

Impact of Endophthalmitis on the Risk of Acute Myocardial Infarction in Ankylosing Spondylitis Patients: A Population-Based Retrospective Cohort Study
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source
2.2. Ethical Considerations
2.3. Patient Selection
2.4. Comorbidities
2.5. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ward, M.M.; Deodhar, A.; Gensler, L.S.; Dubreuil, M.; Yu, D.; Khan, M.A.; Haroon, N.; Borenstein, D.; Wang, R.; Biehl, A.; et al. 2019 Update of the American College of Rheumatology/Spondylitis Association of America/Spondyloarthritis Research and Treatment Network Recommendations for the Treatment of Ankylosing Spondylitis and Nonradiographic Axial Spondyloarthritis. Arthritis Rheumatol. 2019, 71, 1599–1613. [Google Scholar] [CrossRef]
- Golder, V.; Schachna, L. Ankylosing spondylitis: An update. Aust. Fam. Phys. 2013, 42, 780–784. [Google Scholar]
- Mathieu, S.; Pereira, B.; Soubrier, M. Cardiovascular events in ankylosing spondylitis: An updated meta-analysis. Semin. Arthritis Rheum. 2015, 44, 551–555. [Google Scholar] [CrossRef]
- Prati, C.; Demougeot, C.; Guillot, X.; Sondag, M.; Verhoeven, F.; Wendling, D. Vascular involvement in axial spondyloarthropathies. Jt. Bone Spine 2019, 86, 159–163. [Google Scholar] [CrossRef]
- Han, C.; Robinson, D.W., Jr.; Hackett, M.V.; Paramore, L.C.; Fraeman, K.H.; Bala, M.V. Cardiovascular disease and risk factors in patients with rheumatoid arthritis, psoriatic arthritis, and ankylosing spondylitis. J. Rheumatol. 2006, 33, 2167–2172. [Google Scholar]
- Schieir, O.; Tosevski, C.; Glazier, R.H.; Hogg-Johnson, S.; Badley, E.M. Incident myocardial infarction associated with major types of arthritis in the general population: A systematic review and meta-analysis. Ann. Rheum. Dis. 2017, 76, 1396–1404. [Google Scholar] [CrossRef]
