

Impact of Body Composition and Sarcopenia on Mortality in Chronic Obstructive Pulmonary Disease Patients

 , , ,
, , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Data Collection
2.2. Anthropometry
2.3. Bioelectrical Impedance Analysis (BIA)
2.4. Muscle Mass
2.5. Muscle Strength
2.6. Sarcopenia
2.7. Exercise Tolerance
2.8. Pulmonary Function
2.9. Endpoint
2.10. Statistical Analysis
3. Results
4. Discussion
Strengths and Limitations of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mirza, S.; Clay, R.D.; Koslow, M.A.; Scanlon, P.D. COPD Guidelines: A Review of the 2018 GOLD Report. Mayo Clin. Proc. 2018, 93, 1488–1502. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. The Top 10 Causes of Death. Available online: https://www.who.int/news-room/fact-sheets/detail/the-top-10-causes-of-death (accessed on 6 December 2022).
- Jones, S.E.; Maddocks, M.; Kon, S.S.; Canavan, J.L.; Nolan, C.M.; Clark, A.L.; Polkey, M.I.; Man, W.D. Sarcopenia in COPD: Prevalence, clinical correlates and response to pulmonary rehabilitation. Thorax 2015, 70, 213–218. [Google Scholar] [CrossRef] [PubMed]
- Maddocks, M.; Kon, S.S.; Jones, S.E.; Canavan, J.L.; Nolan, C.M.; Higginson, I.J.; Gao, W.; Polkey, M.I.; Man, W.D. Bioelectrical impedance phase angle relates to function, disease severity and prognosis in stable chronic obstructive pulmonary disease. Clin. Nutr. 2015, 34, 1245–1250. [Google Scholar] [CrossRef] [PubMed]
- Burtin, C.; Ter Riet, G.; Puhan, M.A.; Waschki, B.; Garcia-Aymerich, J.; Pinto-Plata, V.; Celli, B.; Watz, H.; Spruit, M.A. Handgrip weakness and mortality risk in COPD: A multicentre analysis. Thorax 2016, 71, 86–87. [Google Scholar] [CrossRef]
- De Blasio, F.; Scalfi, L.; Di Gregorio, A.; Alicante, P.; Bianco, A.; Tantucci, C.; Bellofiore, B.; de Blasio, F. Raw bioelectrical impedance analysis variables are independent predictors of early all-cause mortality in patients with COPD. Chest 2019, 155, 1148–1157. [Google Scholar] [CrossRef] [PubMed]
- Orea-Tejeda, A.; Gómez-Martínez, M.; González-Islas, D.; Flores-Cisneros, L.; Keirns-Davis, C.; Sánchez-Santillán, R.; Pérez-García, I.; Martínez-Luna, N.; Robles-Hernández, R.; Sánchez-Moreno, C.; et al. The impact of hydration status and fluid distribution on pulmonary function in COPD patients. Sci. Rep. 2022, 12, 1216. [Google Scholar] [CrossRef]
- Norman, K.; Stobäus, N.; Pirlich, M.; Bosy-Westphal, A. Bioelectrical phase angle and impedance vector analysis--clinical relevance and applicability of impedance parameters. Clin. Nutr. 2012, 31, 854–861. [Google Scholar] [CrossRef]
