
Survival Outcome of Gastric Signet Ring Cell Carcinoma Based on the Optimal Number of Examined Lymph Nodes: A Nomogram- and Machine-Learning-Based Approach
 and
and
Abstract
:1. Introduction
2. Patients and Methods
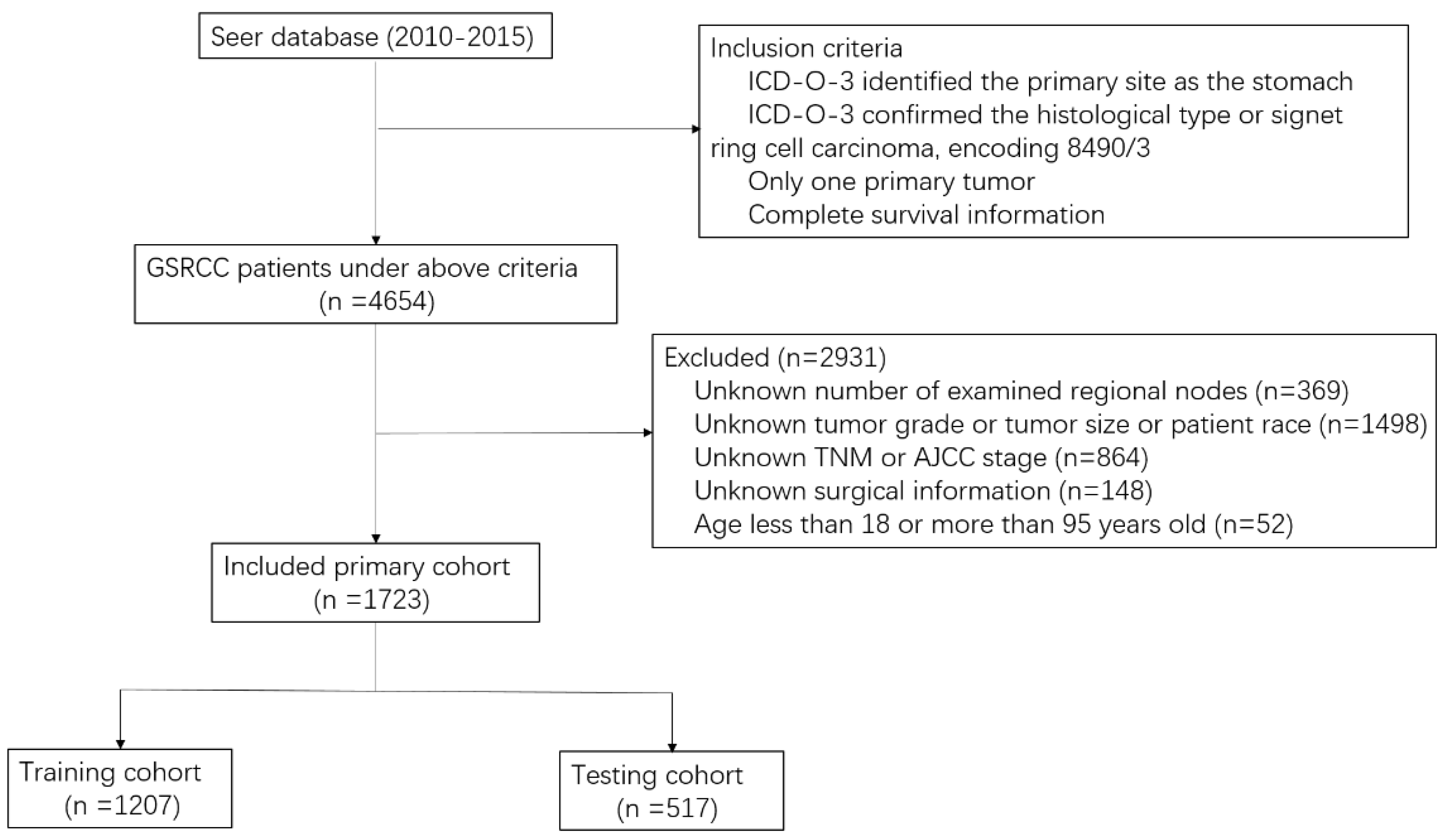
2.1. Data Source and Study Population
2.2. Calculation of Cutoff Value for ELNs
2.3. Model Development
2.4. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Demarcation of the Minimum Number of ELNs
3.3. Baseline Comparisons on ELNs ≥ 32 and ELNs < 32 (Pre-PSM and Post-PSM)
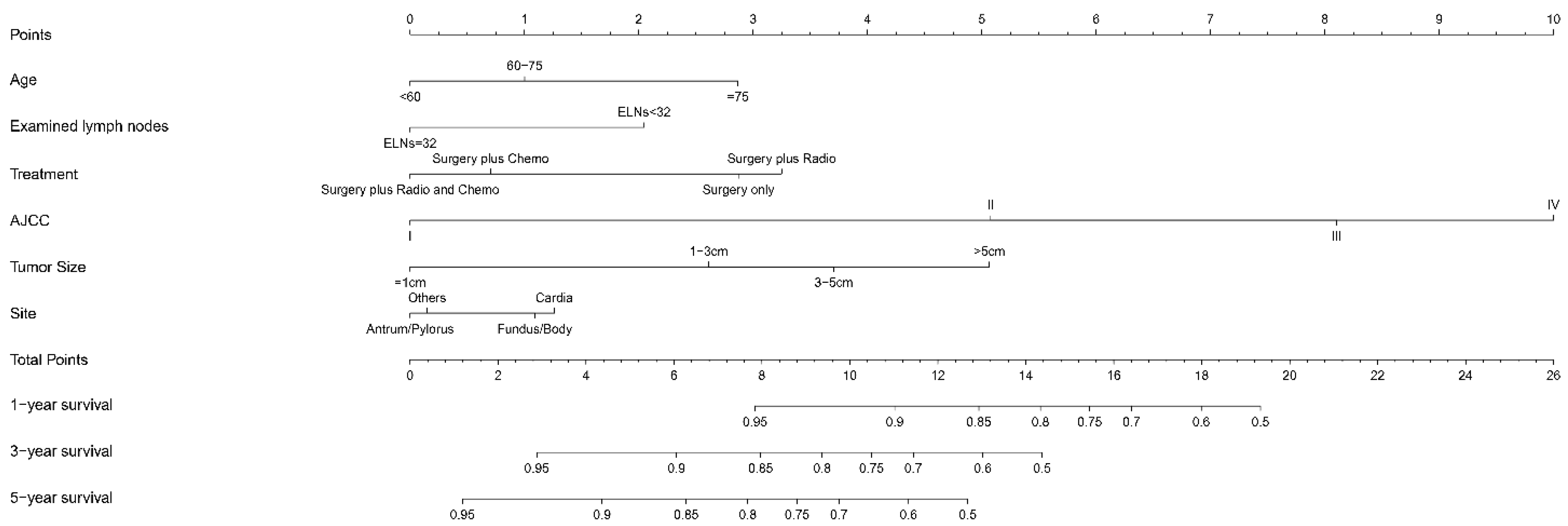
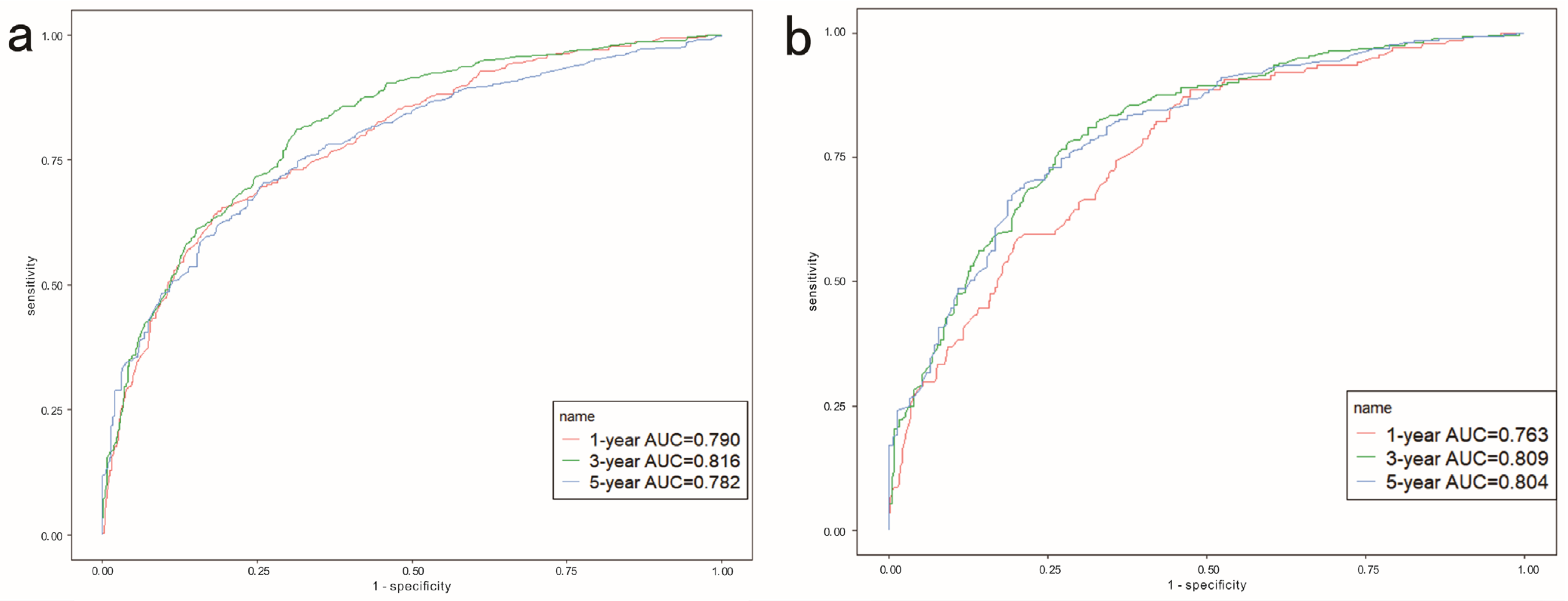
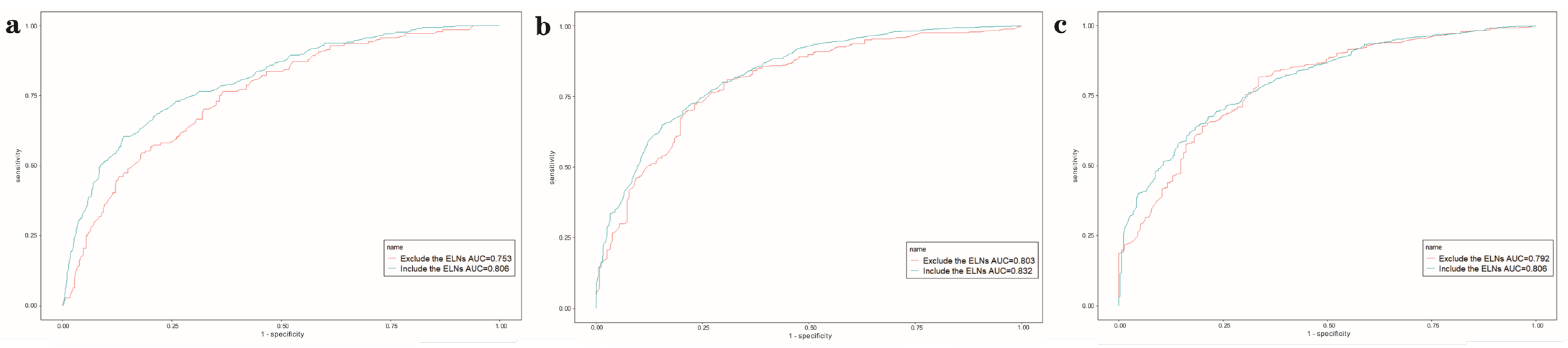
3.4. Development and Assessment of the Nomogram
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Smyth, E.C.; Nilsson, M.; Grabsch, H.I.; van Grieken, N.C.; Lordick, F. Gastric cancer. Lancet 2020, 396, 635–648. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Zhu, Z.; Ma, F.; Xue, L.; Tian, Y. Gastric Signet Ring Cell Carcinoma: Current Management and Future Challenges. Cancer Manag. Res. 2020, 12, 7973–7981. [Google Scholar] [CrossRef] [PubMed]
- Arai, T. Where does signet-ring cell carcinoma come from and where does it go? Gastric Cancer 2019, 22, 651–652. [Google Scholar] [CrossRef] [PubMed]
- Tang, C.-T.; Chen, Y.; Zeng, C. Prognostic analysis of gastric signet ring cell carcinoma and mucinous carcinoma: A propensity score-matched study and competing risk analysis. Aging 2020, 12, 22059–22077. [Google Scholar] [CrossRef]
- Zhang, S.; Liu, Y.; Jiao, Z.; Li, Z.; Wang, J.; Li, C.; Qu, X.; Xu, L. Development and Validation of a Prognostic Nomogram for Gastric Signet Ring Cell Carcinoma: A Multicenter Population-Based Study. Front. Oncol. 2021, 11, 603031. [Google Scholar] [CrossRef]
- Yang, X.-F.; Yang, L.Y.X.-F.; Mao, X.-Y.; Wu, D.-Y.; Zhang, S.-M.; Xin, Y. Pathobiological behavior and molecular mechanism of signet ring cell carcinoma and mucinous adenocarcinoma of the stomach: A comparative study. World J. Gastroenterol. 2004, 10, 750–754. [Google Scholar] [CrossRef]