- Rueda-Gotor, J.; Ferraz-Amaro, I.; Genre, F.; González Mazón, I.; Corrales, A.; Portilla, V.; Llorca, J.; Agudo-Bilbao, M.; Aurrecoechea, E.; Expósito, R.; et al. Cardiovascular and disease-related features associated with extra-articular manifestations in axial spondyloarthritis. A multicenter study of 888 patients. Semin. Arthritis Rheum. 2022, 57, 152096. [Google Scholar] [CrossRef]
- Nurmohamed, M.T.; van der Horst-Bruinsma, I.; Maksymowych, W.P. Cardiovascular and cerebrovascular diseases in ankylosing spondylitis: Current insights. Curr. Rheumatol. Rep. 2012, 14, 415–421. [Google Scholar] [CrossRef]
- Gopalamurugan, A.B.; Wheatcroft, S.; Hunter, P.; Thomas, M.R. Bilateral endophthalmitis and ARDS complicating group G streptococcal endocarditis. Lancet 2005, 366, 2062. [Google Scholar] [CrossRef]
- Yin, W.; Zhou, H.; Li, C. Endogenous Klebsiella pneumoniae endophthalmitis. Am. J. Emerg. Med. 2014, 32, 1300.e1303–1300.e1305. [Google Scholar] [CrossRef]
- Filipowicz, A.; Coca, M.N.; Blair, B.M.; Chang, P.Y. Acute Myocarditis with Cardiogenic Shock and Multiple Organ Failure, Followed by Bilateral Panuveitis Masquerading as Endogenous Endophthalmitis, Due to Toxoplasma Gondii in an Immunocompetent Patient. Retin. Cases Brief Rep. 2021, 15, 575–580. [Google Scholar] [CrossRef]
- Nakata, M.; Mashidori, T.; Higa, N.; Manita, M.; Chibana, N.; Tabata, K. Infective Endocarditis with No Underlying Disease for Which Bacterial Endophthalmitis Have Been the First Symptom. Intern. Med. 2020, 59, 2061–2065. [Google Scholar] [CrossRef] [PubMed]
- Mitaka, H.; Gomez, T.; Perlman, D.C. Scleritis and Endophthalmitis Due to Streptococcus pyogenes Infective Endocarditis. Am. J. Med. 2020, 133, e15–e16. [Google Scholar] [CrossRef] [PubMed]
