
Immunotherapy for Prostate Cancer: A Current Systematic Review and Patient Centric Perspectives

 ,
,  , and
, and
Abstract
1. Introduction
1.1. Brief Overview
1.2. Rationale
1.3. Aims and Objectives
2. Methods
2.1. Literature Search
- Participants: Adult patients with prostate cancer;
- Intervention: Any form of immunotherapy;
- Comparator: Standard care (chemotherapy, radiotherapy, surgery) or placebo;
- Outcome: Any form of survival, progression, responder rate, adverse events, or other treatment outcomes.
2.2. Eligibility Criteria
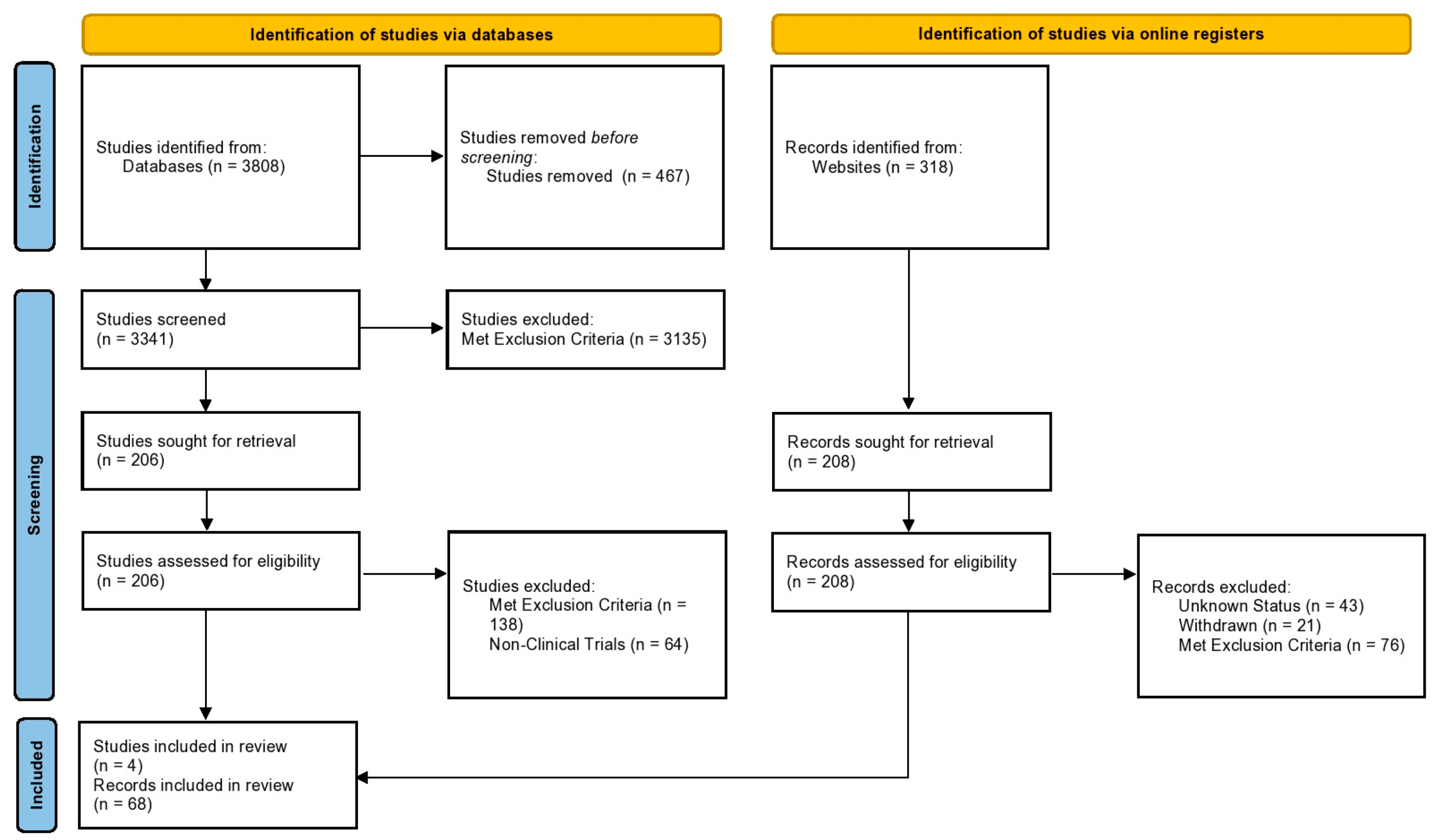
2.3. Study Selection
2.4. Data Extraction
2.5. Risk of Bias Assessment
2.6. Protocol Registration and Role of Funding
3. Results
3.1. Phase III Clinical Trials
3.2. Ongoing Clinical Trials
3.3. Risk-of-Bias Synthesis
4. Discussion
4.1. Limitations
4.2. Future Directions
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wang, I.; Song, L.; Wang, B.Y.; Kalebasty, A.R.; Uchio, E.; Zi, X. Prostate Cancer Immunotherapy: A Review of Recent Advancements with Novel Treatment Methods and Efficacy. Am. J. Clin. Exp. Urol. 2022, 10, 210. [Google Scholar] [PubMed]
- Sfanos, K.S.; Bruno, T.C.; Maris, C.H.; Xu, L.; Thoburn, C.J.; DeMarzo, A.M.; Meeker, A.K.; Isaacs, W.B.; Drake, C.G. Phenotypic Analysis of Prostate-Infiltrating Lymphocytes Reveals TH17 and Treg Skewing. Clin. Cancer Res. 2008, 14, 3254–3261. [Google Scholar] [CrossRef] [PubMed]
- Bubendorf, L.; Schöpfer, A.; Wagner, U.; Sauter, G.; Moch, H.; Willi, N.; Gasser, T.C.; Mihatsch, M.J. Metastatic Patterns of Prostate Cancer: An Autopsy Study of 1589 Patients. Hum. Pathol. 2000, 31, 578–583. [Google Scholar] [CrossRef] [PubMed]
- Prokhnevska, N.; Emerson, D.A.; Kissick, H.T.; Redmond, W.L. Immunological Complexity of the Prostate Cancer Microenvironment Influences the Response to Immunotherapy. In Prostate Cancer; Springer: Cham, Switzerland, 2019; pp. 121–147. [Google Scholar]
- Drake, C.G.; Doody, A.D.H.; Mihalyo, M.A.; Huang, C.-T.; Kelleher, E.; Ravi, S.; Hipkiss, E.L.; Flies, D.B.; Kennedy, E.P.; Long, M. Androgen Ablation Mitigates Tolerance to a Prostate/Prostate Cancer-Restricted Antigen. Cancer Cell 2005, 7, 239–249. [Google Scholar] [CrossRef]
- Mercader, M.; Bodner, B.K.; Moser, M.T.; Kwon, P.S.; Park, E.S.Y.; Manecke, R.G.; Ellis, T.M.; Wojcik, E.M.; Yang, D.; Flanigan, R.C. T Cell Infiltration of the Prostate Induced by Androgen Withdrawal in Patients with Prostate Cancer. Proc. Natl. Acad. Sci. USA 2001, 98, 14565–14570. [Google Scholar] [CrossRef]
- Horn, L.; Spigel, D.R.; Vokes, E.E.; Holgado, E.; Ready, N.; Steins, M.; Poddubskaya, E.; Borghaei, H.; Felip, E.; Paz-Ares, L. Nivolumab versus Docetaxel in Previously Treated Patients with Advanced Non–Small-Cell Lung Cancer: Two-Year Outcomes from Two Randomized, Open-Label, Phase III Trials (CheckMate 017 and CheckMate 057). J. Clin. Oncol. 2017, 35, 3924. [Google Scholar] [CrossRef]
- Kwon, E.D.; Drake, C.G.; Scher, H.I.; Fizazi, K.; Bossi, A.; Van den Eertwegh, A.J.M.; Krainer, M.; Houede, N.; Santos, R.; Mahammedi, H. Ipilimumab versus Placebo after Radiotherapy in Patients with Metastatic Castration-Resistant Prostate Cancer That Had Progressed after Docetaxel Chemotherapy (CA184-043): A Multicentre, Randomised, Double-Blind, Phase 3 Trial. Lancet Oncol. 2014, 15, 700–712. [Google Scholar] [CrossRef]
- Kantoff, P.W.; Higano, C.S.; Shore, N.D.; Berger, E.R.; Small, E.J.; Penson, D.F.; Redfern, C.H.; Ferrari, A.C.; Dreicer, R.; Sims, R.B. Sipuleucel-T Immunotherapy for Castration-Resistant Prostate Cancer. N. Engl. J. Med. 2010, 363, 411–422. [Google Scholar] [CrossRef]
- Kawalec, P.; Paszulewicz, A.; Holko, P.; Pilc, A. Sipuleucel-T Immunotherapy for Castration-Resistant Prostate Cancer. A Systematic Review and Meta-Analysis. Arch. Med. Sci. 2012, 8, 767–775. [Google Scholar] [CrossRef]
- Huber, M.L.; Haynes, L.; Parker, C.; Iversen, P. Interdisciplinary Critique of Sipuleucel-T as Immunotherapy in Castration-Resistant Prostate Cancer. J. Natl. Cancer Inst. 2012, 104, 273–279. [Google Scholar] [CrossRef]
- Powles, T.; Csőszi, T.; Özgüroğlu, M.; Matsubara, N.; Géczi, L.; Cheng, S.Y.S.; Fradet, Y.; Oudard, S.; Vulsteke, C.; Barrera, R.M. Pembrolizumab Alone or Combined with Chemotherapy versus Chemotherapy as First-Line Therapy for Advanced Urothelial Carcinoma (KEYNOTE-361): A Randomised, Open-Label, Phase 3 Trial. Lancet Oncol. 2021, 22, 931–945. [Google Scholar] [CrossRef]
- Motzer, R.J.; Escudier, B.; McDermott, D.F.; George, S.; Hammers, H.J.; Srinivas, S.; Tykodi, S.S.; Sosman, J.A.; Procopio, G.; Plimack, E.R. Nivolumab versus Everolimus in Advanced Renal-Cell Carcinoma. N. Engl. J. Med. 2015, 373, 1803–1813. [Google Scholar] [CrossRef]
- Luke, J.J.; Rutkowski, P.; Queirolo, P.; Del Vecchio, M.; Mackiewicz, J.; Chiarion-Sileni, V.; de la Cruz Merino, L.; Khattak, M.A.; Schadendorf, D.; Long, G. V Pembrolizumab versus Placebo as Adjuvant Therapy in Completely Resected Stage IIB or IIC Melanoma (KEYNOTE-716): A Randomised, Double-Blind, Phase 3 Trial. Lancet 2022, 399, 1718–1729. [Google Scholar] [CrossRef]
- Motzer, R.J.; Tannir, N.M.; McDermott, D.F.; Frontera, O.A.; Melichar, B.; Choueiri, T.K.; Plimack, E.R.; Barthélémy, P.; Porta, C.; George, S. Nivolumab plus Ipilimumab versus Sunitinib in Advanced Renal-Cell Carcinoma. N. Engl. J. Med. 2018, 378, 1277–1290. [Google Scholar] [CrossRef]
- Larkin, J.; Chiarion-Sileni, V.; Gonzalez, R.; Grob, J.J.; Cowey, C.L.; Lao, C.D.; Schadendorf, D.; Dummer, R.; Smylie, M.; Rutkowski, P. Combined Nivolumab and Ipilimumab or Monotherapy in Untreated Melanoma. N. Engl. J. Med. 2015, 373, 23–34. [Google Scholar] [CrossRef]
- Petrylak, D.P.; De Wit, R.; Chi, K.N.; Drakaki, A.; Sternberg, C.N.; Nishiyama, H.; Castellano, D.; Hussain, S.; Fléchon, A.; Bamias, A. Ramucirumab plus Docetaxel versus Placebo plus Docetaxel in Patients with Locally Advanced or Metastatic Urothelial Carcinoma after Platinum-Based Therapy (RANGE): A Randomised, Double-Blind, Phase 3 Trial. Lancet 2017, 390, 2266–2277. [Google Scholar] [CrossRef]
- Lee, N.Y.; Ferris, R.L.; Psyrri, A.; Haddad, R.I.; Tahara, M.; Bourhis, J.; Harrington, K.; Chang, P.M.-H.; Lin, J.-C.; Razaq, M.A. Avelumab plus Standard-of-Care Chemoradiotherapy versus Chemoradiotherapy Alone in Patients with Locally Advanced Squamous Cell Carcinoma of the Head and Neck: A Randomised, Double-Blind, Placebo-Controlled, Multicentre, Phase 3 Trial. Lancet Oncol. 2021, 22, 450–462. [Google Scholar] [CrossRef]
- Bilusic, M.; Madan, R.A.; Gulley, J.L. Immunotherapy of Prostate Cancer: Facts and HopesProstate Cancer Immunotherapy. Clin. Cancer Res. 2017, 23, 6764–6770. [Google Scholar] [CrossRef]
- Ruiz de Porras, V.; Pardo, J.C.; Notario, L.; Etxaniz, O.; Font, A. Immune Checkpoint Inhibitors: A Promising Treatment Option for Metastatic Castration-Resistant Prostate Cancer? Int. J. Mol. Sci. 2021, 22, 4712. [Google Scholar] [CrossRef]
- Sedhom, R.; Antonarakis, E.S. Clinical Implications of Mismatch Repair Deficiency in Prostate Cancer. Futur. Oncol. 2019, 15, 2395–2411. [Google Scholar] [CrossRef]