- Wang, H.; Peng, Y.; Huang, Q.; Wu, J.; Zhang, M. Prognostic Nomograms for Nonelderly Adults with Gastric Signet Ring Cell Carcinoma. BioMed Res. Int. 2021, 2021, 1274527. [Google Scholar] [CrossRef]
- Morkavuk, Ş.B.; Çulcu, S.; Tez, M.; Ünal, A.E. The efficiency of D1(+) lymphadenectomy in signet ring cell carcinoma: Comparison of postoperative early and late outcomes between standard lymphadenectomy and D1(+) lymphadenectomy. Libyan J. Med. 2021, 16, 1973761. [Google Scholar] [CrossRef]
- Wei, F.; Lyu, H.; Wang, S.; Chu, Y.; Chen, F. Positive lymph node ratio as a novel indicator of prognosis in gastric signet ring cell carcinoma: A population-based retrospective study. Transl. Cancer Res. 2020, 9, 3658–3668. [Google Scholar] [CrossRef]
- Xu, Z.; Jing, J.; Ma, G. Development and validation of prognostic nomogram based on log odds of positive lymph nodes for patients with gastric signet ring cell carcinoma. Chin. J. Cancer Res. 2020, 32, 778–793. [Google Scholar] [CrossRef]
- Ajani, J.A.; D’Amico, T.A.; Bentrem, D.J.; Chao, J.; Cooke, D.; Corvera, C.; Das, P.; Enzinger, P.C.; Enzler, T.; Fanta, P.; et al. Gastric Cancer, Version 2.2022, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Cancer Netw. 2022, 20, 167–192. [Google Scholar] [CrossRef] [PubMed]
- Hu, Q.; Pan, S.; Guo, Z. A novel pN3 gastric cancer staging system with superior prognostic utility based upon the examination of over 31 lymph nodes: A propensity score-matching analysis. BMC Gastroenterol. 2021, 21, 352. [Google Scholar] [CrossRef] [PubMed]
- Erstad, D.J.; Blum, M.; Estrella, J.S.; Das, P.; Minsky, B.D.; Ajani, J.A.; Mansfield, P.F.; Ikoma, N.; Badgwell, B.D. Navigating Nodal Metrics for Node-Positive Gastric Cancer in the United States: An NCDB-Based Study and Validation of AJCC Guidelines. J. Nat. Compr. Cancer Netw. 2021, 19, 86–97. [Google Scholar] [CrossRef] [PubMed]
- Camp, R.L.; Dolled-Filhart, M.; Rimm, D.L. X-tile: A new bio-informatics tool for biomarker assessment and outcome-based cut-point optimization. Clin. Cancer Res. 2004, 10, 7252–7259. [Google Scholar] [CrossRef]
- Dabiri, Y.; Van der Velden, A.; Sack, K.L.; Choy, J.S.; Kassab, G.S.; Guccione, J.M. Prediction of Left Ventricular Mechanics Using Machine Learning. Front. Phys. 2019, 7, 117. [Google Scholar] [CrossRef]
