
Antisclerostin Effect on Osseointegration and Bone Remodeling

 , , and
, , and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Information Sources and Search Strategy
2.2. Inclusion Criteria
2.3. Exclusion Criteria
2.4. Selection of Studies and Data Extraction
3. Results
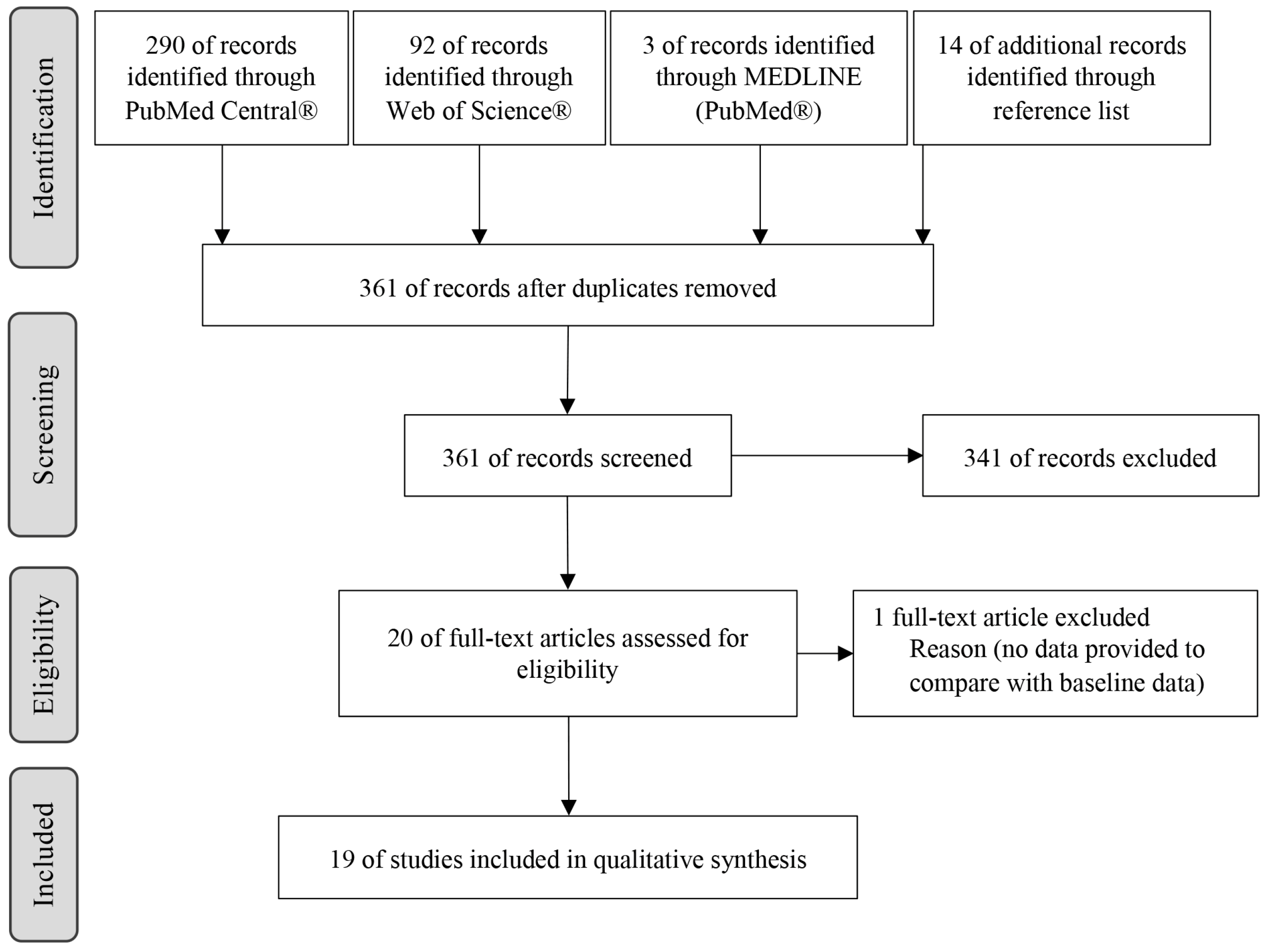
3.1. Study Selection
3.2. Study Characteristics and Details
3.3. Included Studies
3.3.1. Dosages Used
3.3.2. Implant Characteristics
3.4. Osseointegration and Bone-Implant Contact (BIC)
3.4.1. Bone Mineral Density (BMD)
3.4.2. Bone Area/Total Area (BA/TA) and Bone Volume Fraction (BVF)
3.4.3. Bone Thickness, Trabecular Thickness (Tb.Th) and Cortical Thickness (Ct.Th)
3.4.4. Trabecular Number (Tb.N) and Trabecular Separation (Tb.Sp)
3.5. Bone Remodeling
3.5.1. Bone Mineral Density (BMD) and Bone Content
3.5.2. Bone Area (BA)/Total Area (TA) and Bone Volume Fraction (BVF)
3.5.3. Bone Volume, Bone Height and Bone Area
3.5.4. Trabecular, Cortical, Medullary and Subperiosteal Areas
3.5.5. Trabecular Thickness (Tb.Th) and Cortical Thickness (Ct.Th)
3.5.6. Structural Model Index (SMI)
3.5.7. Mineralizing Surface (MS) and Mineral Apposition Rate (MAR)
3.5.8. Bone Formation Rate (BFR)
3.5.9. Bone Formation/Resorption Biomarkers
3.5.10. Bone Strength Endpoints
Maximum Load
Stiffness
3.6. Incidents Found
4. Discussion
4.1. Osseointegration of Implants
4.2. Bone Mineral Density (BMD)
4.3. Bone Area (BA)/Total Area (TA) and Bone Volume (BV)/Total Volume (TV)
4.4. Cortical and Trabecular Analysis
4.5. Bone Formation Rate (BFR)
4.6. Bone Strength and Stiffness
4.7. Bone Biomarkers
4.8. Study Applicability
4.9. Limitations of the Study
5. Conclusions
Supplementary Materials
Funding
Conflicts of Interest
References
- Brunkow, M.E.; Gardner, J.C.; Van Ness, J.; Paeper, B.W.; Kovacevich, B.R.; Proll, S.; Skonier, J.E.; Zhao, L.; Sabo, P.J.; Fu, Y.; et al. Bone dysplasia sclerosteosis results from loss of the SOST gene product, a novel cystine knot-containing protein. Am. J. Hum. Genet. 2001, 68, 577–589. [Google Scholar] [CrossRef]
- Balemans, W.; Ebeling, M.; Patel, N.; Van Hul, E.; Olson, P.; Dioszegi, M.; Lacza, C.; Wuyts, W.; Van Den Ende, J.; Willems, P.; et al. Increased bone density in sclerosteosis is due to the deficiency of a novel secreted protein (SOST). Hum. Mol. Genet. 2001, 10, 537–543. [Google Scholar] [CrossRef]
- Bezooijen, R.; Papapoulos, S.; Hamdy, N.; Dijke, P.; Löwik, C. Control of bone formation by osteocytes? lessons from the rare skeletal disorders sclerosteosis and van Buchem disease. BoneKEy-Osteovision 2005, 2, 33–38. [Google Scholar] [CrossRef]
- van Bezooijen, R.L.; Roelen, B.A.; Visser, A.; van der Wee-Pals, L.; de Wilt, E.; Karperien, M.; Hamersma, H.; Papapoulos, S.E.; ten Dijke, P.; Löwik, C.W.G.M. Sclerostin is an osteocyte-expressed negative regulator of bone formation, but not a classical BMP antagonist. J. Exp. Med. 2004, 199, 805–814. [Google Scholar] [CrossRef]
- Poole, K.E.; van Bezooijen, R.L.; Loveridge, N.; Hamersma, H.; Papapoulos, S.E.; Löwik, C.W.; Reeve, J. Sclerostin is a delayed secreted product of osteocytes that inhibits bone formation. FASEB J. 2005, 19, 1842–1844. [Google Scholar] [CrossRef] [PubMed]
- Lewiecki, E.M. Role of sclerostin in bone and cartilage and its potential as a therapeutic target in bone diseases. Ther. Adv. Musculoskelet. Dis. 2014, 6, 48–57. [Google Scholar] [CrossRef] [PubMed]
- Winkler, D.G.; Sutherland, M.S.; Ojala, E.; Turcott, E.; Geoghegan, J.C.; Shpektor, D.; Skonier, J.E.; Yu, C.; Latham, J.A. Sclerostin inhibition of Wnt-3a-induced C3H10T1/2 cell differentiation is indirect and mediated by bone morphogenetic proteins. J. Biol. Chem. 2005, 280, 2498–2502. [Google Scholar] [CrossRef]
- Krishnan, V.; Bryant, H.U.; Macdougald, O.A. Regulation of bone mass by Wnt signaling. J. Clin. Investig. 2006, 116, 1202–1209. [Google Scholar] [CrossRef] [PubMed]
- van Bezooijen, R.L.; Svensson, J.P.; Eefting, D.; Visser, A.; van der Horst, G.; Karperien, M.; Quax, P.H.A.; Vrieling, H.; Papapoulos, S.E.; ten Dijke, P.; et al. Wnt but not BMP signaling is involved in the inhibitory action of sclerostin on BMP-stimulated bone formation. J. Bone Miner. Res. 2007, 22, 19–28. [Google Scholar] [CrossRef]
