + Temozolomide) | 91 | 46 (22–70) | ||||||
| Platinum + Chemo (Placebo + Carboplatin + Paclitaxel) | 98 | 44 (24–66) | ||||||
| Du, F. 2020 | NA | 2 | China | Adjuvant | TNBC | Platinum + Chemo (Docetaxel or Paclitaxel + Carboplatin) | 6 | NA |
| Chemo (Epirubicin + Cyclophosphamide, followed by Docetaxel or Paclitaxel) | 9 | NA | ||||||
| Fasching, P. A. 2021 | GeparOLA | 2 | German | Neoadjuvant | HER2-negative BC | PARPi + Chemo (Olaparib + Paclitaxel) | 41 | 48 (25–71) |
| Platinum + Chemo (Carboplatinum + Paclitaxel) | 18 | 45 (26–67) | ||||||
| Fasching, P. A. 2018 | GeparQuinto | 3 | German | Neoadjuvant | TNBC | Bev + chemo (Bevacizumab + Epirubicin + Cyclophosphamide, followed by Docetaxel) | 39 | 48 (37–59) |
| Chemo (Epirubicin + Cyclophosphamide, followed by Docetaxel) | 51 | 48 (38–58) | ||||||
| Geyer, C. E. 2022 | BrightTNess | 3 | Multicenter | Neoadjuvant | TNBC | PARPi + Platinum + Chemo (Veliparib + Carboplatin + Paclitaxel) | 46 | 51 (41–59) |
| Platinum + Chemo (Placebo + Carboplatin + Paclitaxel) | 24 | 49 (40–57) | ||||||
| Chemo (Paclitaxel) | 22 | 50 (42–59) | ||||||
| Hahnen, E. 2017 | GeparSixto | 3 | German | Neoadjuvant | TNBC | Bev + chemo + Platinum (Bevacizumab + Paclitaxel + Doxorubicin + Carboplatin) | 26 | 48 (37–59) |
| Bev + chemo (Paclitaxel + Doxorubicin + Carboplatin) | 24 | 48 (37–59) | ||||||
| Robson, M. 2019 | OlympiAD | 3 | Multicenter | Advanced | HER2-negative BC | PARPi (Olaparib) | 205 | 41.5 |
| Chemo (Capecitabine, Vinorelbine, or Eribulin) | 97 | 42 | ||||||
| Kalra, M. 2021 | NA | 3 | USA | Adjuvant | TNBC | PARPi + Platinum (Rucaparib + Cisplatin) | 8 | 47 (21–75) |
| Platinum (Cisplatin) | 14 | 48 (27–69) | ||||||
| Kummar, S. 2016 | NA | 2 | USA | Advanced | TNBC | PARPi + Chemo (Veliparib + Cyclophosphamide) | 2 | 54 (34–77) |
| Chemo (Cyclophosphamide) | 5 | 54 (34–77) | ||||||
| Litton, J. K. 2020 | EMBRACA | 3 | USA | Advanced | HER2-negative ABC | PARPi (Talazoparib) | 219 | 45 (27–84) |
| Chemo (Capecitabine, Eribulin, Gemcitabine, or Vinorelbine) | 114 | 50 (24–88) | ||||||
| Zhang, J. 2018 | CBCSG006 | 3 | China | Advanced | TNBC | Platinum + Chemo (Cisplatin + Gemcitabine) | 6 | NA |
| Chemo (Paclitaxel + Gemcitabine) | 8 | NA | ||||||
| Pohl-Rescigno, E. 2020 | GeparOcto | 3 | Multicenter | Neoadjuvant | HER2-negative BC | Platinum + Chemo (Carboplatin + Paclitaxel + Doxorubicin) | 47 | 48 (21–76) |
| Chemo (Epirubicin + Aclitaxel + Cyclophosphamide) | 49 | 48 (21–76) | ||||||
| Tung, N. 2020 | INFORM | 2 | USA | Neoadjuvant | HER2–negative BC | Platinum (Cisplatin) | 60 | 42 (24–73) |
| Chemo (Doxorubicin-Cyclophosphamide) | 58 | 42 (24–73) | ||||||
| Turner, N. C. 2021 | BRAVO | 3 | Multicenter | Advanced | HER2–negative BC | PARPi (Niraparib) | 141 | NA |
| Chemo (Eribulin, Capecitabine, Vinorelbine, or Gemcitabine) | 74 | NA | ||||||
| Tutt, A. 2018 | TNT | 3 | UK | Advanced | TNBC | Platinum (Carboplatin) | 25 | 56 (48–63) |
| Chemo (Docetaxel) | 18 | 55 (48–63) | ||||||
| Tutt, A. N. J. 2021 | OlympiA | 3 | Multicenter | Adjuvant | HER2–negative BC | PARPi (Olaparib) | 921 | 43 (33–53) |
| Placebo (Placebo) | 915 | 44 (33–53) | ||||||