- Taghavi, S.; Jayarajan, S.N.; Davey, A.; Willis, A.I. Prognostic significance of signet ring gastric cancer. J. Clin. Oncol. 2012, 30, 3493–3498. [Google Scholar] [CrossRef]
- Li, Y.; Ma, F.-H.; Xue, L.-Y.; Tian, Y.-T. Neoadjuvant chemotherapy vs upfront surgery for gastric signet ring cell carcinoma: A retrospective, propensity score-matched study. World J. Gastroenterol. 2020, 26, 818–827. [Google Scholar] [CrossRef]
- Kerckhoffs, K.G.P.; Liu, D.H.W.; Saragoni, L.; van der Post, R.S.; Langer, R.; Bencivenga, M.; Iglesias, M.; Gallo, G.; Hewitt, L.C.; Fazzi, G.E.; et al. Mucin expression in gastric- and gastro-oesophageal signet-ring cell cancer: Results from a comprehensive literature review and a large cohort study of Caucasian and Asian gastric cancer. Gastric Cancer 2020, 23, 765–779. [Google Scholar] [CrossRef]
- Lee, H.K.; Yang, H.-K.; Kim, W.H.; Lee, K.U.; Choe, K.J.; Kim, J.-P. Influence of the number of lymph nodes examined on staging of gastric cancer. Br. J. Surg. 2001, 88, 1408–1412. [Google Scholar] [CrossRef]
- Zhu, Z.; written on behalf of AME Lung Cancer Collaborative Group; Song, Z.; Jiao, W.; Mei, W.; Xu, C.; Huang, Q.; An, C.; Shi, J.; Wang, W.; et al. A large real-world cohort study of examined lymph node standards for adequate nodal staging in early non-small cell lung cancer. Transl. Lung Cancer Res. 2021, 10, 815–825. [Google Scholar] [CrossRef]
- Smith, D.D.; Schwarz, R.R.; Schwarz, R.E. Impact of total lymph node count on staging and survival after gastrectomy for gastric cancer: Data from a large US-population database. J. Clin. Oncol. 2005, 23, 7114–7124. [Google Scholar] [CrossRef] [PubMed]
- Brenkman, H.J.F.; Goense, L.; Brosens, L.A.; Mohammad, N.H.; Vleggaar, F.P.; Ruurda, J.P.; van Hillegersberg, R. A High Lymph Node Yield is Associated with Prolonged Survival in Elderly Patients Undergoing Curative Gastrectomy for Cancer: A Dutch Population-Based Cohort Study. Ann. Surg. Oncol. 2017, 24, 2213–2223. [Google Scholar] [CrossRef]