- Hagiya, H.; Semba, T.; Morimoto, T.; Yamamoto, N.; Yoshida, H.; Tomono, K. Panophthalmitis caused by Streptococcus dysgalactiae subsp. Equisimilis: A case report and literature review. J. Infect. Chemother. 2018, 24, 936–940. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, C.Y.; Su, C.C.; Shao, S.C.; Sung, S.F.; Lin, S.J.; Kao Yang, Y.H.; Lai, E.C. Taiwan’s National Health Insurance Research Database: Past and future. Clin. Epidemiol. 2019, 11, 349–358. [Google Scholar] [CrossRef] [PubMed]
- Weng, T.H.; Chang, H.C.; Chung, C.H.; Lin, F.H.; Tai, M.C.; Tsao, C.H.; Chien, K.H.; Chien, W.C. Epidemiology and Mortality-Related Prognostic Factors in Endophthalmitis. Invest. Ophthalmol. Vis. Sci. 2018, 59, 2487–2494. [Google Scholar] [CrossRef]
- Lin, T.Y.; Lai, Y.F.; Chien, W.C.; Chen, Y.H.; Sun, C.A.; Chung, C.H.; Chen, J.T.; Chen, C.L. Association Between Endophthalmitis and the Incidence of Acute Coronary Syndrome in Patients with Ankylosing Spondylitis: A Nationwide, Population-Based Cohort Study. Front. Immunol. 2022, 13, 843796. [Google Scholar] [CrossRef]
- Rathore, V.; Singh, N.; Mahat, R.K.; Kocak, M.Z.; Fidan, K.; Ayazoglu, T.A.; Aydin Karahan, Y.G.; Onk, D.; Akar, E.; Yolcu, A. Risk Factors for Acute Myocardial Infarction: A Review. Ejmi 2018, 2, 1–7. [Google Scholar] [CrossRef]
- Chou, C.H.; Lin, M.C.; Peng, C.L.; Wu, Y.C.; Sung, F.C.; Kao, C.H.; Liu, S.H. A nationwide population-based retrospective cohort study: Increased risk of acute coronary syndrome in patients with ankylosing spondylitis. Scand. J. Rheumatol. 2014, 43, 132–136. [Google Scholar] [CrossRef]
- Hahn, B.H.; Grossman, J.; Chen, W.; McMahon, M. The pathogenesis of atherosclerosis in autoimmune rheumatic diseases: Roles of inflammation and dyslipidemia. J. Autoimmun. 2007, 28, 69–75. [Google Scholar] [CrossRef]