- Palicelli, A.; Croci, S.; Bisagni, A.; Zanetti, E.; De Biase, D.; Melli, B.; Sanguedolce, F.; Ragazzi, M.; Zanelli, M.; Chaux, A. What Do We Have to Know about PD-L1 Expression in Prostate Cancer? A Systematic Literature Review (Part 6): Correlation of PD-L1 Expression with the Status of Mismatch Repair System, BRCA, PTEN, and Other Genes. Biomedicines 2022, 10, 236. [Google Scholar] [CrossRef] [PubMed]
- Markowski, M.C.; Shenderov, E.; Eisenberger, M.A.; Kachhap, S.; Pardoll, D.M.; Denmeade, S.R.; Antonarakis, E.S. Extreme Responses to Immune Checkpoint Blockade Following Bipolar Androgen Therapy and Enzalutamide in Patients with Metastatic Castration Resistant Prostate Cancer. Prostate 2020, 80, 407–411. [Google Scholar] [CrossRef] [PubMed]
- Iannantuono, G.M.; Torino, F.; Rosenfeld, R.; Guerriero, S.; Carlucci, M.; Sganga, S.; Capotondi, B.; Riondino, S.; Roselli, M. The Role of Histology-Agnostic Drugs in the Treatment of Metastatic Castration-Resistant Prostate Cancer. Int. J. Mol. Sci. 2022, 23, 8535. [Google Scholar] [CrossRef] [PubMed]
- Vogelzang, N.J.; Beer, T.M.; Gerritsen, W.; Oudard, S.; Wiechno, P.; Kukielka-Budny, B.; Samal, V.; Hajek, J.; Feyerabend, S.; Khoo, V. Efficacy and Safety of Autologous Dendritic Cell–Based Immunotherapy, Docetaxel, and Prednisone vs Placebo in Patients with Metastatic Castration-Resistant Prostate Cancer: The VIABLE Phase 3 Randomized Clinical Trial. JAMA Oncol. 2022, 8, 546–552. [Google Scholar] [CrossRef]
- Fizazi, K.; Drake, C.G.; Beer, T.M.; Kwon, E.D.; Scher, H.I.; Gerritsen, W.R.; Bossi, A.; Van den Eertwegh, A.J.M.; Krainer, M.; Houede, N. Final Analysis of the Ipilimumab versus Placebo Following Radiotherapy Phase III Trial in Postdocetaxel Metastatic Castration-Resistant Prostate Cancer Identifies an Excess of Long-Term Survivors. Eur. Urol. 2020, 78, 822–830. [Google Scholar] [CrossRef]
- Noguchi, M.; Fujimoto, K.; Arai, G.; Uemura, H.; Hashine, K.; Matsumoto, H.; Fukasawa, S.; Kohjimoto, Y.; Nakatsu, H.; Takenaka, A. A Randomized Phase III Trial of Personalized Peptide Vaccination for Castration-resistant Prostate Cancer Progressing after Docetaxel. Oncol. Rep. 2021, 45, 159–168. [Google Scholar] [CrossRef]
- Gulley, J.L.; Borre, M.; Vogelzang, N.J.; Ng, S.; Agarwal, N.; Parker, C.C.; Pook, D.W.; Rathenborg, P.; Flaig, T.W.; Carles, J. Phase III Trial of PROSTVAC in Asymptomatic or Minimally Symptomatic Metastatic Castration-Resistant Prostate Cancer. J. Clin. Oncol. 2019, 37, 1051. [Google Scholar] [CrossRef]
- Vitkin, N.; Nersesian, S.; Siemens, D.R.; Koti, M. The Tumor Immune Contexture of Prostate Cancer. Front. Immunol. 2019, 10, 603. [Google Scholar] [CrossRef]
- Rebuzzi, S.E.; Rescigno, P.; Catalano, F.; Mollica, V.; Vogl, U.M.; Marandino, L.; Massari, F.; Pereira Mestre, R.; Zanardi, E.; Signori, A. Immune Checkpoint Inhibitors in Advanced Prostate Cancer: Current Data and Future Perspectives. Cancers 2022, 14, 1245. [Google Scholar] [CrossRef]
- Patel, V.G.; Oh, W.K.; Galsky, M.D. Treatment of Muscle-invasive and Advanced Bladder Cancer in 2020. CA Cancer J. Clin. 2020, 70, 404–423. [Google Scholar] [CrossRef]
- Vaddepally, R.K.; Kharel, P.; Pandey, R.; Garje, R.; Chandra, A.B. Review of Indications of FDA-Approved Immune Checkpoint Inhibitors per NCCN Guidelines with the Level of Evidence. Cancers 2020, 12, 738. [Google Scholar] [CrossRef]
- Kooshkaki, O.; Derakhshani, A.; Hosseinkhani, N.; Torabi, M.; Safaei, S.; Brunetti, O.; Racanelli, V.; Silvestris, N.; Baradaran, B. Combination of Ipilimumab and Nivolumab in Cancers: From Clinical Practice to Ongoing Clinical Trials. Int. J. Mol. Sci. 2020, 21, 4427. [Google Scholar] [CrossRef]
- Lasek, W.; Zapała, Ł. Therapeutic Metastatic Prostate Cancer Vaccines: Lessons Learnt from Urologic Oncology. Cent. Eur. J. Urol. 2021, 74, 300. [Google Scholar]
- Hammerstrom, A.E.; Cauley, D.H.; Atkinson, B.J.; Sharma, P. Cancer Immunotherapy: Sipuleucel-T and Beyond. Pharmacother. J. Hum. Pharmacol. Drug Ther. 2011, 31, 813–828. [Google Scholar] [CrossRef]
- Joniau, S.; Abrahamsson, P.-A.; Bellmunt, J.; Figdor, C.; Hamdy, F.; Verhagen, P.; Vogelzang, N.J.; Wirth, M.; Van Poppel, H.; Osanto, S. Current Vaccination Strategies for Prostate Cancer. Eur. Urol. 2012, 61, 290–306. [Google Scholar] [CrossRef]
- Dang, Q.; Sun, Z.; Wang, Y.; Wang, L.; Liu, Z.; Han, X. Ferroptosis: A Double-Edged Sword Mediating Immune Tolerance of Cancer. Cell Death Dis. 2022, 13, 1–16. [Google Scholar] [CrossRef]
- Gu, Y.; Duan, J.; Yang, N.; Yang, Y.; Zhao, X. MRNA Vaccines in the Prevention and Treatment of Diseases. MedComm 2022, 3, e167. [Google Scholar] [CrossRef]
- Verheye, E.; Bravo Melgar, J.; Deschoemaeker, S.; Raes, G.; Maes, A.; De Bruyne, E.; Menu, E.; Vanderkerken, K.; Laoui, D.; De Veirman, K. Dendritic Cell-Based Immunotherapy in Multiple Myeloma: Challenges, Opportunities, and Future Directions. Int. J. Mol. Sci. 2022, 23, 904. [Google Scholar] [CrossRef]
- Devico Marciano, N.; Kroening, G.; Dayyani, F.; Zell, J.A.; Lee, F.-C.; Cho, M.; Valerin, J.G. BRCA-Mutated Pancreatic Cancer: From Discovery to Novel Treatment Paradigms. Cancers 2022, 14, 2453. [Google Scholar] [CrossRef]
- Sutherland, S.I.M.; Ju, X.; Horvath, L.G.; Clark, G.J. Moving on from Sipuleucel-T: New Dendritic Cell Vaccine Strategies for Prostate Cancer. Front. Immunol. 2021, 12, 641307. [Google Scholar] [CrossRef]
- Handy, C.E.; Antonarakis, E.S. Sipuleucel-T for the Treatment of Prostate Cancer: Novel Insights and Future Directions. Futur. Oncol. 2018, 14, 907–917. [Google Scholar] [CrossRef] [PubMed]
- Caram, M.E.V.; Ross, R.; Lin, P.; Mukherjee, B. Factors Associated with Use of Sipuleucel-T to Treat Patients with Advanced Prostate Cancer. JAMA Netw. Open 2019, 2, e192589. [Google Scholar] [CrossRef] [PubMed]
- Madan, R.A.; Antonarakis, E.S.; Drake, C.G.; Fong, L.; Yu, E.Y.; McNeel, D.G.; Lin, D.W.; Chang, N.N.; Sheikh, N.A.; Gulley, J.L. Putting the Pieces Together: Completing the Mechanism of Action Jigsaw for Sipuleucel-T. JNCI J. Natl. Cancer Inst. 2020, 112, 562–573. [Google Scholar] [CrossRef] [PubMed]
- Sater, H.A.; Marté, J.L.; Donahue, R.N.; Walter-Rodriguez, B.; Heery, C.R.; Steinberg, S.M.; Cordes, L.M.; Chun, G.; Karzai, F.; Bilusic, M. Neoadjuvant PROSTVAC Prior to Radical Prostatectomy Enhances T-Cell Infiltration into the Tumor Immune Microenvironment in Men with Prostate Cancer. J. Immunother. Cancer 2020, 8, e000655. [Google Scholar] [CrossRef] [PubMed]
- Parsons, J.K.; Pinto, P.A.; Pavlovich, C.P.; Uchio, E.; Kim, H.L.; Nguyen, M.N.; Gulley, J.L.; Jamieson, C.; Hsu, P.; Wojtowicz, M. A Randomized, Double-Blind, Phase II Trial of PSA-TRICOM (PROSTVAC) in Patients with Localized Prostate Cancer: The Immunotherapy to Prevent Progression on Active Surveillance Study. Eur. Urol. Focus 2018, 4, 636. [Google Scholar] [CrossRef]
- Bansal, D.; Beck, R.; Arora, V.; Knoche, E.M.; Picus, J.; Reimers, M.A.; Roth, B.J.; Gulley, J.L.; Schreiber, R.; Pachynski, R.K. A Pilot Trial of Neoantigen DNA Vaccine in Combination with Nivolumab/Ipilimumab and Prostvac in Metastatic Hormone-Sensitive Prostate Cancer (MHSPC). 2021. Available online: https://ascopubs.org/doi/abs/10.1200/JCO.2022.40.16_suppl.5068 (accessed on 3 December 2022).