- Ichikura, T.; Ogawa, T.; Chochi, K.; Kawabata, T.; Sugasawa, H.; Mochizuki, H. Minimum number of lymph nodes that should be examined for the International Union Against Cancer/American Joint Committee on Cancer TNM classification of gastric carcinoma. World J. Surg. 2003, 27, 330–333. [Google Scholar] [CrossRef]
- Schwarz, R.E.; Smith, D.D. Clinical impact of lymphadenectomy extent in resectable gastric cancer of advanced stage. Ann. Surg. Oncol. 2007, 14, 317–328. [Google Scholar] [CrossRef] [PubMed]
- Mirkin, K.A.; Hollenbeak, C.S.; Wong, J. Greater Lymph Node Retrieval Improves Survival in Node-Negative Resected Gastric Cancer in the United States. J. Gastric Cancer 2017, 17, 306–318. [Google Scholar] [CrossRef] [PubMed]
- Amin, M.B.; Greene, F.L.; Edge, S.B.; Compton, C.C.; Gershenwald, J.E.; Brookland, R.K.; Meyer, L.; Gress, D.M.; Byrd, D.R.; Winchester, D.P. The Eighth Edition AJCC Cancer Staging Manual: Continuing to build a bridge from a population-based to a more “personalized” approach to cancer staging. CA Cancer J. Clin. 2017, 67, 93–99. [Google Scholar] [CrossRef] [PubMed]
- Huang, L.; Zhang, X.; Wei, Z.; Xu, A. Importance of Examined Lymph Node Number in Accurate Staging and Enhanced Survival in Resected Gastric Adenocarcinoma—The More, the Better? A Cohort Study of 8,696 Cases From the US and China, 2010–2016. Front. Oncol. 2020, 10, 539030. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | All Patients (n = 1723) | Training Cohort (n = 1206) | Validation Cohort (n = 517) |
|---|---|---|---|
| Age (median, IQR) | 63 (53–72) | 63 (52–72) | 62 (52–72) |
| Sex [No. (%)] | |||
| Male | 873 (50.7) | 613 (50.8) | 260 (50.3) |
| Female | 850 (49.3) | 593 (49.2) | 257 (49.7) |
| Race [No. (%)] | |||
| White | 1151 (66.8) | 797 (66.1) | 354 (68.5) |
| Black | 203 (11.8) | 145 (12) | 58 (11.2) |
| Other | 369 (21.4) | 264 (21.9) | 105 (20.3) |
| Grade [No. (%)] | |||
| I | 2 (0.1) | 1 (0.1) | 1 (0.2) |
| II | 45 (2.6) | 32 (2.7) | 13 (2.5) |
| III | 1628 (94.5) | 1141 (94.5) | 487 (94.2) |
| IV | 48 (2.8) | 32 (2.7) | 16 (3.1) |
| Size [No. (%)] | |||
| ≤1 cm | 117 (6.8) | 85 (7) | 39 (7.5) |
| 1–2 cm | 249 (14.5) | 173 (14.3) | 80 (15.5) |
| 2–3 cm | 267 (15.5) | 186 (15.4) | 74 (14.3) |
| 3–4 cm | 236 (13.7) | 168 (13.9) | 76 (14.7) |