- Södergren, A.; Askling, J.; Bengtsson, K.; Forsblad-d’Elia, H.; Jernberg, T.; Lindström, U.; Ljung, L.; Mantel, Ä.; Jacobsson, L.T.H. Characteristics and outcome of a first acute myocardial infarction in patients with ankylosing spondylitis. Clin. Rheumatol. 2021, 40, 1321–1329. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.H.; Fang, C.C.; Tsai, L.M.; Gan, S.T.; Lin, S.H.; Li, Y.H. Patterns of Acute Myocardial Infarction in Taiwan from 2009 to 2015. Am. J. Cardiol. 2018, 122, 1996–2004. [Google Scholar] [CrossRef] [PubMed]
- Park, C.J.; Choi, Y.J.; Kim, J.G.; Han, I.B.; Do Han, K.; Choi, J.M.; Sohn, S. Association of Acute Myocardial Infarction with ankylosing Spondylitis: A nationwide longitudinal cohort study. J. Clin. Neurosci. 2018, 56, 34–37. [Google Scholar] [CrossRef] [PubMed]
- So, A.; Chan, J.; Sayre, E.; Avina-Zubieta, J. SAT0384 Risk of myocardial infarction and cerebrovascular accident in ankylosing spondylitis: A general population-based study. Ann. Rheum. Dis. 2017, 76, 916–917. [Google Scholar] [CrossRef]
- Musher, D.M.; Abers, M.S.; Corrales-Medina, V.F. Acute Infection and Myocardial Infarction. N. Engl. J. Med. 2019, 380, 171–176. [Google Scholar] [CrossRef]
- Putot, A.; Chague, F.; Manckoundia, P.; Cottin, Y.; Zeller, M. Post-Infectious Myocardial Infarction: New Insights for Improved Screening. J. Clin. Med. 2019, 8, 827. [Google Scholar] [CrossRef]
- Lacomba, M.S.; Martin, C.M.; Chamond, R.R.; Galera, J.M.G.; Omar, M.; Estevez, E.C. Aqueous and Serum Interferon γ, Interleukin (IL) 2, IL-4, and IL-10 in Patients with Uveitis. Arch. Ophthalmol. 2000, 118, 768–772. [Google Scholar] [CrossRef]
- Takase, H.; Futagami, Y.; Yoshida, T.; Kamoi, K.; Sugita, S.; Imai, Y.; Mochizuki, M. Cytokine Profile in Aqueous Humor and Sera of Patients with Infectious or Noninfectious Uveitis. Investig. Ophthalmol. Vis. Sci. 2006, 47, 1557–1561. [Google Scholar] [CrossRef]