- ten Dijke, P.; Krause, C.; de Gorter, D.J.; Löwik, C.W.; van Bezooijen, R.L. Osteocyte-derived sclerostin inhibits bone formation: Its role in bone morphogenetic protein and Wnt signaling. J. Bone Jt. Surg. Am. 2008, 90 (Suppl. 1), 31–35. [Google Scholar] [CrossRef]
- Hill, T.P.; Später, D.; Taketo, M.M.; Birchmeier, W.; Hartmann, C. Canonical Wnt/beta-catenin signaling prevents osteoblasts from differentiating into chondrocytes. Dev. Cell. 2005, 8, 727–738. [Google Scholar] [CrossRef] [PubMed]
- Hoeppner, L.H.; Secreto, F.J.; Westendorf, J.J. Wnt signaling as a therapeutic target for bone diseases. Expert. Opin. Ther. Targets 2009, 13, 485–496. [Google Scholar] [CrossRef]
- Komatsu, D.E.; Mary, M.N.; Schroeder, R.J.; Robling, A.G.; Turner, C.H.; Warden, S.J. Modulation of Wnt signaling influences fracture repair. J. Orthop. Res. 2010, 28, 928–936. [Google Scholar] [CrossRef] [PubMed]
- Zhang, R.; Oyajobi, B.O.; Harris, S.E.; Chen, D.; Tsao, C.; Deng, H.W.; Zhao, M. Wnt/β-catenin signaling activates bone morphogenetic protein 2 expression in osteoblasts. Bone 2013, 52, 145–156. [Google Scholar] [CrossRef]
- Baron, R.; Kneissel, M. WNT signaling in bone homeostasis and disease: From human mutations to treatments. Nat. Med. 2013, 19, 179–192. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Zhang, Y.; Kang, H.; Liu, W.; Liu, P.; Zhang, J.; Harris, S.E.; Wu, D. Sclerostin binds to LRP5/6 and antagonizes canonical Wnt signaling. J. Biol. Chem. 2005, 280, 19883–19887. [Google Scholar] [CrossRef]
- Sutherland, M.K.; Geoghegan, J.C.; Yu, C.; Turcott, E.; Skonier, J.E.; Winkler, D.G.; Latham, J.A. Sclerostin promotes the apoptosis of human osteoblastic cells: A novel regulation of bone formation. Bone 2004, 35, 828–835. [Google Scholar] [CrossRef]
- Khosla, S.; Westendorf, J.J.; Oursler, M.J. Building bone to reverse osteoporosis and repair fractures. J. Clin. Investig. 2008, 118, 421–428. [Google Scholar] [CrossRef]
- Eyaid, W.; Al-Qattan, M.M.; Al Abdulkareem, I.; Fetaini, N.; Al Balwi, M. A novel homozygous missense mutation (c.610G>A, p.Gly204Ser) in the WNT7A gene causes tetra-amelia in two Saudi families. Am. J. Med. Genet. A 2011, 155, 599–604. [Google Scholar] [CrossRef]
- Johnson, M.L. LRP5 and bone mass regulation: Where are we now? Bonekey Rep. 2012, 1, 1. [Google Scholar] [CrossRef]
- Niemann, S.; Zhao, C.; Pascu, F.; Stahl, U.; Aulepp, U.; Niswander, L.; Weber, J.L.; Müller, U. Homozygous WNT3 mutation causes tetra-amelia in a large consanguineous family. Am. J. Hum. Genet. 2004, 74, 558–563. [Google Scholar] [CrossRef]
- Parr, B.A.; McMahon, A.P. Dorsalizing signal Wnt-7a required for normal polarity of D-V and A-P axes of mouse limb. Nature 1995, 374, 350–353. [Google Scholar] [CrossRef]
- Kramer, I.; Loots, G.G.; Studer, A.; Keller, H.; Kneissel, M. Parathyroid hormone (PTH)-induced bone gain is blunted in SOST overexpressing and deficient mice. J. Bone Miner. Res. 2010, 25, 178–189. [Google Scholar] [CrossRef] [PubMed]
- Sun, M.; Chen, Z.; Wu, X.; Yu, Y.; Wang, L.; Lu, A.; Zhang, G.; Li, F. The Roles of Sclerostin in Immune System and the Applications of Aptamers in Immune-Related Research. Front. Immunol. 2021, 12, 602330. [Google Scholar] [CrossRef] [PubMed]
- Shirazi, S.; Ravindran, S.; Cooper, L.F. Topography-mediated immunomodulation in osseointegration; Ally or Enemy. Biomaterials 2022, 291, 121903. [Google Scholar] [CrossRef]
- Gooi, J.H.; Pompolo, S.; Karsdal, M.A.; Kulkarni, N.H.; Kalajzic, I.; McAhren, S.H.; Han, B.; Onyia, J.E.; Ho, P.W.M.; Gillespie, M.T.; et al. Calcitonin impairs the anabolic effect of PTH in young rats and stimulates expression of sclerostin by osteocytes. Bone 2010, 46, 1486–1497. [Google Scholar] [CrossRef]
- Bellido, T.; Ali, A.A.; Gubrij, I.; Plotkin, L.I.; Fu, Q.; O’Brien, C.A.; Manolagas, S.C.; Jilka, R.L. Chronic elevation of parathyroid hormone in mice reduces expression of sclerostin by osteocytes: A novel mechanism for hormonal control of osteoblastogenesis. Endocrinology 2005, 146, 4577–4583. [Google Scholar] [CrossRef] [PubMed]
- Bellido, T.; Saini, V.; Pajevic, P.D. Effects of PTH on osteocyte function. Bone 2013, 54, 250–257. [Google Scholar] [CrossRef]
