


Assessment Tools for the Admission of Older Adults to Inpatient Rehabilitation: A Scoping Review


Abstract
1. Introduction
2. Materials and Methods
2.1. Information Sources and Search
2.2. Inclusion Criteria
2.3. Exclusion Criteria
2.4. Types of Outcomes
2.5. Data Analysis
3. Results
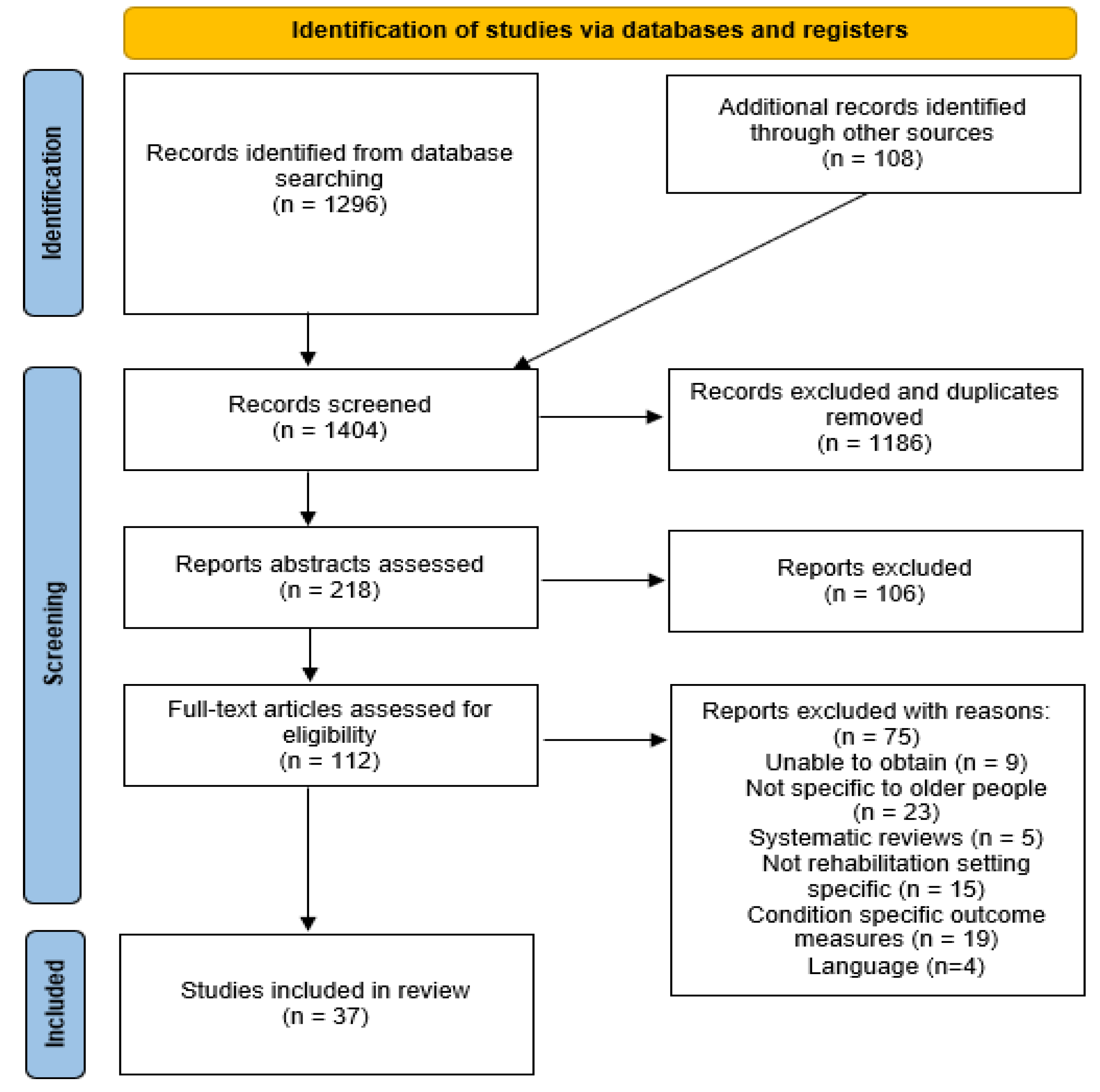
3.1. Study Selection
3.2. Study Characteristics
3.3. Definition of Rehabilitation
3.4. Assessment for Geriatric Rehabilitation
3.5. Assessments Used for Geriatric Rehabilitation
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| GR | Geriatric rehabilitation |
| MDT | Multidisciplinary team |
| RP | Rehabilitation potential |
| WHO | World Health Organization |
| ICF | International Classification of Functioning, Disability and Health |
| CGA | Comprehensive geriatric assessment |
| PADLs | Personal Activities of Daily Living |
| IADLs | Instrumental Activities of Daily Living |
References
- National Statistics Office (NSO) Malta (2021). World Population Day: 11 July News Release 9 July 2021. Available online: https://nso.gov.mt/en/News_Releases/Documents/2021/07/News2021_122.pdf (accessed on 31 August 2022).