- Reimers, M.A.; Slane, K.E.; Pachynski, R.K. Immunotherapy in Metastatic Castration-Resistant Prostate Cancer: Past and Future Strategies for Optimization. Curr. Urol. Rep. 2019, 20, 1–10. [Google Scholar] [CrossRef]
- Philippou, Y.; Sjoberg, H.; Lamb, A.D.; Camilleri, P.; Bryant, R.J. Harnessing the Potential of Multimodal Radiotherapy in Prostate Cancer. Nat. Rev. Urol. 2020, 17, 321–338. [Google Scholar] [CrossRef]
- Gandaglia, G.; Leni, R.; Rosiello, G.; Fossati, N.; Briganti, A. Clinical Case Debate: Immunotherapy Versus Alternative Therapies in the Neoadjuvant and Adjuvant Setting of Localized, High-Risk Prostate Cancer. In Neoadjuvant Immunotherapy Treatment of Localized Genitourinary Cancers; Springer: Berlin/Heidelberg, Germany, 2022; pp. 145–160. [Google Scholar]
- Jafari, S.; Molavi, O.; Kahroba, H.; Hejazi, M.S.; Maleki-Dizaji, N.; Barghi, S.; Kiaie, S.H.; Jadidi-Niaragh, F. Clinical Application of Immune Checkpoints in Targeted Immunotherapy of Prostate Cancer. Cell Mol. Life Sci. 2020, 77, 3693–3710. [Google Scholar] [CrossRef]
- Sentana-Lledo, D.; Sartor, O.; Balk, S.P.; Einstein, D.J. Immune Mechanisms behind Prostate Cancer in Men of African Ancestry: A Review. Prostate 2022, 82, 883–893. [Google Scholar] [CrossRef]
- Bailey, S.; Lassoued, W.; Papanicolau-Sengos, A.; Marte, J.; Williams, N.; Hankin, A.; Manu, M.; Dahut, W.; Pinto, P.; Karzai, F. 420 PROSTVAC in Combination with Nivolumab Enhanced Immune Cell Infiltration in Prostate Cancer. BMJ 2021, 9, 2. [Google Scholar] [CrossRef]
- Bilusic, M.; Gulley, J.L. Neoadjuvant Immunotherapy: An Evolving Paradigm Shift? JNCI J. Natl. Cancer Inst. 2021, 113, 799–800. [Google Scholar] [CrossRef]
- Silvestri, I.; Tortorella, E.; Giantulli, S.; Scarpa, S.; Sciarra, A. Immunotherapy in Prostate Cancer: Recent Advances and Future Directions. Urology 2019, 7, 51–61. [Google Scholar]
- Tse, B.W.; Jovanovic, L.; Nelson, C.C.; de Souza, P.; Power, C.A.; Russell, P.J. From Bench to Bedside: Immunotherapy for Prostate Cancer. Biomed. Res. Int. 2014, 2014, 981434. [Google Scholar] [CrossRef]
- Ishii, N.; Hatakeyama, S.; Yoneyama, T.; Tanaka, R.; Narita, T.; Fujita, N.; Okamoto, T.; Yamamoto, H.; Yoneyama, T.; Hashimoto, Y. Humoral Response after SARS-CoV-2 MRNA Vaccination in Patients with Prostate Cancer Using Steroids. In Urologic Oncology: Seminars and Original Investigations; Elsevier: Amsterdam, The Netherlands, 2022; Volume 40, pp. 451.e1–451.e8. [Google Scholar]
- Lorentzen, C.L.; Haanen, J.B.; Met, Ö.; Svane, I.M. Clinical Advances and Ongoing Trials on MRNA Vaccines for Cancer Treatment. Lancet Oncol. 2022, 23, e450–e458. [Google Scholar] [CrossRef]
- Islam, M.A.; Rice, J.; Reesor, E.; Zope, H.; Tao, W.; Lim, M.; Ding, J.; Chen, Y.; Aduluso, D.; Zetter, B.R. Adjuvant-Pulsed MRNA Vaccine Nanoparticle for Immunoprophylactic and Therapeutic Tumor Suppression in Mice. Biomaterials 2021, 266, 120431. [Google Scholar] [CrossRef]
- Tryggestad, A.M.A.; Axcrona, K.; Axcrona, U.; Bigalke, I.; Brennhovd, B.; Inderberg, E.M.; Hønnåshagen, T.K.; Skoge, L.J.; Solum, G.; Sæbøe-Larssen, S. Long-term First-in-man Phase I/II Study of an Adjuvant Dendritic Cell Vaccine in Patients with High-risk Prostate Cancer after Radical Prostatectomy. Prostate 2022, 82, 245–253. [Google Scholar] [CrossRef]
- Pisano, C.; Tucci, M.; Di Stefano, R.F.; Turco, F.; Scagliotti, G.V.; Di Maio, M.; Buttigliero, C. Interactions between Androgen Receptor Signaling and Other Molecular Pathways in Prostate Cancer Progression: Current and Future Clinical Implications. Crit. Rev. Oncol. Hematol. 2021, 157, 103185. [Google Scholar] [CrossRef]
- Rice, M.A.; Malhotra, S.V.; Stoyanova, T. Second-Generation Antiandrogens: From Discovery to Standard of Care in Castration Resistant Prostate Cancer. Front. Oncol. 2019, 9, 801. [Google Scholar] [CrossRef]
- Deluce, J.E.; Cardenas, L.; Lalani, A.-K.; Maleki Vareki, S.; Fernandes, R. Emerging Biomarker-Guided Therapies in Prostate Cancer. Curr. Oncol. 2022, 29, 5054–5076. [Google Scholar] [CrossRef]
- Gandaglia, G.; Leni, R.; Briganti, A. An Introduction on Immunotherapy in Prostate Cancer. In Neoadjuvant Immunotherapy Treatment of Localized Genitourinary Cancers; Springer: Berlin/Heidelberg, Germany, 2022; pp. 125–131. [Google Scholar]
- Huntington, N.D.; Cursons, J.; Rautela, J. The Cancer–Natural Killer Cell Immunity Cycle. Nat. Rev. Cancer 2020, 20, 437–454. [Google Scholar] [CrossRef]
- Zhou, Y.; Husman, T.; Cen, X.; Tsao, T.; Brown, J.; Bajpai, A.; Li, M.; Zhou, K.; Yang, L. Interleukin 15 in Cell-Based Cancer Immunotherapy. Int. J. Mol. Sci. 2022, 23, 7311. [Google Scholar] [CrossRef] [PubMed]
- Van Audenaerde, J.R.M.; Marcq, E.; von Scheidt, B.; Davey, A.S.; Oliver, A.J.; De Waele, J.; Quatannens, D.; Van Loenhout, J.; Pauwels, P.; Roeyen, G. Novel Combination Immunotherapy for Pancreatic Cancer: Potent Anti-tumor Effects with CD40 Agonist and Interleukin-15 Treatment. Clin. Transl. Immunol. 2020, 9, e1165. [Google Scholar] [CrossRef] [PubMed]
- Isvoranu, G.; Surcel, M.; Munteanu, A.N.; Bratu, O.G.; Ionita-Radu, F.; Neagu, M.T.; Chiritoiu-Butnaru, M. Therapeutic Potential of Interleukin-15 in Cancer. Exp. Ther. Med. 2021, 22, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Redman, J.M.; Madan, R.A.; Karzai, F.; Bilusic, M.; Cordes, L.; Marte, J.; Manu, M.; Williams, N.; Hankin, A.; Floudas, C. 616MO Efficacy of BN-Brachyury (BNVax)+ Bintrafusp Alfa (BA)+ N-803 in Castration-Resistant Prostate Cancer (CRPC): Results from a Preliminary Analysis of the Quick Efficacy Seeking Trial (QuEST1). Ann. Oncol. 2020, 31, S511. [Google Scholar] [CrossRef]
- Wolf, P.; Alzubi, J.; Gratzke, C.; Cathomen, T. The Potential of CAR T Cell Therapy for Prostate Cancer. Nat. Rev. Urol. 2021, 18, 556–571. [Google Scholar] [CrossRef]
- Schepisi, G.; Cursano, M.C.; Casadei, C.; Menna, C.; Altavilla, A.; Lolli, C.; Cerchione, C.; Paganelli, G.; Santini, D.; Tonini, G. CAR-T Cell Therapy: A Potential New Strategy against Prostate Cancer. J. Immunother. Cancer 2019, 7, 1–11. [Google Scholar] [CrossRef]
- Yu, H.; Pan, J.; Guo, Z.; Yang, C.; Mao, L. CART Cell Therapy for Prostate Cancer: Status and Promise. Onco. Targets. Ther. 2019, 12, 391. [Google Scholar] [CrossRef]
- Alzubi, J.; Dettmer-Monaco, V.; Kuehle, J.; Thorausch, N.; Seidl, M.; Taromi, S.; Schamel, W.; Zeiser, R.; Abken, H.; Cathomen, T. PSMA-Directed CAR T Cells Combined with Low-Dose Docetaxel Treatment Induce Tumor Regression in a Prostate Cancer Xenograft Model. Mol. Ther. 2020, 18, 226–235. [Google Scholar] [CrossRef]
- Dana, H.; Chalbatani, G.M.; Jalali, S.A.; Mirzaei, H.R.; Grupp, S.A.; Suarez, E.R.; Rapôso, C.; Webster, T.J. CAR-T Cells: Early Successes in Blood Cancer and Challenges in Solid Tumors. Acta Pharm. Sin. B 2021, 11, 1129–1147. [Google Scholar] [CrossRef]
- Lemoine, J.; Ruella, M.; Houot, R. Overcoming Intrinsic Resistance of Cancer Cells to CAR T-Cell KillingIntrinsic Resistance of Cancer Cells to CAR T-Cell Killing. Clin. Cancer Res. 2021, 27, 6298–6306. [Google Scholar] [CrossRef]
- Charrot, S.; Hallam, S. CAR-T Cells: Future Perspectives. Hemasphere 2019, 3, e188. [Google Scholar] [CrossRef]
- Slovin, S.F.; Dorff, T.B.; Falchook, G.S.; Wei, X.X.; Gao, X.; McKay, R.R.; Oh, D.Y.; Wibmer, A.G.; Spear, M.A.; McCaigue, J. Phase 1 Study of P-PSMA-101 CAR-T Cells in Patients with Metastatic Castration-Resistant Prostate Cancer (MCRPC). J. Clin. Oncol 2022, 40, 98. [Google Scholar] [CrossRef]