| Yu, K. D. 2020 | PATTERN | 3 | China | Adjuvant | TNBC | Platinum + Chemo (Carboplatin + Paclitaxel) | 34 | 51 (44–57) |
| Chemo (Cyclophosphamide, Epirubicin, and Fluorouracil, followed by Docetaxcel) | 32 | 51 (44–57) | ||||||
| Zheng, F. 2022 | NA | 2 | China | Adjuvant | TNBC | Platinum + Chemo (Carboplatin + Paclitaxel + Docetaxel) | 12 | 48 (43–54) |
| Chemo (Epirubicin, Cyclophosphamide, followed by Docetaxel or Paclitaxel) | 26 | 47 (42–56) | ||||||
| Emens, L. A. 2021 | IMpassion130 | 3 | Multicenter | Advanced | TNBC | Atezo + Chemo (Atezolizumab + Nab-paclitaxel) | 39 | NA |
| Chemo (Nab-paclitaxel) | 50 | NA | ||||||
| Sella, T. 2018 | NA | 2 | Israel | Neoadjuvant | TNBC | Platinum + Chemo (Anthracycline + Cyclophosphamide, followed by Paclitaxel + Carboplatin) | 14 | 42 |
| Chemo (Anthracycline + Cyclophosphamide) | 34 | 43 |
| OS (Hazard Ratios (HR) with 95% CI) | |||||||
|---|---|---|---|---|---|---|---|
| PARPi + Platinum + Chemo | |||||||
| 0.85 (0.67, 1.09) | Platinum + Chemo | ||||||
| 1.11 (0.32, 3.87) | 1.30 (0.38, 4.44) | PARPi | |||||
| 0.97 (0.28, 3.37) | 1.14 (0.34, 3.85) | 0.88 (0.74, 1.04) | Chemo | ||||
| 1.37 (0.19, 9.62) | 1.6 (0.23, 11.08) | 1.24 (0.27, 5.58) | 1.40 (0.31, 6.27) | Platinum | |||
| 0.75 (0.20, 2.83) | 0.88 (0.24, 3.24) | 0.68 (0.44, 1.05) | 0.77 (0.48, 1.24) | 0.55 (0.12, 2.65) | Placebo | ||
| 1.37 (0.35, 5.45) | 1.61 (0.42, 6.24) | 1.24 (0.67, 2.31) | 1.41 (0.77, 2.56) | 1.00 (0.20, 5.06) | 1.82 (0.85, 3.90) | Atezo + Chemo | |
| 0.58 (0.37, 0.89) | 0.67 (0.47, 0.97) | 0.52 (0.14, 1.87) | 0.59 (0.17, 2.10) | 0.42 (0.06, 3.02) | 0.76 (0.20, 2.95) | 0.42 (0.10, 1.70) | PARPi + Chemo |
| PFS (hazard ratios (HR) with 95% CI) | |||||||
| PARPi + Platinum + Chemo | |||||||
| 0.64 (0.33, 1.19) | Platinum + Chemo | ||||||
| 0.54 (0.07, 3.89) | 0.84 (0.12, 5.54) | PARPi | |||||
| 0.35 (0.05, 2.44) | 0.55 (0.09, 3.44) | 0.65 (0.41, 1.10) | Chemo | ||||
| 0.64 (0.07, 5.98) | 1.00 (0.12, 8.64) | 1.20 (0.36, 4.11) | 1.83 (0.60, 5.59) | Platinum | |||
| 0.51 (0.06, 4.29) | 0.80 (0.10, 6.14) | 0.95 (0.34, 2.77) | 1.46 (0.58, 3.66) | 0.80 (0.19, 3.38) | Atezo + Chemo | ||
| 0.35 (0.11, 0.99) | 0.54 (0.23, 1.29) | 0.64 (0.08, 5.17) | 0.98 (0.13, 7.37) | 0.54 (0.05, 5.39) | 0.67 (0.07, 6.19) | PARPi + Chemo | |
| DFS (hazard ratios (HR) with 95% CI) | |||||||
| Bev + Chemo | |||||||
| 1.38 (0.38, 5.03) | Chemo | ||||||
| 2.42 (0.44, 12.62) | 1.75 (0.58, 5.00) | PARPi + Platinum + Chemo | |||||
| 2.00 (0.42, 8.80) | 1.44 (0.61, 3.16) | 0.82 (0.27, 2.39) | Platinum + Chemo | ||||
| 1.34 (0.09, 19.90) | 0.96 (0.05, 18.96) | 0.55 (0.02, 13.15) | 0.67 (0.03, 14.72) | Bev + Chemo + Platinum | |||
| pCR (odds ratios (OR) with 95% CI) | |||||||
| Bev + Chemo | |||||||
| 1.06 (0.32, 3.56) | Bev + Chemo + Platinum | ||||||
| 2.32 (0.99, 5.59) | 2.19 (0.50, 9.56) | Chemo | |||||
| 2.02 (0.41, 10.28) | 1.90 (0.26, 14.24) | 0.86 (0.23, 3.45) | PARPi + Chemo | ||||
| 1.19 (0.37, 3.90) | 1.12 (0.21, 6.00) | 0.51 (0.23, 1.14) | 0.59 (0.14, 2.43) | PARPi + Platinum + Chemo | |||
| 1.14 (0.37, 3.61) | 1.08 (0.20, 5.61) | 0.49 (0.23, 1.04) | 0.57 (0.12, 2.62) | 0.96 (0.32, 2.88) | Platinum | ||