- Robling, A.G.; Niziolek, P.J.; Baldridge, L.A.; Condon, K.W.; Allen, M.R.; Alam, I.; Mantila, S.M.; Gluhak-Heinrich, J.; Bellido, T.M.; Harris, S.E.; et al. Mechanical stimulation of bone in vivo reduces osteocyte expression of Sost/sclerostin. J. Biol. Chem. 2008, 283, 5866–5875. [Google Scholar] [CrossRef] [PubMed]
- Genetos, D.C.; Yellowley, C.E.; Loots, G.G. Prostaglandin E2 signals through PTGER2 to regulate sclerostin expression. PLoS ONE 2011, 6, e17772. [Google Scholar] [CrossRef]
- Walker, E.C.; McGregor, N.E.; Poulton, I.J.; Solano, M.; Pompolo, S.; Fernandes, T.J.; Constable, M.J.; Nicholson, G.C.; Zhang, J.-G.; Nicola, N.A.; et al. Oncostatin M promotes bone formation independently of resorption when signaling through leukemia inhibitory factor receptor in mice. J. Clin. Investig. 2010, 120, 582–592. [Google Scholar] [CrossRef]
- Ke, H.Z.; Richards, W.G.; Li, X.; Ominsky, M.S. Sclerostin and Dickkopf-1 as therapeutic targets in bone diseases. Endocr. Rev. 2012, 33, 747–783. [Google Scholar] [CrossRef]
- McDonald, M.M.; Morse, A.; Mikulec, K.; Peacock, L.; Yu, N.; Baldock, P.A.; Birke, O.; Liu, M.; Ke, H.Z.; Little, D.G. Inhibition of sclerostin by systemic treatment with sclerostin antibody enhances healing of proximal tibial defects in ovariectomized rats. J. Orthop. Res. 2012, 30, 1541–1548. [Google Scholar] [CrossRef]
- Tian, X.; Jee, W.S.; Li, X.; Paszty, C.; Ke, H.Z. Sclerostin antibody increases bone mass by stimulating bone formation and inhibiting bone resorption in a hindlimb-immobilization rat model. Bone 2011, 48, 197–201. [Google Scholar] [CrossRef]
- Virdi, A.S.; Irish, J.; Sena, K.; Liu, M.; Ke, H.Z.; McNulty, M.A.; Sumner, D.R. Sclerostin antibody treatment improves implant fixation in a model of severe osteoporosis. J. Bone Jt. Surg. Am. 2015, 97, 133–140. [Google Scholar] [CrossRef]
- Li, X.; Ominsky, M.S.; Warmington, K.S.; Morony, S.; Gong, J.; Cao, J.; Gao, Y.; Shalhoub, V.; Tipton, B.; Haldankar, R.; et al. Sclerostin antibody treatment increases bone formation, bone mass, and bone strength in a rat model of postmenopausal osteoporosis. J. Bone Miner. Res. 2009, 24, 578–588. [Google Scholar] [CrossRef]
- Padhi, D.; Jang, G.; Stouch, B.; Fang, L.; Posvar, E. Single-dose, placebo-controlled, randomized study of AMG 785, a sclerostin monoclonal antibody. J. Bone Miner. Res. 2011, 26, 19–26. [Google Scholar] [CrossRef]
- Li, X.; Warmington, K.S.; Niu, Q.T.; Asuncion, F.J.; Barrero, M.; Grisanti, M.; Dwyer, D.; Stouch, B.; Thway, T.M.; Stolina, M.; et al. Inhibition of sclerostin by monoclonal antibody increases bone formation, bone mass, and bone strength in aged male rats. J. Bone Miner. Res. 2010, 25, 2647–2656. [Google Scholar] [CrossRef]
- Virdi, A.S.; Liu, M.; Sena, K.; Maletich, J.; McNulty, M.; Ke, H.Z.; Sumner, D.R. Sclerostin antibody increases bone volume and enhances implant fixation in a rat model. J. Bone Jt. Surg. Am. 2012, 94, 1670–1680. [Google Scholar] [CrossRef]
- Yu, S.H.; Hao, J.; Fretwurst, T.; Liu, M.; Kostenuik, P.; Giannobile, W.V.; Jin, Q. Sclerostin-Neutralizing Antibody Enhances Bone Regeneration Around Oral Implants. Tissue Eng. Part. A 2018, 24, 1672–1679. [Google Scholar] [CrossRef] [PubMed]
- McClung, M.R.; Grauer, A.; Boonen, S.; Bolognese, M.A.; Brown, J.P.; Diez-Perez, A.; Langdahl, B.L.; Reginster, J.-Y.; Zanchetta, J.R.; Wasserman, S.M.; et al. Romosozumab in postmenopausal women with low bone mineral density. N. Engl. J. Med. 2014, 370, 412–420. [Google Scholar] [CrossRef]
- McColm, J.; Hu, L.; Womack, T.; Tang, C.C.; Chiang, A.Y. Single- and multiple-dose randomized studies of blosozumab, a monoclonal antibody against sclerostin, in healthy postmenopausal women. J. Bone Miner. Res. 2014, 29, 935–943. [Google Scholar] [CrossRef]
- Padhi, D.; Allison, M.; Kivitz, A.J.; Gutierrez, M.J.; Stouch, B.; Wang, C.; Jang, G. Multiple doses of sclerostin antibody romosozumab in healthy men and postmenopausal women with low bone mass: A randomized, double-blind, placebo-controlled study. J. Clin. Pharmacol. 2014, 54, 168–178. [Google Scholar] [CrossRef]