- Elphick, H.L.; Mankad, K.; Madan, S.; Parker, C.; Liddle, B.J. The Determinants of Successful In-Hospital Rehabilitation in People Aged 90 Years and Older. Gerontology 2007, 53, 116–120. [Google Scholar] [CrossRef] [PubMed]
- Falahati, A.; Sahaf, R.; Kamrani, A.A.A.; Momtaz, Y.A.; Rassafiani, M.; Fillenbaum, G. Validity and Reliability of OARS Multidimensional Functional Assessment Questionnaire in Iranian Elderly. Iran. Rehabil. J. 2018, 16, 169–176. [Google Scholar] [CrossRef]
- Kool, J.; Oesch, P.; Bachmann, S. Predictors for living at home after geriatric inpatient rehabilitation: A prospective cohort study. J. Rehabil. Med. 2017, 49, 185–190. [Google Scholar] [CrossRef] [PubMed]
- van der Laag, P.J.; Arends, S.A.; Bosma, M.S.; Hoogen, A.V.D. Factors associated with successful rehabilitation in older adults: A systematic review and best evidence synthesis. Geriatr. Nurs. 2020, 42, 83–93. [Google Scholar] [CrossRef] [PubMed]
- D’Souza, A.N.; Said, C.M.; Leggett, N.E.; Tomkins, M.S.; Kay, J.E.; Granger, C.L. Assessment tools and factors used to predict discharge from acute general medical wards: A systematic review. Disabil. Rehabil. 2021, 44, 3373–3387. [Google Scholar] [CrossRef]
- van Balen, R.; Gordon, A.L.; Schols, J.M.G.A.; Drewes, Y.M.; Achterberg, W.P. What is geriatric rehabilitation and how should it be organized? A Delphi study aimed at reaching European consensus. Eur. Geriatr. Med. 2019, 10, 977–987. [Google Scholar] [CrossRef]
- Allan, C.M.; Campbell, W.; Guptill, C.; Stephenson, F.F.; Campbell, K.E. A conceptual model for interprofessional education: The international classification of functioning, disability and health (ICF). J. Interprofessional Care 2006, 20, 235–245. [Google Scholar] [CrossRef]
- Landi, F.; Bernabei, R.; Russo, A.; Zuccalã, G.; Onder, G.; Carosella, L.; Cesari, M.; Cocchi, A. Predictors of Rehabilitation Outcomes in Frail Patients Treated in a Geriatric Hospital. J. Am. Geriatr. Soc. 2002, 50, 679–684. [Google Scholar] [CrossRef]
- World Health Organization (WHO) (2002). Towards a Common Language for Functioning, Disability and Health. Available online: https://cdn.who.int/media/docs/default-source/classification/icf/icfbeginnersguide.pdf (accessed on 31 August 2022).