- Narayan, V.; Barber-Rotenberg, J.S.; Jung, I.-Y.; Lacey, S.F.; Rech, A.J.; Davis, M.M.; Hwang, W.-T.; Lal, P.; Carpenter, E.L.; Maude, S.L. PSMA-Targeting TGFβ-Insensitive Armored CAR T Cells in Metastatic Castration-Resistant Prostate Cancer: A Phase 1 Trial. Nat. Med. 2022, 28, 724–734. [Google Scholar] [CrossRef]
- Priceman, S.J.; Gerdts, E.A.; Tilakawardane, D.; Kennewick, K.T.; Murad, J.P.; Park, A.K.; Jeang, B.; Yamaguchi, Y.; Yang, X.; Urak, R. Co-Stimulatory Signaling Determines Tumor Antigen Sensitivity and Persistence of CAR T Cells Targeting PSCA+ Metastatic Prostate Cancer. Oncoimmunology 2018, 7, e1380764. [Google Scholar] [CrossRef]
- Weimin, S.; Abula, A.; Qianghong, D.; Wenguang, W. Chimeric Cytokine Receptor Enhancing PSMA-CAR-T Cell-Mediated Prostate Cancer Regression. Cancer Biol. Ther. 2020, 21, 570–580. [Google Scholar] [CrossRef]
- Schubert, M.-L.; Schmitt, M.; Wang, L.; Ramos, C.A.; Jordan, K.; Müller-Tidow, C.; Dreger, P. Side-Effect Management of Chimeric Antigen Receptor (CAR) T-Cell Therapy. Ann. Oncol. 2021, 32, 34–48. [Google Scholar] [CrossRef]
- Gust, J.; Taraseviciute, A.; Turtle, C.J. Neurotoxicity Associated with CD19-Targeted CAR-T Cell Therapies. CNS Drugs 2018, 32, 1091–1101. [Google Scholar] [CrossRef]
- Belin, C.; Devic, P.; Ayrignac, X.; Dos Santos, A.; Paix, A.; Sirven-Villaros, L.; Simard, C.; Lamure, S.; Gastinne, T.; Ursu, R. Description of Neurotoxicity in a Series of Patients Treated with CAR T-Cell Therapy. Sci. Rep. 2020, 10, 1–9. [Google Scholar] [CrossRef]
- Park, S.; Pascua, E.; Lindquist, K.C.; Kimberlin, C.; Deng, X.; Mak, Y.S.L.; Melton, Z.; Johnson, T.O.; Lin, R.; Boldajipour, B. Direct Control of CAR T Cells through Small Molecule-Regulated Antibodies. Nat. Commun. 2021, 12, 1–10. [Google Scholar] [CrossRef]
- Boulch, M.; Cazaux, M.; Loe-Mie, Y.; Thibaut, R.; Corre, B.; Lemaître, F.; Grandjean, C.L.; Garcia, Z.; Bousso, P. A Cross-Talk between CAR T Cell Subsets and the Tumor Microenvironment Is Essential for Sustained Cytotoxic Activity. Sci. Immunol. 2021, 6, eabd4344. [Google Scholar] [CrossRef]
- Runcie, K.; Budman, D.R.; John, V.; Seetharamu, N. Bi-Specific and Tri-Specific Antibodies-the next Big Thing in Solid Tumor Therapeutics. Mol. Med. 2018, 24, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Zorko, N.A.; Ryan, C.J. Novel Immune Engagers and Cellular Therapies for Metastatic Castration-Resistant Prostate Cancer: Do We Take a BiTe or Ride BiKEs, TriKEs, and CARs? Prostate Cancer Prostatic Dis. 2021, 24, 986–996. [Google Scholar] [CrossRef] [PubMed]
- Giraudet, A.-L.; Kryza, D.; Hofman, M.; Moreau, A.; Fizazi, K.; Flechon, A.; Hicks, R.J.; Tran, B. PSMA Targeting in Metastatic Castration-Resistant Prostate Cancer: Where Are We and Where Are We Going? Ther. Adv. Med. Oncol. 2021, 13, 17588359211053898. [Google Scholar] [CrossRef] [PubMed]
- Tran, B.; Horvath, L.; Dorff, T.; Rettig, M.; Lolkema, M.P.; Machiels, J.P.; Rottey, S.; Autio, K.; Greil, R.; Adra, N. 609O Results from a Phase I Study of AMG 160, a Half-Life Extended (HLE), PSMA-Targeted, Bispecific T-Cell Engager (BiTE®) Immune Therapy for Metastatic Castration-Resistant Prostate Cancer (MCRPC). Ann. Oncol. 2020, 31, S507. [Google Scholar] [CrossRef]
- Khadka, R.H.; Sakemura, R.; Kenderian, S.S.; Johnson, A.J. Management of Cytokine Release Syndrome: An Update on Emerging Antigen-Specific T Cell Engaging Immunotherapies. Immunotherapy 2019, 11, 851–857. [Google Scholar] [CrossRef]
- Singh, A.; Dees, S.; Grewal, I.S. Overcoming the Challenges Associated with CD3+ T-Cell Redirection in Cancer. Br. J. Cancer 2021, 124, 1037–1048. [Google Scholar] [CrossRef]
- Al-Haideri, M.; Tondok, S.B.; Safa, S.H.; Rostami, S.; Jalil, A.T.; Al-Gazally, M.E.; Alsaikhan, F.; Rizaev, J.A.; Mohammad, T.A.M.; Tahmasebi, S. CAR-T Cell Combination Therapy: The next Revolution in Cancer Treatment. Cancer Cell Int. 2022, 22, 1–26. [Google Scholar] [CrossRef]
- Al Saber, M.; Biswas, P.; Dey, D.; Kaium, M.A.; Islam, M.A.; Tripty, M.I.A.; Rahman, M.D.H.; Rahaman, T.I.; Biswas, M.Y.; Paul, P. A Comprehensive Review of Recent Advancements in Cancer Immunotherapy and Generation of CAR T Cell by CRISPR-Cas9. Processes 2021, 10, 16. [Google Scholar] [CrossRef]
- Akbari, P.; Katsarou, A.; Daghighian, R.; van Mil, L.W.H.G.; Huijbers, E.J.M.; Griffioen, A.W.; van Beijnum, J.R. Directing CAR T Cells towards the Tumor Vasculature for the Treatment of Solid Tumors. Biochim. Biophys. Acta-Rev. Cancer 2022, 1877, 188701. [Google Scholar] [CrossRef]
- Graff, J.N.; Beer, T.M.; Alumkal, J.J.; Slottke, R.E.; Redmond, W.L.; Thomas, G.V.; Thompson, R.F.; Wood, M.A.; Koguchi, Y.; Chen, Y. A Phase II Single-Arm Study of Pembrolizumab with Enzalutamide in Men with Metastatic Castration-Resistant Prostate Cancer Progressing on Enzalutamide Alone. J. Immunother. Cancer 2020, 8, e000642. [Google Scholar] [CrossRef]
- Mughees, M.; Kaushal, J.B.; Sharma, G.; Wajid, S.; Batra, S.K.; Siddiqui, J.A. Chemokines and Cytokines: Axis and Allies in Prostate Cancer Pathogenesis. In Seminars in Cancer Biology; Academic Press: Cambridge, MA, USA, 2022. [Google Scholar]
- Perera, M.P.J.; Thomas, P.B.; Risbridger, G.P.; Taylor, R.; Azad, A.; Hofman, M.S.; Williams, E.D.; Vela, I. Chimeric Antigen Receptor T-Cell Therapy in Metastatic Castrate-Resistant Prostate Cancer. Cancers 2022, 14, 503. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| No | Author, Year | Journal | Phase | Design | Inclusion Criteria | Intervention | 1° Outcome Measure(s) | Follow-Up | Sample Size | Efficacy Outcomes | Remarks |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Vogelzang, 2022 [25] | JAMA Oncology | Phase 3 | Double-blind, parallel-group, placebo-controlled, RCT; NCT02111577 | mCRPC with >4 months of castration period | DCVAC/PCa (add-on and maintenance) every 3–4 weeks up to 15 doses or placebo; in combination with chemotherapy (docetaxel plus prednisone) | OS | 58 months | 1182 | No difference in median OS between DCVAC/PCa (23.9 months, 95% CI = 21.6–25.3) and placebo groups (24.3 months, 95% CI = 22.6–26); HR = 1.04; 95% CI, 0.90–1.21; p = 0.6 | Primary objectives were unmet; treatment-emergent adverse events in DCVAC/PCa (9.2%) or placebo (12.7%) were comparable |
| 2 | Fizazi, 2021 [26] | European Urology | Phase 3 | Double-blind RCT (CA184–043); NCT00861614 | mCRPC, histologically/cytologically confirmed adenocarcinoma; ≥1 bone metastases, testosterone < 0.50 ng/mL | Bone-directed RT followed by ipilimumab IV (10 mg/kg) or placebo every 3 weeks (up to four doses); non-progressing patients: ipilimumab (10 mg/kg) or placebo as maintenance therapy every 3 months | OS | 2.4 years | 799 | OS rates were higher in the ipilimumab vs. placebo arms at 2 years: 25.2% vs. 16.6%, 3 years: 15.3% vs. 7.9%, 4 years: 10.1% vs. 3.3%, and 5 years: 7.9% vs. 2.7% | Disease progression was the most frequent cause of death in both arms; seven patients (1.8%) in the ipilimumab arm and one patient (0.3%) in the placebo arm died due to study drug toxicity |
