Abstract
Pancreatic neuroendocrine tumors, or pNETs, represent a rare and clinically heterogenous subset of pancreatic neoplasms. One such pNET, the insulinoma, is found to be malignant in just 4% of all insulinomas. Due to the exceedingly uncommon occurrence of these tumors, there is controversy regarding the optimal evidence-based management for these patients. We therefore report on a 70-year-old male patient admitted with 3 months of episodic confusion with concurrent hypoglycemia. The patient was found to have inappropriately elevated endogenous insulin levels during these episodes, and somatostatin-receptor subtype 2 selective imaging revealed a pancreatic mass metastatic to local lymph nodes, spleen, and the liver. Fine needle aspiration of pancreatic and liver lesions confirmed the diagnosis of a low grade pancreatic neuroendocrine tumor. Molecular analysis of tumor tissue revealed a novel mutational profile consistent with pNET. The patient was initiated on octreotide therapy. However, treatment with octreotide alone demonstrated limited efficacy in controlling the patient’s symptoms, prompting consideration of other therapies.
1. Introduction
The population incidence of neuroendocrine tumors has been steadily rising since the 1970s as compared to the relatively stagnant population incidence of all malignant neoplasms, per the National Cancer Institute’s Surveillance, Epidemiology, and End Results (SEER) database [1]. Of this increasing incidence of neuroendocrine tumors, the majority of the increase is attributable to localized NETs, as opposed to those with regional or distant metastases [1]. Neuroendocrine tumors may arise from many different tissues in the body and represent a heterogenous group. Aside from lung NETs, the most common subtypes of NETs are gastrointestinal in nature, including neoplasms arising from the luminal portion of the gastrointestinal (GI) tract as well as pancreatic endocrine cells [1]. Pancreatic neuroendocrine tumors (pNETs) are commonly subdivided into two groups: functioning and non-functioning tumors. Functioning pNETs are those which secrete biologically active peptide hormones and present with clinically typical symptoms. One such pNET, the insulinoma, presents with a composite of classic symptoms termed Whipple’s Triad: fasting hypoglycemia (glucose < 50 mg/dL), symptoms during the hypoglycemic episodes, and relief of symptoms with the administration of glucose [2]. Insulin release is tightly regulated under normal physiologic conditions. In the case of the insulinoma, however, the release of insulin becomes uncoupled from glucose metabolism, leading to a state of hyperinsulinemic hypoglycemia [3]. Recent advances in molecular genetics and radiologic imaging modalities have permitted further characterization of these pNETs [4]. We bring forward the case of a novel mutational profile in the malignant insulinoma of a 70-year-old male which will enhance the knowledge of the molecular landscape of pNETs, specifically of insulinomas.
2. Case
A 70-year-old male with a history of gastroesophageal reflux disease (GERD) presented for admission at the request of his endocrinologist for evaluation of recurrent hypoglycemic episodes. The patient was in his usual state of health until approximately 3 months prior to admission, when he began to develop episodes of sweating, generalized weakness, nausea, and confusion. These episodes became progressively more frequent and severe over the next three months, at which point the patient had such a severe episode of generalized weakness that his wife brought him to the local Emergency Department (ED), where he was found to have a blood glucose of 35 mg/dL. The patient was treated with a glucose load which resolved his symptoms, and he was discharged home with a glucometer and a recommendation to carry small snacks with him in case of symptomatic hypoglycemia. The patient’s wife recorded early morning glucose levels frequently around 40 mg/dL over the following month which coincided with episodes of confusion, diaphoresis, and generalized weakness. The patient began waking for night-time snacks to mitigate these episodes. At the recommendation of their endocrinologist, the patient was admitted to our institution for further assessment of these hypoglycemic episodes.