- Yao, Y.; Kauffmann, F.; Maekawa, S.; Sarment, L.V.; Sugai, J.V.; Schmiedeler, C.A.; Doherty, E.J.; Holdsworth, G.; Kostenuik, P.J.; Giannobile, W.V. Sclerostin antibody stimulates periodontal regeneration in large alveolar bone defects. Sci. Rep. 2020, 10, 16217. [Google Scholar] [CrossRef]
- Martins, B.G.S.; Fernandes, J.C.H.; Martins, A.G.; Castilho, R.M.; Fernandes, G.V.O. Surgical and Nonsurgical Treatment Protocols for Peri-implantitis: An Overview of Systematic Reviews. Int. J. Oral Maxillofac. Implant. 2022, 37, 660–676. [Google Scholar] [CrossRef]
- Borges, H.; Correia, A.R.M.; Castilho, R.M.; Fernandes, G.V.O. Zirconia Implants and Marginal Bone Loss: A Systematic Review and Meta-Analysis of Clinical Studies. Int. J. Oral Maxillofac. Implant. 2020, 35, 707–720. [Google Scholar] [CrossRef]
- Fernandes, G.V.O.; Costa, B.M.G.N.; Trindade, H.F.; Castilho, R.M.; Fernandes, J.C.H. Comparative analysis between extra-short implants (≤6 mm) and 6 mm-longer implants: A meta-analysis of randomized controlled trial. Aust. Dent. J. 2022, 67, 194–211. [Google Scholar] [CrossRef]
- Wittneben, J.G.; Buser, D.; Salvi, G.E.; Bürgin, W.; Hicklin, S.; Brägger, U. Complication and failure rates with implant-supported fixed dental prostheses and single crowns: A 10-year retrospective study. Clin. Implant Dent. Relat. Res. 2014, 16, 356–364. [Google Scholar] [CrossRef]
- Howe, M.S.; Keys, W.; Richards, D. Long-term (10-year) dental implant survival: A systematic review and sensitivity meta-analysis. J. Dent. 2019, 84, 9–21. [Google Scholar] [CrossRef]
- Barfeie, A.; Wilson, J.; Rees, J. Implant surface characteristics and their effect on osseointegration. Br. Dent. J. 2015, 218, E9. [Google Scholar] [CrossRef]
- Vohra, F.; Al-Rifaiy, M.Q.; Almas, K.; Javed, F. Efficacy of systemic bisphosphonate delivery on osseointegration of implants under osteoporotic conditions: Lessons from animal studies. Arch. Oral Biol. 2014, 59, 912–920. [Google Scholar] [CrossRef]
- Mohan, S.; Baylink, D.J. Evidence that the inhibition of TE85 human bone cell proliferation by agents which stimulate cAMP production may in part be mediated by changes in the IGF-II regulatory system. Growth Regul. 1991, 1, 110–118. [Google Scholar]
- Gabet, Y.; Müller, R.; Levy, J.; Dimarchi, R.; Chorev, M.; Bab, I.; Kohavi, D. Parathyroid hormone 1–34 enhances titanium implant anchorage in low-density trabecular bone: A correlative micro-computed tomographic and biomechanical analysis. Bone 2006, 39, 276–282. [Google Scholar] [CrossRef]
- Le Guéhennec, L.; Soueidan, A.; Layrolle, P.; Amouriq, Y. Surface treatments of titanium dental implants for rapid osseointegration. Dent. Mater. 2007, 23, 844–854. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Ann. Intern. Med. 2009, 151, 264–269, w64. [Google Scholar] [CrossRef]
- Schardt, C.; Adams, M.B.; Owens, T.; Keitz, S.; Fontelo, P. Utilization of the PICO framework to improve searching PubMed for clinical questions. BMC Med. Inform. Decis. Mak. 2007, 7, 16. [Google Scholar] [CrossRef]
- Korn, P.; Kramer, I.; Schlottig, F.; Tödtman, N.; Eckelt, U.; Bürki, A.; Ferguson, S.J.; Kautz, A.; Schnabelrauch, M.; Range, U.; et al. Systemic sclerostin antibody treatment increases osseointegration and biomechanical competence of zoledronic-acid-coated dental implants in a rat osteoporosis model. Eur Cell Mater. 2019, 37, 333–346. [Google Scholar] [CrossRef]
- Liu, M.; Kurimoto, P.; Zhang, J.; Niu, Q.T.; Stolina, M.; Dechow, P.C.; Feng, J.Q.; Hesterman, J.; Silva, M.D.; Ominsky, M.S.; et al. Sclerostin and DKK1 Inhibition Preserves and Augments Alveolar Bone Volume and Architecture in Rats with Alveolar Bone Loss. J. Dent. Res. 2018, 97, 1031–1038. [Google Scholar] [CrossRef]
- Wu, J.; Cai, X.H.; Qin, X.X.; Liu, Y.X. The effects of sclerostin antibody plus parathyroid hormone (1–34) on bone formation in ovariectomized rats. Z Gerontol. Geriatr. 2018, 51, 550–556. [Google Scholar] [CrossRef]
- Taut, A.D.; Jin, Q.; Chung, J.H.; Galindo-Moreno, P.; Yi, E.S.; Sugai, J.V.; Ke, H.Z.; Liu, M.; Giannobile, W.V. Sclerostin antibody stimulates bone regeneration after experimental periodontitis. J. Bone Miner. Res. 2013, 28, 2347–2356. [Google Scholar] [CrossRef]