- Norman, K.; Wirth, R.; Neubauer, M.; Eckardt, R.; Stobäus, N. The bioimpedance phase angle predicts low muscle strength, impaired quality of life, and increased mortality in old patients with cancer. J. Am. Med. Dir. Assoc. 2015, 16, 173.E17–173.E22. [Google Scholar] [CrossRef]
- De Blasio, F.; Di Gregorio, A.; de Blasio, F.; Bianco, A.; Bellofiore, B.; Scalfi, L. Malnutrition and sarcopenia assessment in patients with chronic obstructive pulmonary disease according to international diagnostic criteria, and evaluation of raw BIA variables. Respir. Med. 2018, 134, 1–5. [Google Scholar] [CrossRef]
- Martínez-Luna, N.; Orea-Tejeda, A.; González-Islas, D.; Flores-Cisneros, L.; Keirns-Davis, C.; Sánchez-Santillán, R.; Pérez-García, I.; Gastelum-Ayala, Y.; Martínez-Vázquez, V.; Martínez-Reyna, Ó. Association between body composition, sarcopenia and pulmonary function in chronic obstructive pulmonary disease. BMC Pulm. Med. 2022, 22, 106. [Google Scholar] [CrossRef]
- Beaudart, C.; Zaaria, M.; Pasleau, F.; Reginster, J.Y.; Bruyère, O. Health Outcomes of Sarcopenia: A Systematic Review and Meta-Analysis. PLoS ONE 2017, 12, e0169548. [Google Scholar] [CrossRef]
- Zhang, X.; Wang, C.; Dou, Q.; Zhang, W.; Yang, Y.; Xie, X. Sarcopenia as a predictor of all-cause mortality among older nursing home residents: A systematic review and meta-analysis. BMJ Open 2018, 8, e021252. [Google Scholar] [CrossRef] [PubMed]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyère, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Sarcopenia: Revised European consensus on definition and diagnosis. Age Ageing 2019, 48, 16–31. [Google Scholar] [CrossRef] [PubMed]
- Eagan, T.M.; Gabazza, E.C.; D’Alessandro-Gabazza, C.; Gil-Bernabe, P.; Aoki, S.; Hardie, J.A.; Bakke, P.S.; Wagner, P.D. TNF-α is associated with loss of lean body mass only in already cachectic COPD patients. Respir. Res. 2012, 13, 48. [Google Scholar] [CrossRef] [PubMed]
- Langen, R.C.; Gosker, H.R.; Remels, A.H.; Schols, A.M. Triggers and mechanisms of skeletal muscle wasting in chronic obstructive pulmonary disease. Int. J. Biochem. Cell Biol. 2013, 45, 2245–2256. [Google Scholar] [CrossRef]
- Sepúlveda-Loyola, W.; Osadnik, C.; Phu, S.; Morita, A.A.; Duque, G.; Probst, V.S. Diagnosis, prevalence, and clinical impact of sarcopenia in COPD: A systematic review and meta-analysis. J. Cachexia Sarcopenia Muscle 2020, 11, 1164–1176. [Google Scholar] [CrossRef] [PubMed]