On admission, physical examination revealed a well-developed male in no acute distress without abnormal findings. All vital signs were stable and within normal limits. Labs were notable for a blood glucose of 116 mg/dL, aspartate aminotransferase (AST) of 51 units per liter (U/L), and otherwise unremarkable laboratory studies including serum levels for metanephrines, normetanephrines, parathyroid hormone (PTH), thyroid-stimulating hormone (TSH), cortisol, and prolactin. The patient underwent a planned 72-h fast to investigate for the presence of an insulinoma, given his history of Whipple’s Triad. Approximately 12 h after the fast began, the blood glucose level declined to 36 mg/dL and the patient experienced shakiness and demonstrated confusion, at which time relevant blood samples were obtained, with results displayed in Table 1.

Table 1.
Laboratory Evaluation at 12 Hours Fasted.
Recurrent hyperinsulinemic hypoglycemia has a broad range of possible differential diagnoses in the pediatric and adult patient population [5]. For instance, it may also be seen in autoimmune-mediated insulin release [6]; however, insulin autoantibody titers were negative in this patient. Surreptitious endogenous insulin administration was also considered, but C-peptide would have been discordantly lower than our measured level. A negative sulfonylurea urine panel also ruled out oral insulinogenic agents as the culprit. This patient’s proinsulin level was significantly higher than the upper limit of normal, particularly compared to the elevated insulin level. Markedly elevated proinsulin and an increased ratio of proinsulin-to-insulin has been associated with malignant insulinoma as opposed to benign insulinoma [7].
We next pursued cross-sectional imaging to help us distinguish between diffuse islet cell hyperplasia, which can cause a noninsulinoma pancreatogenous hypoglycemia syndrome (NIPHS), from an insulinoma [8]. Magnetic resonance imaging (MRI) of the abdomen (Figure 1A) revealed multiple liver masses, the largest of which was 7.6 by 5.2 cm (cm) in the right lobe, in addition to a 5.3 by 4.3 cm mass in the spleen, three masses in the pancreatic tail, and regional lymphadenopathy, with imaging characteristics typical for neuroendocrine tumors. These findings were highly concerning for the diagnosis of malignant insulinoma in the clinical context of hyperinsulinemic hypoglycemia.
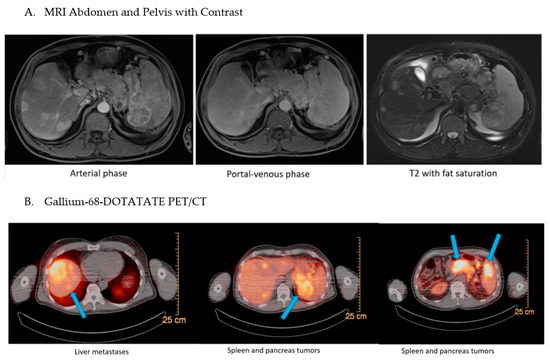
Figure 1.
Imaging Studies of the Abdomen and Pelvis. (A) For diagnostic purposes, MRI was obtained using gadolinium contrast. Representative images of three phases are shown as indicated. (B) The patient was subjected to a Gallium-68-DOTATATE PET/CT and several areas of high-intensity uptake are delineated by arrows in the series of cross-sections.
To assess for other metastatic lesions of neuroendocrine origin, the patient then underwent a 68-Gallium DOTATATE positron emission tomography/computed tomography (PET/CT) scan, which uses a radiopharmaceutical tracer that binds selectively to the somatostatin-receptor subtype 2 which is frequently expressed by pNETs [9]. The results, pictured in Figure 1B, showed highly increased uptake in the pancreas, multiple liver lesions, spleen, and intra-abdominal lymph nodes, which suggested in this clinical context that the masses identified on this molecular abdominal imaging likely represent metastatic malignancy of pancreatic origin.
The Gastroenterology service was consulted and an endoscopic ultrasound with fine-needle aspiration (FNA) of both a liver and pancreatic lesion was performed.