| 3 | Noguchi, 2021 [27] | Oncology Reports | Phase 3 | Double-blind RCT; UMIN000011308 | HLA-A24-positive patients with castration-resistant PC; within 12 months of docetaxel chemotherapy | Personalized peptide vaccination or placebo using the minimization technique with age stratification factors: <75 or ≥75, and use of enzalutamide or abiraterone (with or without) | OS | 29.8 months and 27.4 months | 310 | The estimated median OS was 16.1 months (95% CI= 13–18.2) with PPV and 16.9 months (95% CI = 13.1–20.4) with placebo; HR = 1.04 (95% CI = 0.8–1.37, p = 0.77) | Both groups experience the same proportion of grade ≥ three adverse events (41%); OS did not expand with peptide vaccine therapy in HLA-A24-positive patients |
| 4 | Gulley, 2019 [28] | Journal of Clinical Oncology | Phase 3 | Multicenter, double-blind RCT; NCT01322490 | Progressive mCRPC, testosterone level < 50 ng/dL, current use of a GnRH agonist/antagonist (unless surgically castrated), chemotherapy naïve for metastatic PC | PROSTVAC plus GM-CSF, 250 μg, lyophilized (Arm VG), PROSTVAC plus placebo GM-CSF (Arm V), or vaccine placebo plus placebo GM-CSF (Arm P) | OS | 25 weeks | 1297 | None of the active treatment arms had an effect on median OS; Arm V, OS = 34.4 months, HR = 1.01 (95% CI = 0.84–1.2, p = 0.47); Arm VG, OS = 33.2 months, HR = 1.02 (95% CI = 0.86–1.22, p = 0.59); Placebo = 34.3 months | While PROSTVAC was well tolerated with <1% adverse events, no benefits were present for OS |
| No. | NCT Number | Status | Conditions | Interventions | Key Outcome Measures |
|---|---|---|---|---|---|
| 1 | NCT04301414 | Recruiting | Prostate Cancer | BMS-986218 and Degarelix | Adverse events; pCR; PSA |
| 2 | NCT04615845 | Recruiting | CRPC | Cellgram-DC-PC | Safety; immune response and tumor markers; PSA |
| 3 | NCT02740985 | Active, not recruiting | mCRPC and others | AZD4635; Durvalumab; Abiraterone Acetate; Enzalutamide; Oleclumab; Docetaxel | DLTs; adverse events; pharmacokinetics; tumor Response; PFS |
| 4 | NCT04388852 | Recruiting | CRPC; Metastatic Prostate Carcinoma; Stage IV, IVA, IVB Prostate Cancer AJCC v8 | Ipilimumab; Valemetostat | Adverse events; immunologic and molecular effects; TTF; ORR |
| 5 | NCT04660929 | Recruiting | HER2-positive; Prostate Cancer and various others | CT-0508 | Safety and tolerability; ORR, PFS |
| 6 | NCT01140373 | Active, not recruiting | Prostate Cancer | Engineered autologous T cells; Cyclophosphamide | Safety and tolerability; bone metastases/biomarkers of bone metastasis; humoral and cell-mediated immunity to PSMA and other known prostate cancer antigens; PSA; anti-PSMA autologous T cells |
| 7 | NCT03177460 | Active, not recruiting | Prostate Adenocarcinoma; Stage III, IIIA, IIIB, IIIC Prostate Cancer AJCC v8; Testosterone Greater Than 150 ng/dL | Daratumumab; FMS Inhibitor JNJ-40346527; Radical Prostatectomy | Adverse events; pCR; immune changes in blood/tumor tissue |
| 8 | NCT02009449 | Active, not recruiting | Prostate Cancer and various others | Pegilodecakin; Paclitaxel or Docetaxel and Carboplatin/Cisplatin; Oxaliplatin/Leucovorin/5-Fluorouracil; Gemcitabine/nab-paclitaxel; Capecitabine; Pazopanib; Pembrolizumab; Paclitaxel; Nivolumab; Gemcitabine/carboplatin | Safety and tolerability; adverse events; pharmacokinetics; change in tumor burden measured by volumetric CT/MRI; progression in bone-by-bone scintigraphy; anti-Pegilodecakin antibody formation |
| 9 | NCT04077021 | Active, not recruiting | mCRPC, Adenocarcinoma | CCW702 | Safety and tolerability; clinical efficacy |
| 10 | NCT04580485 | Recruiting | CRPC and various others | INCB106385; INCMGA00012 | Treatment-emergent adverse events; pharmacokinetic measures; ORR; DOR; Change in tumoral gene expression/immune cell activation |
| 11 | NCT03556228 | Recruiting | Any Solid Tumors; Prostate Cancer and various others | VMD-928 300 and 100 mg tablet | Adverse events; pharmacokinetics; analgesic; change in TrkA protein expression; correlation between clinical antitumor/analgesic response and TrkA protein expression/AUC |
| 12 | NCT03805594 | Active, not recruiting | CRPC; Metastatic PC; Prostate Adenocarcinoma; Stage IV, IVA, IVB Prostate Cancer | Lutetium Lu 177-PSMA-617; Pembrolizumab | ORR; adverse events; median DOR; PSA response rate; radiographic PFS; OS |
| 13 | NCT05077098 | Recruiting | Recurrent Prostate Cancer | ADXS-504 | Safety and tolerability; rates of treatment-related adverse events |
| 14 | NCT03792841 | Active, not recruiting | mCRPC | Acapatamab; Pembrolizumab; Etanercept; Cytochrome P450 Cocktail | Treatment-emergent adverse events; pharmacokinetics; ORR; PSA; DOR; PFS; OS; CTC response |
| 15 | NCT04477512 | Recruiting | Metastatic Hormone Refractory Prostate Cancer | Cabozantinib; Nivolumab; Abiraterone acetate; Prednisone | DLTs; PSA; ORR; OS; PFS; DSS; adverse events |
| 16 | NCT04514484 | Recruiting | Advanced/recurred PC; CRPC-Metastatic PC; Stage IV Prostate Cancer AJCC v8, and various others | Cabozantinib S-malate; Nivolumab | DLTs; immune status |
| 17 | NCT05354375 | Recruiting | Prostate Cancer | CAR-T cell immunotherapy | Safety; adverse events; PFS; OS |
| 18 | NCT04221542 | Recruiting | Prostate Cancer | AMG 509; Abiraterone; Enzalutamide; Pembrolizumab | Adverse events; DLTs; pharmacokinetics; ORR; DOR; PSA; PFS; OS |
| 19 | NCT05010200 | Recruiting | Prostate Cancer | PGV-001; Poly-ICLC; CDX-301 | Adverse events; immune cell changes; radiographic-free survival |
| No. | NCT Number | Phases | Age | N | Study Type and Design | Completion Date | Collaborators | Locations |
|---|---|---|---|---|---|---|---|---|
| 1 | NCT04301414 | Early Phase 1 | ≥18 years | 24 | Interventional; Randomized, Open Label, Treatment | May-24 | Matthew Dallos; Bristol-Myers Squibb; Ferring Pharmaceuticals; Columbia University | United States |
| 2 | NCT04615845 | Phase 1 | 20–80 years | 10 | Interventional; Single Group, Open Label, Treatment | Dec-22 | Pharmicell Co., Ltd. | Republic of Korea |
| 3 | NCT02740985 | Phase 1 | 18–130 years | 313 | Interventional; Non-Randomized, Open Label, Treatment | 28-Dec-22 | AstraZeneca | Various, United States |
| 4 | NCT04388852 | Phase 1 | ≥18 years | 80 | Interventional; Single Group, Open Label, Treatment | 31-Jan-23 | M.D. Anderson Cancer Center; National Cancer Institute (NCI) | United States |
| 5 | NCT04660929 | Phase 1 | ≥18 years | 18 | Interventional; Single Group, Open Label, Treatment | Feb-23 | Carisma Therapeutics Inc | Various, United States |
| 6 | NCT01140373 | Phase 1 | ≥18 years | 13 | Interventional; Single Group, Open Label, Treatment | Jun-23 | Memorial Sloan Kettering Cancer Center; United States Department of Defense | United States |
| 7 | NCT03177460 | Phase 1 | ≥18 years | 33 | Interventional; Non-Randomized, Open Label, Treatment | 29-Jun-23 | M.D. Anderson Cancer Center; National Cancer Institute (NCI) | United States |
| 8 | NCT02009449 | Phase 1 | ≥18 years | 350 | Interventional; Non-Randomized, Single Group, Open Label, Treatment | 17-Nov-23 | Eli Lilly and Company; ARMO BioSciences | Various, United States |
| 9 | NCT04077021 | Phase 1 | ≥18 years | 22 | Interventional; Non-Randomized, Open Label, Treatment | Dec-23 | Calibr, a division of Scripps Research | United States |