- Bachmann, S.; Finger, C.; Huss, A.; Egger, M.; Stuck, A.E.; Clough-Gorr, K.M. Inpatient rehabilitation specifically designed for geriatric patients: Systematic review and meta-analysis of randomised controlled trials. BMJ 2010, 340, c1718. [Google Scholar] [CrossRef]
- World Health Organization (WHO) (2022). Ageing. Health Topics. Available online: https://www.who.int/health-topics/ageing#tab=tab_1 (accessed on 31 August 2022).
- Hershkovitz, A.; Kalandariov, Z.; Hermush, V.; Weiss, R.; Brill, S. Factors Affecting Short-Term Rehabilitation Outcomes of Disabled Elderly Patients With Proximal Hip Fracture. Arch. Phys. Med. Rehabil. 2007, 88, 916–921. [Google Scholar] [CrossRef]
- Smit, E.B.; Bouwstra, H.; Van Der Wouden, J.C.; Hertogh, C.M.P.M.; Wattel, E.M.; Roorda, L.D.; Terwee, C.B. Development of a Patient-Reported Outcomes Measurement Information System (PROMIS®) short form for measuring physical function in geriatric rehabilitation patients. Qual. Life Res. 2020, 29, 2563–2572. [Google Scholar] [CrossRef]
- Kabboord, A.D.; Godfrey, D.; Gordon, A.; Gladman, J.R.F.; Van Eijk, M.; Van Balen, R.; Achterberg, W.P. The modified functional comorbidity index performed better than the Charlson index and original functional comorbidity index in predicting functional outcome in geriatric rehabilitation: A prospective observational study. BMC Geriatr. 2020, 20, 114. [Google Scholar] [CrossRef]
- Adunsky, A.; Levenkrohn, S.; Fleissig, Y.; Arad, M.; Heruti, R.J. Rehabilitation outcomes in patients with full weight-bearing hip fractures. Arch. Gerontol. Geriatr. 2001, 33, 123–131. [Google Scholar] [CrossRef]
- Adunsky, A.; Lusky, A.; Arad, M.; Heruti, R.J. A Comparative Study of Rehabilitation Outcomes of Elderly Hip Fracture Patients: The Advantage of a Comprehensive Orthogeriatric Approach. J. Gerontol. Ser. A 2003, 58, M542–M547. [Google Scholar] [CrossRef]
- Baztán, J.J.; Gálvez, C.P.; Socorro, A. Recovery of Functional Impairment after Acute Illness and Mortality: One-Year Follow-Up Study. Gerontology 2009, 55, 269–274. [Google Scholar] [CrossRef]
- D’Alton, M.; Larkin, J.; McKeag, A.; Coakley, G.; Nolan, E.; O’Connor, M.; Dolan, E. 137 Does the Clinical Frailty Scale Predict Rehabilitation Potential in Older Patients? Age Ageing 2019, 48, iii17–iii65. [Google Scholar] [CrossRef]
- Volpato, S.; Cavalieri, M.; Guerra, G.; Sioulis, F.; Ranzini, M.; Maraldi, C.; Fellin, R.; Guralnik, J.M. Performance-Based Functional Assessment in Older Hospitalized Patients: Feasibility and Clinical Correlates. J. Gerontol. Ser. A 2008, 63, 1393–1398. [Google Scholar] [CrossRef]
- Chin, R.P.H.; Ng, B.H.P.; Cheung, L.P.C. Factors predicting rehabilitation outcomes of elderly patients with hip fracture. Hong Kong Med. J. 2008, 14, 209. [Google Scholar]
- Sweet, L.; Van Adel, M.; Metcalfe, V.; Wright, L.; Harley, A.; Leiva, R.; Taler, V. The Montreal Cognitive Assessment (MoCA) in geriatric rehabilitation: Psychometric properties and association with rehabilitation outcomes. Int. Psychogeriatr. 2011, 23, 1582–1591. [Google Scholar] [CrossRef]
- Dutzi, I.; Schwenk, M.; Kirchner, M.; Bauer, J.M.; Hauer, K. “What would you like to achieve?” Goal-Setting in Patients with Dementia in Geriatric Rehabilitation. BMC Geriatr. 2019, 19, 280. [Google Scholar] [CrossRef]
- Aquilani, R.; Zuccarelli, G.C.; Maestri, R.; Rutili, C.; Colombo, M.; Condino, A.M.; Barbieri, A.; Cecchetti, A.; Vanzati, S.; Bonazza, E.; et al. Inflammation, pressure ulcers and poor functional status predict negative rehabilitation outcomes in postacute geriatric patients. Aging Clin. Exp. Res. 2020, 33, 463–467. [Google Scholar] [CrossRef] [PubMed]