Smears and cell blocks were prepared from the fine needle aspiration sampling of both liver and pancreatic lesions. Papanicolaou (Pap) stained smears, as well as Hematoxylin and Eosin (H&E) stained cell block tissue sections were used for further examination. Cells from either liver or pancreas lesions share a similar cytomorphology and immunocytochemical profile. These single or loosely grouped lesional cells are relatively small and uniform in size with eccentrically located round or oval nuclei with finely stippled chromatin and moderate eosinophilic cytoplasm. Immunohistochemistry (IHC) studies revealed cells positive for pan-cytokeratin AE1/3 and neuroendocrine markers including CD56, synaptophysin, and chromogranin. However, cells were negative for beta-catenin, S100, and TTF-1. Proliferation rate as indicated by Ki67 was less than 3%. Mitotic count was less than 2 per 10 high power field. These findings suggested a well differentiated, low grade (G1) pancreatic neuroendocrine tumor (pNET) most consistent with malignant insulinoma. Selected cytopathology and IHC examinations are shown in Figure 2.
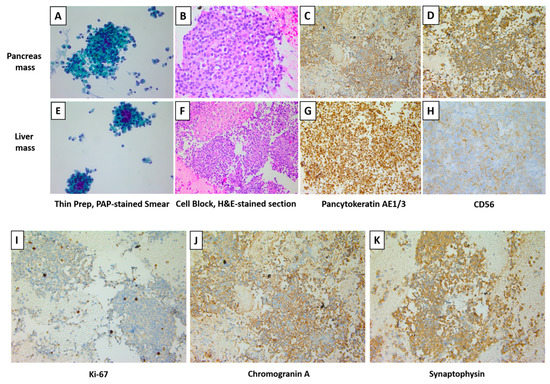
Figure 2.
The Cytomorphology, Immunocytochemical, and Biomarker profile of both Liver and Pancreas Lesions. Paraffin embedded cellblock material from fine needle aspiration of the pancreatic and liver masses. (A,E): Cellular aspirate of loosely cohesive clusters of cells and single cells (Papanicolaou stain). (B,F): Cell block tissue sections (H&E stain). (C,G): The cells are positive for pan-cytokeratin stain. (D,H): The cells are positive for neuroendocrine marker CD56. (I–K): Paraffin embedded cellblock material from fine needle aspiration of the pancreatic mass was subjected to immunohistochemistry staining for Ki-67, chromogranin A, and synaptophysin, all of which are positive. The original magnifications are as follows: ×400 (A), ×400 (B), ×200 (C), ×400 (D), ×400 (E), ×200 (F), ×200 (G), ×400 (H), ×400 (I), ×200 (J), and ×200 (K).
To further characterize this patient’s tumor, genomic sequencing was performed using FoundationOne®CDx (F1CDx; Supplementary Materials), which is summarized in Table 2.
Table 2.
Molecular Profiling of Liver Metastasis.
Initial therapy of hypoglycemic episodes included subcutaneous injections of octreotide (150 micrograms subcutaneously three times daily), a somatostatin analogue that suppresses insulin, growth hormone, and glucagon secretion. However, the monotherapy with octreotide failed to prevent the onset of hypoglycemia overnight while fasting in the few days following its initiation. The patient experienced ongoing labile blood glucose levels despite escalating doses of octreotide and the addition of diazoxide 50 mg twice daily as an adjunctive agent. The patient finally attained relief from overnight hypoglycemia (maintenance of blood glucose greater than 70 mg/dL for 8 h overnight) with a combination of octreotide 300 micrograms (mcg) subcutaneous injections three times daily, Diazoxide 100 mg twice daily, and ingestion of a slurry of cornstarch and cold water prior to bedtime. On discharge, octreotide was transitioned from three times daily dosing to a monthly depot injection of 20 mg. The patient’s treatment course was complicated by the development of lower extremity edema with the addition of diazoxide which was adequately managed with furosemide 40 mg daily. The patient was discharged in stable condition with a glucometer and outpatient follow up.