- Lahmar, I.; Abou-Bacar, A.; Abdelrahman, T.; Guinard, M.; Babba, H.; Ben Yahia, S.; Kairallah, M.; Speeg-Schatz, C.; Bourcier, T.; Sauer, A.; et al. Cytokine Profiles in Toxoplasmic and Viral Uveitis. J. Infect. Dis. 2009, 199, 1239–1249. [Google Scholar] [CrossRef]
- Deshmukh, D.; Chakrabarti, M.; Jayasudha, R.; Hasnat Ali, M.; Tyagi, M.; Sharma, S.; Joseph, J. Elevated cytokine levels in vitreous as biomarkers of disease severity in infectious endophthalmitis. PLoS ONE 2018, 13, e0205292. [Google Scholar] [CrossRef]
- Gandhi, J.; Dave, V.P.; Joseph, J. Cytokine profiling plays a crucial role in activating immune system in fungal endophthalmitis. Int. J. Infect. Dis. 2020, 101, 240. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Endophthalmitis | Total | With | Without | p Value | |||
|---|---|---|---|---|---|---|---|
| Characteristics | n | % | n | % | n | % | |
| Total | 2785 | 557 | 20.00 | 2228 | 80.00 | ||
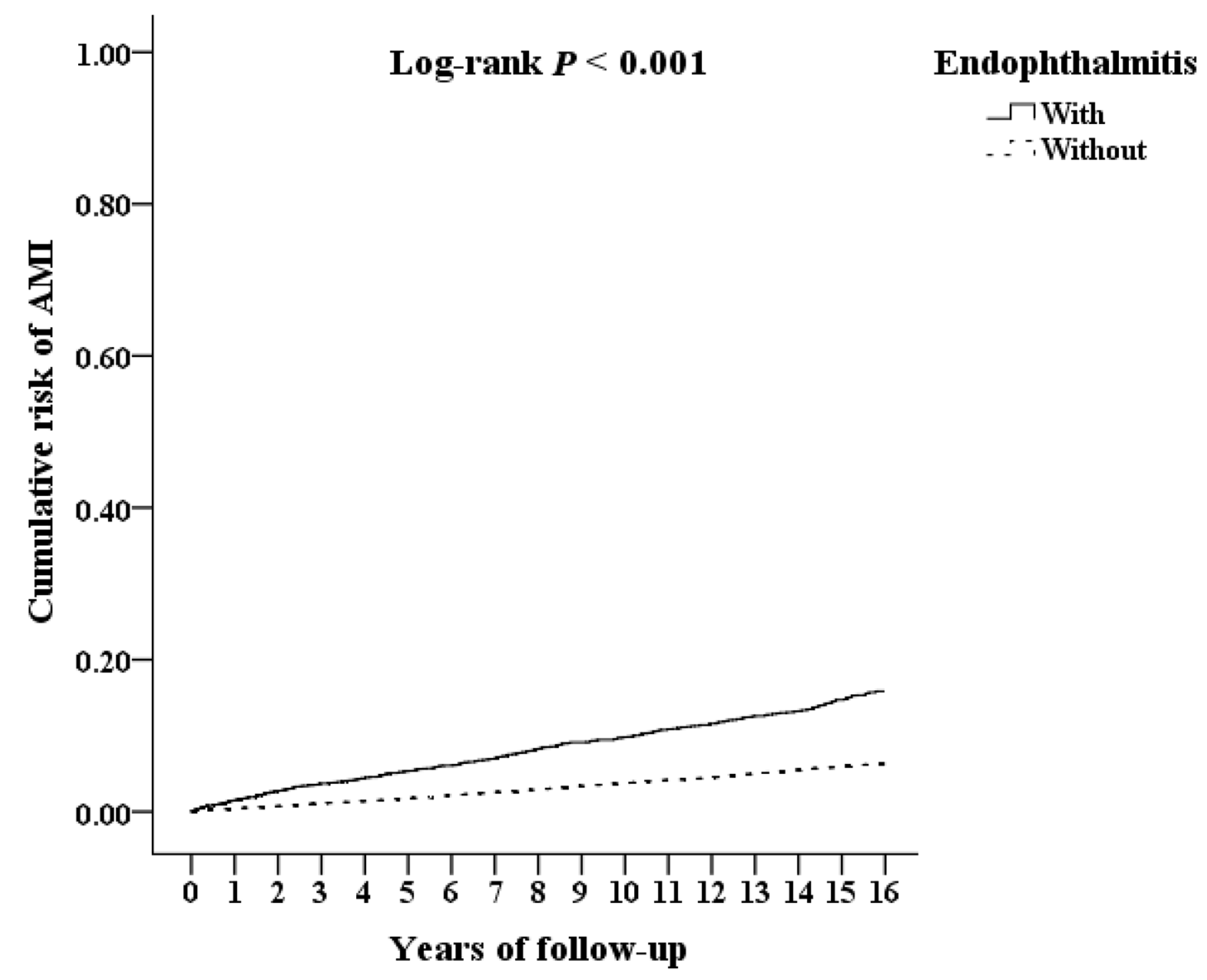
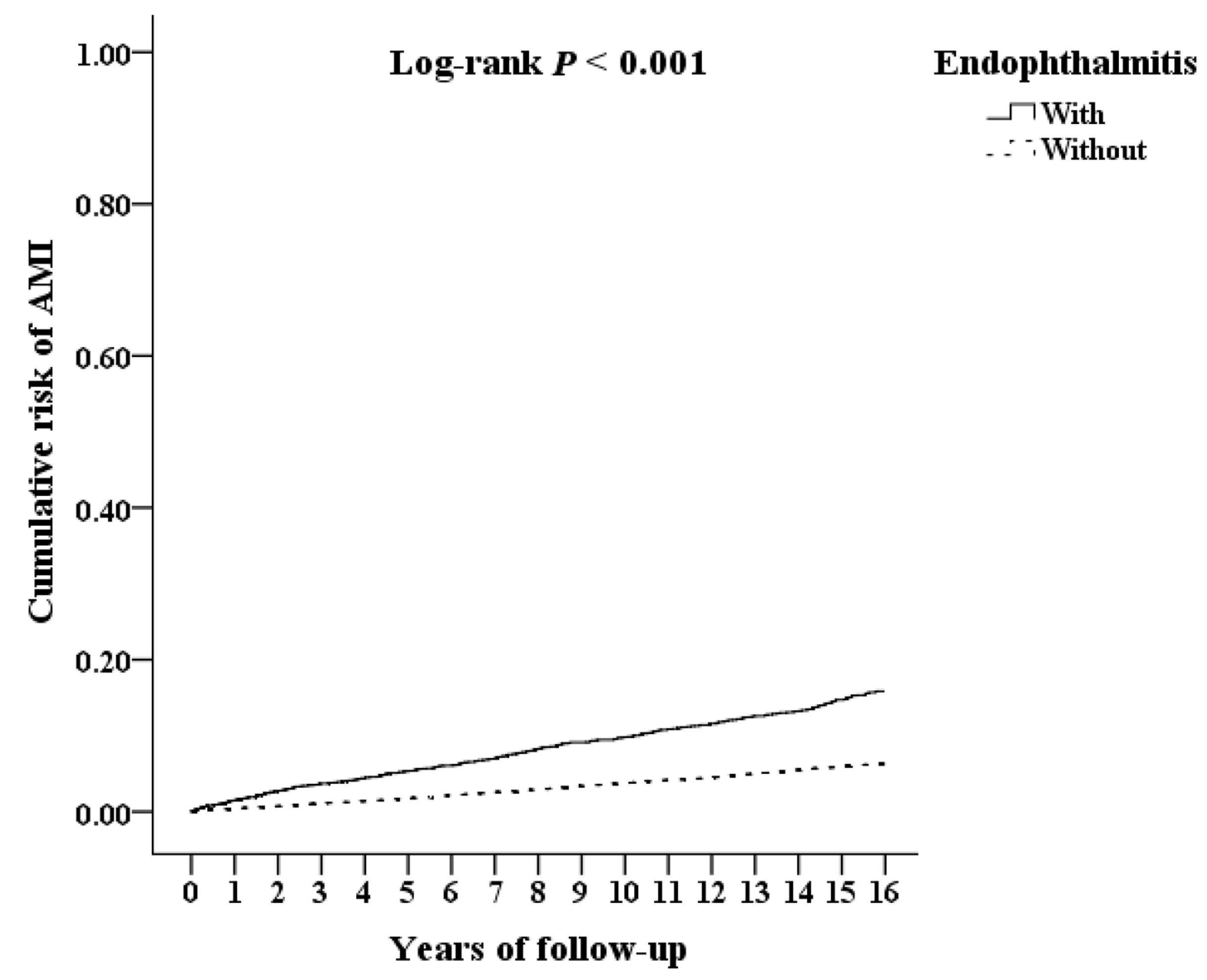
| AMI | 262 | 9.41 | 69 | 12.39 | 193 | 8.66 | <0.001 |
| Gender | 0.999 | ||||||
| Male | 1535 | 55.12 | 307 | 55.12 | 1228 | 55.12 | |
| Female | 1250 | 44.88 | 250 | 44.88 | 1000 | 44.88 | |
| Age (years) | 41.18 ± 19.77 | 40.53 ± 19.18 | 41.33 ± 19.90 | 0.045 | |||
| Age group (years) | 0.086 | ||||||
| 20–39 | 1619 | 58.13 | 308 | 55.30 | 1311 | 58.84 | |
| 40–59 | 770 | 27.65 | 154 | 27.65 | 616 | 27.65 | |
| ≧60 | 396 | 14.22 | 95 | 17.06 | 301 | 13.51 | |
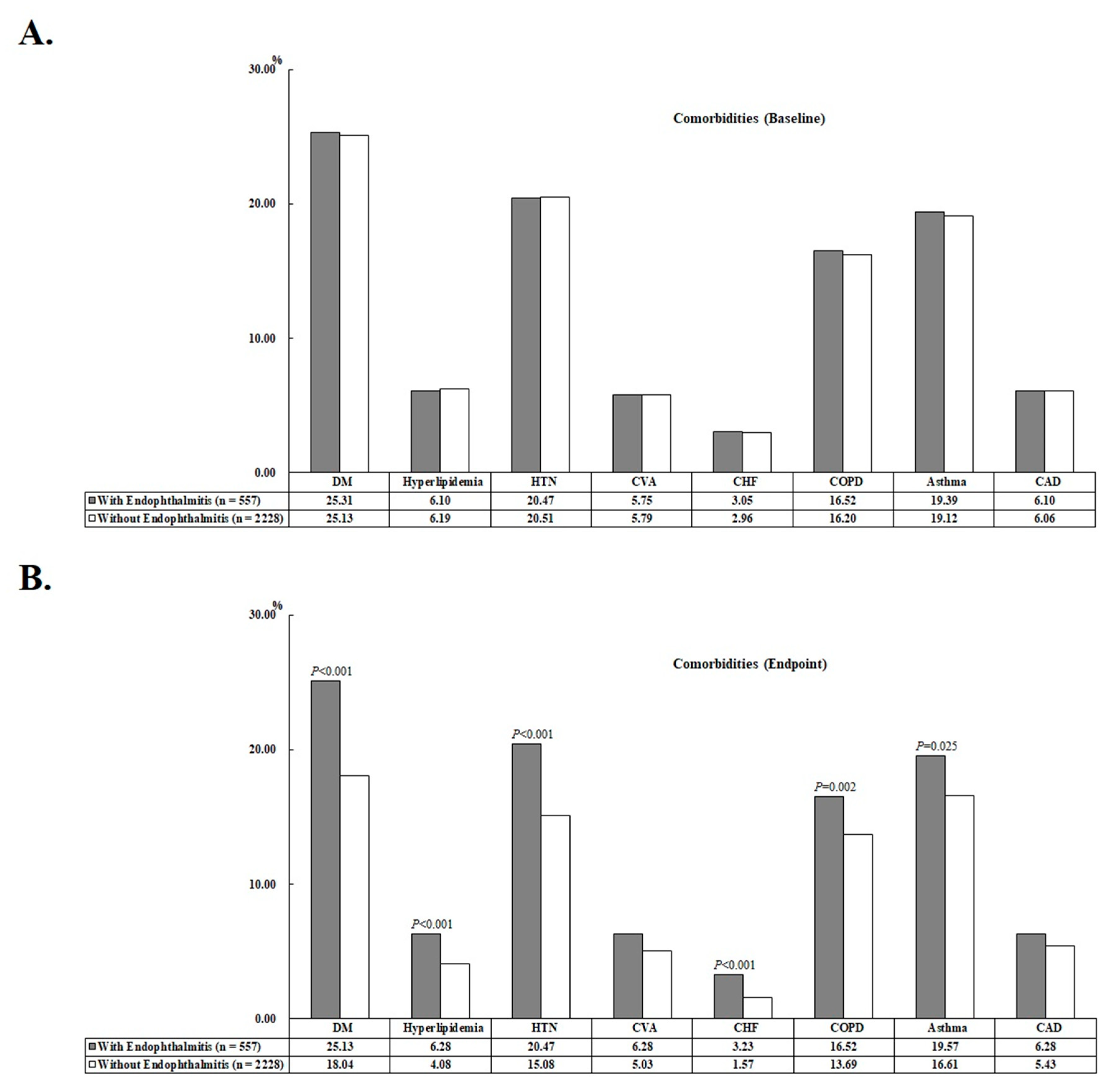
| DM | 542 | 19.46 | 140 | 25.13 | 402 | 18.04 | <0.001 |
| Hyperlipidemia | 126 | 4.52 | 35 | 6.28 | 91 | 4.08 | <0.001 |
| HTN | 450 | 16.16 | 114 | 20.47 | 336 | 15.08 | <0.001 |