- Lin, B.; Bai, L.; Wang, S.; Lin, H. The association of systemic interleukin 6 and interleukin 10 levels with sarcopenia in elderly patients with chronic obstructive pulmonary disease. Int. J. Gen. Med. 2021, 14, 5893–5902. [Google Scholar] [CrossRef] [PubMed]
- Vogelmeier, C.F.; Criner, G.J.; Martinez, F.J.; Anzueto, A.; Barnes, P.J.; Bourbeau, J.; Celli, B.R.; Chen, R.; Decramer, M.; Fabbri, L.M.; et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive lung disease 2017 report. GOLD executive summary. Am. J. Respir. Crit. Care Med. 2017, 195, 557–582. [Google Scholar] [CrossRef]
- Lohman, T.G.; Roche, A.F.; Martorell, R. Anthropometric Standardization Reference Manual; Human Kinetics Books: Chicago, IL, USA, 1988. [Google Scholar]
- Lukaski, H.C.; Johnson, P.E.; Bolonchuk, W.W.; Lykken, G.I. Assessment of fat-free mass using bioelectrical impedance measurements of the human body. Am. J. Clin. Nutr. 1985, 41, 810–817. [Google Scholar] [CrossRef]
- Piccoli, A.; Nescolarde, L.; Rosell, J. Análisis convencional y vectorial de bioimpedancia en la práctica clínica. Nefrología 2002, 22, 228–238. [Google Scholar]
- Kyle, U.G.; Genton, L.; Pichard, C. Low phase angle determined by bioelectrical impedance analysis is associated with malnutrition and nutritional risk at hospital admission. Clin. Nutr. 2013, 32, 294–299. [Google Scholar] [CrossRef] [PubMed]
- Sergi, G.; De Rui, M.; Veronese, N.; Bolzetta, F.; Berton, L.; Carraro, S.; Bano, G.; Coin, A.; Manzato, E.; Perissinotto, E. Assessing appendicular skeletal muscle mass with bioelectrical impedance analysis in free-living Caucasian older adults. Clin. Nutr. 2015, 34, 667–673. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-García, W.D.; García-Castañeda, L.; Orea-Tejeda, A.; Mendoza-Núñez, V.; González-Islas, D.G.; Santillán-Díaz, C.; Castillo-Martínez, L. Handgrip strength: Reference values and its relationship with bioimpedance and anthropometric variables. Clin. Nutr. ESPEN 2017, 19, 54–58. [Google Scholar] [CrossRef]
- ATS Committee on Proficiency Standards for Clinical Pulmonary Function Laboratories. ATS statement: Guidelines for the six-minute walk test. Am. J. Respir. Crit. Care Med. 2002, 166, 111–117. [Google Scholar] [CrossRef]
- Miller, M.R.; Hankinson, J.; Brusasco, V.; Burgos, F.; Casaburi, R.; Coates, A.; Crapo, R.; Enright, P.; van der Grinten, C.P.; Gustafsson, P.; et al. Standardisation of spirometry. Eur. Respir. J. 2005, 26, 319–338. [Google Scholar] [CrossRef] [PubMed]
