
Identification of Key Factors Influencing the Choice of the Type of Vaginal Pessary for Women Presenting with Pelvic Organ Prolapse: Semi-Directive Interviews and Development of an Algorithm
 , , , and
, , , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Criteria for Inclusion of Interviewed Health Professionals (Expert Group)
2.2. Semi-Directive Interviews
2.3. Algorithm Development
2.4. External Assessment of the Algorithm
2.5. Approval by the Ethics Committee
3. Results
3.1. Semi-Directive Interviews
3.2. Parameters in the Choice of Pessary
3.3. Method of Evaluation of the Size/Dimensions of the Pessary to Prescribe
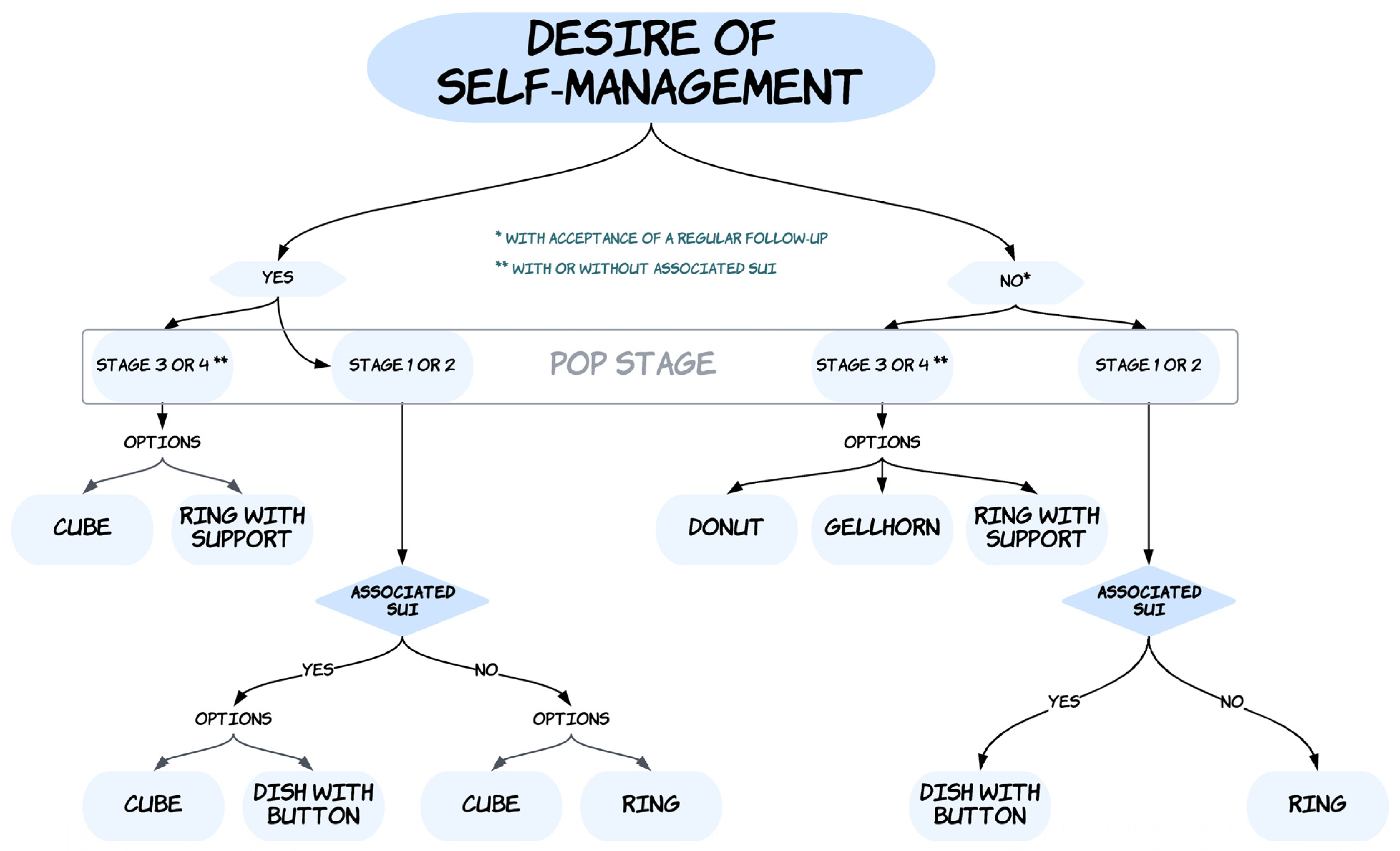
3.4. Development of an Algorithm for the Choice of Pessary
3.5. External Assessment by a Group of Non-Experts of the Usefulness of the Algorithm
4. Discussion
4.1. What Are the Actual Clinical Implications of This Study?
4.2. What Does This Study Add to the Existing Literature on the Topic?
4.3. What Are the Limitations of the Current Study and What Are the Future Study Perspectives?
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Tsiapakidou, S.; Nygaard, C.C.; Falconi, G.; Pape, J.; Betschart, C.; Doumouchtsis, S.K.; CHORUS: An International Collaboration for Harmonising Outcomes, Research and Standards in Urogynaecology and Women’s Health (i-chorus.org). Systematic review and appraisal of clinical practice guidelines on pelvic organ prolapse using the AGREE II tool. Neurourol. Urodyn. 2021, 40, 1402–1413. [Google Scholar] [CrossRef] [PubMed]
- Pizzoferrato, A.C.; Thuillier, C.; Vénara, A.; Bornsztein, N.; Bouquet, S.; Cayrac, M.; Cornillet-Bernard, M.; Cotelle, O.; Cour, F.; Cretinon, S.; et al. Management of female pelvic organ prolapse—Summary of the 2021 HAS guidelines. J. Gynecol. Obstet. Hum. Reprod. 2023, 16, 102535. [Google Scholar] [CrossRef]
- Sansone, S.; Sze, C.; Eidelberg, A.; Stoddard, M.; Cho, A.; Asdjodi, S.; Mao, J.; Elterman, D.S.; Zorn, K.C.; Chughtai, B. Role of Pessaries in the Treatment of Pelvic Organ Prolapse: A Systematic Review and Meta-analysis. Obstet. Gynecol. 2022, 140, 613–622. [Google Scholar] [CrossRef]
- Bugge, C.; Adams, E.J.; Gopinath, D.; Stewart, F.; Dembinsky, M.; Sobiesuo, P.; Kearney, R. Pessaries (mechanical devices) for managing pelvic organ prolapse in women. Cochrane Database Syst. Rev. 2020, 11, CD004010. [Google Scholar] [PubMed]
- Schiavi, M.C.; D’Oria, O.; Faiano, P.; Prata, G.; Di Pinto, A.; Sciuga, V.; Colagiovanni, V.; Giannini, A.; Zullo, M.A.; Monti, M.; et al. Vaginal Native Tissue Repair for Posterior Compartment Prolapse: Long-Term Analysis of Sexual Function and Quality of Life in 151 Patients. Female Pelvic Med. Reconstr. Surg. 2018, 24, 419–423. [Google Scholar] [CrossRef] [PubMed]