3. Discussion
The patient in our case was one of those approximately 1 to 3 per 10 million individuals found to have malignant insulinoma. The National Comprehensive Cancer Network’s 2020 guidelines recommend consideration of lanreotide or octreotide, somatostatin analogues, as treatment options for non-resectable, symptomatic, metastatic neuroendocrine tumors of the pancreas [10]. This guidance is based on the findings in the CLARINET and PROMID trials, both of which demonstrated improved progression-free survival with octreotide vs. placebo in midgut neuroendocrine tumors [11,12]. Considering this backdrop of compelling data for the use of octreotide in patients with tumors with robust concentration of SSR2 receptors, as identified in our patient, octreotide was initiated in this case. Unfortunately, the patient continued to struggle with hypoglycemic episodes despite octreotide dose escalation, which prompts consideration of other available treatment modalities. Given somatostatin analogues may also suppress secretion of glucagon, there is inconsistency in their effects on blood glucose levels. The North American Neuroendocrine Tumor Society (NANETS) 2020 Consensus Guidelines support 177Lu-DOTATATE Peptide Receptor Radionuclide Therapy (PRRT) for progressing pNET patients [13]. PRRT therapy utilizes Tyr3-octreotate (TATE) to bind to the SSR2 receptor and thereby deliver the attached radionuclide directly to the malignant cells. Small case series have shown this treatment to be effective in controlling hypoglycemic symptoms in patients with malignant insulinoma [14]. If our patient is deemed to progress in the outpatient setting clinically or radiographically, this data would support trialing PRRT therapy, in alignment with 2020 NCCN guidelines. In addition, everolimus, an mTOR inhibitor, has been reported effective in controlling insulin-induced hypoglycemia in malignant insulinomas refractory to somatostatin analogues, and could be considered in this patient [15,16].
Given the rarity of insulinoma, and particularly metastatic insulinoma, less is known about its genomic profile. In a study using whole-exome gene sequencing to compare the genomic profiles of 84 insulinomas with 127 non-functioning pNETs (NF-pNETs), Yin Yang 1 (YY1) mutations were unique to a minority of insulinomas (25%) and not noted in any NF-pNETs. YY1 is a transcription factor involved in various functions including cell growth and development. Mutation of the third zinc finger region of YY1 has been shown to alter its transcriptional activity, which promotes tumorigenesis in insulinoma [17]. Unfortunately, YY1 testing is not yet included in the comprehensive molecular panel for which this patient’s tumor tissue was submitted (Supplementary Materials). In contrast, the NF-pNET group contained frequent mutations in MEN1 (42%), DAXX (21%), ATRX (13%), and mTOR pathway genes (14%) [18]. Literature becomes even more sparse when narrowing focus to specifically malignant insulinomas. One group examined a cohort of 35 primary insulinomas which included five metastatic insulinomas. Of these, all five retained ATRX expression, while one had DAXX loss [19]. It was posited from these results that ATRX and DAXX mutations, which are typically more characteristic of NF-pNETs, may be more common in malignant insulinomas than in their less aggressive counterparts [19]. Groups sequencing larger cohorts including insulinomas have reported ATRX mutations in insulinoma very rarely [20]. Affirming these reports, the L2027R ATRX mutation noted in our patient affords additional credence to this suggestion that chromosomal instability from DAXX/ATRX mutations may represent an important genomic basis for the aggressive behavior of malignant insulinoma [19].
This patient’s tumor is the first malignant insulinoma to our knowledge to possess simultaneous mutations in ATRX, ROS1, and KMT2A. For other malignancies harboring these genomic alterations, additional investigation and trials of targeted therapeutics have yielded promising results. Innovation in novel therapeutics for insulinoma, particularly for the rare and high-mortality malignant insulinoma, will hinge on gathering and reporting molecular profiles such as this one (Supplementary Materials).
4. Conclusions
The diagnosis of a pancreatic neuroendocrine tumor requires a methodical approach with a keen focus on ruling out more common disease processes, particularly in the case of insulinoma. Given the rarity of insulinoma and the relatively recent advent of comprehensive molecular testing, there are few molecular profiles of insulinoma in the literature. We therefore present a novel mutational profile for consideration. Additional molecular data such as that reported here will be critical to achieving therapeutic advances for malignant insulinoma.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/jcm12041280/s1, Supplementary File S1: FoundationOne®CDx (F1CDx) Technical_Specifications; Supplementary File S2: Insulinoma clinical trials listed on ClinicalTrials.gov as of 11 June 2022.