- Virk, M.S.; Alaee, F.; Tang, H.; Ominsky, M.S.; Ke, H.Z.; Lieberman, J.R. Systemic administration of sclerostin antibody enhances bone repair in a critical-sized femoral defect in a rat model. J. Bone Jt. Surg. Am. 2013, 95, 694–701. [Google Scholar] [CrossRef]
- Liu, S.; Virdi, A.S.; Sena, K.; Sumner, D.R. Sclerostin antibody prevents particle-induced implant loosening by stimulating bone formation and inhibiting bone resorption in a rat model. Arthritis Rheum. 2012, 64, 4012–4020. [Google Scholar] [CrossRef]
- Ominsky, M.S.; Li, C.; Li, X.; Tan, H.L.; Lee, E.; Barrero, M.; Asuncion, F.J.; Dwyer, D.; Han, C.-Y.; Vlasseros, F.; et al. Inhibition of sclerostin by monoclonal antibody enhances bone healing and improves bone density and strength of nonfractured bones. J. Bone Miner. Res. 2011, 26, 1012–1021. [Google Scholar] [CrossRef] [PubMed]
- Agholme, F.; Li, X.; Isaksson, H.; Ke, H.Z.; Aspenberg, P. Sclerostin antibody treatment enhances metaphyseal bone healing in rats. J. Bone Miner. Res. 2010, 25, 2412–2418. [Google Scholar] [CrossRef]
- Ominsky, M.S.; Vlasseros, F.; Jolette, J.; Smith, S.Y.; Stouch, B.; Doellgast, G.; Gong, J.; Gao, Y.; Cao, J.; Graham, K.; et al. Two doses of sclerostin antibody in cynomolgus monkeys increases bone formation, bone mineral density, and bone strength. J. Bone Miner. Res. 2010, 25, 948–959. [Google Scholar] [CrossRef]
- Tian, X.; Setterberg, R.B.; Li, X.; Paszty, C.; Ke, H.Z.; Jee, W.S. Treatment with a sclerostin antibody increases cancellous bone formation and bone mass regardless of marrow composition in adult female rats. Bone 2010, 47, 529–533. [Google Scholar] [CrossRef]
- Saag, K.G.; Petersen, J.; Brandi, M.L.; Karaplis, A.C.; Lorentzon, M.; Thomas, T.; Maddox, J.; Fan, M.; Meisner, P.D.; Grauer, A. Romosozumab or Alendronate for Fracture Prevention in Women with Osteoporosis. N. Engl. J. Med. 2017, 377, 1417–1427. [Google Scholar] [CrossRef]
- Fabre, S.; Funck-Brentano, T.; Cohen-Solal, M. Anti-Sclerostin Antibodies in Osteoporosis and Other Bone Diseases. J. Clin. Med. 2020, 9, 3439. [Google Scholar] [CrossRef]


{kind=link}
| Author | Year | Country (Study) | Study Center | Study Type | Species | Sample Size (Initial) | Sample Size (Final) | Age (Mean) | Gender | ||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Korn et al. [57] | 2019 | Switzerland | Basel-Stadt Cantonal Veterinary Office | Animal | Wistar rats | 128 | 124 | 6-month-old | female | ||
| Liu et al. [58] | 2018 | USA | - | Animal | Sprague-Dawley rats | 50 | 40 OVX a | 50 | 40 OVX a | 6-month-old | female |
| 10 Sham b | 10 Sham b | ||||||||||
| Sprague-Dawley rats | 45 | 45 | 8-month-old | male | |||||||
| Wu et al. [59] | 2018 | China | - | Animal | Sprague-Dawley rats | 50 | 5 Sham | 40 OVX | 3-month-old | female | |
| 5 OVX | |||||||||||
| 40 OVX | |||||||||||
| Yu et al. [40] | 2018 | USA | University of Michigan | Animal | Sprague-Dawley rats | 60 | 60 | 8-month-old | male | ||
| Virdi et al. [35] | 2015 | USA | - | Animal | Sprague-Dawley rats | 144 | 72 OVX a | 142 | 71 OVX a | 4.5-month-old | female |
| 72 Sham b | 71 Sham b | ||||||||||
| Taut et al. [60] | 2013 | USA | - | Animal | Sprague-Dawley rats | 69 | 69 | 9–10-week-old | male | ||
| Virk et al. [61] | 2013 | USA | University of Connecticut Health Center | Animal | Lewis rats | 72 | 72 | 14-week-old | male | ||
| Lewis rats | 30 | 30 | 14-week-old | male | |||||||
| Liu et al. [62] | 2012 | USA | - | Animal | Sprague-Dawley rats | 36 | 36 | - | male | ||
| McDonald et al. [33] | 2012 | Australia | - | Animal | Sprague-Dawley rats | 132 | 66 Sham b | 127 | - | female | |
| 66 OVX a | |||||||||||
| Virdi et al. [39] | 2012 | USA | - | Animal | Sprague-Dawley rats | 90 | 88 | 6-month-old | male | ||
| Ominsky et al. [63] | 2011 | Canada | Charles River Laboratories | Animal | Sprague-Dawley rats | 35 | 32 | 7–7.5-month-old | male | ||
| Cynomolgus monkeys | 43 | 29 | 4–5 years old | male | |||||||
| Tian et al. [34] | 2011 | USA | University of Utah | Animal | Sprague-Dawley rats | 67 | 67 | 10-month-old | female | ||
| Agholme et al. [64] | 2010 | Sweden | - | Animal | Sprague-Dawley rats | 68 | 64 | 10-month-old | male | ||