- Hankinson, J.L.; Odencrantz, J.R.; Fedan, K.B. Spirometric reference values from a sample of the general U.S. population. Am. J. Respir. Crit. Care Med. 1999, 159, 179–187. [Google Scholar] [CrossRef] [PubMed]
- Schols, A.M.; Broekhuizen, R.; Weling-Scheepers, C.A.; Wouters, E.F. Body composition and mortality in chronic obstructive pulmonary disease. Am. J. Clin. Nutr. 2005, 82, 53–59. [Google Scholar] [CrossRef]
- Benz, E.; Wijnant, S.R.A.; Trajanoska, K.; Arinze, J.T.; de Roos, E.W.; de Ridder, M.; Williams, R.; van Rooij, F.; Verhamme, K.M.C.; Ikram, M.A.; et al. Sarcopenia, systemic immune-inflammation index and all-cause mortality in middle-aged and older people with COPD and asthma: A population-based study. ERJ Open Res. 2022, 8, 628–2021. [Google Scholar] [CrossRef]
- Ribeiro, H.S.; Neri, S.G.R.; Oliveira, J.S.; Bennett, P.N.; Viana, J.L.; Lima, R.M. Association between sarcopenia and clinical outcomes in chronic kidney disease patients: A systematic review and meta-analysis. Clin. Nutr. 2022, 41, 1131–1140. [Google Scholar] [CrossRef]
- Kim, S.; Yoon, H.K.; Rhee, C.K.; Jung, H.W.; Lee, H.; Jo, Y.S. hand grip strength and likelihood of moderate-to-severe airflow limitation in the general population. Int. J. Chronic Obstr. Pulm. Dis. 2022, 17, 1237–1245. [Google Scholar] [CrossRef]
- Celis-Morales, C.A.; Welsh, P.; Lyall, D.M.; Steell, L.; Petermann, F.; Anderson, J.; Iliodromiti, S.; Sillars, A.; Graham, N.; Mackay, D.F.; et al. Associations of grip strength with cardiovascular, respiratory, and cancer outcomes and all cause mortality: Prospective cohort study of half a million UK Biobank participants. BMJ 2018, 361, k1651. [Google Scholar] [CrossRef] [PubMed]
- Hopkinson, N.S.; Tennant, R.C.; Dayer, M.J.; Swallow, E.B.; Hansel, T.T.; Moxham, J.; Polkey, M.I. A prospective study of decline in fat free mass and skeletal muscle strength in chronic obstructive pulmonary disease. Respir. Res. 2007, 8, 25. [Google Scholar] [CrossRef] [PubMed]
- Couillard, A.; Prefaut, C. From muscle disuse to myopathy in COPD: Potential contribution of oxidative stress. Eur. Respir. J. 2005, 26, 703–719. [Google Scholar] [CrossRef] [PubMed]
- Byun, M.K.; Cho, E.N.; Chang, J.; Ahn, C.M.; Kim, H.J. Sarcopenia correlates with systemic inflammation in COPD. Int. J. Chronic Obstr. Pulm. Dis. 2017, 12, 669–675. [Google Scholar] [CrossRef]