- de Tayrac, R.; Antosh, D.D.; Baessler, K.; Cheon, C.; Deffieux, X.; Gutman, R.; Lee, J.; Nager, C.; Schizas, A.; Sung, V.; et al. Summary: 2021 International Consultation on Incontinence Evidence-Based Surgical Pathway for Pelvic Organ Prolapse. J. Clin. Med. 2022, 11, 6106. [Google Scholar] [CrossRef] [PubMed]
- Patel, M.; Mellen, C.; O’Sullivan, D.M.; LaSala, C.A. Impact of pessary use on prolapse symptoms, quality of life, and body image. Am. J. Obstet. Gynecol. 2010, 202, 499.e1–499.e4. [Google Scholar] [CrossRef] [PubMed]
- Boyd, S.S.; Subramanian, D.; Propst, K.; O’Sullivan, D.; Tulikangas, P. Pelvic Organ Prolapse Severity and Genital Hiatus Size With Long-Term Pessary Use. Female Pelvic Med. Reconstr. Surg. 2021, 27, e360–e362. [Google Scholar] [CrossRef] [PubMed]
- Handa, V.L.; Garrett, E.; Hendrix, S.; Gold, E.; Robbins, J. Progression and remission of pelvic organ prolapse: A longitudinal study of menopausal women. Am. J. Obstet. Gynecol. 2004, 190, 27–32. [Google Scholar] [CrossRef] [PubMed]
- Mao, M.; Ai, F.; Kang, J.; Zhang, Y.; Liang, S.; Zhou, Y.; Zhu, L. Successful long-term use of Gellhorn pessary and the effect on symptoms and quality of life in women with symptomatic pelvic organ prolapse. Menopause 2019, 26, 145–151. [Google Scholar] [CrossRef]
- Bugge, C.; Dembinsky, M.; Kearney, R.; Hagen, S. Does self-management of vaginal pessaries improve care for women with pelvic organ prolapse? BMJ 2021, 372, n310. [Google Scholar] [CrossRef] [PubMed]
- Tong, A.; Sainsbury, P.; Craig, J. Consolidated criteria for reporting qualitative research (COREQ): A 32-item checklist for interviews and focus groups. Int. J. Qual. Health Care 2007, 19, 349–357. [Google Scholar] [CrossRef] [PubMed]
- Jorm, A.F. Using the Delphi expert consensus method in mental health research. Aust. N. Z. J. Psychiatry 2015, 49, 887–897. [Google Scholar] [CrossRef] [PubMed]
- Vardon, D.; Martin-Lasnel, M.; Agostini, A.; Fauvet, R.; Pizzoferrato, A.C. Vaginal pessary for pelvic organ prolapse: A survey among French gynecological surgeons. J. Gynecol. Obstet. Hum. Reprod. 2021, 50, 101833. [Google Scholar] [CrossRef] [PubMed]
- Pizzoferrato, A.C.; Nyangoh-Timoh, K.; Martin-Lasnel, M.; Fauvet, R.; de Tayrac, R.; Villot, A. Vaginal Pessary for Pelvic Organ Prolapse: A French Multidisciplinary Survey. J. Women’s Health 2022, 31, 870–877. [Google Scholar] [CrossRef] [PubMed]
- Barsky, M.; Kelley, R.; Bhora, F.Y.; Hardart, A. Customized Pessary Fabrication Using Three-Dimensional Printing Technology. Obstet. Gynecol. 2018, 131, 493–497. [Google Scholar] [CrossRef] [PubMed]
- Manzini, C.; Withagen, M.I.J.; van den Noort, F.; Grob, A.T.M.; van der Vaart, C.H. Transperineal ultrasound to estimate the appropriate ring pessary size for women with pelvic organ prolapse. Int. Urogynecol. J. 2022, 33, 1981–1987. [Google Scholar] [CrossRef] [PubMed]