| Li et al. [38] | 2010 | USA | - | Animal | Sprague-Dawley rats | 28 | 26 | 16-month-old | male | ||
| Ominsky et al. [65] | 2010 | Canada | Charles River Laboratories | Animal | Cynomolgus monkeys | 12 | 12 | 3–5 years old | female | ||
| Tian et al. [66] | 2010 | USA | University of Utah | Animal | Sprague-Dawley rats | 32 | 32 | 10-month-old | female | ||
| Saag et al. [67] | 2017 | - | Multicenter international | RCT, ph.3 c | Human | 4093 | 3150 | 55–90 years old | women | ||
| McClung et al. [41] | 2014 | - | Multicenter international (28 centers) | RCT, ph.2 d | Human | 419 | 383 | 55–89 years old | women | ||
| Padhi et al. [43] | 2014 | USA | 4 centers | RCT e | Human | 48 | 32 women | 46 | 31 women | 45–80 years old | Postmenopausal women & men |
| 16 men | 15 men | ||||||||||
| Sample Size (Initial) | Sample Size (Final) | Control | Drug (Name) | Administration Route | Dosage (Unit) | Period of Treatment | Implant | |||
|---|---|---|---|---|---|---|---|---|---|---|
| Korn et al. (2019) [57] | 128 | 124 | non antibody applied | sclerostin antibody | intravenous | 100 mg/kg once week | 2 or 4 weeks | Reference-coated implant | ||
| ZOL-coated implant | ||||||||||
| Liu et al. (2018) [58] | 50 | 40 OVX | 50 | 40 OVX | saline solution | Scl-Ab VI | subcutaneous | 18.2 mg/kg twice week | 5 weeks | not placed |
| Scl-Ab VI + DAB d | 18.1 mg/kg + 18.1 mg/kg twice week | |||||||||
| 10 Sham | 10 Sham | - | - | |||||||
| 45 | 45 | saline solution | Scl-Ab VI | subcutaneous | 25 mg/kg twice week | 15 weeks | not placed | |||
| Scl-Ab VI + DAB d | 25 mg/kg + 25 mg/kg twice week | |||||||||
| Wu et al. (2018) [59] | 50 | 5 Sham | - | - | - | - | - | - | - | |
| 5 OVX | - | - | - | - | - | - | - | |||
| 40 OVX | 40 OVX | vehicle | Scl-Ab e | subcutaneous | 25 mg/kg twice week | 12 weeks | not placed | |||
| PTH 1-34 f | 60 μg/kg thrice week | |||||||||
| Scl-Ab e + PTH 1-34 f | 25 mg/kg twice week + 60 μg/kg thrice week | |||||||||
| Yu et al. (2018) [40] | 60 | 60 | PBS a | Scl-Ab | subcutaneous | 25 mg/kg | 10, 14 or 28 days | cp-Ti, solid cylinder with titanium plasma-sprayed surface implant | ||
| Virdi et al. (2015) [35] | 144 | 72 OVX | 142 | 71 OVX | vehicle | Scl-Ab III g | subcutaneous | 25 mg/kg twice week | 4, 8 or 12 weeks | cp-Ti with dual acid-etched surface implant |
| 72 Sham | 71 Sham | |||||||||
| Taut et al. (2013) [60] | 69 | 69 | EP b: vehicle healthy: PBS | EP b: Scl-Ab III g | subcutaneous | 25 mg/kg twice week | 3 or 6 weeks | not placed | ||
| locally | 15 μL of 35.6 mg/mL solution m twice week | |||||||||
| Virk et al. (2013) [61] | 72 | 72 | PBS a | Scl-Ab III g | subcutaneous | 25 mg/kg twice week | 0–12 weeks n | not placed | ||
| 0–2 weeks o | ||||||||||
| 2–4 weeks p | ||||||||||
| 30 | 30 | PBS a | Scl-Ab III g | - | 25 mg/kg | 12 weeks | not placed | |||
| Liu et al. (2012) [62] | 36 | 36 | particle vehicle + antibody vehicle | PE suspension h + antibody vehicle | intraarticular + subcutaneous | 50 μL once week + vehicle twice week | 12 weeks | titanium rods, dual acid-etched surface | ||
| PE suspension h + Scl-Ab III g | 50 µL once week + 25 mg/kg twice week | |||||||||
| McDonald et al. (2012) [33] | 132 | 66 Sham | 127 | saline solution | Scl-Ab III g | subcutaneous | 25 mg/kg twice week | 1, 2 or 3 weeks | not placed | |
| 66 OVX | ||||||||||
| Virdi et al. (2012) [39] | 90 | 88 | saline solution | Scl-Ab i | subcutaneous | 25 mg/kg | 2, 4 or 8 weeks | cp-Ti with dual acid-etched surface implant | ||
| Ominsky et al. (2011) [63] | 35 | 32 | vehicle | Scl-Ab III g | subcutaneous | 25 mg/kg twice week | 7 weeks | not placed | ||
| 43 | 29 | vehicle | Scl-Ab V j | subcutaneous | 30 mg/kg every 2 weeks | 10 weeks | stainless steel K-wire | |||
| Tian et al. (2011) [34] | 67 | 67 | saline solution | Scl-Ab III g | subcutaneous | 5 mg/kg twice week | 4 weeks | not placed | ||
| 25 mg/kg twice week | ||||||||||
| Agholme et al. (2010) [64] | 68 | 64 | saline solution | Scl-Ab III g | subcutaneous | 25 mg/kg twice weeks | 2 or 4 weeks | stainless steel screws (mechanical tests); PMMA screws (μCT) | ||
| Li et al. (2010) [38] | 28 | 26 | vehicle | Scl-Ab III g | subcutaneous | 25 mg/kg twice week | 5 weeks | not placed | ||