| 10 | NCT04580485 | Phase 1 | ≥18 years | 230 | Interventional; Non-Randomized, Parallel Assignment, Open Label, Treatment | 29-Dec-23 | Incyte Corporation | Various, United States, Belgium, France, Italy, Spain, United Kingdom |
| 11 | NCT03556228 | Phase 1 | ≥18 years | 74 | Interventional; Sequential Assignment, Open Label, Treatment | Jun-24 | VM Oncology, LLC | Various, United States |
| 12 | NCT03805594 | Phase 1 | ≥18 years | 43 | Interventional; Non-Randomized, Open Label, Treatment | 30-Apr-24 | University of California, San Francisco; Prostate Cancer Foundation; National Cancer Institute (NCI) | United States |
| 13 | NCT05077098 | Phase 1 | 18–99 Years | 21 | Interventional; Single Group, Open Label, Treatment | Sep-24 | Mark Stein; Columbia University | United States |
| 14 | NCT03792841 | Phase 1 | ≥18 years | 212 | Interventional; Non-Randomized, Open Label, Treatment | 16-May-25 | Amgen | Various, Australia, Austria, Belgium, Canada, Japan, Singapore, Taiwan |
| 15 | NCT04477512 | Phase 1 | ≥18 years | 22 | Interventional; Non-Randomized, Open Label, Treatment | 31-Aug-25 | Washington University School of Medicine; Bristol-Myers Squibb; Exelixis | United States |
| 16 | NCT04514484 | Phase 1 | ≥18 years | 18 | Interventional; Single Group, Open Label, Treatment | 2-Nov-25 | National Cancer Institute (NCI) | United States |
| 17 | NCT05354375 | Phase 1 | 18–75 Years | 20 | Interventional; Single Group, Open Label, Treatment | 30-Nov-26 | The Affiliated Hospital of Xuzhou Medical University; Xuzhou Medical University | China |
| 18 | NCT04221542 | Phase 1 | ≥18 years | 459 | Interventional; Non-Randomized, Open Label, Treatment | 9-Aug-27 | Amgen | Various, United States, Australia, Japan, Korea, Taiwan |
| 19 | NCT05010200 | Phase 1 | ≥18 years | 27 | Interventional; Non-Randomized, Open Label, Prevention | Dec-27 | Ashutosh Kumar Tewari; Icahn School of Medicine at Mount Sinai | United States |
| No. | NCT Number | Status | Conditions | Interventions | Key Outcome Measures |
|---|---|---|---|---|---|
| 1 | NCT03658447 | Active, not recruiting | mCRPC | Pembrolizumab; 177Lu-PSMA | PSA; treatment-emergent adverse events (safety); tolerability; Radiographic PFS; ORR DOR; TTR response; pain; quality of life |
| 2 | NCT04071236 | Recruiting | CRPC; Metastatic Malignant Neoplasm in the Lymph Nodes; Metastatic Prostate Carcinoma; Stage IV Prostate Cancer AJCC v8 | Avelumab; Peposertib; Radium Ra 223 Dichloride | DLTs, PFS; OS; SSE; toxicity and adverse events |
| 3 | NCT04382898 | Active, not recruiting | Prostate Cancer | BNT112; Cemiplimab | DLTs; adverse events; ORR; PSA levels; change in PSA doubling time |
| 4 | NCT03689699 | Active, not recruiting | Prostate Cancer; Adenocarcinoma | Nivolumab; Degarelix; BMS-986253 | PSA; safety and tolerability; RFS |
| 5 | NCT01688492 | Active, not recruiting | Prostate Cancer | Ipilimumab | PFS; PSA kinetics; changes in radionuclide bone scan |
| 6 | NCT03217747 | Active, not recruiting | CRPC; Metastasis in the Bone; Stage IV, IVA, IVB Prostate Cancer AJCC v8; | Avelumab; Ivuxolimab; Radiation Therapy; Utomilumab | Adverse events; CD8 immune biomarkers in tumor and blood; ORR; PFS; DOR; OS |
| 7 | NCT02933255 | Recruiting | Prostate Cancer | PROSTVAC-V/F; Nivolumab | Safety; immune cell changes; T cells in the tumor; pathologic responses; PSA changes; MRI changes |
| 8 | NCT03493945 | Recruiting | Metastatic Prostate Cancer; Prostate Cancer; Advanced Solid Tumor; Solid Tumor | M7824; N-803; MVA-BN-Brachyury; FPV-Brachyury; Epacadostat | PFS; safety profile |
| 9 | NCT05000294 | Recruiting | Prostate Cancer and various others | Atezolizumab; Tivozanib | ORR; PFS; OS; DCR |
| 10 | NCT03518606 | Active, not recruiting | Prostate Cancer and various others | Durvalumab; Tremelimumab; Metronomic Vinorelbine | MTD and RP2D |
| 11 | NCT03543189 | Recruiting | Prostate Cancer | Nivolumab; Brachytherapy; External Beam Radiation Therapy; Androgen Deprivation Therapy | Safety; DLTs; RFS; PSA |
| 12 | NCT04109729 | Recruiting | mCRPC | Nivolumab | Safety; PSA; PFS; bone metabolism markers; SSE |
| 13 | NCT05553639 | Not yet recruiting | Prostate Cancer Metastatic | HB-302/HB-301 Alternating 2-Vector Therapy | N/A |
| 14 | NCT04946370 | Recruiting | Prostate Cancer | 225Ac-J591; Pembrolizumab; Androgen receptor pathway inhibitor | DLTs; composite response rate; OS; PFS; OS; PSA |
| No. | NCT Number | Phases | N | Study Type and Design | Completion Date | Collaborators | Locations |
|---|---|---|---|---|---|---|---|
| 1 | NCT03658447 | Phase 1, 2 | 37 | Interventional; Single Group, Open Label, Treatment | Dec-22 | Peter MacCallum Cancer Centre, Australia | Australia |
| 2 | NCT04071236 | Phase 1, 2 | 90 | Interventional; Randomized, Open Label, Treatment | 31-Jan-23 | National Cancer Institute (NCI) | Various, United States |
| 3 | NCT04382898 | Phase 1, 2 | 115 | Interventional; Randomized, Open Label, Treatment | Jul-23 | BioNTech SE | Various, United States, Germany, Hungary, United Kingdom |
| 4 | NCT03689699 | Phase 1, 2 | 60 | Interventional; Randomized, Open Label, Treatment | Aug-23 | Matthew Dallos; Bristol-Myers Squibb; Columbia University | United States |
| 5 | NCT01688492 | Phase 1, 2 | 57 | Interventional; Single Group, Open Label, Treatment | Sep-23 | Memorial Sloan Kettering Cancer Center; Bristol-Myers Squibb; Northwestern University; Oregon Health and Science University | United States |
| 6 | NCT03217747 | Phase 1, 2 | 173 | Interventional; Non-Randomized, Open Label, Treatment | 30-Sep-23 | M.D. Anderson Cancer Center; National Cancer Institute (NCI) | United States |
| 7 | NCT02933255 | Phase 1, 2 | 29 | Interventional; Non-Randomized, Open Label, Treatment | 1-Dec-23 | National Cancer Institute (NCI); National Institutes of Health Clinical Center (CC) | United States |
| 8 | NCT03493945 | Phase 1, 2 | 113 | Interventional; Randomized, Open Label, Treatment | 31-Dec-23 | National Cancer Institute (NCI); National Institutes of Health Clinical Center (CC) | United States |
| 9 | NCT05000294 | Phase 1, 2 | 29 | Interventional; Sequential Assignment, Open Label, Treatment | Jun-24 | University of Florida; Genentech, Inc.; Aveo Oncology Pharmaceuticals | United States |
| 10 | NCT03518606 | Phase 1, 2 | 150 | Interventional; Non-Randomized, Open Label, Treatment | 30-Dec-24 | UNICANCER; National Cancer Institute, France; AstraZeneca; Pierre Fabre Laboratories | Various, France |
| 11 | NCT03543189 | Phase 1, 2 | 44 | Interventional; Single Group, Open Label, Treatment | Dec-24 | H. Lee Moffitt Cancer Center and Research Institute; Bristol-Myers Squibb | United States |
| 12 | NCT04109729 | Phase 1, 2 | 36 | Interventional; Single Group, Open Label, Treatment | 30-Apr-25 | University of Utah | United States |
| 13 | NCT05553639 | Phase 1, 2 | 70 | Interventional; Single Group, Open Label, Treatment | Sep-26 | Hookipa Biotech GmbH | United States |
| 14 | NCT04946370 | Phase 1, 2 | 76 | Interventional; Randomized, Open Label, Treatment | Jun-28 | Weill Medical College of Cornell University; United States Department of Defense; Merck Sharp & Dohme LLC | Various, United States |