- Stolee, P.; Stadnyk, K.; Myers, A.M.; Rockwood, K. An Individualized Approach to Outcome Measurement in Geriatric Rehabilitation. J. Gerontol. Ser. A 1999, 54, M641–M647. [Google Scholar] [CrossRef] [PubMed]
- Gosselin, S.; Desrosiers, J.; Corriveau, H.; Hébert, R.; Rochette, A.; Provencher, V.; Côté, S.; Tousignant, M. Outcomes during and after inpatient rehabilitation: Comparison between adults and older adults. Acta Derm. -Venereol. 2008, 40, 55–60. [Google Scholar] [CrossRef] [PubMed]
- Cowley, A.; Goldberg, S.E.; Gordon, A.L.; Logan, P.A. Rehabilitation potential in older people living with frailty: A systematic mapping review. BMC Geriatr. 2021, 21, 533. [Google Scholar] [CrossRef]
- Low, S.; Wee, E.; Dorevitch, M. Impact of place of residence, frailty and other factors on rehabilitation outcomes post hip fracture. Age Ageing 2020, 50, 423–430. [Google Scholar] [CrossRef]
- Jupp, B.J.; Mallela, S.K.; Kwan, J.; Allen, S.; Sharma, J.C.; Vassallo, M. Development and evaluation of the GEMS (gait, eyesight, mental state, sedation) tool as an aid to predict outcome after hospitalization. Geriatr. Gerontol. Int. 2011, 11, 8–15. [Google Scholar] [CrossRef]
- Semel, J.; Gray, J.M.; Ahn, H.J.; Nasr, H.; Chen, J.J. Predictors of Outcome Following Hip Fracture Rehabilitation. PM&R 2010, 2, 799–805. [Google Scholar] [CrossRef]
- Ruchinskas, R.A.; Singer, H.K.; Repetz, N.K. Clock drawing, clock copying, and physical abilities in geriatric rehabilitation. Arch. Phys. Med. Rehabil. 2001, 82, 920–924. [Google Scholar] [CrossRef]
- Vogt, L.; Wieland, K.; Bach, M.; Himmelreich, H.; Banzer, W. Cognitive status and ambulatory rehabilitation outcome in geriatric patients. J. Rehabil. Med. 2008, 40, 876–878. [Google Scholar] [CrossRef]
- Grill, E.; Kus, S.; Müller, M.; Strobl, R. Patient goals in post-acute geriatric rehabilitation: Goal attainment is an indicator for improved functioning. J. Rehabil. Med. 2011, 43, 156–161. [Google Scholar] [CrossRef]
- McPhail, S.M.; Nalder, E.; Hill, A.-M.; Haines, T.P. Physiotherapists Have Accurate Expectations of Their Patients’ Future Health-Related Quality of Life after First Assessment in a Subacute Rehabilitation Setting. BioMed Res. Int. 2013, 2013, 340371. [Google Scholar] [CrossRef]
- Myers, J.S.; Grigsby, J.; Teel, C.S.; Kramer, A.M. Nurses’ assessment of rehabilitation potential and prediction of functional status at discharge from inpatient rehabilitation. Int. J. Rehabil. Res. 2009, 32, 264–266. [Google Scholar] [CrossRef]
- Liu, S.K.; Montgomery, J.; Yan, Y.; Mecchella, J.N.; Bartels, S.J.; Masutani, R.; Batsis, J.A. Association Between Hospital Admission Risk Profile Score and Skilled Nursing or Acute Rehabilitation Facility Discharges in Hospitalized Older Adults. J. Am. Geriatr. Soc. 2016, 64, 2095–2100. [Google Scholar] [CrossRef]
- Wan, C.S.; Reijnierse, E.M.; Maier, A.B. Risk Factors of Readmissions in Geriatric Rehabilitation Patients: RESORT. Arch. Phys. Med. Rehabil. 2021, 102, 1524–1532. [Google Scholar] [CrossRef]
- Nouvenne, A.; Ticinesi, A.; Cerundolo, N.; Prati, B.; Parise, A.; Chiussi, G.; Frosio, L.; Guerra, A.; Brianti, E.; Fabi, M.; et al. Implementing a multidisciplinary rapid geriatric observation unit for non-critical older patients referred to hospital: Observational study on real-world data. Aging Clin. Exp. Res. 2021, 34, 599–609. [Google Scholar] [CrossRef]
- EuroQol Research Foundation (2022). EQ-5D About. Available online: https://euroqol.org/eq-5d-instruments/ (accessed on 31 August 2022).