| 5 mg/kg twice week | ||||||||||
| Ominsky et al. (2010) [65] | 12 | 12 | vehicle | Scl-Ab IV k | subcutaneous | 3 mg/kg once month | 29 days | not placed | ||
| 10 mg/kg once month | ||||||||||
| 30 mg/kg once month | ||||||||||
| Tian et al. (2010) [66] | 32 | 32 | saline solution | Scl-Ab III g | subcutaneous | 5 mg/kg twice week | 4 weeks | not placed | ||
| 25 mg/kg twice week | ||||||||||
| Saag et al. (2017) [67] | 4093 | 3150 | Alendronate c → alendronate c | Romosozumab l → alendronate c | subcutaneous → oral | 210 mg once month → 70 mg once week | 0-12 months q → 12–36 months r | not placed | ||
| McClung et al. (2014) [41] | 419 | 383 | placebo | romosozumab | subcutaneous | 140 mg every 3 months | 12 months | not placed | ||
| 210 mg every 3 months | ||||||||||
| 70 mg once month | ||||||||||
| 140 mg once month | ||||||||||
| 210 mg once month | ||||||||||
| alendronate | oral | 70 mg once week | ||||||||
| teriparatide | subcutaneous | 20 μg once day | ||||||||
| Padhi et al. (2014) [43] | 48 | 32 women | 46 | 31 women | placebo | romosozumab | subcutaneous | 1 mg/kg every 2 weeks | 12 weeks | not placed |
| 2 mg/kg every 4 weeks | ||||||||||
| 2 mg/kg every 2 weeks | ||||||||||
| 3 mg/kg every 4 weeks | ||||||||||
| 16 men | 15 men | romosozumab | subcutaneous | 1 mg/kg every 2 weeks | ||||||
| 3 mg/kg every 4 weeks | ||||||||||
| Saag et al. (2017) [67] | McClung et al. (2014) [41] | Padhi et al. (2014) [43] | |||||||||||||||||
| Drug/Control | Double-Blind Period | Primary Analysis Period | Placebo | Alendronate | Teraparatide | Romosozumab | Placebo | Romosozumab | |||||||||||
| Alendronate → Alendronate | Romosozumab → Alendronate | Alendronate → Alendronate | Romosozumab → Alendronate | Women | Men | ||||||||||||||
| Dosage (unit) | 70 mg → 70 mg once week | 210 mg once month → 70 mg once week | 70 mg → 70mg once week | 210 mg once month → 70 mg once week | - | 70 mg once week | 20 μg once day | 140 mg every 3 moths | 210 mg every 3 months | 70 mg once month | 140 mg once month | 210 mg once month | - | 1 mg/kg every 2 weeks | 2 mg/kg every 4 weeks | 2 mg/kg every 2 weeks | 3 mg/kg every 4 weeks | 1 mg/kg every 2 weeks | 3 mg/kg every 4 weeks |
| Number of participants | 2014 | 2040 | 2014 | 2040 | 50 | 51 | 54 | 53 | 53 | 50 | 48 | 51 | 12 | 6 | 6 | 6 | 6 | 6 | 6 |
| Adverse Events | 1584 (78.6%) | 1544 (75.7%) | 1784 (88.6%) | 1766 (86.6%) | 45 (90%) | 44 (86.3%) | 37 (68.5%) | 43 (81.1%) | 46 (86.8%) | 48 (96%) | 42 (87.5%) | 42 (87.4%) | 10 (83%) | 6 (100%) | 6 (100%) | 6 (100%) | 5 (83%) | 5 (83%) | 5 (83%) |
| Headache | - | - | - | - | 8 (16%) | 4 (7.8%) | 3 (5.6%) | 7 (13.2%) | 3 (5.7%) | 4 (8.0%) | 3 (6.3%) | 5 (9.8%) | 4 (33%) | 1 (17%) | 1 (17%) | 1 (17%) | 2 (33%) | 3 (50%) | 2 (33%) |
| Upper respiratory tract infection | - | - | - | - | - | - | - | - | - | - | - | - | 1 (8%) | 3 (50%) | 1 (17%) | 2 (33%) | 0 | 2 (33%) | 0 |
| Arthralgia | - | - | - | - | 4 (8%) | 5 (9.8%) | 5 (9.3%) | 19 (17%) | 5 (9.4%) | 8 (16%) | 6 (12.5%) | 3 (5.9%) | 2 (17%) | 0 | 2 (33%) | 0 | 1 (17%) | 1 (17%) | 1 (17%) |
| Pain in Extremity | - | - | - | - | 2 (4%) | 2 (3.9%) | 5 (9.3%) | 7 (13.2%) | 3 (5.7%) | 10 (20%) | 5 (10.4%) | 6 (11.8%) | 2 (17%) | 0 | 2 (33%) | 0 | 1 (17%) | 0 | 1 (17%) |
| Abdominal pain | - | - | - | - | - | - | - | - | - | - | - | - | 1 (8%) | 0 | 1 (17%) | 1 (17%) | 0 | 1 (17%) | 0 |
| Back pain | 228 (11.3%) | 186 (9.1%) | 393 (19.5%) | 329 (16.1%) | 3 (6.0%) | 5 (9.8%) | 3 (5.6%) | 4 (7.5%) | 7 (13.2%) | 5 (10%) | 7 (14.6%) | 3 (5.9%) | 2 (17%) | 3 (50%) | 0 | 0 | 0 | 0 | 0 |
| Injection site pain | - | - | - | - | 0 | 0 | 0 | 2 (3.8%) | 4 (7.5%) | 3 (6%) | 4 (8.3%) | 3 (5.9%) | 0 | 0 | 0 | 2 (33%) | 0 | 1 (17%) | 0 |
| Injection site reaction | 53 (2.6%) | 90 (4.4%) | 53 (2.6%) | 90 (4.4%) | - | - | - | - | - | - | - | - | 0 | 0 | 0 | 1 (17%) | 1 (17%) | 0 | 1 (17%) |
| Lymphadenopathy | - | - | - | - | - | - | - | - | - | - | - | - | 0 | 1 (17%) | 0 | 1 (17%) | 1 (17%) | 0 | 0 |
| Nasopharyngitis | 218 (10.8%) | 213 (10.4%) | 373 (18.5%) | 363 (17.8%) | 7 (14%) | 3 (5.9%) | 4 (7.4%) | 10 (18.9%) | 5 (9.4%) | 19 (38.0%) | 13 (27.1%) | 8 (15.7%) | - | - | - | - | - | - | - |