| 4–5 cm | 201 (11.6) | 148 (12.3) | 65 (12.6) |
| >5 cm | 653 (37.9) | 446 (37.1) | 183 (35.4) |
| Examined lymph node count (year, mean ± SD) | 20.4 ± 0.33 | 20.3 ± 0.39 | 20.7 ± 0.62 |
| Site [No. (%)] | |||
| Cardia | 239 (13.9) | 165 (13.7) | 74 (14.3) |
| Fundus of stomach | 42 (2.4) | 34 (2.8) | 8 (1.6) |
| Body of stomach | 207 (12) | 143 (11.9) | 64 (12.4) |
| Gastric antrum | 492 (28.6) | 342 (28.4) | 150 (29) |
| Pylorus | 91 (5.3) | 71 (5.9) | 20 (3.9) |
| Lesser curvature of stomach | 228 (13.2) | 158 (13.1) | 70 (13.5) |
| Greater curvature of stomach | 102 (5.9) | 73 (6.1) | 27 (5.2) |
| Overlapping | 177 (10.3) | 115 (9.5) | 62 (12) |
| Stomach NOS | 145 (8.4) | 103 (8.6) | 42 (8.1) |
| Therapy [No. (%)] | |||
| Surgery only | 633 (36.7) | 447 (37.1) | 186 (36) |
| Surgery plus radio | 22 (1.3) | 14 (1.2) | 8 (1.5) |
| Surgery plus chemo | 517 (30) | 354 (29.3) | 163 (31.5) |
| Surgery plus cadio and chemo | 551 (32) | 391 (32.4) | 160 (31) |
| AJCC [No. (%)] | |||
| I | 379 (22) | 273 (22.6) | 106 (20.5) |
| II | 374 (21.7) | 268 (22.2) | 106 (20.5) |
| III | 785 (45.6) | 540 (44.8) | 245 (47.4) |
| IV | 185 (10.7) | 125 (10.4) | 60 (11.6) |
| Overall survival [No. (%)] | |||
| 1-year | 1278 (74.2) | 902 (74.8) | 376 (72.7) |
| 3-year | 810 (47) | 577 (47.8) | 233 (45.1) |
| 5-year | 510 (29.6) | 355 (29.4) | 155 (30) |
| Cut off Value for ELNs | Chi-Square Score | Relative Risk | p Value |
|---|---|---|---|
| <15 vs. ≥15 | 3.02 | 1.05 | 0.18 |
| <16 vs. ≥16 | 2.92 | 1.04 | 0.083 |
| <17 vs. ≥17 | 3.67 | 1.05 | 0.088 |
| <18 vs. ≥18 | 3.53 | 1.06 | 0.056 |
| <19 vs. ≥19 | 5.35 | 1.07 | 0.061 |
| <20 vs. ≥20 | 4.21 | 1.06 | 0.021 |
| <21 vs. ≥21 | 4.45 | 1.06 | 0.041 |
| <22 vs. ≥22 | 3.96 | 1.05 | 0.035 |
| <23 vs. ≥23 | 3.53 | 1.05 | 0.047 |
| <24 vs. ≥24 | 2.51 | 1.03 | 0.58 |
| <25 vs. ≥25 | 4.39 | 1.05 | 0.11 |
| <26 vs. ≥26 | 3.79 | 1.05 | 0.037 |
| <27 vs. ≥27 | 3.06 | 1.05 | 0.052 |
| <28 vs. ≥28 | 3.4 | 1.06 | 0.081 |
| <29 vs. ≥29 | 4.04 | 1.07 | 0.066 |
| <30 vs. ≥30 | 3.44 | 1.07 | 0.045 |
| <31 vs. ≥31 | 4.35 | 1.09 | 0.063 |
| <32 vs. ≥32 | 5.45 | 1.11 | 0.037 |