- de Albuquerque Coelho, S.C.; Pereira, G.M.V.; Brito, L.G.O.; Juliato, C.R.T. Cross sectional study on assessment of ring pessary cleaning and removal every six months: Adverse events and complications. Int. Urogynecol. J. 2022, 33, 397–403. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Total | n = 17 |
| Age in y. mean (s.d.) | 45.8 (12.5) |
| Sex: female n.(%) | 12 (70.6) |
| Years of professional practice mean (s.d.) | 16.9 (8.3) |
| Type of practice n.(%) | |
| Private | 5 (29.4) |
| Salaried | 8 (47.1) |
| Mixed | 4 (23.5) |
| POP surgical practice: “yes” n.(%) | 11 (64.8) |
| Training in the prescription of pessaries n.(%) | |
| Peer training | 8 (47.1) |
| Self-study (books, journals, and internet) | 15 (58.8) |
| Training organized by industry | 4 (23.5) |
| Mean number of new pessaries prescribed/week 1 n.(s.d.) | 4.7 (1.4) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Le Quoy, M.-A.; Cotelle, O.; de Tayrac, R.; Happillon, F.; Pelhuche, A.; Wenner-Vidal, V.; Liagre, B.; Cour, F.; Armengaud, C.; Chene, G.; et al. Identification of Key Factors Influencing the Choice of the Type of Vaginal Pessary for Women Presenting with Pelvic Organ Prolapse: Semi-Directive Interviews and Development of an Algorithm. J. Clin. Med. 2023, 12, 1548. https://doi.org/10.3390/jcm12041548
Le Quoy M-A, Cotelle O, de Tayrac R, Happillon F, Pelhuche A, Wenner-Vidal V, Liagre B, Cour F, Armengaud C, Chene G, et al. Identification of Key Factors Influencing the Choice of the Type of Vaginal Pessary for Women Presenting with Pelvic Organ Prolapse: Semi-Directive Interviews and Development of an Algorithm. Journal of Clinical Medicine. 2023; 12(4):1548. https://doi.org/10.3390/jcm12041548
Chicago/Turabian StyleLe Quoy, Marie-Amélie, Odile Cotelle, Renaud de Tayrac, Florence Happillon, Antoine Pelhuche, Valérie Wenner-Vidal, Blandine Liagre, Florence Cour, Camille Armengaud, Gautier Chene, and et al. 2023. "Identification of Key Factors Influencing the Choice of the Type of Vaginal Pessary for Women Presenting with Pelvic Organ Prolapse: Semi-Directive Interviews and Development of an Algorithm" Journal of Clinical Medicine 12, no. 4: 1548. https://doi.org/10.3390/jcm12041548
APA StyleLe Quoy, M.-A., Cotelle, O., de Tayrac, R., Happillon, F., Pelhuche, A., Wenner-Vidal, V., Liagre, B., Cour, F., Armengaud, C., Chene, G., Cerutti, E., Doucet, F., Pizzoferrato, A.-C., & Deffieux, X. (2023). Identification of Key Factors Influencing the Choice of the Type of Vaginal Pessary for Women Presenting with Pelvic Organ Prolapse: Semi-Directive Interviews and Development of an Algorithm. Journal of Clinical Medicine, 12(4), 1548. https://doi.org/10.3390/jcm12041548