| No. | NCT Number | Status | Conditions | Interventions | Key Outcome Measures |
|---|---|---|---|---|---|
| 1 | NCT03207867 | Active, not recruiting | mCRPC | NIR178; PDR001 | ORR; DCR; DOR; OS; PFS; safety and tolerability; pharmacokinetics |
| 2 | NCT03866382 | Recruiting | Metastatic Prostate Small-Cell Neuroendocrine Carcinoma; Stage IV, IVA, IVB Prostate Cancer AJCC v8 | Cabozantinib S-malate; Ipilimumab; Nivolumab | ORR; DOR; PFS; OS; CBR; adverse events |
| 3 | NCT02768363 | Active, not recruiting | Prostate Cancer | Aglatimagene besadenovec; valacyclovir | PFS; PSA; time to radical treatment; adverse events |
| 4 | NCT04104893 | Recruiting | mCRPC | Pembrolizumab | PSA; ORR; time to progression of disease; OS; adverse events (safety and tolerability) |
| 5 | NCT03651271 | Active, not recruiting | Advanced Metastatic Cancer; Advanced Prostate Cancer | Nivolumab Monotherapy; Nivolumab + Ipilimumab | CBR; CD8 cells in biopsies; safety; ORR |
| 6 | NCT03570619 | Active, not recruiting | mCRPC; Metastatic Cancer; Solid Tumor | Nivolumab; Ipilimumab | Patient response with CDK12 loss of function to treatment; PFS; TTP; OS; PSA |
| 7 | NCT02703623 | Active, not recruiting | CRPC; Metastatic PC; PSA Progression; Stage IV Prostate Adenocarcinoma AJCC v7 | Abiraterone Acetate; Apalutamide; Cabazitaxel; Carboplatin; Ipilimumab; Prednisone | OS; adverse events; androgen receptor response markers signature; TTF |
| 8 | NCT04009967 | Recruiting | Prostate Cancer | Pembrolizumab | Tumor response rate; Immune parameters; PSA; correlation of dMMR/MSI-H with pembrolizumab response |
| 9 | NCT03338790 | Active, not recruiting | Prostate Cancer | Nivolumab; docetaxel; enzalutamide; rucaparib; prednisone | ORR; PSA; PFS; time to response; DOR; adverse events; deaths; laboratory abnormalities |
| 10 | NCT03821246 | Recruiting | Prostate Adenocarcinoma; Localized Prostate Cancer | Atezolizumab; Tocilizumab; Etrumadenant | Positive response; adverse events; pCR; MRD; PSA response |
| 11 | NCT05177770 | Recruiting | mCRPC | SRF617; Etrumadenant; Zimberelimab | PSA; adverse events; ORR; DOR; DCR; pharmacokinetics; SSEs |
| 12 | NCT03315871 | Recruiting | Prostate Cancer | PROSTVAC-V; PROSTVAC-F; MSB0011359C (M7824); CV301 | PSA; adverse events |
| 13 | NCT02020070 | Active, not recruiting | Metastatic Castration-Sensitive Prostate Cancer | Degarelix; Ipilimumab; Radical Prostatectomy | PSA; PFS; OS; toxicity |
| 14 | NCT03385655 | Recruiting | Prostate Cancer | Adavosertib; Savolitinib; Darolutamide; CFI-400945; Ipatasertib; Durvalumab and Tremelimumab; Carboplatin | PSA decline of 50%; PSA progression; objective response; adverse events; PFS; OS |
| 15 | NCT03764540 | Recruiting | Metastatic Prostate Cancer | Cabazitaxel plus prednisone; Docetaxel plus prednisone | PSA response rate; PFS; OS; TTP; tumor response; DOR; pain response |
| 16 | NCT05502315 | Not yet recruiting | CRPC; Metastatic Cancer | Cabozantinib; Nivolumab | PFS; ORR; OS; CTC; adverse events; SSEs |
| 17 | NCT03795207 | Recruiting | Node/Bone Metastases; Prostate Cancer | SBRT + Durvalumab | PFS; ADT free survival; OS; acute toxicity; time to castration resistance |
| 18 | NCT05361798 | Recruiting | Prostate Cancer | M9241; SBRT | Safety; T cell clonality (immunologic activity); peripheral immune response |
| 19 | NCT04751929 | Recruiting | Prostate Cancer; mCRPC | Abemaciclib; Atezolizumab | PFS; ORR; DLTs; adverse events; CBR; DOR; DOT; TTP; OS |
| 20 | NCT04336943 | Recruiting | Biochemically Recurrent Prostate Carcinoma; Prostate Adenocarcinoma | Durvalumab; Olaparib | PSA; adverse events; quality of life |
| 21 | NCT03333616 | Recruiting | Non-adenocarcinoma Prostate Cancer, and various others | Ipilimumab; Nivolumab | ORR; DOR; OS; safety and tolerability; adverse events |
| 22 | NCT04717154 | Recruiting | Prostatic Neoplasms, Castration-Resistant | Ipilimumab; Nivolumab | DCR; adverse effects; ORR; PFS |
| 23 | NCT04126070 | Recruiting | Hormone-Sensitive Prostate Cancer; Prostate Adenocarcinoma; Metastasis Prostate Adenocarcinoma | ADT; Nivolumab; Docetaxel | PSA; ORR; OR; time to castration resistance/clinical progression/serologic progression; severe adverse events |
| 24 | NCT04592237 | Recruiting | Aggressive PC; CRPC; Metastatic Prostate Carcinoma; Metastatic Prostate Neuroendocrine Carcinoma; Metastatic Prostate Small-Cell Carcinoma; Stage IV Prostate Cancer AJCC v8 | Cabazitaxel; Carboplatin; Cetrelimab; Niraparib | PFS; OS; RR; adverse events |
| 25 | NCT04090528 | Recruiting | CRPC; Metastatic Cancer; Prostate Cancer | pTVG-HP; pTVG-AR; Pembrolizumab | PFS; ORR; PSA; RR; OS; antigen-specific Th1 immune response; safety and tolerability |
| 26 | NCT04926181 | Recruiting | Small Cell Neuroendocrine Carcinoma; Prostate Cancer; Small-Cell Carcinoma | Apalutamide; Cetrelimab | Composite RR; adverse events; median PFS; PSA; OS; OSS; DOR |
| 27 | NCT05445882 | Not yet recruiting | CRPC | Bintrafusp alfa; N-803; BN-Brachyury | Clinical efficacy; DOR; safety |
| 28 | NCT05168618 | Recruiting | CRPC; Metastatic Prostate Adenocarcinoma; Stage IV, IVA, IVB Prostate Cancer AJCC v8 | Atezolizumab; Cabozantinib S-malate | DCR; PSA; PFS; OS; adverse events |
| 29 | NCT05568550 | Not yet recruiting | Prostate Cancer | Pembrolizumab; Olaparib; ADT; Radiation Therapy | Clinical RR; biochemical/metastasis-free survival; molecular alterations in homologous recombination repair genes |
| 30 | NCT03879122 | Active, not recruiting | Metastatic Hormone-sensitive Prostate Cancer | Ipilimumab 5 MG/ML; Nivolumab 10 MG/ML; Docetaxel; ADT | OS; PSA; PFS; time to CRPC; PFS; SSEs; toxicity; quality of life |
| 31 | NCT01436968 | Active, not recruiting | Prostate Cancer | Aglatimagene besadenovec + valacyclovir; Placebo + valacyclovir | DFS; OS; PSA; safety; quality of life |
| 32 | NCT03686683 | Active, not recruiting | Adenocarcinoma, Prostate | Sipuleucel-T | Efficacy in reducing histopathologic reclassification to a higher Gleason grade |
| 33 | NCT05544227 | Recruiting | mCRPC | SV-102 | Anti-tumor activity; adverse events; treatment discontinuation |
| 34 | NCT05544240 | Recruiting | mCRPC | SV-101 | Anti-tumor activity; adverse events; treatment discontinuation |
| 35 | NCT02971358 | Recruiting | Locally Advanced and Metastatic Prostate Cancer | Radical prostatectomy | Perioperative complications; time to start ADT |
| No. | NCT Number | Phases | N | Study Type and Design | Completion Date | Collaborators | Locations |
|---|---|---|---|---|---|---|---|
| 1 | NCT03207867 | Phase 2 | 317 | Interventional; Non-Randomized, Open Label, Treatment | 21-Dec-22 | Novartis Pharmaceuticals; Novartis | Various, United States, Argentina, Australia, Belgium, Czechia, France, Germany, Italy, Japan, Netherlands, Singapore, Spain, Switzerland, Taiwan |
| 2 | NCT03866382 | Phase 2 | 224 | Interventional; Single Group, Open Label, Treatment | 28-Feb-23 | National Cancer Institute (NCI) | United States |
| 3 | NCT02768363 | Phase 2 | 187 | Interventional; Randomized; Quadruple Masking, Treatment | Mar-23 | Candel Therapeutics, Inc. | Various, United States, Mexico |
| 4 | NCT04104893 | Phase 2 | 30 | Interventional; Single Group, Open Label, Treatment | 31-Mar-23 | VA Office of Research and Development; Merck Sharp & Dohme LLC | Various, United States |