| Gastroenteritis | - | - | - | - | 3 (6%) | 2 (3.9%) | 1 (1.9%) | 2 (3.8%) | 5 (9.4%) | 3 (6%) | 4 (8.3%) | 8 (15.7%) | - | - | - | - | - | - | - |
| Cough | - | - | - | - | 2 (4%) | 4 (7.8%) | 0 | 3 (5.7%) | 1 (1.9%) | 8 (16%) | 4 (8.3%) | 4 (7.8%) | - | - | - | - | - | - | - |
| Constipation | - | - | - | - | 2 (4%) | 3 (5.9%) | 2 (3.7%) | 2 (3.8%) | 5 (9.4%) | 4 (8%) | 4 (8.3%) | 2 (3.9%) | - | - | - | - | - | - | - |
| Bronchitis | - | - | - | - | 2 (4%) | 1 (2%) | 2 (3.7%) | 5 (9.4%) | 1 (1.9%) | 5 (10%) | 3 (6.3%) | 2 (3.9%) | - | - | - | - | - | - | - |
| Urinary tract infection | - | - | - | - | 0 | 4 (7.8%) | 3 (5.6%) | 3 (5.7%) | 5 (9.4%) | 0 | 3 (6.3%) | 5 (9.8%) | - | - | - | - | - | - | - |
| Fatigue | - | - | - | - | 2 (4.0%) | 2 (3.9%) | 0 | 1 (1.9%) | 1 (1.9%) | 5 (10%) | 5 (10.4%) | 2 (3.9%) | - | - | - | - | - | - | - |
| Musculoskeletal pain | - | - | - | - | 2 (4.0%) | 2 (3.9%) | 2 (3.7%) | 3 (5.7%) | 3 (5.7%) | 4 (8%) | 2 (4.2%) | 1 (2%) | - | - | - | - | - | - | - |
| Adjudicated serious cardiovascular event | 38 (1.9%) | 50 (2.5%) | 122 (6.1%) | 133 (6.5%) | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - |
| Cardiac ischemic event | 6 (0.3%) | 16 (0.8%) | 20 (1.0%) | 30 (1.5%) | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - |
| Cerebrovascular event | 7 (0.3%) | 16 (0.8%) | 27 (1.3%) | 45 (2.2%) | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - |
| Heart failure | 8 (0.4%) | 4 (0.2%) | 23 (1.1%) | 12 (0.6%) | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - |
| Noncoronary revascularization | 5 (0.2%) | 3 (0.1%) | 10 (0.5%) | 6 (0.3%) | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - |
| Peripheral vascular ischemic event not requiring revascularization | 2 (<0.1%) | 0 | 5 (0.2%) | 2 (<0.1%) | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - |
| Osteoarthritis | 146 (7.2%) | 138 (6.8%) | 268 (13.3%) | 247 (12.2%) | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - |
| Hypersensitivity | 118 (5.9%) | 122 (6%) | 185 (9.2%) | 205 (10%) | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - |
| Cancer | 28 (1.4%) | 31 (1.5%) | 85 (4.2%) | 84 (4.1%) | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - |
| Hyperostosis | 12 (0.6%) | 2 (<0.1%) | 27 (1.3%) | 23 (1.1%) | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - |
| Hypocalcemia | 1 (<0.1%) | 1 (<0.1%) | 1 (<0.1%) | 4 (0.2%) | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - |
| Atypical femoral fracture | 0 | 0 | 4 (0.2%) | 2 (<0.1%) | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - |
| Osteonecrosis of the Jaw | 0 | 0 | 1 (<0.1%) | 1 (<0.1%) | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - |
| Serious adverse event | 278 (10.8%) | 262 (12.8%) | 605 (30.0%) | 586 (28.7%) | 7 (14%) | 4 (7.8%) | 5 (9.3%) | 4 (7.5%) | 2 (3.8%) | 5 (10%) | 1 (2.1%) | 5 (9.8%) | - | - | - | - | - | - | - |
| Fatal adverse events (Deaths) | 21 (1.0%) | 30 (1.5%) | 90 (4.5%) | 90 (4.4%) | 1 (2%) | 0 | 0 | 0 | 0 | 1 (2%) | 0 | 0 | - | - | - | - | - | - | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Couto, B.A.d.A.; Fernandes, J.C.H.; Saavedra-Silva, M.; Roca, H.; Castilho, R.M.; Fernandes, G.V.d.O. Antisclerostin Effect on Osseointegration and Bone Remodeling. J. Clin. Med. 2023, 12, 1294. https://doi.org/10.3390/jcm12041294
Couto BAdA, Fernandes JCH, Saavedra-Silva M, Roca H, Castilho RM, Fernandes GVdO. Antisclerostin Effect on Osseointegration and Bone Remodeling. Journal of Clinical Medicine. 2023; 12(4):1294. https://doi.org/10.3390/jcm12041294
Chicago/Turabian StyleCouto, Bárbara Alexandra do Amaral, Juliana Campos Hasse Fernandes, Mariana Saavedra-Silva, Hernan Roca, Rogério Moraes Castilho, and Gustavo Vicentis de Oliveira Fernandes. 2023. "Antisclerostin Effect on Osseointegration and Bone Remodeling" Journal of Clinical Medicine 12, no. 4: 1294. https://doi.org/10.3390/jcm12041294
APA StyleCouto, B. A. d. A., Fernandes, J. C. H., Saavedra-Silva, M., Roca, H., Castilho, R. M., & Fernandes, G. V. d. O. (2023). Antisclerostin Effect on Osseointegration and Bone Remodeling. Journal of Clinical Medicine, 12(4), 1294. https://doi.org/10.3390/jcm12041294