| CVA | 147 | 5.28 | 35 | 6.28 | 112 | 5.03 | 0.145 |
| CHF | 53 | 1.90 | 18 | 3.23 | 35 | 1.57 | <0.001 |
| COPD | 397 | 14.25 | 92 | 16.52 | 305 | 13.69 | 0.002 |
| Asthma | 479 | 17.20 | 109 | 19.57 | 370 | 16.61 | 0.025 |
| CAD | 156 | 5.60 | 35 | 6.28 | 121 | 5.43 | 0.368 |
| CCI_R | 0.91 ± 1.11 | 0.99 ± 1.14 | 0.89 ± 1.10 | <0.001 | |||
| All-cause mortality | 222 | 7.97 | 49 | 8.80 | 173 | 7.76 | 0.324 |
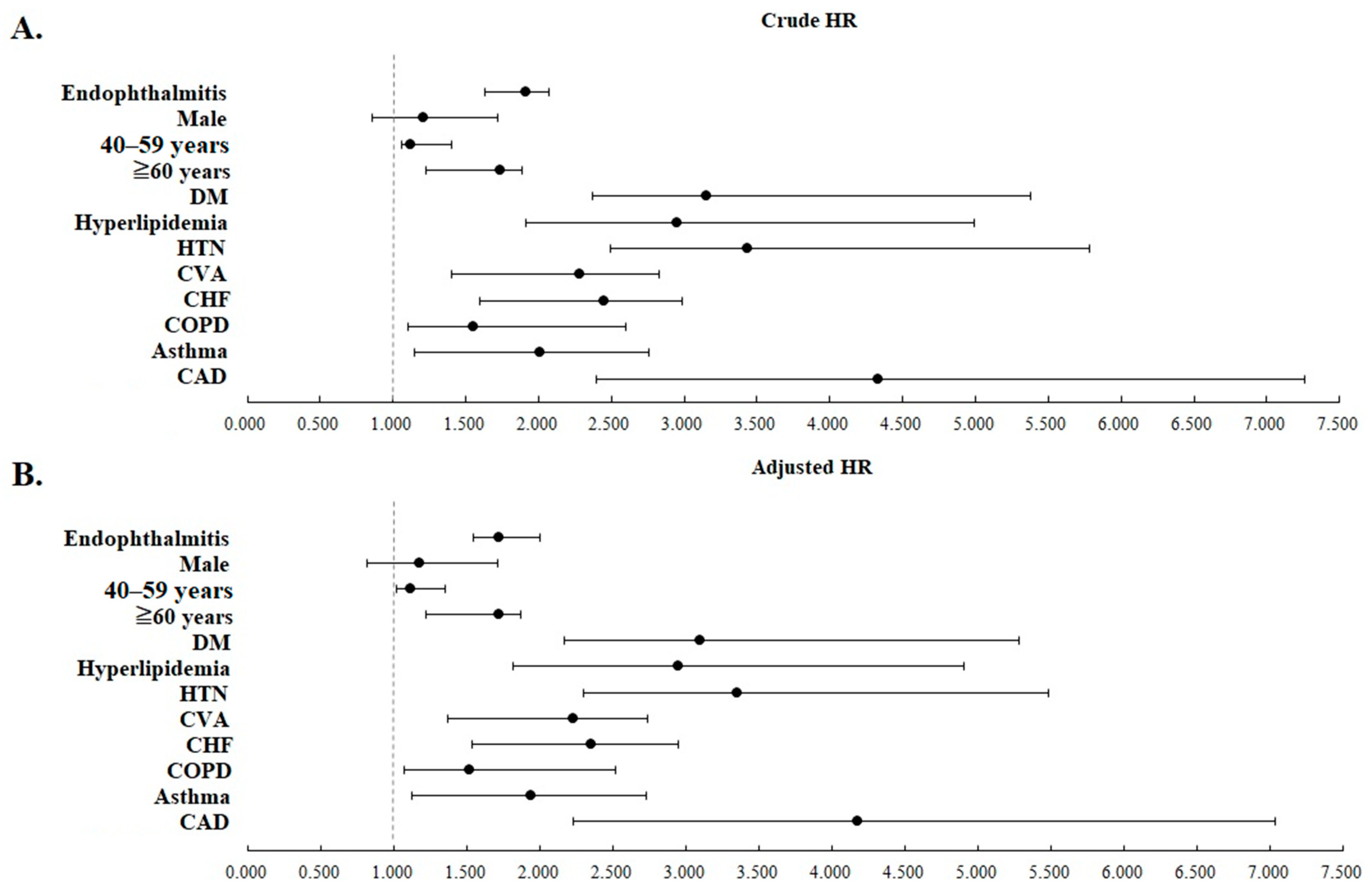
| Variables | Crude HR (95% CI) | p | Adjusted HR (95% CI) | p |
|---|---|---|---|---|
| Endophthalmitis | ||||
| Without | Reference | Reference | ||
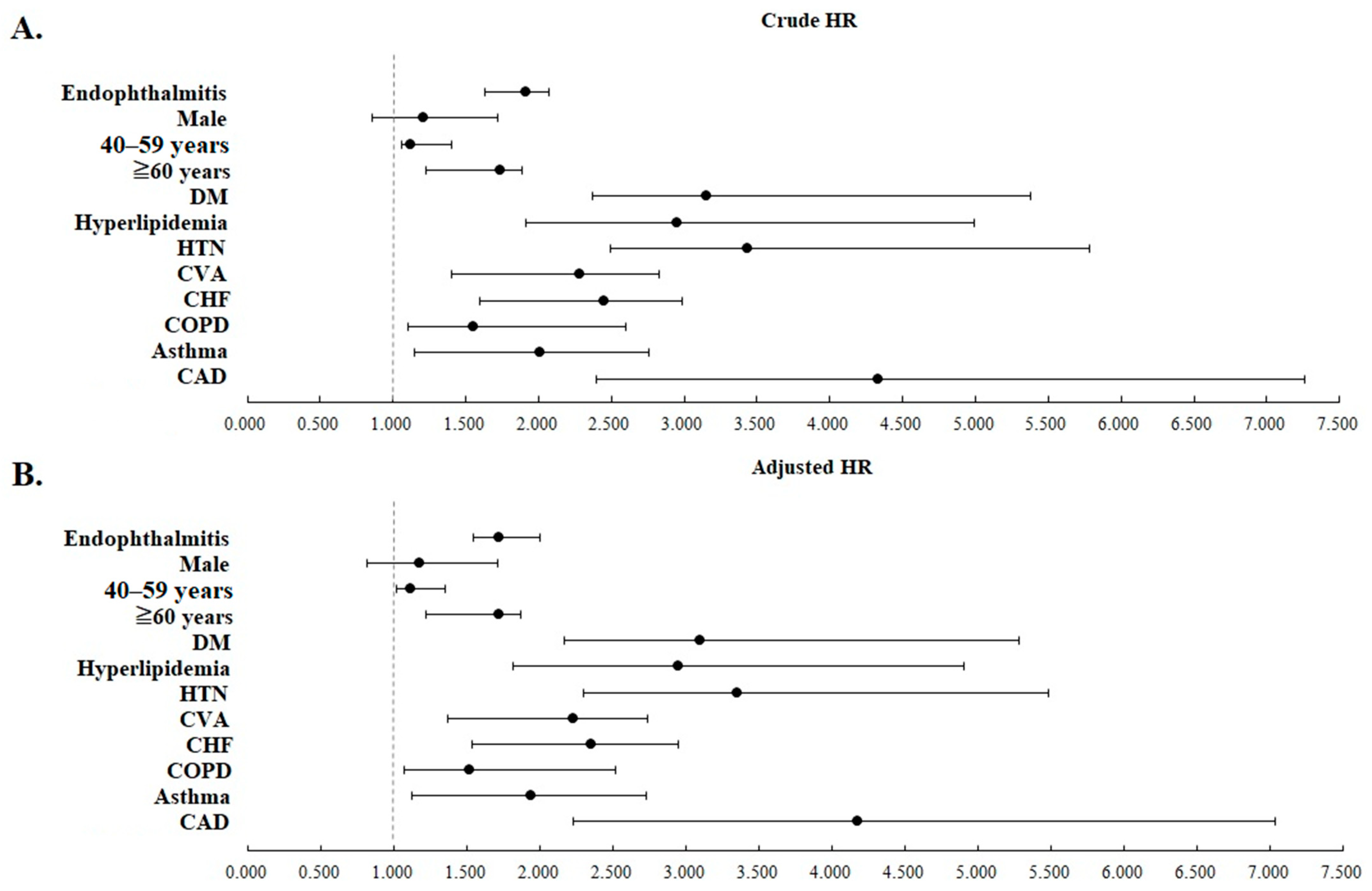
| With | 1.821 (1.527–2.027) | <0.001 | 1.631 (1.464–1.898) | <0.001 |
| Gender | ||||
| Male | 1.169 (0.790–1.565) | 0.302 | 1.144 (0.766–1.528) | 0.309 |
| Female | Reference | Reference | ||
| Age (yrs) | ||||
| 20–39 | Reference | Reference | ||
| 40–59 | 1.106 (1.043–1.308) | 0.028 | 1.074 (1.003–1.266) | 0.047 |
| ≧60 | 1.617 (1.205–1.764) | <0.001 | 1.511 (1.144–1.736) | <0.001 |
| DM | ||||
| Without | Reference | Reference | ||
| With | 2.962 (2.041–4.993) | <0.001 | 2.947 (2.023–4.937) | <0.001 |
| Hyperlipidemia | ||||
| Without | Reference | Reference | ||
| With | 2.714 (1.560–4.312) | <0.001 | 2.586 (1.508–4.203) | <0.001 |
| HTN | ||||
| Without | Reference | Reference | ||
| With | 3.155 (2.069–5.099) | <0.001 | 3.063 (2.020–5.088) | <0.001 |
| CVA | ||||
| Without | Reference | Reference | ||
| With | 2.225 (1.366–2.734) | <0.001 | 2.137 (1.244–2.652) | <0.001 |
| CHF | ||||
| Without | Reference | Reference | ||
| With | 2.349 (1.532–2.948) | <0.001 | 2.329 (1.470–2.856) | <0.001 |
| COPD | ||||
| Without | Reference | Reference | ||
| With | 1.479 (1.054–2.448) | <0.001 | 1.448 (1.039–2.377) | 0.003 |