- Tröster, T.; Thalmann, M.; Fischer, K.; Bieri-Brüning, G.; Beeler, P.E.; Bischoff-Ferrari, H.A.; Gagesch, M. Frailty, underweight and impaired mobility are associated with institutionalisation after post-acute care. Swiss Med. Wkly. 2020, 150, w20276. [Google Scholar] [CrossRef]
- Singh, I.; Gallacher, J.; Davis, K.; Johansen, A.; Eeles, E.; Hubbard, R.E. Predictors of adverse outcomes on an acute geriatric rehabilitation ward. Age Ageing 2012, 41, 242–246. [Google Scholar] [CrossRef]
- Gillner, A.; Hulten, A.; Kerstell, J.; Olsson, R.; Steen, B.; Svanborg, A. Intensive Short-term Rehabilitation of Geriatric Patients: Initial Results and One-Year Follow Up. Scand. J. Rehabil. Med. 1969, 1, 133. [Google Scholar] [PubMed]
- Muir-Hunter, S.W.; Fat, G.L.; Mackenzie, R.; Wells, J.; Montero-Odasso, M. Defining rehabilitation success in older adults with dementia–results from an inpatient geriatric rehabilitation unit. J. Nutr. Health Aging 2015, 20, 439–445. [Google Scholar] [CrossRef]
- Calle, A.; Onder, G.; Morandi, A.; Bellelli, G.; Ortolani, E.; Pérez, L.M.; Mesas, M.; Sanniti, A.; Mazzanti, P.; Platto, C.N.; et al. Frailty Related Factors as Predictors of Functional Recovery in Geriatric Rehabilitation: The Sarcopenia and Function in Aging Rehabilitation (SAFARI) Multi-Centric Study. J. Nutr. Health Aging 2018, 22, 1099–1106. [Google Scholar] [CrossRef]
- Johansen, I.; Lindbaek, M.; Stanghelle, J.; Brekke, M. Effective rehabilitation of older people in a district rehabilitation centre. J. Rehabil. Med. 2011, 43, 461–464. [Google Scholar] [CrossRef] [PubMed]
- Valderrama-Gama, E.; Damián, J.; Guallar, E.; Rodríguez-Mañas, L. Previous Disability as a Predictor of Outcome in a Geriatric Rehabilitation Unit. J. Gerontol. Ser. A 1998, 53, M405–M409. [Google Scholar] [CrossRef] [PubMed]
- Barnes, D.E.; Mehta, K.M.; Boscardin, W.J.; Fortinsky, R.H.; Palmer, R.M.; Kirby, K.; Landefeld, C.S. Prediction of Recovery, Dependence or Death in Elders Who Become Disabled During Hospitalization. J. Gen. Intern. Med. 2012, 28, 261–268. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef]
- Higgins, J.; Thomas, J. Cochrane Handbook for Systematic Reviews of Interventions, 2nd ed.; John Wiley and Sons, Ltd.: Chichester, UK, 2019; pp. 143–176. [Google Scholar]
- Konda, S.R.; Lott, A.; Saleh, H.; Schubl, S.; Chan, J.; Egol, K.A. How Does Frailty Factor Into Mortality Risk Assessment of a Middle-Aged and Geriatric Trauma Population? Geriatr Orthop Surg Rehabil. 2017, 8, 225–230. [Google Scholar] [CrossRef] [PubMed]
- Deom, C.E.; Carpenter, J.; Bodine, A.J.; Taylor, S.M.; Heinemann, A.W.; Lieber, R.L.; Sliwa, J.A. A Mobility Measure for Inpatient Rehabilitation Using Multigroup, Multidimensional Methods. J Neurol Phys Ther. 2021, 45, 101–111. [Google Scholar] [CrossRef]