- Vestbo, J.; Prescott, E.; Almdal, T.; Dahl, M.; Nordestgaard, B.G.; Andersen, T.; Sørensen, T.I.; Lange, P. Body mass, fat-free body mass, and prognosis in patients with chronic obstructive pulmonary disease from a random population sample: Findings from the Copenhagen City Heart Study. Am. J. Respir. Crit. Care Med. 2006, 173, 79–83. [Google Scholar] [CrossRef]
- Batsis, J.A.; Mackenzie, T.A.; Emeny, R.T.; Lopez-Jimenez, F.; Bartels, S.J. Low lean mass with and without obesity, and mortality: Results from the 1999-2004 national health and nutrition examination survey. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2017, 72, 1445–1451. [Google Scholar] [CrossRef]
- Schnyder, S.; Handschin, C. Skeletal muscle as an endocrine organ: PGC-1α, myokines and exercise. Bone 2015, 80, 115–125. [Google Scholar] [CrossRef]
- Höglund, J.; Boström, C.; Sundh, J. Six-minute walking test and 30 s chair-stand-test as predictors of mortality in COPD—A cohort study. Int. J. Chronic Obstr. Pulm. Dis. 2022, 17, 2461–2469. [Google Scholar] [CrossRef]
- Celli, B.R.; Cote, C.G.; Marin, J.M.; Casanova, C.; Montes de Oca, M.; Mendez, R.A.; Pinto Plata, V.; Cabral, H.J. The body-mass index, airflow obstruction, dyspnea, and exercise capacity index in chronic obstructive pulmonary disease. N. Engl. J. Med. 2004, 350, 1005–1012. [Google Scholar] [CrossRef]
- Tsimogianni, A.M.; Papiris, S.A.; Stathopoulos, G.T.; Manali, E.D.; Roussos, C.; Kotanidou, A. Predictors of outcome after exacerbation of chronic obstructive pulmonary disease. J. Gen. Intern. Med. 2009, 24, 1043–1048. [Google Scholar] [CrossRef][Green Version]
- Evans, W.J.; Morley, J.E.; Argilés, J.; Bales, C.; Baracos, V.; Guttridge, D.; Jatoi, A.; Kalantar-Zadeh, K.; Lochs, H.; Mantovani, G.; et al. Cachexia: A new definition. Clin. Nutr. 2008, 27, 793–799. [Google Scholar] [CrossRef] [PubMed]
- Bernardes, S.; Eckert, I.C.; Burgel, C.F.; Teixeira, P.J.Z.; Silva, F.M. Increased energy and/or protein intake improves anthropometry and muscle strength in COPD patients: A systematic review with meta-analysis on randomized controlled clinical trials. Br. J. Nutr. 2022, 1–55. [Google Scholar] [CrossRef] [PubMed]
- Beaumont, M.; Forget, P.; Couturaud, F.; Reychler, G. Effects of inspiratory muscle training in COPD patients: A systematic review and meta-analysis. Clin. Respir. J. 2018, 12, 2178–2188. [Google Scholar] [CrossRef] [PubMed]
- Lee, E.N.; Kim, M.J. Meta-analysis of the effect of a pulmonary rehabilitation program on respiratory muscle strength in patients with chronic obstructive pulmonary disease. Asian Nurs. Res. 2019, 13, 1–10. [Google Scholar] [CrossRef]