| Asthma | ||||
| Without | Reference | Reference | ||
| With | 1.930 (1.075–2.659) | <0.001 | 1.919 (1.041–2.606) | 0.009 |
| CAD | ||||
| Without | Reference | Reference | ||
| With | 4.188(2.289–7.094) | <0.001 | 4.090 (2.191–7.017) | <0.001 |
| CCI_R | 1.210 (1.144–1.226) | <0.001 | 1.176 (1.132–1.210) | <0.001 |
| Endophthalmitis | With | Without (Reference) | Adjusted HR (95% CI) | p | ||
|---|---|---|---|---|---|---|
| Stratified Subgroups | Events | Rate (per 105 PYs) | Events | Rate (per 105 PYs) | ||
| Total | 69 | 1278.08 | 193 | 872.93 | 1.631 (1.464–1.898) | <0.001 |
| Gender | ||||||
| Male | 37 | 1242.71 | 102 | 837.40 | 1.680 (1.509–1.956) | <0.001 |
| Female | 32 | 1321.56 | 91 | 916.51 | 1.602 (1.437–1.863) | <0.001 |
| Age (yrs) | ||||||
| 20–39 | 39 | 1308.56 | 126 | 968.74 | 1.534 (1.386–1.796) | <0.001 |
| 40–59 | 19 | 1278.41 | 55 | 897.82 | 1.571 (1.411–1.828) | <0.001 |
| ≧60 | 11 | 1180.07 | 12 | 403.10 | 3.227 (2.896–3.753) | <0.001 |
| DM | ||||||
| Without | 55 | 1361.57 | 181 | 996.68 | 1.544 (1.386–1.797) | <0.001 |
| With | 14 | 1029.94 | 12 | 303.86 | 3.272 (2.938–3.808) | <0.001 |
| Hyperlipidemia | ||||||
| Without | 62 | 1223.69 | 186 | 878.26 | 1.575 (1.415–1.833) | <0.001 |
| With | 7 | 2107.86 | 7 | 751.68 | 3.089 (2.773–3.594) | <0.001 |
| HTN | ||||||
| Without | 52 | 1210.93 | 179 | 954.19 | 1.432 (1.286–1.667) | <0.001 |
| With | 17 | 1539.13 | 14 | 417.88 | 4.148 (3.724–4.826) | <0.001 |
| CVA | ||||||
| Without | 65 | 1276.32 | 187 | 893.15 | 1.596 (1.433–1.858) | <0.001 |
| With | 4 | 1307.27 | 6 | 511.81 | 3.282 (2.946–3.818) | <0.001 |
| CHF | ||||||
| Without | 67 | 1277.94 | 192 | 880.60 | 1.653 (1.483–1.922) | <0.001 |
| With | 2 | 1282.63 | 1 | 326.50 | 3.246 (2.915–3.778) | <0.001 |
| COPD | ||||||