- Zogg, C.K.; Falvey, J.R.; Dimick, J.B.; Haider, A.H.; Davis, K.A.; Grauer, J.N. Changes in Discharge to Rehabilitation: Potential Unintended Consequences of Medicare Total Hip Arthroplasty/Total Knee Arthroplasty Bundled Payments, Should They Be Implemented on a Nationwide Scale? J. Arthroplasty 2019, 34, 1058–1065.e4. [Google Scholar] [CrossRef] [PubMed]
- Sermon, A.; Slock, C.; Coeckelberghs, E.; Seys, D.; Panella, M.; Bruyneel, L.; Nijs, S.; Akiki, A.; Castillon, P.; Chipperfield, A.; et al. Quality indicators in the treatment of geriatric hip fractures: Literature review and expert consensus. Arch. Osteoporos. 2021, 16, 152. [Google Scholar] [CrossRef]
- Lemos, J.L.; Welch, J.M.; Xiao, M.; Shapiro, L.M.; Adeli, E.; Kamal, R.N. Is Frailty Associated with Adverse Outcomes After Orthopaedic Surgery?: A Systematic Review and Assessment of Definitions. JBJS Rev. 2021, 9. [Google Scholar] [CrossRef]
- Keppler, A.M.; Holzschuh, J.; Pfeufer, D.; Gleich, J.; Neuerburg, C.; Kammerlander, C.; Böcker, W.; Fürmetz, J. Mobility improvement in the first 6 postoperative weeks in orthogeriatric fracture patients. Eur. J. Trauma Emerg. Surg. 2022, 48, 2867–2872. [Google Scholar] [CrossRef]
- Pai, S.L.; Jacob, A.K.; Wang, R.D. Preoperative optimization of geriatric and frail patients. Int. Anesthesiol. Clin. 2022, 60, 33–42. [Google Scholar] [CrossRef] [PubMed]
- Pereira, S.R.; Chiu, W.; Turner, A.; Chevalier, S.; Joseph, L.; Huang, A.R.; Morais, J.A. How can we improve targeting of frail elderly patients to a geriatric day-hospital rehabilitation program? BMC Geriatr. 2010, 10, 82. [Google Scholar] [CrossRef] [PubMed]
- Belloni, G.; Seematter-Bagnoud, L.; Krief, H.; Aminian, K.; Büla, C.J. Falls Efficacy Is Associated With Better Gait and Functional Outcomes After Rehabilitation in Older Patients. Arch. Phys. Med. Rehabil. 2021, 102, 1134–1139. [Google Scholar] [CrossRef] [PubMed]
- Külzer, A.M.; Scolari, C.C.; Gus, M. Relationship between usual physical, cognitive and social activities and functional recovery at hospital discharge after acute stroke. J. Rehabil Med. 2008, 40, 195–199. [Google Scholar] [CrossRef] [PubMed]
- McClure, J.A.; Salter, K.; Meyer, M.; Foley, N.; Kruger, H.; Teasell, R. Predicting length of stay in patients admitted to stroke rehabilitation with high levels of functional independence. Disabil Rehabil. 2011, 33, 2356–2361. [Google Scholar] [CrossRef] [PubMed]
- Munten, G. Nursing sensitive quality indicators for nursing home care: International review of literature, policy and practice1). NED. TIJDS. EVID. PRACT. 2014, 16–17. [Google Scholar] [CrossRef]


{kind=link}
| Theme of Study | Number of Articles | Percent of Articles (%) |
|---|---|---|
| Factors impacting rehabilitation | 19 | 51.4 |