| 1.53 (0.52, 4.53) | 1.44 (0.29, 7.23) | 0.66 (0.34, 1.25) | 0.76 (0.22, 2.44) | 1.28 (0.58, 2.83) | 1.34 (0.50, 3.56) | Platinum + Chemo | |
| ORR (odds ratios (OR) with 95% CI) | |||||||
| Chemo | |||||||
| 0.30 (0.12, 0.80) | PARPi | ||||||
| 0.10 (0.001, 1.91) | 0.34 (0.004, 7.12) | PARPi + Chemo | |||||
| 0.02 (0.0003, 0.38) | 0.06 (0.0009, 1.40) | 0.18 (0.03, 1.76) | PARPi + Platinum + Chemo | ||||
| 0.22 (0.03, 1.57) | 0.74 (0.08, 6.34) | 2.20 (0.06, 233) | 11.93 (0.32, 1163) | Platinum | |||
| 0.03 (0.0006, 0.49) | 0.10 (0.002, 1.87) | 0.28 (0.07, 1.97) | 1.58 (0.50, 5.41) | 0.13 (0.002, 4.26) | Platinum + Chemo | ||
| PFS of TNBC subgroup (hazard ratios (HR) with 95% CI) | |||||||
| PARPi + Platinum + Chemo | |||||||
| 0.76 (0.41, 1.43) | Platinum + Chemo | ||||||
| 0.81 (0.11, 5.93) | 1.07 (0.16, 7.17) | PARPi | |||||
| 0.41 (0.06, 2.78) | 0.54 (0.09, 3.36) | 0.51 (0.28, 0.93) | Chemo | ||||
| 0.74 (0.08, 6.88) | 0.98 (0.12, 8.35) | 0.92 (0.26, 3.22) | 1.81 (0.61, 5.48) | Platinum | |||
| 0.60 (0.07, 4.89) | 0.79 (0.10, 5.94) | 0.73 (0.25, 2.19) | 1.46 (0.59, 3.59) | 0.80 (0.19, 3.29) | Atezo + Chemo | ||
| 0.31 (0.10, 0.96) | 0.41 (0.16, 1.04) | 0.39 (0.05, 3.15) | 0.76 (0.10, 5.79) | 0.42 (0.04, 4.13) | 0.52 (0.06, 4.73) | PARPi + Chemo | |
| PFS of hormone receptor (HR)-positive subgroup (hazard ratios (HR) with 95% CI) | |||||||
| PARPi + Platinum + Chemo | |||||||
| 0.67 (0.42, 1.07) | Platinum + Chemo | ||||||
| 0.41 (0.18, 0.96) | 0.61 (0.30, 1.24) | PARPi + Chemo | |||||
| ORR of TNBC subgroup (odds ratios (OR) with 95% CI) | |||||||
| Chemo | |||||||
| 0.11 (0.01, 0.87) | PARPi | ||||||
| 0.000 (0.000, 0.18) | 0.000 (0.000, 1.95) | PARPi + Chemo | |||||
| 0.22 (0.01, 3.87) | 2.06 (0.06, 65.41) | 3.86 (0.89, 75.18) | Platinum | ||||
| 0.08 (0.001, 2.74) | 0.71 (0.01, 40.78) | 2.83 (0.18, 58.20) | 0.34 (0.002, 33.32) | Platinum + Chemo | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sun, W.; Wu, Y.; Ma, F.; Fan, J.; Qiao, Y. Efficacy of PARP Inhibitor, Platinum, and Immunotherapy in BRCA-Mutated HER2-Negative Breast Cancer Patients: A Systematic Review and Network Meta-Analysis. J. Clin. Med. 2023, 12, 1588. https://doi.org/10.3390/jcm12041588
Sun W, Wu Y, Ma F, Fan J, Qiao Y. Efficacy of PARP Inhibitor, Platinum, and Immunotherapy in BRCA-Mutated HER2-Negative Breast Cancer Patients: A Systematic Review and Network Meta-Analysis. Journal of Clinical Medicine. 2023; 12(4):1588. https://doi.org/10.3390/jcm12041588
Chicago/Turabian StyleSun, Wanyi, Yun Wu, Fei Ma, Jinhu Fan, and Youlin Qiao. 2023. "Efficacy of PARP Inhibitor, Platinum, and Immunotherapy in BRCA-Mutated HER2-Negative Breast Cancer Patients: A Systematic Review and Network Meta-Analysis" Journal of Clinical Medicine 12, no. 4: 1588. https://doi.org/10.3390/jcm12041588
APA StyleSun, W., Wu, Y., Ma, F., Fan, J., & Qiao, Y. (2023). Efficacy of PARP Inhibitor, Platinum, and Immunotherapy in BRCA-Mutated HER2-Negative Breast Cancer Patients: A Systematic Review and Network Meta-Analysis. Journal of Clinical Medicine, 12(4), 1588. https://doi.org/10.3390/jcm12041588