| Without | 64 | 1415.78 | 188 | 981.41 | 1.620 (1.455–1.885) | <0.001 |
| With | 5 | 569.31 | 5 | 169.29 | 3.343 (3.001–3.890) | <0.001 |
| Asthma | ||||||
| Without | 62 | 1417.35 | 185 | 1014.80 | 1.591 (1.428–1.851) | <0.001 |
| With | 7 | 683.34 | 8 | 206.22 | 3.272 (2.937–3.808) | <0.001 |
| CAD | ||||||
| Without | 64 | 1268.26 | 189 | 905.25 | 1.570 (1.410–1.827) | <0.001 |
| With | 5 | 1418.60 | 4 | 324.85 | 5.165 (4.637–6.010) | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lin, T.-Y.; Lai, Y.-F.; Chien, W.-C.; Chen, Y.-H.; Chung, C.-H.; Chen, J.-T.; Chen, C.-L. Impact of Endophthalmitis on the Risk of Acute Myocardial Infarction in Ankylosing Spondylitis Patients: A Population-Based Retrospective Cohort Study. J. Clin. Med. 2023, 12, 1211. https://doi.org/10.3390/jcm12031211
Lin T-Y, Lai Y-F, Chien W-C, Chen Y-H, Chung C-H, Chen J-T, Chen C-L. Impact of Endophthalmitis on the Risk of Acute Myocardial Infarction in Ankylosing Spondylitis Patients: A Population-Based Retrospective Cohort Study. Journal of Clinical Medicine. 2023; 12(3):1211. https://doi.org/10.3390/jcm12031211
Chicago/Turabian StyleLin, Ting-Yi, Yi-Fen Lai, Wu-Chien Chien, Yi-Hao Chen, Chi-Hsiang Chung, Jiann-Torng Chen, and Ching-Long Chen. 2023. "Impact of Endophthalmitis on the Risk of Acute Myocardial Infarction in Ankylosing Spondylitis Patients: A Population-Based Retrospective Cohort Study" Journal of Clinical Medicine 12, no. 3: 1211. https://doi.org/10.3390/jcm12031211
APA StyleLin, T.-Y., Lai, Y.-F., Chien, W.-C., Chen, Y.-H., Chung, C.-H., Chen, J.-T., & Chen, C.-L. (2023). Impact of Endophthalmitis on the Risk of Acute Myocardial Infarction in Ankylosing Spondylitis Patients: A Population-Based Retrospective Cohort Study. Journal of Clinical Medicine, 12(3), 1211. https://doi.org/10.3390/jcm12031211