- Siafakas, N.M.; Vermeire, P.; Pride, N.B.; Paoletti, P.; Gibson, J.; Howard, P.; Yernault, J.C.; Decramer, M.; Higenbottam, T.; Postma, D.S.; et al. Optimal assessment and management of chronic obstructive pulmonary disease (COPD). The European respiratory society task force. Eur. Respir. J. 1995, 8, 1398–1420. [Google Scholar] [CrossRef]
- Marin, J.M.; Carrizo, S.J.; Casanova, C.; Martinez-Camblor, P.; Soriano, J.B.; Agusti, A.G.; Celli, B.R. Prediction of risk of COPD exacerbations by the BODE index. Respir. Med. 2009, 103, 373–378. [Google Scholar] [CrossRef]


{kind=link}
| Total Population n = 240 | Non Survival n = 31 | Survival n = 209 | p-Value | |
|---|---|---|---|---|
| Clinical variables | ||||
| Age, years | 72.32 ± 8.24 | 78.70 ± 7.16 | 71.37 ± 8.66 | <0.001 |
| Male, n (%) | 123 (51.25) | 19 (61.29) | 104 (49.76) | 0.231 |
| Diabetes, n (%) | 62 (25.83) | 4 (12.90) | 58 (27.75) | 0.078 |
| Hypertension, n (%) | 118 (49.17) | 16 (51.61) | 102 (48.80) | 0.770 |
| Overweight or obesity, n (%) | 167 (69.58) | 17 (54.84) | 150 (71.77) | 0.056 |
| Heart Failure, n (%) | 101 (42.08) | 17 (54.84) | 84 (40.19) | 0.123 |
| FEV1, (%) | 57.61 ± 23.55 | 62.25 ± 23.57 | 56.94 ± 23.54 | 0.283 |
| FEV1, (L) | 1.26 ± 0.63 | 1.23 ± 0.57 | 1.27 ± 0.64 | 0.772 |
| FEV1/FVC | 0.55 ± 0.15 | 0.59 ± 0.17 | 0.55 ± 0.15 | 0.184 |
| GOLD Stage, n (%) | ||||
| 1–2 | 133 (60.18) | 19 (67.86) | 114 (59.07) | |
| 3–4 | 88 (39.82) | 9 (32.14) | 79 (40.93) | 0.375 |
| BODE index | 3 [2 to 4] | 4 [2 to 5] | 3 [1 to 4] | <0.001 |
| Hospitalization, n (%) | 54 (22.50) | 13 (41.94) | 41 (19.62) | 0.005 |
| Length of hospital stay, d | 8 [3,4,5,6,7,8,9,10,11,12,13,14] | 8 [1,2,3,4,5,6,7,8,9,10,11,12,13,14,15,16,17] | 8 [4,5,6,7,8,9,10,11,12] | 0.793 |
| Exacerbations in the previous year, n (%) | 43 (17.92) | 10 (32.26) | 33 (15.79) | 0.026 |
| Body composition | ||||
| Height, cm | 157.02 ± 11.76 | 156.28 ± 11.97 | 157.12 ± 11.76 | 0.709 |
| Weight, kg | 70.02 ± 18.35 | 65.60 ± 14.61 | 70.67 ± 18.78 | 0.151 |
| Body Mass Index, kg/m2 | 28.44 ± 7.43 | 26.67 ± 5.53 | 28.70 ± 7.65 | 0.156 |
| Fat Mass, kg | 39.83 ± 10.13 | 38.56 ± 7.80 | 39.97 ± 10.35 | 0.611 |
| Fat Free Mass Index, kg/m | 16.62 ± 3.42 | 16.57 ± 2.38 | 16.63 ± 3.54 | 0.955 |
| Total body water, % | 51.64 ± 8.17 | 53.18 ± 7.05 | 51.40 ± 8.32 | 0.274 |