| 5 | NCT03651271 | Phase 2 | 220 | Interventional; Non-Randomized, Open Label, Treatment | May-23 | Parker Institute for Cancer Immunotherapy; Bristol-Myers Squibb; Cancer Research Institute, New York City | Various, United States |
| 6 | NCT03570619 | Phase 2 | 65 | Interventional; Non-Randomized, Open Label, Treatment | May-23 | University of Michigan Rogel Cancer Center; Memorial Sloan Kettering Cancer Center; University of California, San Francisco | Various, United States |
| 7 | NCT02703623 | Phase 2 | 196 | Interventional; Randomized, Open Label, Treatment | 18-May-23 | M.D. Anderson Cancer Center; National Cancer Institute (NCI) | United States |
| 8 | NCT04009967 | Phase 2 | 30 | Interventional; Single Group, Open Label, Treatment | 30-May-23 | CHU de Quebec-Universite Laval; Merck Sharp & Dohme LLC | Canada |
| 9 | NCT03338790 | Phase 2 | 292 | Interventional; Non-Randomized, Open Label, Treatment | 15-Jul-23 | Bristol-Myers Squibb; Clovis Oncology, Inc.; Astellas Pharma Inc | Various, United States, Australia, Brazil, Canada, Chile, France, Germany, Mexico, Spain |
| 10 | NCT03821246 | Phase 2 | 68 | Interventional; Non-Randomized, Open Label, Treatment | 31-Oct-23 | Lawrence Fong; Genentech, Inc.; University of California, San Francisco | United States |
| 11 | NCT05177770 | Phase 2 | 40 | Interventional; Single Group, Open Label, Treatment | Nov-23 | Surface Oncology; Arcus Biosciences, Inc. | Various, United States |
| 12 | NCT03315871 | Phase 2 | 40 | Interventional; Non-Randomized, Open Label, Treatment | 1-Dec-23 | National Cancer Institute (NCI); National Institutes of Health Clinical Center (CC) | United States |
| 13 | NCT02020070 | Phase 2 | 16 | Interventional; Non-Randomized, Open Label, Treatment | Dec-23 | Memorial Sloan Kettering Cancer Center; Ferring Pharmaceuticals | United States |
| 14 | NCT03385655 | Phase 2 | 500 | Interventional; Non-Randomized, Open Label, Treatment | 31-Jul-24 | Canadian Cancer Trials Group; Canadian Cancer Clinical Trials Network; BC Cancer Foundation | Various, Canada |
| 15 | NCT03764540 | Phase 2 | 214 | Interventional; Randomized, Open Label, Treatment | 30-Sep-24 | Centre hospitalier de l’Università de Montreal (CHUM); Genzyme, a Sanofi Company | Canada |
| 16 | NCT05502315 | Phase 2 | 50 | Interventional; Single Group, Open Label, Treatment | 12-Oct-24 | Rana McKay, MD; Exelixis; Bristol-Myers Squibb; Hoosier Cancer Research Network | N/A |
| 17 | NCT03795207 | Phase 2 | 96 | Interventional; Randomized, Open Label, Treatment | 21-Nov-24 | Institut Cancerologie de l’Ouest; AstraZeneca | Various, France |
| 18 | NCT05361798 | Phase 2 | 65 | Interventional; Randomized, Open Label, Treatment | 1-Dec-24 | National Cancer Institute (NCI); National Institutes of Health Clinical Center (CC) | United States |
| 19 | NCT04751929 | Phase 2 | 75 | Interventional; Randomized, Open Label, Treatment | 20-Dec-24 | Dana-Farber Cancer Institute; Eli Lilly and Company; Genentech, Inc. | United States |
| 20 | NCT04336943 | Phase 2 | 30 | Interventional; Single Group, Open Label, Treatment | 30-Apr-25 | University of Washington; AstraZeneca | United States |
| 21 | NCT03333616 | Phase 2 | 100 | Interventional; Single Group, Open Label, Treatment | 31-May-25 | Dana-Farber Cancer Institute; Bristol-Myers Squibb | Various, United States |
| 22 | NCT04717154 | Phase 2 | 75 | Interventional; Single Group, Open Label, Treatment | 30-Jun-25 | Radboud University Medical Center; Bristol-Myers Squibb | The Netherlands |
| 23 | NCT04126070 | Phase 2 | 60 | Interventional; Non-Randomized, Open Label, Treatment | 30-Jun-25 | Xiao X. Wei; Bristol-Myers Squibb; Dana-Farber Cancer Institute | United States |
| 24 | NCT04592237 | Phase 2 | 120 | Interventional; Randomized, Open Label, Treatment | 31-Dec-25 | M.D. Anderson Cancer Center; Janssen Pharmaceuticals | United States |
| 25 | NCT04090528 | Phase 2 | 60 | Interventional; Randomized, Open Label, Treatment | Dec-25 | University of Wisconsin, Madison; Merck Sharp & Dohme LLC; Madison Vaccines, Inc; Prostate Cancer Foundation | United States |
| 26 | NCT04926181 | Phase 2 | 24 | Interventional; Single Group, Open Label, Treatment | 31-May-26 | Rahul Aggarwal; Janssen Scientific Affairs, LLC; University of California, San Francisco | United States |
| 27 | NCT05445882 | Phase 2 | 28 | Interventional; Non-Randomized, Open Label, Treatment | 1-Aug-26 | National Cancer Institute (NCI); National Institutes of Health Clinical Center (CC) | United States |
| 28 | NCT05168618 | Phase 2 | 33 | Interventional; Single Group, Open Label, Treatment | Jan-27 | University of Utah; National Cancer Institute (NCI) | United States |
| 29 | NCT05568550 | Phase 2 | 64 | Interventional; Randomized, Open Label, Treatment | 2-Jan-28 | Zin W Myint; Merck Sharp & Dohme LLC; University of Kentucky | United States |
| 30 | NCT03879122 | Phase 2, 3 | 135 | Interventional; Randomized, Open Label, Treatment | 31-Dec-24 | Spanish Oncology Genito-Urinary Group; Syntax for Science, S.L; Bristol-Myers Squibb | Various, Spain |
| 31 | NCT01436968 | Phase 3 | 711 | Interventional; Randomized; Quadruple Masking, Treatment | Jun-2023 | Candel Therapeutics, Inc. | Various, United States, Puerto Rico |
| 32 | NCT03686683 | Phase 3 | 450 | Interventional; Randomized, Open Label, Treatment | May-23 | Dendreon; PRA Health Sciences | Various, United States |
| 33 | NCT05544227 | Not Applicable | 20 | Interventional; Single Group, Open Label, Treatment | 31-Dec-23 | Williams Cancer Foundation; Syncromune, Inc. | Mexico |
| 34 | NCT05544240 | Not Applicable | 20 | Interventional; Single Group, Open Label, Treatment | 31-Dec-23 | Williams Cancer Foundation; Syncromune, Inc. | Mexico |
| 35 | NCT02971358 | Not Applicable | 200 | Interventional; Single Group, Open Label, Treatment | Dec-27 | Medical University of Vienna | Austria |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rehman, L.u.; Nisar, M.H.; Fatima, W.; Sarfraz, A.; Azeem, N.; Sarfraz, Z.; Robles-Velasco, K.; Cherrez-Ojeda, I. Immunotherapy for Prostate Cancer: A Current Systematic Review and Patient Centric Perspectives. J. Clin. Med. 2023, 12, 1446. https://doi.org/10.3390/jcm12041446
Rehman Lu, Nisar MH, Fatima W, Sarfraz A, Azeem N, Sarfraz Z, Robles-Velasco K, Cherrez-Ojeda I. Immunotherapy for Prostate Cancer: A Current Systematic Review and Patient Centric Perspectives. Journal of Clinical Medicine. 2023; 12(4):1446. https://doi.org/10.3390/jcm12041446
Chicago/Turabian StyleRehman, Laeeq ur, Muhammad Hassan Nisar, Wajeeha Fatima, Azza Sarfraz, Nishwa Azeem, Zouina Sarfraz, Karla Robles-Velasco, and Ivan Cherrez-Ojeda. 2023. "Immunotherapy for Prostate Cancer: A Current Systematic Review and Patient Centric Perspectives" Journal of Clinical Medicine 12, no. 4: 1446. https://doi.org/10.3390/jcm12041446
APA StyleRehman, L. u., Nisar, M. H., Fatima, W., Sarfraz, A., Azeem, N., Sarfraz, Z., Robles-Velasco, K., & Cherrez-Ojeda, I. (2023). Immunotherapy for Prostate Cancer: A Current Systematic Review and Patient Centric Perspectives. Journal of Clinical Medicine, 12(4), 1446. https://doi.org/10.3390/jcm12041446