Author Contributions
Conceptualization, H.C.W. and M.R.; formal analysis, H.X., B.N. and L.B.; writing—original draft preparation, L.B. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Informed Consent Statement
Informed consent for publication was obtained from the participant involved in the brief report.
Data Availability Statement
Not applicable.
Acknowledgments
The authors would like to acknowledge David L. Manuel, for providing radiographic images included in this manuscript as well as the patient for the permission to publish this report.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Dasari, A.; Shen, C.; Halperin, D.; Zhao, B.; Zhou, S.; Xu, Y.; Shih, T.; Yao, J.C. Trends in the Incidence, Prevalence, and Survival Outcomes in Patients with Neuroendocrine Tumors in the United States. JAMA Oncol. 2017, 3, 1335–1342. [Google Scholar] [CrossRef] [PubMed]
- von Eyben, F.E.; Grodum, E.; Gjessing, H.J.; Hagen, C.; Nielsen, H. Metabolic remission with octreotide in patients with insulinoma. J. Intern. Med. 1994, 235, 245–248. [Google Scholar] [CrossRef] [PubMed]
- Haris, B.; Saraswathi, S.; Hussain, K. Somatostatin analogues for the treatment of hyperinsulinaemic hypoglycaemia. Ther. Adv. Endocrinol. Metab. 2020, 11, 2042018820965068. [Google Scholar] [CrossRef] [PubMed]
- Nockel, P.; Babic, B.; Millo, C.; Herscovitch, P.; Patel, D.; Nilubol, N.; Sadowski, S.M.; Cochran, C.; Gorden, P.; Kebebew, E. Localization of Insulinoma Using 68Ga-DOTATATE PET/CT Scan. J. Clin. Endocrinol. Metab. 2017, 102, 195–199. [Google Scholar] [CrossRef] [PubMed]
- Shah, P.; Rahman, S.A.; Demirbilek, H.; Güemes, M.; Hussain, K. Hyperinsulinaemic hypoglycaemia in children and adults. Lancet Diabetes Endocrinol. 2017, 5, 729–742. [Google Scholar] [CrossRef] [PubMed]
- Censi, S.; Mian, C.; Betterle, C. Insulin autoimmune syndrome: From diagnosis to clinical management. Ann. Transl. Med. 2018, 6, 335. [Google Scholar] [CrossRef] [PubMed]
- Yu, R.; Nissen, N.N.; Hendifar, A.; Tang, L.; Song, Y.L.; Chen, Y.J.; Fan, X. A Clinicopathological Study of Malignant Insulinoma in a Contemporary Series. Pancreas 2017, 46, 48–56. [Google Scholar] [CrossRef] [PubMed]
- Williams, A.J.; Coates, P.J.; Lowe, D.G.; McLean, C.; Gale, E.A. Immunochemical investigation of insulinomas for islet amyloid polypeptide and insulin: Evidence for differential synthesis and storage. Histopathology 1992, 21, 215–223. [Google Scholar] [CrossRef] [PubMed]
- Lee, L.; Ito, T.; Jensen, R.T. Imaging of pancreatic neuroendocrine tumors: Recent advances, current status, and controversies. Expert. Rev. Anticancer Ther. 2018, 18, 837–860. [Google Scholar] [CrossRef] [PubMed]
- Network, N.C.C. Neuroendocrine Tumors. Symptoms Causes 2021, 3, 2021. [Google Scholar]
- Rinke, A.; Müller, H.H.; Schade-Brittinger, C.; Klose, K.J.; Barth, P.; Wied, M.; Mayer, C.; Aminossadati, B.; Pape, U.F.; Bläker, M.; et al. Placebo-controlled, double-blind, prospective, randomized study on the effect of octreotide LAR in the control of tumor growth in patients with metastatic neuroendocrine midgut tumors: A report from the PROMID Study Group. J. Clin. Oncol. 2009, 27, 4656–4663. [Google Scholar] [CrossRef] [PubMed]