| Specific outcome measures used for rehabilitation | 11 | 29.7 |
| Assessment of inpatient rehabilitation outcomes | 6 | 16.2 |
| Functional status and mortality after rehabilitation | 5 | 13.5 |
| Nurses’ predictions of rehabilitation | 2 | 5.4 |
| Outcomes for admission to rehabilitation | 1 | 2.7 |
| Rehabilitation applied to the oldest old | 1 | 2.7 |
| Domain | Number of Articles (n) | Percent out of Articles (%) |
|---|---|---|
| Function | 31 | 83.8 |
| Cognition | 29 | 78.4 |
| Medical | 23 | 62.2 |
| Physical | 16 | 43.2 |
| Behaviour | 11 | 35.1 |
| Quality of life | 8 | 21.6 |
| Frailty | 7 | 18.9 |
| Nutrition | 4 | 10.8 |
| Communication and vision | 3 | 8.1 |
| Abuse | 1 | 2.7 |
| Pain | 1 | 2.7 |
| Outcome Measure | Outcome Measure Abbreviation | Number of Uses in Studies (n) | Percent out of Articles (%) |
|---|---|---|---|
| Mini Mental State Examination | MMSE | 19 | 51.4 |
| Barthel Index | BI | 11 | 29.7 |
| Functional Independence Measure | FIM | 10 | 27.0 |
| Charlson Comorbidity Index | CCI | 10 | 27.0 |
| Hand-Grip Strength Test | HGS | 6 | 16.2 |
| Timed Up and Go Test | TUG | 6 | 16.2 |
| Geriatric Depression Scale | GDS | 6 | 16.2 |
| Rockwood Clinical Frailty Score | CFS | 6 | 16.2 |
| Montreal Cognitive Assessment | MoCA | 3 | 8.1 |
| Clock Drawing and Clock Copying Test | CDT | 3 | 8.1 |
| Mini Nutritional Assessment | MNA | 2 | 5.4 |
| EQ-5D-3L | EQ-5D-3L | 2 | 5.4 |
| Domain | Number of Outcome Measures (n) | Percent of Outcome Measures (%) |
|---|---|---|
| Cognition | 40 | 23.3 |
| Function | 35 | 20.4 |
| Physical | 30 | 17.4 |
| Medical | 23 | 13.4 |
| Behaviour | 16 | 9.3 |
| Quality of life | 12 | 7.0 |
| Frailty | 8 | 4.7 |
| Nutrition | 4 | 2.3 |
| Communication and vision | 2 | 1.2 |
| Abuse; Pain | 2 | 1.2 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Muscat, F.; Camilleri, L.; Attard, C.; Lungaro Mifsud, S. Assessment Tools for the Admission of Older Adults to Inpatient Rehabilitation: A Scoping Review. J. Clin. Med. 2023, 12, 919. https://doi.org/10.3390/jcm12030919
Muscat F, Camilleri L, Attard C, Lungaro Mifsud S. Assessment Tools for the Admission of Older Adults to Inpatient Rehabilitation: A Scoping Review. Journal of Clinical Medicine. 2023; 12(3):919. https://doi.org/10.3390/jcm12030919
Chicago/Turabian StyleMuscat, Francesca, Liberato Camilleri, Conrad Attard, and Stephen Lungaro Mifsud. 2023. "Assessment Tools for the Admission of Older Adults to Inpatient Rehabilitation: A Scoping Review" Journal of Clinical Medicine 12, no. 3: 919. https://doi.org/10.3390/jcm12030919
APA StyleMuscat, F., Camilleri, L., Attard, C., & Lungaro Mifsud, S. (2023). Assessment Tools for the Admission of Older Adults to Inpatient Rehabilitation: A Scoping Review. Journal of Clinical Medicine, 12(3), 919. https://doi.org/10.3390/jcm12030919