| Extracellular water, % | 27.77 ± 6.03 | 30.01 ± 3.84 | 27.48 ± 6.22 | 0.155 |
| Impedance ratio | 0.83 [0.81–0.85] | 0.84 [0.83–0.86] | 0.83 [0.81–0.85] | 0.149 |
| Handgrip strength, kg | 22.75 ± 8.63 | 20.68 ± 8.77 | 23.02 ± 8.60 | 0.213 |
| Phase angle, ° | 5.05 ± 0.96 | 4.62 ± 1.06 | 5.11 ± 0.95 | 0.008 |
| ASMMI, kg/m2 | 6.85 ± 1.17 | 6.70 ± 0.90 | 6.88 ± 1.20 | 0.336 |
| Low muscle strength, n (%) | 91 (44.61) | 16 (66.67) | 75 (41.67) | 0.021 |
| Low muscle mass, n (%) | 93 (39.57) | 16 (51.61) | 77 (37.75) | 0.141 |
| Sarcopenia, n (%) | 77 (32.08) | 17 (54.84) | 60 (28.71) | 0.004 |
| Exercise tolerance, m | 319.04 ± 133.06 | 259.55 ± 175.50 | 327.87 ± 123.68 | 0.043 |
| HR | CI 95% | p-Value | |
|---|---|---|---|
| Age, years | 1.11 | 1.05 to 1.17 | 0.001 |
| Male | 1.95 | 0.94 to 4.03 | 0.069 |
| Diabetes | 0.48 | 0.14 to 1.50 | 0.089 |
| Hypertension | 1.12 | 0.55 to 2.28 | 0.739 |
| Overweight or obesity | 0.59 | 0.29 to1.21 | 0.157 |
| Heart Failure | 1.92 | 0.94 to 3.93 | 0.072 |
| FEV1, (%) | 1.00 | 0.98 to 1.02 | 0.651 |
| FEV1, (L) | 0.91 | 0.47 to 1.79 | 0.805 |
| FEV1/FVC | 3.45 | 0.29 to 40.73 | 0.325 |
| III-IV GOLD Stage | 1.05 | 0.68 to 1.62 | 0.793 |
| BODE index | 1.50 | 1.24 to 1.83 | <0.001 |
| Hospitalization | 1.77 | 0.86 to 3.65 | 0.119 |
| Length of hospital stay | 1.06 | 0.97 to 1.03 | 0.654 |
| Exacerbations in the previous year | 1.91 | 0.89 to 4.06 | 0.093 |
| Body composition | |||
| Height, cm | 1.00 | 0.97 to 1.03 | 0.764 |
| Weight, kg | 0.98 | 0.96 to 1.01 | 0.325 |
| Body Mass Index, kg/m2 | 0.96 | 0.90 to 1.01 | 0.185 |
| Fat Mass, % | 0.97 | 0.92 to 1.02 | 0.334 |
| Fat Free Mass Index, kg/m | 0.98 | 0.83 to 1.16 | 0.844 |
| Total body water, % | 1.02 | 0.97 to 1.06 | 0.351 |
| Extracellular water, % | 1.01 | 0.96 to 1.06 | 0.577 |
| IR above 50th percentile | 1.87 | 0.88 to 3.96 | 0.102 |
| Handgrip strength, kg | 0.97 | 0.92 to 1.02 | 0.275 |
| Phase angle, ° | 0.54 | 0.35 to 0.84 | 0.007 |
| PhA below 50th percentile | 4.04 | 1.73 to 9.41 | 0.001 |
| ASMMI, kg/m2 | 0.96 | 0.70 to 1.33 | 0.846 |
| Low muscle strength | 2.76 | 1.17 to 6.46 | 0.019 |
| Low muscle mass | 1.64 | 0.80 to 3.35 | 0.176 |
| Sarcopenia | 2.57 | 1.26 to 5.25 | 0.009 |
| Exercise tolerance, per meter increase | 0.99 | 0.992 to 1.00 | 0.061 |
| HR | CI 95% | p-Value | |
|---|---|---|---|
| Height, cm | 1.00 | 0.97 to 1.03 | 0.764 |
| Weight, kg | 0.98 | 0.96 to 1.01 | 0.325 |
| Body Mass Index, kg/m2 | 0.98 | 0.96 to 1.01 | 0.325 |