- Rinke, A.; Wittenberg, M.; Schade-Brittinger, C.; Aminossadati, B.; Ronicke, E.; Gress, T.M.; Müller, H.H.; Arnold, R. Placebo-Controlled, Double-Blind, Prospective, Randomized Study on the Effect of Octreotide LAR in the Control of Tumor Growth in Patients with Metastatic Neuroendocrine Midgut Tumors (PROMID): Results of Long-Term Survival. Neuroendocrinology 2017, 104, 26–32. [Google Scholar] [CrossRef] [PubMed]
- Halfdanarson, T.R.; Strosberg, J.R.; Tang, L.; Bellizzi, A.M.; Bergsland, E.K.; O’Dorisio, T.M.; Halperin, D.M.; Fishbein, L.; Eads, J.; Hope, T.A.; et al. The North American Neuroendocrine Tumor Society Consensus Guidelines for Surveillance and Medical Management of Pancreatic Neuroendocrine Tumors. Pancreas 2020, 49, 863–881. [Google Scholar] [CrossRef] [PubMed]
- Magalhães, D.; Sampaio, I.L.; Ferreira, G.; Bogalho, P.; Martins-Branco, D.; Santos, R.; Duarte, H. Peptide receptor radionuclide therapy with (177)Lu-DOTA-TATE as a promising treatment of malignant insulinoma: A series of case reports and literature review. J. Endocrinol. Invest. 2019, 42, 249–260. [Google Scholar] [CrossRef] [PubMed]
- Baratelli, C.; Brizzi, M.P.; Tampellini, M.; Scagliotti, G.V.; Priola, A.; Terzolo, M.; Pia, A.; Berruti, A. Intermittent everolimus administration for malignant insulinoma. Endocrinol. Diabetes Metab. Case Rep. 2014, 2014, 140047. [Google Scholar] [CrossRef] [PubMed]
- Akahori, H. Clinical remission of an inoperable malignant insulinoma by the combination treatment with octreotide and everolimus. J. Gen. Fam. Med. 2019, 20, 107–110. [Google Scholar] [CrossRef] [PubMed]
- Chen, Q.; Wang, W.J.; Jia, Y.X.; Yuan, H.; Wu, P.F.; Ge, W.L.; Meng, L.D.; Huang, X.M.; Shen, P.; Yang, T.Y.; et al. Effect of the transcription factor YY1 on the development of pancreatic endocrine and exocrine tumors: A narrative review. Cell Biosci. 2021, 11, 86. [Google Scholar] [CrossRef] [PubMed]
- Hong, X.; Qiao, S.; Li, F.; Wang, W.; Jiang, R.; Wu, H.; Chen, H.; Liu, L.; Peng, J.; Wang, J.; et al. Whole-genome sequencing reveals distinct genetic bases for insulinomas and non-functional pancreatic neuroendocrine tumours: Leading to a new classification system. Gut 2020, 69, 877–887. [Google Scholar] [CrossRef] [PubMed]
- Hackeng, W.M.; Schelhaas, W.; Morsink, F.H.M.; Heidsma, C.M.; van Eeden, S.; Valk, G.D.; Vriens, M.R.; Heaphy, C.M.; Nieveen van Dijkum, E.J.M.; Offerhaus, G.J.A.; et al. Alternative Lengthening of Telomeres and Differential Expression of Endocrine Transcription Factors Distinguish Metastatic and Non-metastatic Insulinomas. Endocr. Pathol. 2020, 31, 108–118. [Google Scholar] [CrossRef] [PubMed]
- Di Domenico, A.; Pipinikas, C.P.; Maire, R.S.; Bräutigam, K.; Simillion, C.; Dettmer, M.S.; Vassella, E.; Thirlwell, C.; Perren, A.; Marinoni, I. Epigenetic landscape of pancreatic neuroendocrine tumours reveals distinct cells of origin and means of tumour progression. Commun. Biol. 2020, 3, 740. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).