| <33 vs. ≥33 | 3.91 | 1.10 | 0.02 |
| <34 vs. ≥34 | 4.69 | 1.10 | 0.048 |
| <35 vs. ≥35 | 3.48 | 1.10 | 0.03 |
| Characteristics | Before Matching | After Matching | ||||
|---|---|---|---|---|---|---|
| ELN < 32 (n = 1430) | ELN ≥ 32 (n = 293) | p | ELN < 32 (n = 548) | ELN ≥ 32 (n = 291) | p | |
| Age (median, IQR) | 63 (52–73) | 60 (50–68) | 60 (51–71) | 60 (50–68) | 0.121 | |
| Sex [No. (%)] | 0.843 | 0.640 | ||||
| Male | 723 (50.6) | 150 (51.2) | 288 (52.6) | 148 (52.9) | ||
| Female | 707 (49.4) | 143 (48.8) | 260 (47.4) | 143 (49.1) | ||
| Race [No. (%)] | 0.015 | 0.519 | ||||
| White | 955 (66.8) | 196 (66.9) | 359 (65.5) | 194 (66.7) | ||
| Black | 181 (12.7) | 22 (7.5) | 72 (13.1) | 22 (7.5) | ||
| Other | 294 (20.5) | 75 (25.6) | 117 (21.4) | 75 (25.8) | ||
| Grade [No. (%)] | 0.789 | 0.988 | ||||
| I | 2 (0.1) | 0 | 0 | 0 | ||
| II | 39 (2.7) | 6 (2) | 9 (1.6) | 5 (1.7) | ||
| III | 1348 (94.3) | 280 (95.6) | 525 (95.8) | 279 (95.9) | ||
| IV | 41 (2.9) | 7 (2.4) | 14 (2.6) | 7 (2.4) | ||
| Size [No. (%)] | 0.002 | 0.485 | ||||
| ≤1 cm | 107 (7.5) | 10 (3.4) | 24 (4.4) | 10 (3.4) | ||
| 1–2 cm | 212 (14.8) | 37 (12.6) | 53 (9.7) | 35 (12) | ||
| 2–3 cm | 225 (15.7) | 42 (14.3) | 65 (11.8) | 42 (14.4) | ||
| 3–4 cm | 205 (14.3) | 31 (10.6) | 77 (14.1) | 31 (10.7) | ||
| 4–5 cm | 169 (11.8) | 32 (10.9) | 68 (12.4) | 32 (11) | ||
| >5 cm | 512 (35.9) | 141 (48.2) | 261 (47.6) | 141 (48.5) | ||
| Site [No. (%)] | 0.003 | 0.064 | ||||
| Cardia | 210 (14.7) | 29 (9.9) | 69 (12.6) | 28 (9.6) | ||
| Fundus of stomach | 34 (2.4) | 8 (2.7) | 10 (1.8) | 8 (2.7) | ||
| Body of stomach | 159 (11.1) | 48 (16.4) | 60 (10.9) | 47 (16.2) | ||
| Gastric antrum | 427 (29.9) | 65 (22.2) | 155 (28.3) | 65 (22.3) | ||
| Pylorus | 81 (5.7) | 10 (3.4) | 31 (5.7) | 10 (3.4) | ||
| Lesser curvature of stomach | 182 (12.7) | 46 (15.7) | 74 (13.6) | 46 (15.8) | ||
| Greater curvature of stomach | 84 (5.9) | 18 (6.1) | 27 (4.9) | 18 (6.2) | ||
| Overlapping | 141 (9.8) | 36 (12.3) | 78 (14.2) | 36 (12.4) | ||
| Stomach NOS | 112 (7.8) | 33 (11.3) | 44 (8) | 33 (11.4) | ||
| Therapy [No. (%)] | 0.001 | 0.130 | ||||