| Fat Mass, % | 1.05 | 0.94 to 1.17 | 0.367 |
| Fat Free Mass Index, kg/m | 0.94 | 0.77 to 1.15 | 0.878 |
| Total body water, % | 1.00 | 0.95 to 1.06 | 0.730 |
| Extracellular water, % | 1.01 | 0.95 to 1.06 | 0.683 |
| IR above 50th percentile | 1.61 | 0.73 to 3.52 | 0.231 |
| Handgrip strength, kg | 0.91 | 0.85 to 0.96 | 0.002 |
| Phase angle, ° | 0.59 | 0.37 to 0.94 | 0.026 |
| PhA below 50th percentile | 3.47 | 1.45 to 8.29 | 0.005 |
| ASMMI, kg/m2 | 0.88 | 0.59 to 1.31 | 0.539 |
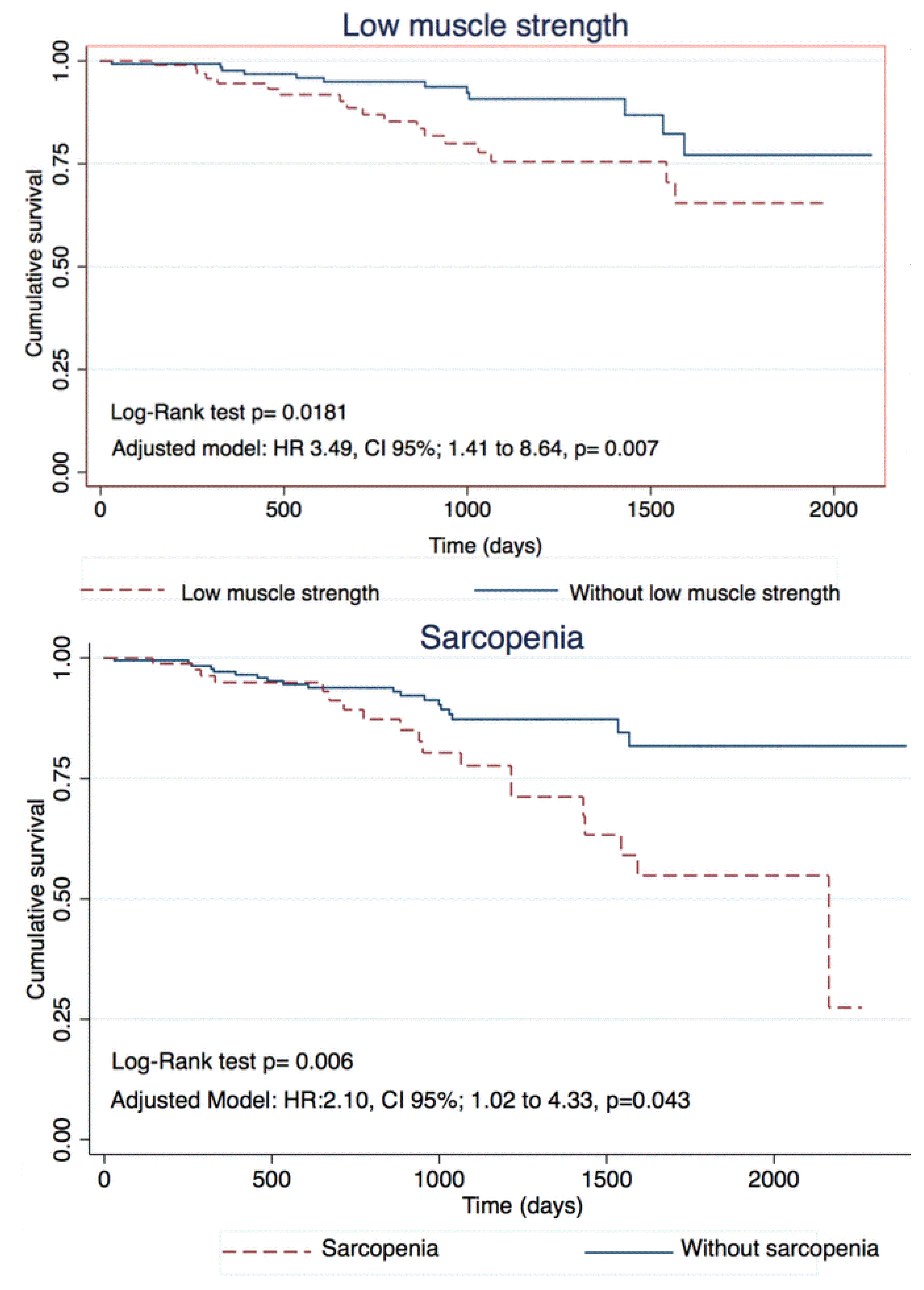
| Low muscle strength | 3.49 | 1.41 to 8.64 | 0.007 |
| Low muscle mass | 1.49 | 0.72 to 3.10 | 0.277 |
| Sarcopenia | 2.10 | 1.02 to 4.33 | 0.043 |
| Exercise tolerance, per meter increase | 0.99 | 0.992 to 0.999 | 0.022 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gómez-Martínez, M.; Rodríguez-García, W.; González-Islas, D.; Orea-Tejeda, A.; Keirns-Davis, C.; Salgado-Fernández, F.; Hernández-López, S.; Jiménez-Valentín, A.; Ríos-Pereda, A.V.; Márquez-Cordero, J.C.; et al. Impact of Body Composition and Sarcopenia on Mortality in Chronic Obstructive Pulmonary Disease Patients. J. Clin. Med. 2023, 12, 1321. https://doi.org/10.3390/jcm12041321
Gómez-Martínez M, Rodríguez-García W, González-Islas D, Orea-Tejeda A, Keirns-Davis C, Salgado-Fernández F, Hernández-López S, Jiménez-Valentín A, Ríos-Pereda AV, Márquez-Cordero JC, et al. Impact of Body Composition and Sarcopenia on Mortality in Chronic Obstructive Pulmonary Disease Patients. Journal of Clinical Medicine. 2023; 12(4):1321. https://doi.org/10.3390/jcm12041321
Chicago/Turabian StyleGómez-Martínez, Manuel, Wendy Rodríguez-García, Dulce González-Islas, Arturo Orea-Tejeda, Candace Keirns-Davis, Fernanda Salgado-Fernández, Samantha Hernández-López, Angelia Jiménez-Valentín, Alejandra Vanessa Ríos-Pereda, Juan Carlos Márquez-Cordero, and et al. 2023. "Impact of Body Composition and Sarcopenia on Mortality in Chronic Obstructive Pulmonary Disease Patients" Journal of Clinical Medicine 12, no. 4: 1321. https://doi.org/10.3390/jcm12041321
APA StyleGómez-Martínez, M., Rodríguez-García, W., González-Islas, D., Orea-Tejeda, A., Keirns-Davis, C., Salgado-Fernández, F., Hernández-López, S., Jiménez-Valentín, A., Ríos-Pereda, A. V., Márquez-Cordero, J. C., Salvatierra-Escobar, M., & López-Vásquez, I. (2023). Impact of Body Composition and Sarcopenia on Mortality in Chronic Obstructive Pulmonary Disease Patients. Journal of Clinical Medicine, 12(4), 1321. https://doi.org/10.3390/jcm12041321