| Surgery only | 555 (38.8) | 78 (26.6) | 161 (29.4) | 76 (26.1) | ||
| Surgery plus radio | 18 (1.3) | 4 (1.4) | 7 (1.3) | 4 (1.4) | ||
| Surgery plus chemo | 391 (27.3) | 126 (43) | 175 (31.9) | 126 (43.3) | ||
| Surgery plus radio and chemo | 466 (32.6) | 85 (29) | 205 (37.4) | 85 (29.2) | ||
| AJCC [No. (%)] | 0.001 | 0.469 | ||||
| I | 329 (23) | 50 (17) | 81 (14.8) | 48 (16.5) | ||
| II | 326 (22.8) | 48 (16.4) | 113 (20.6) | 48 (16.5) | ||
| III | 621 (43.4) | 164 (56) | 304 (55.5) | 164 (56.4) | ||
| IV | 154 (10.8) | 31 (10.6) | 50 (9.1) | 31 (10.6) | ||
| Overall survival [No. (%)] | ||||||
| 1-year | 1043 (72.9) | 235 (80.2) | 0.01 | 393 (71.7) | 233 (80.1) | 0.008 |
| 3-year | 659 (46.1) | 151 (51.5) | 0.088 | 229 (41.8) | 149 (51.2) | 0.009 |
| 5-year | 420 (29.4) | 90 (30.7) | 0.646 | 148 (27) | 88 (30.2) | 0.032 |
| Variable | n | Univariate Analyses | Multivariable Analyses | ||
|---|---|---|---|---|---|
| p | HR | CI | p | ||
| Age | |||||
| <60 | 523 (43.4) | Reference | - | - | Reference |
| 60–75 | 481 (39.9) | 0.002 | 1.251 | 1.065–1.471 | 0.006 |
| ≥75 | 202 (16.7) | <0.001 | 1.898 | 1.543–2.335 | <0.001 |
| Sex | |||||
| Male | 613 (50.8) | Reference | |||
| Female | 593 (49.2) | 0.268 | |||
| Race | |||||
| White | 797 (66.1) | Reference | |||
| Black | 145 (12) | 0.471 | |||
| Other | 264 (21.9) | 0.216 | |||
| Grade | |||||
| I | 1 (0.1) | Reference | |||
| II | 32 (2.7) | 0.819 | |||
| III | 1141 (94.6) | 0.82 | |||
| IV | 32 (2.7) | 0.823 | |||
| Size | |||||
| ≤1 cm | 85 (7) | Reference | - | - | Reference |
| 1–3 cm | 359 (29.8) | <0.001 | 1.813 | 1.097–2.996 | 0.02 |
| 3–5 cm | 316 (26.2) | <0.001 | 2.312 | 1.382–3.868 | 0.001 |
| >5 cm | 446 (37) | <0.001 | 3.131 | 1.867–5.251 | <0.001 |
| ELNs | |||||
| <32 | 1004 (83.3) | Reference | - | - | Reference |
| ≥32 | 202 (16.7) | 0.014 | 0.633 | 0.518–0.775 | <0.001 |
| Site | |||||
| Others | 451 (37.4) | Reference | - | - | Reference |
| Cardia | 165 (13.7) | 0.362 | 1.282 | 1.017–1.617 | 0.036 |
| Fundus/Body | 177 (14.7) | 0.633 | 1.234 | 0.981–1.533 | 0.072 |
| Antrum/Pylorus | 413 (34.2) | 0.042 | 0.967 | 0.729–1.282 | 0.814 |
| Therapy | |||||
| Surgery only | 447 (37.1) | Reference | - | - | Reference |
| Surgery plus radio | 14 (1.2) | 0.006 | 1.090 | 0.617–1.926 | 0.767 |
| Surgery plus chemo | 354 (29.4) | 0.012 | 0.619 | 0.508–0.754 | <0.001 |
| Surgery plus radio and chemo | 391 (32.4) | 0.585 | 0.529 | 0.434–0.644 | <0.001 |
| AJCC | |||||
| I | 273 (22.6) | Reference | - | - | Reference |
| II | 268 (22.2) | <0.001 | 3.127 | 2.308–4.235 | <0.001 |
| III | 540 (44.8) | <0.001 | 6.150 | 4.577–8.264 | <0.001 |
| IV | 125 (10.4) | <0.001 | 9.373 | 6.701–13.111 | <0.001 |
| AUC | ||||
|---|---|---|---|---|
| C-Index (Internal Validation) | 1-Year Survival | 3-Year Survival | 5-Year Survival | |
| Training cohort | 0.748 | 0.790 | 0.816 | 0.782 |
| Testing cohort | - | 0.763 | 0.809 | 0.804 |
| XGBoost | ||||
| Including ELNs | 0.803 | 0.832 | 0.806 | |
| Excluding ELNs | 0.753 | 0.803 | 0.792 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lai, Y.; Xie, J.; Yin, X.; Lai, W.; Tang, J.; Du, Y.; Li, Z. Survival Outcome of Gastric Signet Ring Cell Carcinoma Based on the Optimal Number of Examined Lymph Nodes: A Nomogram- and Machine-Learning-Based Approach. J. Clin. Med. 2023, 12, 1160. https://doi.org/10.3390/jcm12031160
Lai Y, Xie J, Yin X, Lai W, Tang J, Du Y, Li Z. Survival Outcome of Gastric Signet Ring Cell Carcinoma Based on the Optimal Number of Examined Lymph Nodes: A Nomogram- and Machine-Learning-Based Approach. Journal of Clinical Medicine. 2023; 12(3):1160. https://doi.org/10.3390/jcm12031160
Chicago/Turabian StyleLai, Yongkang, Junfeng Xie, Xiaojing Yin, Weiguo Lai, Jianhua Tang, Yiqi Du, and Zhaoshen Li. 2023. "Survival Outcome of Gastric Signet Ring Cell Carcinoma Based on the Optimal Number of Examined Lymph Nodes: A Nomogram- and Machine-Learning-Based Approach" Journal of Clinical Medicine 12, no. 3: 1160. https://doi.org/10.3390/jcm12031160
APA StyleLai, Y., Xie, J., Yin, X., Lai, W., Tang, J., Du, Y., & Li, Z. (2023). Survival Outcome of Gastric Signet Ring Cell Carcinoma Based on the Optimal Number of Examined Lymph Nodes: A Nomogram- and Machine-Learning-Based Approach. Journal of Clinical Medicine, 12(3), 1160. https://doi.org/10.3390/jcm12031160